Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Bactéries multirésistantes : place de l’antibiothérapie actuelle
Abdelfattah CHAKIB Faculté de médecine et de pharmacie Service des maladies infectieuses CHU Ibn Rochd , Casablanca 4 émes journées Nationales de biologie praticienne mars 2012 Robinson Club Agadir

2
Définition d’une bactérie multirésistante
Pas de définition universelle Les bactéries sont dites multirésistantes aux antibiotiques (BMR) lorsque, du fait de l'accumulation des résistances naturelles et acquises, elles ne sont plus sensibles qu'à un petit nombre d'antibiotiques habituellement actifs en thérapeutique.
 lorsque, du fait de l accumulation des résistances naturelles et acquises, elles ne sont plus sensibles qu à un petit nombre d antibiotiques habituellement actifs en thérapeutique.")
9
Choix des BMR prioritaires
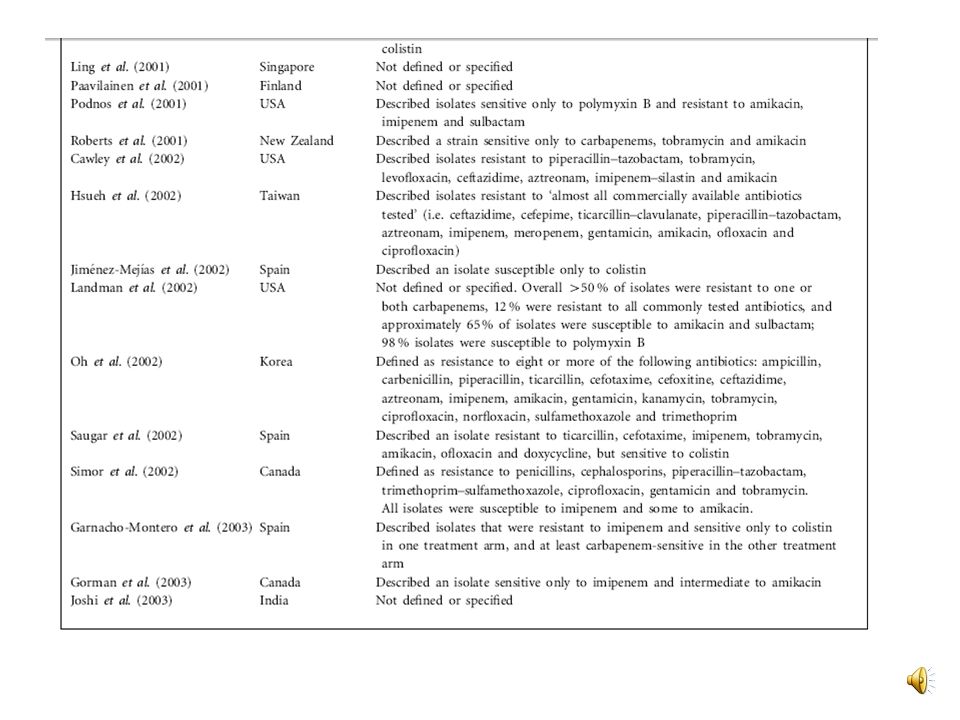
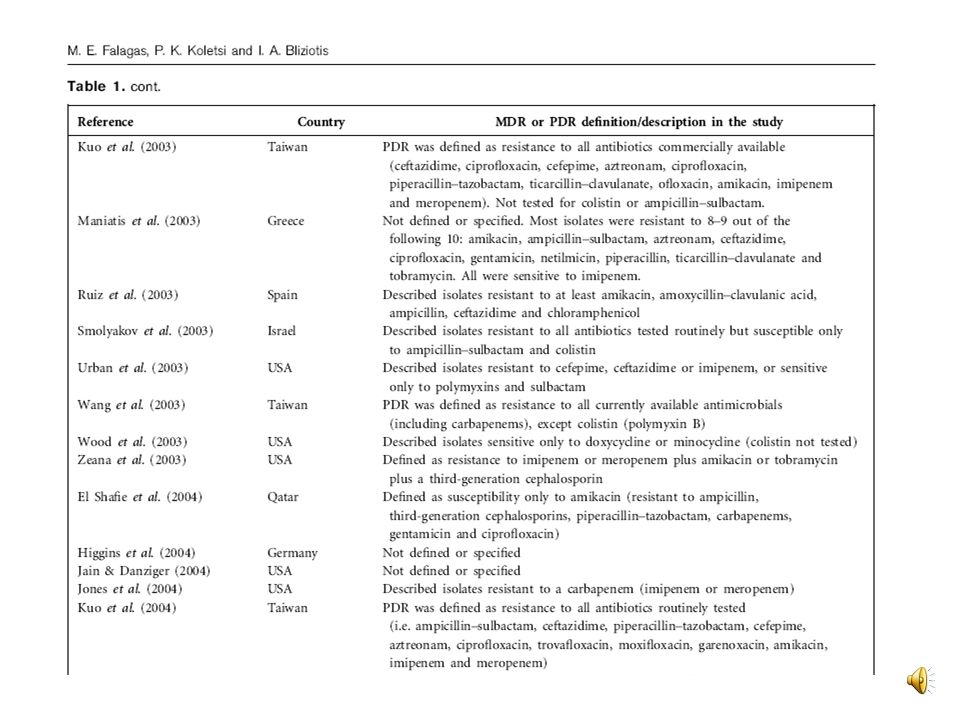
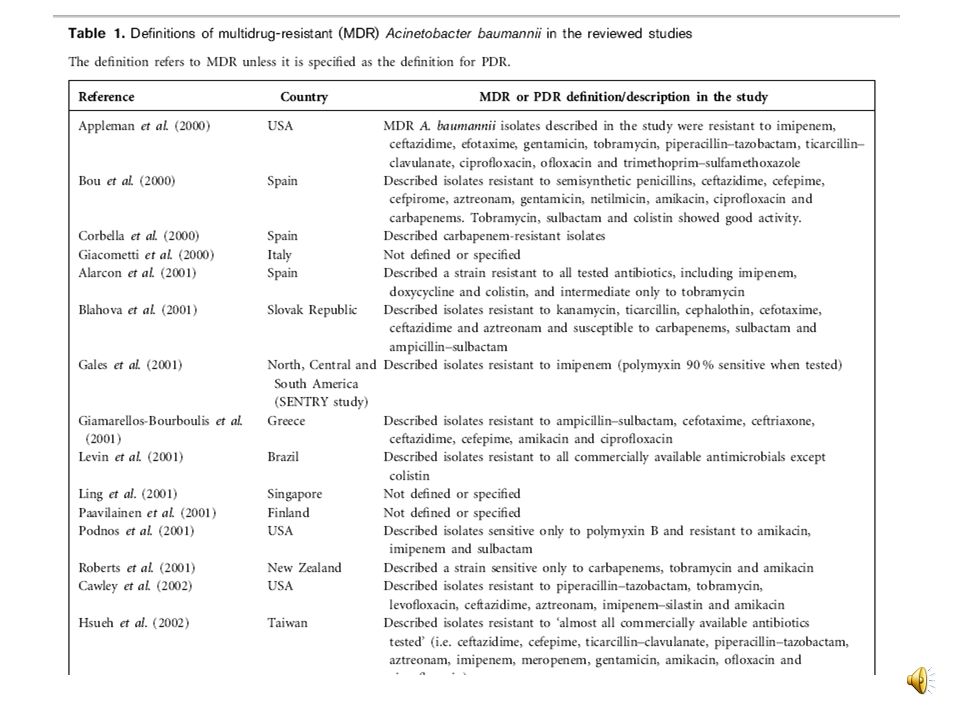
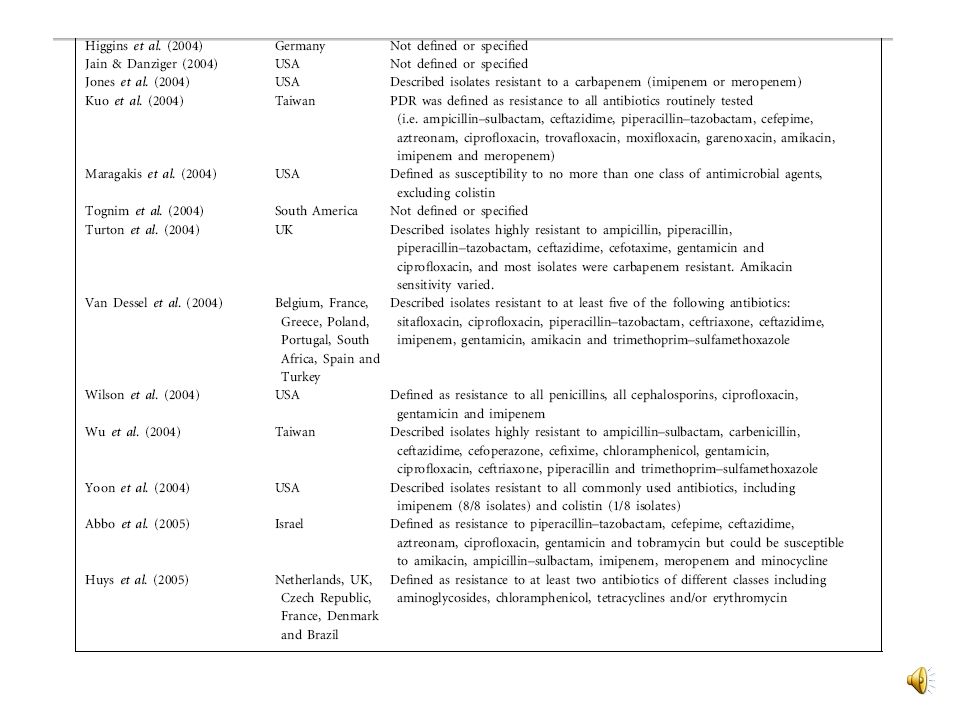
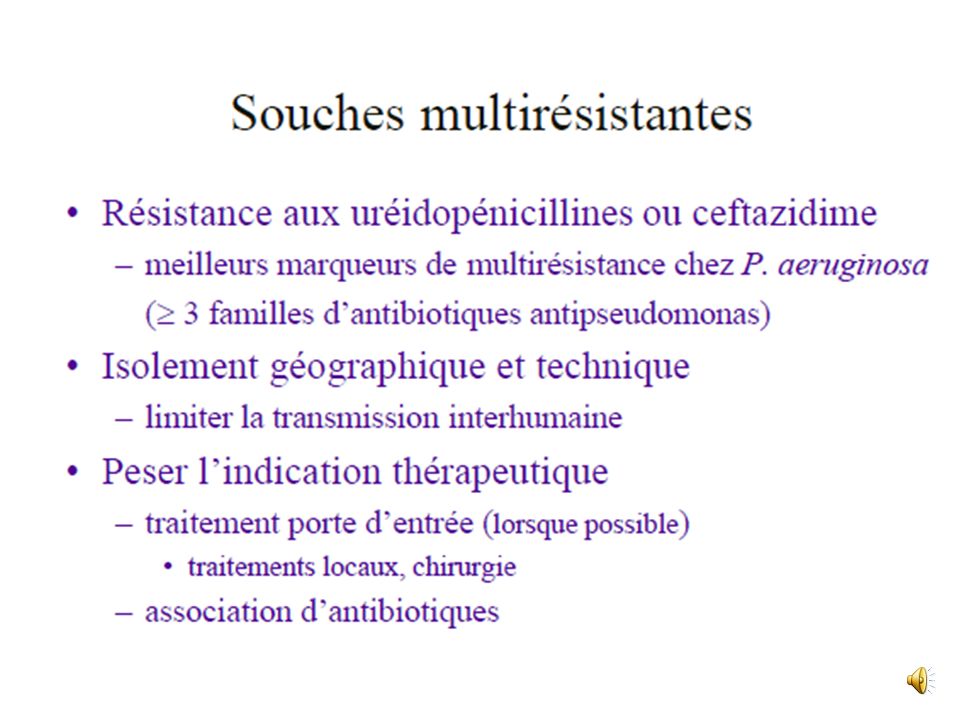
Staphylococcus aureus résistant à la méticilline (SARM) Entérobactéries productrices de ß-lactamase à spectre étendu (EBLSE) résistantes aux ß-lactamines par hyperproduction de céphalosporinase (EBCASE) Pseudomonas aeruginosa multirésistant (PAR) résistant aux ß-lactamines (ticarcilline, ceftazidime ou imipénème) Acinetobacter baumannii multirésistant (ABR) résistant à la ticarcilline, imipénème Entérocoque résistant à la vancomycine (ERV)
 Entérobactéries. productrices de ß-lactamase à spectre étendu (EBLSE) résistantes aux ß-lactamines par hyperproduction de céphalosporinase (EBCASE) Pseudomonas aeruginosa multirésistant (PAR) résistant aux ß-lactamines (ticarcilline, ceftazidime ou imipénème) Acinetobacter baumannii multirésistant (ABR) résistant à la ticarcilline, imipénème. Entérocoque résistant à la vancomycine (ERV)")
10
2 catégories « fonctionnelles » de BMR
Les BMR déjà installées : SARM , EBSLE Les BMR « émergentes , pas encore installées : ERV , EPC

11
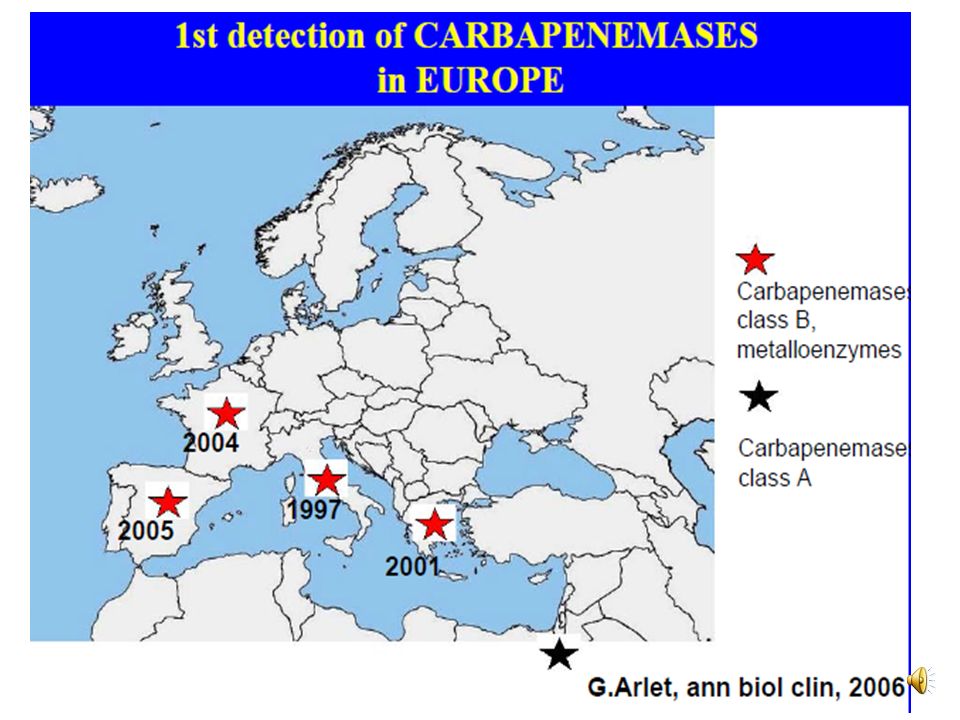
Mondialisation des BMR
K. pneumoniae Cefotaxime-R RFA 1983 E. faecium Vanco-R France 1988 E. faecium Zyvoxid-R USA 2001 S. aureus Vanco-I Japon 1996 S. aureus Vanco-R USA 2002 N. meningitidis Peni-R Spain 1988 S. typhi multiresistance Inde 1990 V. cholerae multiresistance Equateur 1993 S. dysenteriae multiresistance Burundi 1992 N. gonorrhoeae Peni-R Philippines 1976 S. pneumoniae multiresistance South Africa 1977 S. pneumoniae Peni-R Australie 1967

16
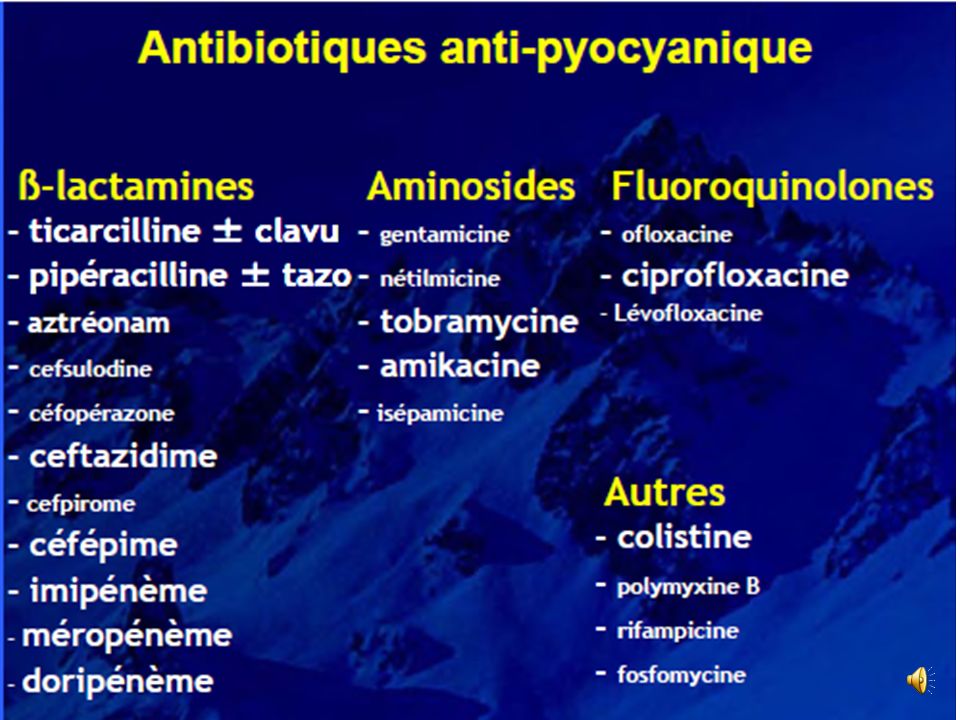
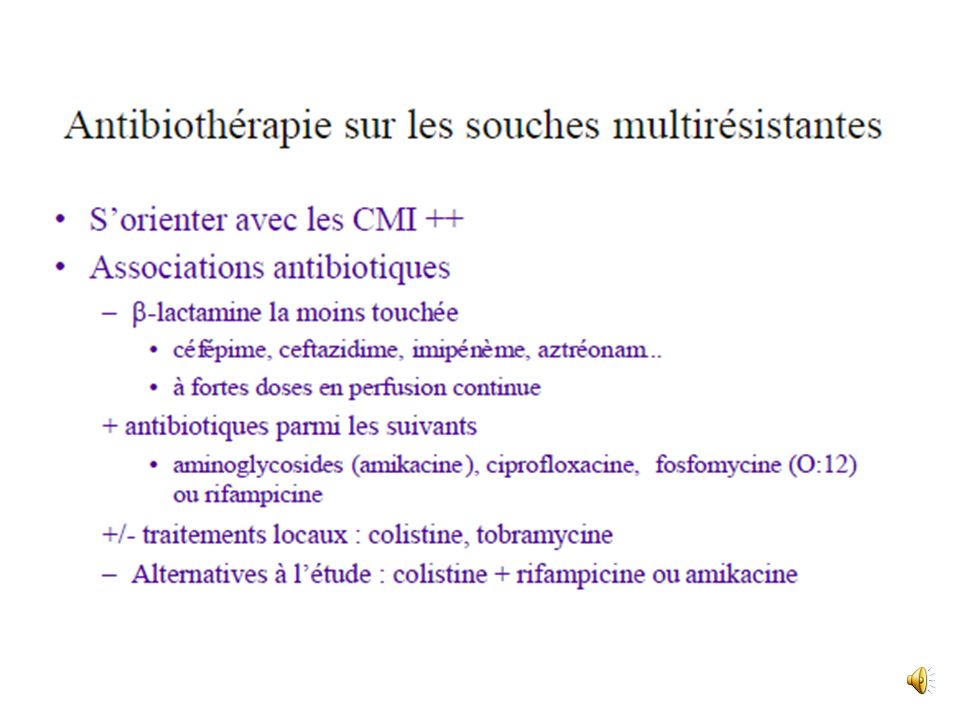
Antibiothérapie des pseudomonas aeruginosa

18
Pseudomonas aeruginosa Resistances naturelles

25
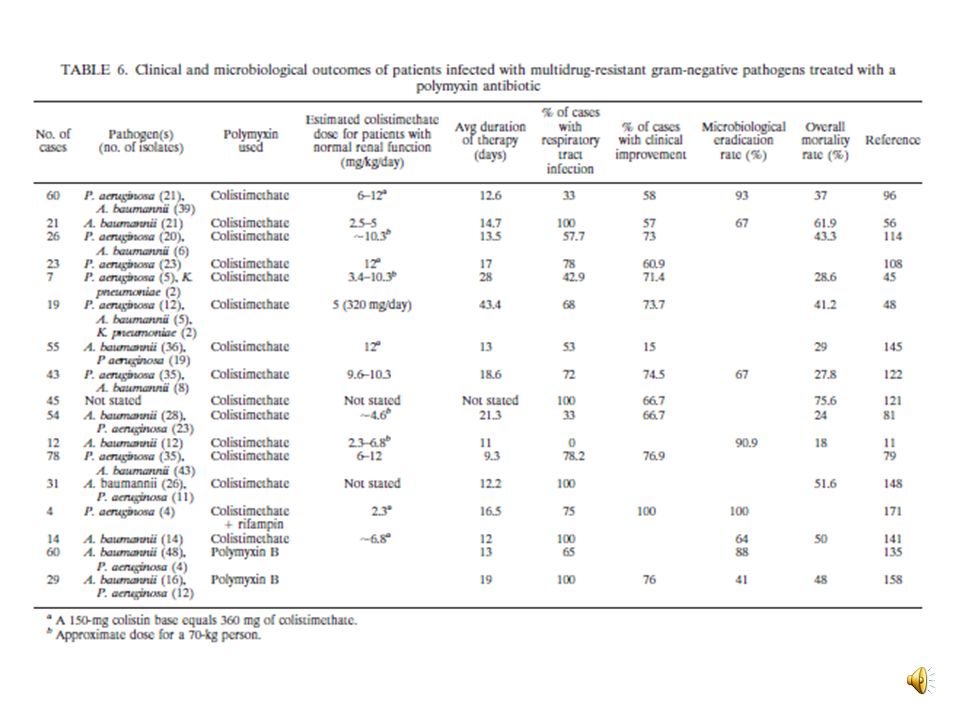
Etude prospective Pseudomonas aerugenosa et Acinetobacter baumanii multiresistants infections dont 78, 2 % pulmonaires Dose moyenne : 5,5 MUI /j Durée moyenne : 9, 3 Evolution clinique favorable: 76 ,9 % Altération de la fonction rénale: 7 cas

30
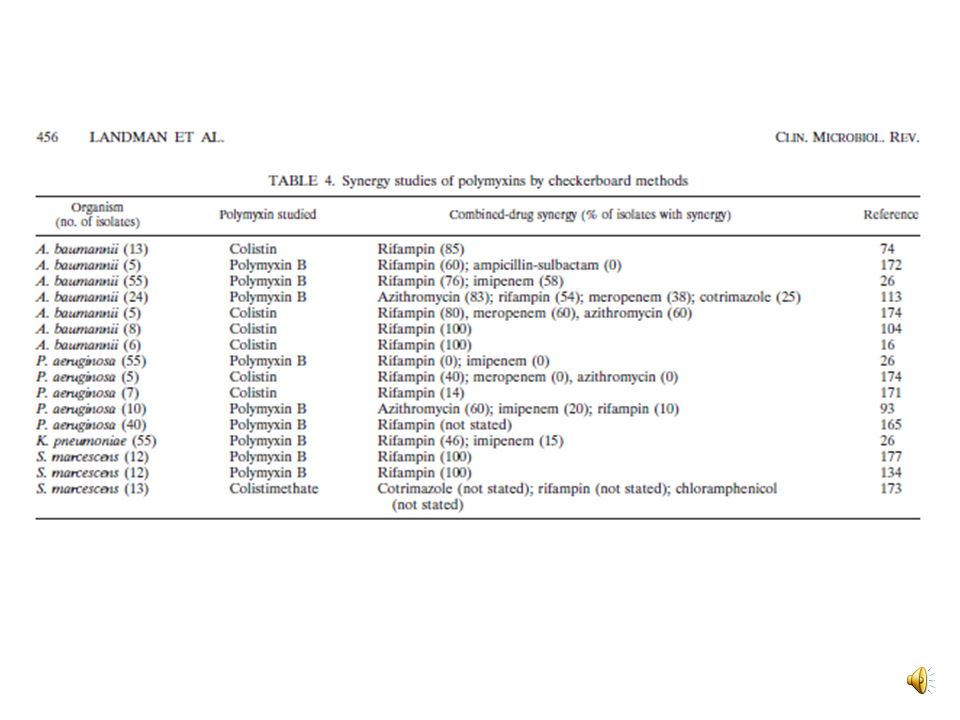
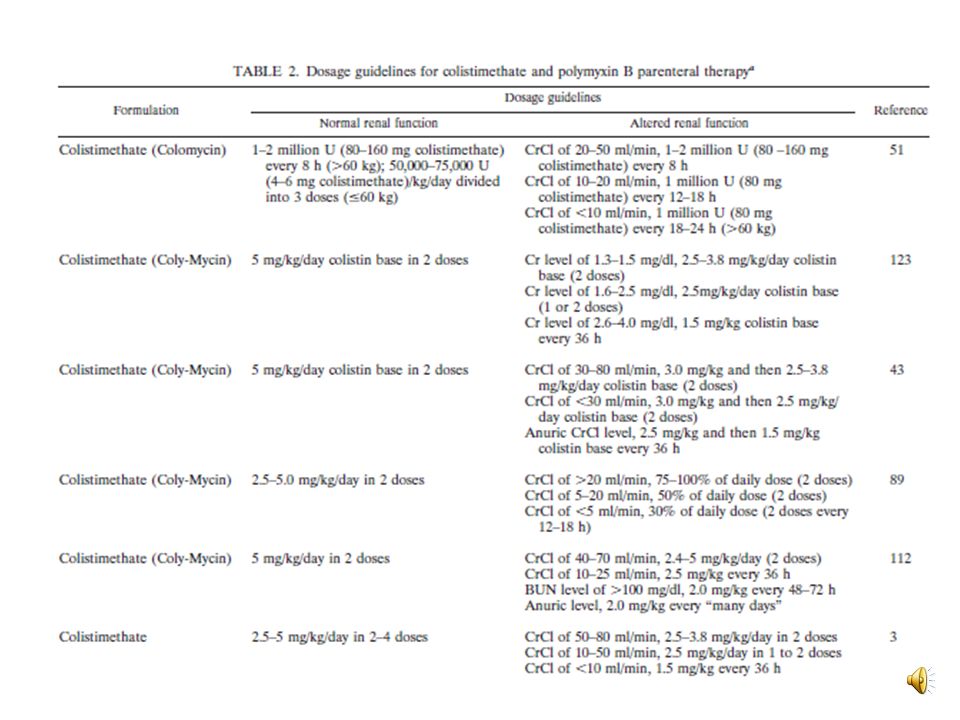
Posologie de la colimycine
IV : à UI/k /j rythme administration: 8-12 h Aérosol : à UI /dans 4 ml de eau salée ( nébulisation )
")
31
Antibiothérapie des Acinetobacter baumanii

32
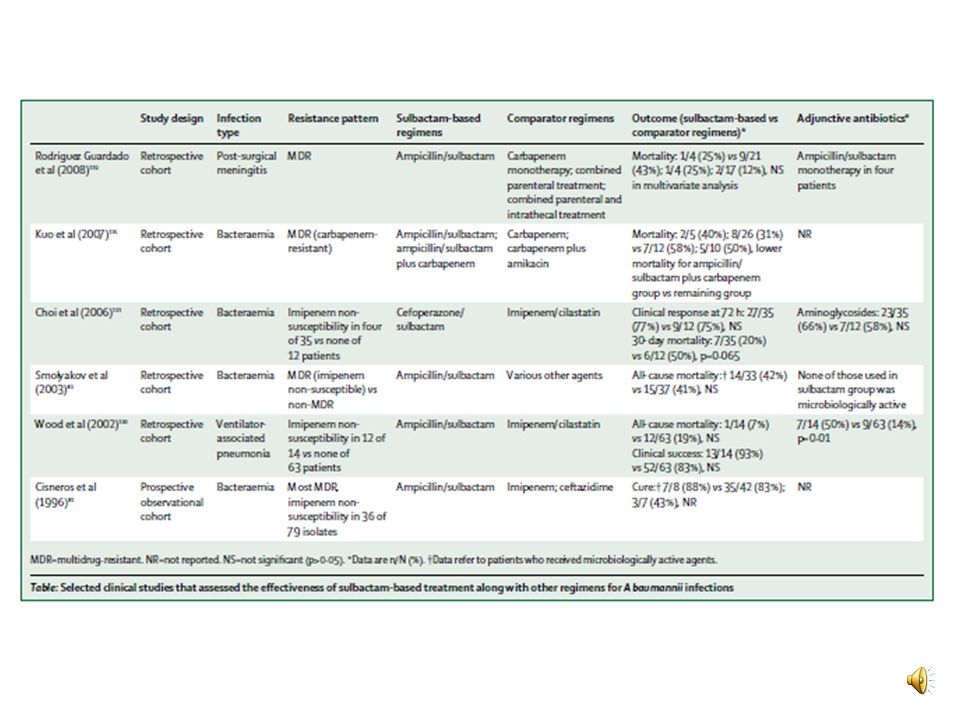
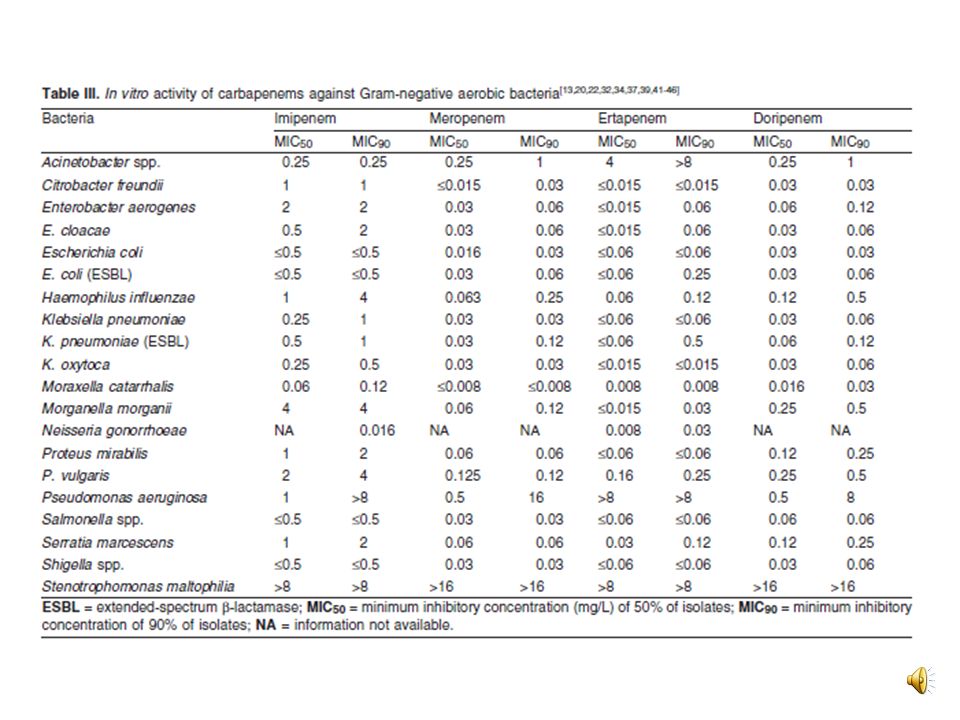
Antibiotiques potentiellement actifs sur A. baumannii
Sulbactam Pénicillines anti-pseudomonas Céphalosporines anti-pseudomonas Carbapénémes anti-pseudomonas Monobactames Aminogylcosides Fluoroquinolones Glycylcyclines Polymyxines

35
Activité des carbapenems sur mycobacterium tuberculosis ?

36
Antibiothérapie du SAMR et GISA

37
La résistance aux glycopeptides
Résistances naturelles A la vancomycine et à la teicoplanine : Leuconostoc, Pediococcus, Erysipelothrix, Lactobacillus hétérofermentaires A la vancomycine (bas niveau) Clostridium innocuum Résistances acquises Entérocoques (VRE) Staphylocoques (GISA, hGISA, VRSA) Résistance aux glycopeptides
 Clostridium innocuum. Résistances acquises. Entérocoques (VRE) Staphylocoques (GISA, hGISA, VRSA) Résistance aux glycopeptides.")
38
Spectre du linézolide Aérobies à Gram positif
Staphylococcus aureus Staphylococcus coagulase négative Streptococcus pneumoniae Streptococcus pyogenes Streptococcus agalactiae Streptocoques du groupe C et G Enterococcus faecalis Enterococcus faecium Anaérobies à Gram positif Clostridium perfringens Peptostreptococcus sp Peptostreptococcus anaerobius .

39
Indications du linézolide
Traitement des pneumonies nosocomiales Traitement des Infections compliquées de la peau et des tissus mous

40
Posologie et durée de traitement
Durée maximale de traitement : 28 jours Aucun ajustement de dose nécessaire lors du relais entre voie IV et voie orale Posologie (IV ou per os) Durée du traitement Pneumonies nosocomiales 600 mg x 2/J 10-14 jours consécutifs Infections compliquées de la peau et des tissus mous .
 Durée du traitement. Pneumonies nosocomiales. 600 mg x 2/J jours consécutifs. Infections compliquées de la peau et des tissus mous. .")
41
Tygacil : 1ère Glycylcycline
Les glycylcyclines : dérivés semi-synthétiques des tétracyclines La tigécycline est un dérivé de la minocycline avec un groupe t-butylglycylamide en position C9 Cette spécificité lui permet de rester stable vis-à-vis des mécanismes de résistance aux tétracyclines Groupe t-butylglycylamide ) N ( C H 3 2 O H3C 9 8 7 Testa RT et al In vitro and in vivo antibacterial activities of the glycylcyclines, a new class of semisynthetic tetracyclines Antimicrob Agents Chemother 1993 ; 37 : Garrisson MW et al. Tigecycline: an investigational glycylcycline antimicrobial with activity against resistant gram-positive organisms. Clin Ther 2005 ; 27 :
 N. ( C. H O. H3C Testa RT et al In vitro and in vivo antibacterial activities of the glycylcyclines, a new class of semisynthetic tetracyclines Antimicrob Agents Chemother 1993 ; 37 : Garrisson MW et al. Tigecycline: an investigational glycylcycline antimicrobial with activity against resistant gram-positive organisms. Clin Ther 2005 ; 27 :")
42
Spectre de Tygacil Bactéries à Gram positif
p5, B-D Espèces habituellement sensibles TYGACIL 2004, p6, E-G Bactéries à Gram positif S. aureus E. faecium (SV + RV) E. faecalis (SV + RV) Streptococcus agalactiae Streptococcus anginosus sp. Streptococcus pyogenes Bactéries à Gram négatif E. coli Klebsiella sp Citrobacter sp Enterobacter cloacae Enterobacter aerogenes Serratia marcescens TYGACIL 2004, p7, H Tigecycline has been shown to be active against a wide variety of pathogens.1 Specifically, tigecycline has broad-spectrum in vitro activity against the following organisms (note that some of the organisms listed below have not been included on the slide): Gram-positive Bacteria: S. aureus, S. epidermidis, E. faecalis, E. faecium, E. avium, E. casseliflavus, E. gallinarum, S. agalactiae, S. anginosus group, and S. pyogenes Gram-negative Bacteria: C. freundii, E. cloacae, E. aerogenes, E. coli, K. oxytoca, K. pneumoniae, and Stenotrophomonas maltophilia Anaerobes: B. fragilis, B. thetaiotaomicron, B. uniformis, B. vulgatus, B. distasonis, B. ovatus, C. perfringens, P. micros, Prevotella spp. Although this list is not all inclusive, it shows the broad spectrum of activity against pathogens that is displayed by tigecycline. Reference 1. Tygacil* package insert. Philadelphia, PA: Wyeth Pharmaceuticals; 2005. *trademark TYGACIL 2004, p5, B-D TYGACIL 2004, p6, E-G TYGACIL 2004, p7, H RCP Tygacil TYGACIL 2004 p9, Y
 E. faecalis (SV + RV) Streptococcus agalactiae. Streptococcus anginosus sp. Streptococcus pyogenes. Bactéries à Gram négatif. E. coli. Klebsiella sp. Citrobacter sp. Enterobacter cloacae. Enterobacter aerogenes. Serratia marcescens. TYGACIL 2004, p7, H. Tigecycline has been shown to be active against a wide variety of pathogens.1 Specifically, tigecycline has broad-spectrum in vitro activity against the following organisms (note that some of the organisms listed below have not been included on the slide): Gram-positive Bacteria: S. aureus, S. epidermidis, E. faecalis, E. faecium, E. avium, E. casseliflavus, E. gallinarum, S. agalactiae, S. anginosus group, and S. pyogenes. Gram-negative Bacteria: C. freundii, E. cloacae, E. aerogenes, E. coli, K. oxytoca, K. pneumoniae, and Stenotrophomonas maltophilia. Anaerobes: B. fragilis, B. thetaiotaomicron, B. uniformis, B. vulgatus, B. distasonis, B. ovatus, C. perfringens, P. micros, Prevotella spp. Although this list is not all inclusive, it shows the broad spectrum of activity against pathogens that is displayed by tigecycline. Reference. 1. Tygacil* package insert. Philadelphia, PA: Wyeth Pharmaceuticals; *trademark. TYGACIL 2004, p5, B-D. TYGACIL 2004, p6, E-G. TYGACIL 2004, p7, H. RCP Tygacil. TYGACIL p9, Y.")
43
Espèces habituellement Espèces inconstamment
Spectre de Tygacil TYGACIL 2004, p5, B-D Espèces habituellement sensibles : Anaérobies B. fragilis sp Prevotella sp Peptostreptococcus sp C. perfringens Espèces inconstamment sensibles : Acinetobacter baumannii Burkholderia cepacia Morganella morganii Proteus sp Providencia sp Stenotrophomonas maltophilia TYGACIL 2004, p6, E-G TYGACIL 2004, p7, H Tigecycline has been shown to be active against a wide variety of pathogens.1 Specifically, tigecycline has broad-spectrum in vitro activity against the following organisms (note that some of the organisms listed below have not been included on the slide): Gram-positive Bacteria: S. aureus, S. epidermidis, E. faecalis, E. faecium, E. avium, E. casseliflavus, E. gallinarum, S. agalactiae, S. anginosus group, and S. pyogenes Gram-negative Bacteria: C. freundii, E. cloacae, E. aerogenes, E. coli, K. oxytoca, K. pneumoniae, and Stenotrophomonas maltophilia Anaerobes: B. fragilis, B. thetaiotaomicron, B. uniformis, B. vulgatus, B. distasonis, B. ovatus, C. perfringens, P. micros, Prevotella spp. Although this list is not all inclusive, it shows the broad spectrum of activity against pathogens that is displayed by tigecycline. Reference 1. Tygacil* package insert. Philadelphia, PA: Wyeth Pharmaceuticals; 2005. *trademark TYGACIL 2004, p5, B-D TYGACIL 2004, p6, E-G Espèce naturellement résistante : Pseudomonas aeruginosa TYGACIL 2004, p7, H RCP Tygacil TYGACIL 2004 p9, Y
: Gram-positive Bacteria: S. aureus, S. epidermidis, E. faecalis, E. faecium, E. avium, E. casseliflavus, E. gallinarum, S. agalactiae, S. anginosus group, and S. pyogenes. Gram-negative Bacteria: C. freundii, E. cloacae, E. aerogenes, E. coli, K. oxytoca, K. pneumoniae, and Stenotrophomonas maltophilia. Anaerobes: B. fragilis, B. thetaiotaomicron, B. uniformis, B. vulgatus, B. distasonis, B. ovatus, C. perfringens, P. micros, Prevotella spp. Although this list is not all inclusive, it shows the broad spectrum of activity against pathogens that is displayed by tigecycline. Reference. 1. Tygacil* package insert. Philadelphia, PA: Wyeth Pharmaceuticals; *trademark. TYGACIL 2004, p5, B-D. TYGACIL 2004, p6, E-G. Espèce naturellement résistante : Pseudomonas aeruginosa. TYGACIL 2004, p7, H. RCP Tygacil. TYGACIL p9, Y.")
44
Activité in vitro contre les pathogènes résistants
S. aureus résistant à la méticilline (SARM) Enterococcus résistant à la vancomycine (ERV) E. faecium E. faecalis Acinetobacter baumannii (inconstamment sensible) La tigécycline n’est pas affectée par les BLSE produites par les entérobactéries TYGACIL 2004, p5, B TYGACIL 2004, p6, F TYGACIL 2005, p5, B TYGACIL 2005, p6, F
 Enterococcus résistant à la vancomycine (ERV) E. faecium. E. faecalis. Acinetobacter baumannii (inconstamment sensible) La tigécycline n’est pas affectée par les BLSE produites par les entérobactéries. TYGACIL 2004, p5, B. TYGACIL 2004, p6, F. TYGACIL 2005, p5, B. TYGACIL 2005, p6, F.")
45
Indications thérapeutiques
Tygacil est indiqué dans : Les infections compliquées de la peau et des tissus mous Les infections intra-abdominales compliquées En développement dans : Les pneumonies communautaires et nosocomiales

46
Les antibiotiques des prochaines années
Ceftobiprole ( Zeftra ® ) Ceftaroline Lipoglycopeptides : Dalbavancine, Télavancine, oritavancine Garénoxacine , Sitafloxacine, Iclaprime Témocilline Ramoplanine
 Ceftaroline. Lipoglycopeptides : Dalbavancine, Télavancine, oritavancine. Garénoxacine , Sitafloxacine, Iclaprime. Témocilline. Ramoplanine.")
47
Antibiothérapie des entérocoques

48
1ers à avoir acquis une résistance plasmidique acquise aux GP
Les entérocoques Naturellement sensibles aux glycopeptides CMI modale à la vancomycine : 1 mg/L CMI modale de la teicoplanine : 0,5 mg/L Sauf E. gallinarum, E. casseliflavus, E. flavescens (< 3% des entérocoques isolés) Résistance naturelle de bas niveau à la vancomycine (CMI 2-32 mg/L) avec une sensibilité conservée à la teicoplanine (phénotype VanC) 1ers à avoir acquis une résistance plasmidique acquise aux GP Résistance aux glycopeptides
 Résistance naturelle de bas niveau à la vancomycine (CMI 2-32 mg/L) avec une sensibilité conservée à la teicoplanine (phénotype VanC) 1ers à avoir acquis une résistance plasmidique acquise aux GP. Résistance aux glycopeptides.")
49
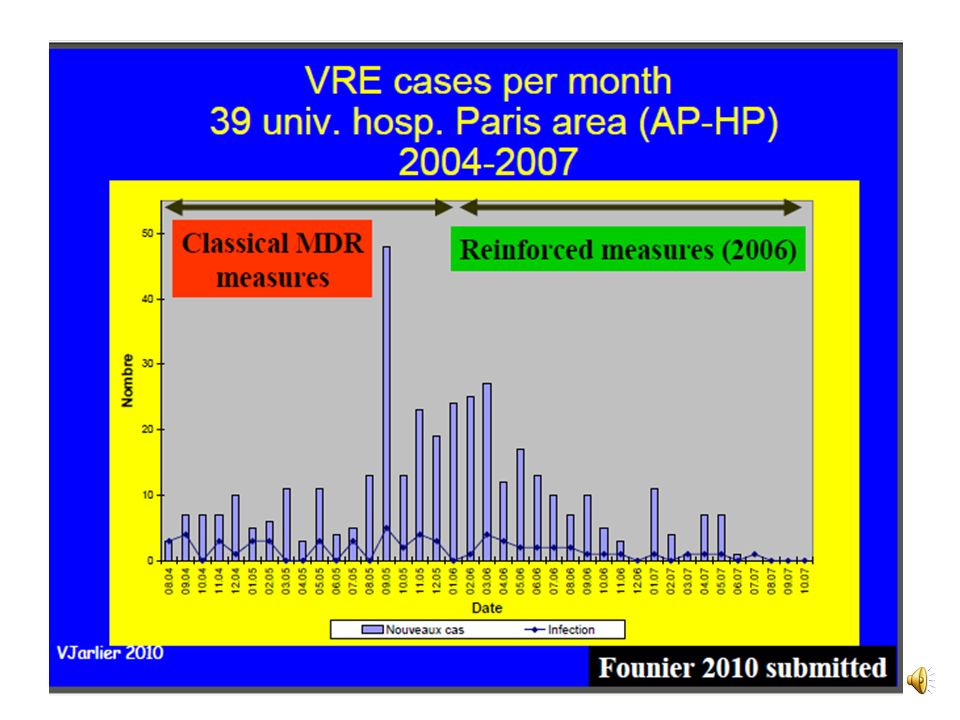
Apparition des VRE : Rôle de la pression de sélection antibiotique
Etats-Unis Sélection par surconsommation de vancomycine par voie orale Epidémies liées à la diffusion de souches clonales au sein d’un hôpital ou entre hôpitaux. Portage extra-hospitalier faible. Europe Rôle de la chaîne alimentaire ? Isolement de E. faecium VanA chez le bétail au Royaume-Uni, en Allemagne et au Danemark Rôle de l’avoparcine utilisé comme facteur de croissance chez les animaux en Europe (interdit depuis 1997) ? Portage dans la population communautaire (discuté) E.U Europe Isolement d’entérocoques VanA d’excréments de cochons et poulet élevés dans des fermes utilisant l’avoparcine alors que les entérocoques isolés dans des fermes n’utilisant pas l’avoparcine sont sensibles aux GP Résistance aux glycopeptides
 Portage dans la population communautaire (discuté) E.U. Europe. Isolement d’entérocoques VanA d’excréments de cochons et poulet élevés dans des fermes utilisant l’avoparcine alors que les entérocoques isolés dans des fermes n’utilisant pas l’avoparcine sont sensibles aux GP. Résistance aux glycopeptides.")
53
Infections à entérocoque
E. faecalis (80-90 %) et E.faecium (5 -10 % ) dominent la pathologie humaine. Infections urinaires communautaires ( 5%) Infections urinaires nosocomiales ( 15 % ) Endocardites ( 10 % ) Infections abdominopelviennes Infections de la peau et parties molles
 et E.faecium (5 -10 % ) dominent la pathologie humaine. Infections urinaires communautaires ( 5%) Infections urinaires nosocomiales ( 15 % ) Endocardites ( 10 % ) Infections abdominopelviennes. Infections de la peau et parties molles.")
54
Infections à entérocoque
Resistance intrinsèque Céphalosporines Vancomycin Aminosides ( bas niveau ) Lincosamides ( bas niveau) Streptogramines Cotrimoxazole ( in vivo seulement ) Résistance acquise Aminopénicillines Gylocopéptides Aminosides ( haut niveau surtout E faecium) Macrolides, lincosamides Streptogramines Chloramphenicol Rifampicine Cyclines Cotrimoxazole Oxazolidinones
 Lincosamides ( bas niveau) Streptogramines. Cotrimoxazole ( in vivo seulement ) Résistance acquise. Aminopénicillines. Gylocopéptides. Aminosides ( haut niveau surtout E faecium) Macrolides, lincosamides. Streptogramines. Chloramphenicol. Rifampicine. Cyclines. Cotrimoxazole. Oxazolidinones.")
55
Traitement des Infections à entérocoques
Première intention Amoxicilline ( 200 mg /kg/j) ou Pénicilline G + Genatmicine (3mg/kg/j) ou nétilmicine Vancomycine (30 mg/kg/j) ou Teicoplanine (12 mg/kg/j) + Streptomycine (1 mg /kg/j) IV ou IM
 ou Pénicilline G. + Genatmicine (3mg/kg/j) ou nétilmicine. Vancomycine (30 mg/kg/j) ou Teicoplanine (12 mg/kg/j) + Streptomycine (1 mg /kg/j) IV ou IM")
56
Conséquences de la résistance bactérienne aux antibiotiques
Acte individuel prescription « criminel » Individuelles Risque accru de décès ? Mauvaise gouvernance Collectives coût accru des soins ?

57
Impact de la résistance sur la mortalité
Pseudomonas aeruginosa, analyse multivariée E. coli & K. pneumoniae à BLSE , analyse multivariée Resistance initiale RR (95% CI) P Emergence de resistance DC 1.3 (0.6–2.8) .52 3.0 (1.2–7.8) .02 Durée de séjour 1.0 (0.9–1.2) .71 1.7 (1.3–2.3) <.001 Coût par jour 1.0 (1.0–1.4) .41 1.1 (0.9–1.3) .43 Carmeli Y, et al. Arch Intern Med 1999; 159:1127–32. Cas (n = 33) Controles (n = 66) OR/RR (95% CI) P DC % 15 9 1.91 (0.49–7.42) .35 Durée de séjour, mediane 11 7 1.73 (1.14–2.65) .01 Coût, mediane US$ 66,590 22,231 1.71 (1.01–2.88) .04 Lautenbach E, et al. Clin Infect Dis 2001; 32:1162–71.
 P. Emergence de resistance. DC. 1.3 (0.6–2.8) (1.2–7.8) .02. Durée de séjour. 1.0 (0.9–1.2) (1.3–2.3) <.001. Coût par jour. 1.0 (1.0–1.4) (0.9–1.3) .43. Carmeli Y, et al. Arch Intern Med 1999; 159:1127–32. Cas. (n = 33) Controles. (n = 66) OR/RR (95% CI) P. DC % (0.49–7.42) .35. Durée de séjour, mediane (1.14–2.65) .01. Coût, mediane US$ 66, , (1.01–2.88) .04. Lautenbach E, et al. Clin Infect Dis 2001; 32:1162–71.")
58
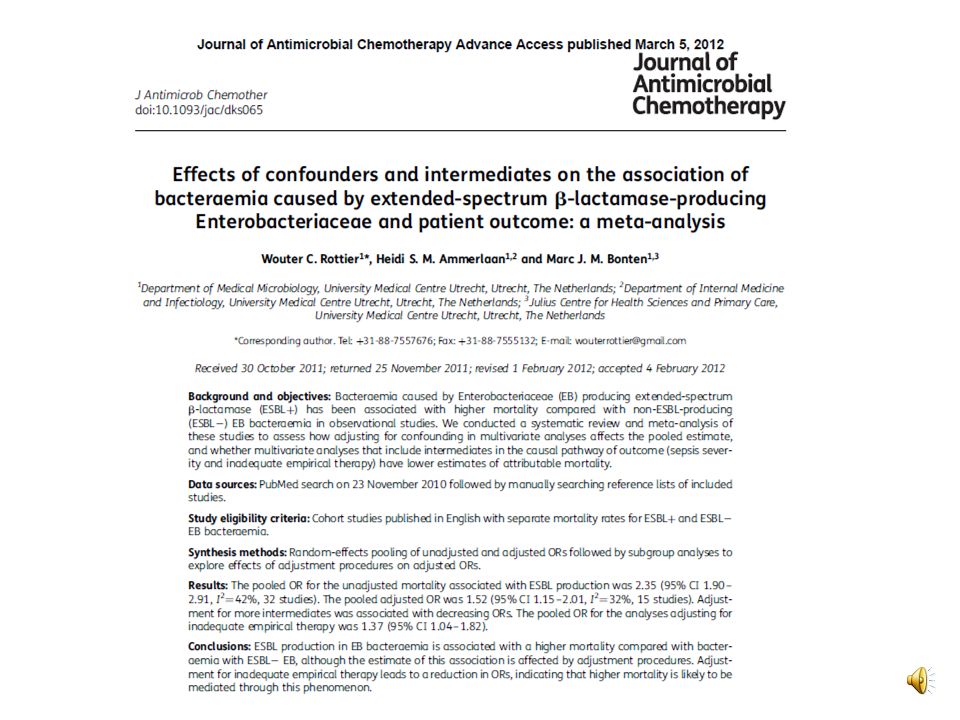
Meta-analysis of mortality in ESBL-producing versus non-ESBL-producing Enterobacteriaceae bacteraemia. Meta-analysis of mortality in ESBL-producing versus non-ESBL-producing Enterobacteriaceae bacteraemia. Forest plot summary of the unadjusted results of the 16 studies included in the meta-analysis. The relative risk (RR) and 95% confidence intervals (CIs) are shown for each study. The pooled RR, represented by the diamond at the bottom of the figure, is 1.85 (95% CI 1.39–2.47, P < 0.001). There was significant heterogeneity among the study results (P = 0.001). Schwaber M J , Carmeli Y J. Antimicrob. Chemother. 2007;60: © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please
 and 95% confidence intervals (CIs) are shown for each study. The pooled RR, represented by the diamond at the bottom of the figure, is 1.85 (95% CI 1.39–2.47, P < 0.001). There was significant heterogeneity among the study results (P = 0.001). Schwaber M J , Carmeli Y J. Antimicrob. Chemother. 2007;60: © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please")
60
Meta-analysis of aORs. Meta-analysis of aORs. The aORs for the effect of ESBL production on mortality reported in each study were pooled. For studies reporting ESBL as not significantly associated with mortality on multivariate analysis, and not presenting an OR, an OR of 1 was imputed with the standard error copied from the unadjusted analysis. ORs >1 indicate a higher mortality in the ESBL+ group. Rottier W C et al. J. Antimicrob. Chemother. 2012;jac.dks065 © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please

63
(a) Comparison of the number of ciprofloxacin trade names for oral use (thick line) and the median price per DDD registered monthly in PHC in Denmark (thin line), and the influence of the introduction of generics. (a) Comparison of the number of ciprofloxacin trade names for oral use (thick line) and the median price per DDD registered monthly in PHC in Denmark (thin line), and the influence of the introduction of generics. The arrow marks the time of introduction of generic versions of ciprofloxacin. (b) The influence of removal of 50% reimbursement and of the introduction of generics on the total use of ciprofloxacin and median price per DDD registered monthly in PHC in Denmark (thin line). Consumption (thick line) is expressed in terms of DDDs per 1000 inhabitants per day. The arrows mark the times of removal of reimbursement of ciprofloxacin and the introduction of generic versions, respectively. 100 DDK≈13 EUR. Jensen U S et al. J. Antimicrob. Chemother. 2010;65: © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please
 Comparison of the number of ciprofloxacin trade names for oral use (thick line) and the median price per DDD registered monthly in PHC in Denmark (thin line), and the influence of the introduction of generics. The arrow marks the time of introduction of generic versions of ciprofloxacin. (b) The influence of removal of 50% reimbursement and of the introduction of generics on the total use of ciprofloxacin and median price per DDD registered monthly in PHC in Denmark (thin line). Consumption (thick line) is expressed in terms of DDDs per 1000 inhabitants per day. The arrows mark the times of removal of reimbursement of ciprofloxacin and the introduction of generic versions, respectively. 100 DDK≈13 EUR. Jensen U S et al. J. Antimicrob. Chemother. 2010;65: © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please")
64
Trends in the frequency of ciprofloxacin resistance among E
Trends in the frequency of ciprofloxacin resistance among E. coli urine isolates from PHC with 95% confidence intervals (thin line) and the consumption of ciprofloxacin by PHC patients from 1995 to 2005 in three to seven Danish counties (thick line) seen in the light of the removal of 50% reimbursement and the introduction of generics. Trends in the frequency of ciprofloxacin resistance among E. coli urine isolates from PHC with 95% confidence intervals (thin line) and the consumption of ciprofloxacin by PHC patients from 1995 to 2005 in three to seven Danish counties (thick line) seen in the light of the removal of 50% reimbursement and the introduction of generics. Consumption is expressed in terms of DDDs per 1000 inhabitants per day. The arrows mark the times of removal of reimbursement of ciprofloxacin and the introduction of generic versions, respectively. Jensen U S et al. J. Antimicrob. Chemother. 2010;65: © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please
 and the consumption of ciprofloxacin by PHC patients from 1995 to 2005 in three to seven Danish counties (thick line) seen in the light of the removal of 50% reimbursement and the introduction of generics. Trends in the frequency of ciprofloxacin resistance among E. coli urine isolates from PHC with 95% confidence intervals (thin line) and the consumption of ciprofloxacin by PHC patients from 1995 to 2005 in three to seven Danish counties (thick line) seen in the light of the removal of 50% reimbursement and the introduction of generics. Consumption is expressed in terms of DDDs per 1000 inhabitants per day. The arrows mark the times of removal of reimbursement of ciprofloxacin and the introduction of generic versions, respectively. Jensen U S et al. J. Antimicrob. Chemother. 2010;65: © The Author Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please")
65
Facteurs intervenants dans la prescription antibiotique
Mauvais diagnostic Méconnaissance des recommandations Promotion et éducation par l’industrie pharmaceutique + Méconnaissance des pathologies et des conséquences écologiques lors de l’utilisation des antibiotiques Sévérité perçue de la maladie + Bonne gouvernance Prescription Demande du patient Éducation de la population Régulation des remboursements Régulation de la promotion à la population - Éducation médicale Tests de diagnostic rapide Facilitation à l’accès des recommandations Régulation de la promotion par l’industrie pharmaceutique - Monnet D CMI 2001

Présentations similaires