Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Dépistage, Populations à risque, Obésité et diabète
Joëlle ARRIVIE, Septembre 2009

2
Mais de qui parle-t’on?

3
A 44-year-old woman desires weight reduction
A 44-year-old woman desires weight reduction. Her history is notable for hypertension, snoring, daytime somnolence, and osteoarthritis. Her father was obese and had type 2 diabetes. On physical examination, her weight is 215 lb (98 kg), her body-mass index (MI) (the weight in kilograms divided by the square of the height in meters) 32.7, her waist circumference 40 in. (102 cm), and her blood pressure 140/92 mn Hg.The stigmata of Cushing’s syndrome are not present. The fasting glucose level is 112 mg per deciliter (6.2 mmol per liter). The fasting cholesterol level is 205 mg per deciliter (5.3 mmol per liter), triglyceride level 224 mg per deciliter (2.5 mmol per liter), highdensity lipoprotein (HDL) cholesterol level 40 mg per deciliter (1.0 mmol per liter), and low-density lipoprotein (LDL) cholesterol level 120 mg per deciliter (3.1 mmol per liter). The thyrotropin level is normal. What would you advise?
, her body-mass index (MI) (the weight in kilograms divided by the square of the height in meters) 32.7, her waist circumference 40 in. (102 cm), and her blood pressure 140/92 mn Hg.The stigmata of Cushing’s syndrome are not present. The fasting glucose level is 112 mg per deciliter (6.2 mmol per liter). The fasting cholesterol level is 205 mg per deciliter (5.3 mmol per liter), triglyceride level 224 mg per deciliter (2.5 mmol per liter), highdensity lipoprotein (HDL) cholesterol level 40 mg per deciliter (1.0 mmol per liter), and low-density lipoprotein (LDL) cholesterol level 120 mg per deciliter (3.1 mmol per liter). The thyrotropin level is normal. What would you advise")
4
Évolution de l’IMC des Français entre 1997 et 2006 selon l’étude ObÉpi
Maigreur (IMC < 18,5 kg/m2) 5 % 4,9 % Poids de référence 58,3 % 53,5 % Surpoids (25 < IMC < 30) 28,5 % 29,2 % Obésité non massive (30 < IMC < 39,9) 7,9 % 11,6 % Obésité massive (IMC > 40) 0,3 % 0,8 % Basdevant A et coll. 4e enquête épidémiologique nationale ObÉpi-Roche rendue publique le 19 sept
 5 % 4,9 % Poids de référence. 58,3 % 53,5 % Surpoids. (25 < IMC < 30) 28,5 % 29,2 % Obésité non massive. (30 < IMC < 39,9) 7,9 % 11,6 % Obésité massive. (IMC > 40) 0,3 % 0,8 % Basdevant A et coll. 4e enquête épidémiologique nationale ObÉpi-Roche rendue publique le 19 sept")
5
Un motif de consultation commun mais une situation complexe …

6
L’adipocyte est une cellule endocrine:

7
Dyslipidémie athérogène
Syndrome métabolique: le socle commun, excès de masse Grasse viscéral et insulino-résistance SYNDROME METABOLIQUE Dyslipidémie athérogène Triglycérides HDL LDL petites, denses INSULINORESISTANCE HYPERGLYCEMIE OBESITE ITG HTA Diabète de type 2 TG / HDL Etat inflammatoire pro-thrombotique PAI-1 Fibrinogène CRP, IL-6, TNF-a Adiponectine Plaque instable Risque d’accident coronaire aigu Despres, JEI, 2006: 29,77

8
Définition du syndrome métabolique NCEP-ATP III
*Diagnosis is established when >3 of these risk factors are present Risk Factor Defining Level Abdominal obesity (Waist circumference) Men >102 cm Women >88 cm TG >150 mg/dL HDL-C <40 mg/dL <50 mg/dL Blood pressure >130 / >85 mm Hg Fasting glucose >110 (>100**) mg/dL Clinical identification of the metabolic syndrome: NCEP-ATP III The NCEP ATP III guidelines define 5 components of the metabolic syndrome; at least 3 of the 5 criteria are required for the diagnosis of the metabolic syndrome. Note that the NCEP metabolic syndrome has different criteria for triglycerides and HDL-C, unlike the WHO definition, which lists high triglycerides and/or low HDL-C as a single factor. Almost all individuals in North America who have the metabolic syndrome have a high waist circumference as one of the criteria. Note also that the NCEP definition of the metabolic syndrome is more liberal than the NCEP major risk factors for blood pressure (140/90 mm Hg) and HDL-C (<40 mg/dl in both men and women) [1]. In 2003, the American Diabetes Association has recommended lowering the limit for impaired fasting glucose from 110 mg/dL to 100 mg/dlL. It seems likely that the NCEP criteria will eventually accept this new criteria for fasting glucose levels [2]. In 2004 a report from the series of workshops sponsored by the NIH, ADA and AHA reported the new ADA IFG criteria in a footnote to a table on the NCEP metabolic syndrome [3]. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus: Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26: ,2003. Grundy SM, Brewer HB, Cleeman JI, Smith SC, Lenfant D, for the Conference Participants. Definition of metabolic syndrome: report of the National, Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109: ** 2003 New ADA IFG criteria (Diabetes Care) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:
 Men. >102 cm. Women. >88 cm. TG. >150 mg/dL. HDL-C. <40 mg/dL. <50 mg/dL. Blood pressure. >130 / >85 mm Hg. Fasting glucose. >110 (>100**) mg/dL. Clinical identification of the metabolic syndrome: NCEP-ATP III. The NCEP ATP III guidelines define 5 components of the metabolic syndrome; at least 3 of the 5 criteria are required for the diagnosis of the metabolic syndrome. Note that the NCEP metabolic syndrome has different criteria for triglycerides and HDL-C, unlike the WHO definition, which lists high triglycerides and/or low HDL-C as a single factor. Almost all individuals in North America who have the metabolic syndrome have a high waist circumference as one of the criteria. Note also that the NCEP definition of the metabolic syndrome is more liberal than the NCEP major risk factors for blood pressure (140/90 mm Hg) and HDL-C (<40 mg/dl in both men and women) [1]. In 2003, the American Diabetes Association has recommended lowering the limit for impaired fasting glucose from 110 mg/dL to 100 mg/dlL. It seems likely that the NCEP criteria will eventually accept this new criteria for fasting glucose levels [2]. In 2004 a report from the series of workshops sponsored by the NIH, ADA and AHA reported the new ADA IFG criteria in a footnote to a table on the NCEP metabolic syndrome [3]. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001;285: The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus: Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26: ,2003. Grundy SM, Brewer HB, Cleeman JI, Smith SC, Lenfant D, for the Conference Participants. Definition of metabolic syndrome: report of the National, Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation. 2004;109: ** 2003 New ADA IFG criteria (Diabetes Care) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA. 2001;285:")
9
Prévalence NHANES III : 24 % chez les H et 23 % chez les F de plus de 20 ans. MONICA (NCEP) 22.5 % des H et 18.5% des F (de ans) DESIR (NCEP) 10 % (16 % + traitement ) des H (de ans) 7% (11) des F (de ans)
 DESIR (NCEP) 10 % (16 % + traitement ) des H (de ans) 7% (11) des F (de ans)")
10
Quels sont les risques?

11
LE SYNDROME METABOLIQUE = UN RISQUE CARDIOVASCULAIRE ACCRU
Ischémie Coronaire Maladies CV Incidence Cumulée % Incidence Cumulée % Syndrome métabolique 10 10 Syndrome métabolique RR : 3.7 RR : 3.5 5 5 Contrôles Contrôles 4 8 12 4 8 12 Années de suivi LAKKA HM, JAMA, 2002, 288:2709 Kuopio Ischaemic Heart Disease Risk Factor Study

12
Hazard Ratio for CVD Mortality, Adjusted for Age and Ethnicity: San Antonio Heart Study
Baseline Status Women Men No DM, No NCEP 1.00 No DM, Yes NCEP 2.07 (0.72–6.00) 1.96 (0.99–3.88) Yes DM, No NCEP 3.53 (0.75–16.7) 2.34 (0.70–7.82) Yes DM, Yes NCEP 8.19 (3.51–19.1) 3.09 (1.49–6.43) Hazard ratio for CVD mortality, adjusted for age and ethnicity: San Antonio Heart Study This slide shows the hazard ratio for cardiovascular disease (CVD) mortality for subjects in the San Antonio Heart Study by presence of diabetes and/or the metabolic syndrome as defined by the NCEP. As expected, the risk for CVD mortality was lowest in subjects without diabetes or the metabolic syndrome. For nondiabetic subjects with the metabolic syndrome, the increased risk for CVD mortality was similar in women (hazard ratio = 2.07) and men (hazard ratio = 1.96). However, in the unusual subjects who had diabetes without the metabolic syndrome, the hazard ratio was considerably higher in women than in men. This is similar to data reported previously from the Framingham Study and other studies. The increased risk for CVD with the addition of the metabolic syndrome to diabetes was particularly prominent in women. Thus, it appears that women are at particularly increased risk of the metabolic syndrome when they also have diabetes. Reference: Hunt KJ, Resendez RG, Williams K, Haffner SM, Stern MP. National Cholesterol Education Program versus World Health Organization metabolic syndrome in relation to all-cause and cardiovascular mortality in the San Antonio Heart Study. Circulation 2004;110: Hunt K et al. Circulation 2004;110:
 1.96 (0.99–3.88) Yes DM, No NCEP (0.75–16.7) 2.34 (0.70–7.82) Yes DM, Yes NCEP (3.51–19.1) 3.09 (1.49–6.43) Hazard ratio for CVD mortality, adjusted for age and ethnicity: San Antonio Heart Study. This slide shows the hazard ratio for cardiovascular disease (CVD) mortality for subjects in the San Antonio Heart Study by presence of diabetes and/or the metabolic syndrome as defined by the NCEP. As expected, the risk for CVD mortality was lowest in subjects without diabetes or the metabolic syndrome. For nondiabetic subjects with the metabolic syndrome, the increased risk for CVD mortality was similar in women (hazard ratio = 2.07) and men (hazard ratio = 1.96). However, in the unusual subjects who had diabetes without the metabolic syndrome, the hazard ratio was considerably higher in women than in men. This is similar to data reported previously from the Framingham Study and other studies. The increased risk for CVD with the addition of the metabolic syndrome to diabetes was particularly prominent in women. Thus, it appears that women are at particularly increased risk of the metabolic syndrome when they also have diabetes. Reference: Hunt KJ, Resendez RG, Williams K, Haffner SM, Stern MP. National Cholesterol Education Program versus World Health Organization metabolic syndrome in relation to all-cause and cardiovascular mortality in the San Antonio Heart Study. Circulation 2004;110: Hunt K et al. Circulation 2004;110:")
13
Incidence du diabète % p<0.0001 P=0.018 p<0.0001 NCEP definition
Incident diabetes after stratification by IGT and the metabolic syndrome This slide examines the risk of the metabolic syndrome (National Cholesterol Education Program [NCEP] definition) as a risk for the development of type 2 diabetes in the San Antonio Heart Study over a 7-year follow-up period. Overall, the metabolic syndrome was associated with a 3.5-fold increased risk for type 2 diabetes. Among subjects with normal glucose tolerance, those with the metabolic syndrome had a 4-fold increased risk for type 2 diabetes. Among subjects with impaired glucose tolerance (IGT), those with the NCEP metabolic syndrome had about a 2.5-fold risk for diabetes. Note that subjects who had both IGT and the NCEP metabolic syndrome had almost a 60% chance of developing type 2 diabetes. For patients in such a high-risk group for type 2 diabetes, the clinician may consider pharmacological interventions as well as behavioral interventions to delay/prevent the onset of type 2 diabetes. Reference: Lorenzo C, Okoloise M, Williams K, Stern MP, Haffner SM. The metabolic syndrome as predictor of type 2 diabetes: the San Antonio Heart Study. Diabetes Care. 2003;26: P=0.018 % p<0.0001 NCEP definition Yes No Yes No IGT Lorenzo C et al. Diabetes Care 2003;26:
 as a risk for the development of type 2 diabetes in the San Antonio Heart Study over a 7-year follow-up period. Overall, the metabolic syndrome was associated with a 3.5-fold increased risk for type 2 diabetes. Among subjects with normal glucose tolerance, those with the metabolic syndrome had a 4-fold increased risk for type 2 diabetes. Among subjects with impaired glucose tolerance (IGT), those with the NCEP metabolic syndrome had about a 2.5-fold risk for diabetes. Note that subjects who had both IGT and the NCEP metabolic syndrome had almost a 60% chance of developing type 2 diabetes. For patients in such a high-risk group for type 2 diabetes, the clinician may consider pharmacological interventions as well as behavioral interventions to delay/prevent the onset of type 2 diabetes. Reference: Lorenzo C, Okoloise M, Williams K, Stern MP, Haffner SM. The metabolic syndrome as predictor of type 2 diabetes: the San Antonio Heart Study. Diabetes Care. 2003;26: P= % p< NCEP definition. Yes. No. Yes. No. IGT. Lorenzo C et al. Diabetes Care 2003;26:")
14
Comment dépister les patients à risque CV en pratique clinique?

15
Relationship between Waist Circumference and Visceral Adipose Tissue Accumulation
Waist Circumference (cm) 120 Visceral Adipose Tissue (cm2) r = 0.80 100 80 60 Relationship between Waist Circumference and Visceral Adipose Tissue Accumulation Nevertheless, waist circumference can be used in clinical practice as a simple correlate of visceral adipose tissue accumulation. However, the shared variance between waist circumference and visceral fat is about 60-70%, which indicates that there is still considerable variation in visceral adipose tissue accumulation for a given waist circumference. This is why a simple clinical index of the presence of metabolic abnormalities of visceral obesity (the simplest metabolic marker being fasting triglyceride concentration) is required in addition to a waist measurement. References: Pouliot MC, Després JP, Lemieux S, et al. Waist circumference and abdominal sagittal diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol. 1994;73: Després JP, Lemieux I, Prud'homme D. Treatment of obesity: need to focus on high risk abdominally obese patients. BMJ. 2001;322: Front Subcutaneous adipose tissue Pouliot MC, et al. Am J Cardiol. 1994;73: ; Després JP, et al. BMJ. 2001;322:
 120. Visceral Adipose Tissue (cm2) r = Relationship between Waist Circumference and Visceral Adipose Tissue Accumulation. Nevertheless, waist circumference can be used in clinical practice as a simple correlate of visceral adipose tissue accumulation. However, the shared variance between waist circumference and visceral fat is about 60-70%, which indicates that there is still considerable variation in visceral adipose tissue accumulation for a given waist circumference. This is why a simple clinical index of the presence of metabolic abnormalities of visceral obesity (the simplest metabolic marker being fasting triglyceride concentration) is required in addition to a waist measurement. References: Pouliot MC, Després JP, Lemieux S, et al. Waist circumference and abdominal sagittal diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol. 1994;73: Després JP, Lemieux I, Prud homme D. Treatment of obesity: need to focus on high risk abdominally obese patients. BMJ. 2001;322: Front. Subcutaneous adipose tissue. Pouliot MC, et al. Am J Cardiol. 1994;73: ; Després JP, et al. BMJ. 2001;322:")
16
INTERHEART: l’obésité abdominale
Le tour de taille : un élément clé pour évaluer le risque cardio-vasculaire Elevated Waist Circumference: A Key Feature in Patients with the Metabolic Syndrome Physicians must detect the presence of abdominal obesity in their practice, and waist circumference should be considered a “vital sign.” Waist circumference must be assessed as an initial step in identifying individuals who are characterized by the clustering abnormalities of the metabolic syndrome. INTERHEART: l’obésité abdominale explique 20 % du risque de faire un IDM Yusuf, lancet, 2004: 364, 937

17
Hypertriglyceridemic waist phenotype:
TG HDL The Definition: Insulin The common form of the metabolic syndrome: High-risk visceral obesity The Core Components Pathophysiology Visceral obesity Insulin resistance The Metabolic Syndrome…Close to a Consensus Furthermore, the American Diabetes Association (ADA)/European Association for the Study of Diabetes (EASD) document questioned the relevance of the metabolic syndrome diagnosis. It was suggested that the metabolic syndrome by itself could not appropriately assess global cardiovascular risk, and this criticism is certainly justified. Whether the metabolic syndrome diagnosis adds to global cardiovascular disease risk assessed by traditional risk factors has not been properly examined in the literature. Furthermore, not all patients with metabolic syndrome are characterized by the same clustering abnormalities, and once a diagnosis is established, traditional risk factors are treated by following guidelines. Whether the presence or absence of the metabolic syndrome will modify the therapeutic pharmacological approaches remains an open question at the moment. AHA: American Heart Association CRP: C-reactive protein CVD: cardiovascular disease HDL: high-density lipoprotein IDF: International Diabetes Federation LDL: low-density lipoprotein NCEP ATP III: National Cholesterol Education Program Adult Treatment Panel III TG: triglycerides Reference: Adapted from Després JP, Lemieux I, Almeras N, Poirer P. Visceral Adipose Tissue and its Contribution to Global Cardiometabolic Risk. Baylor College of Medicine Reports on Cardiometabolic Risk. 2006;1(3):1-10. Small dense LDL CRP Adioponectin Hypertension Diabetes CVD The Clinical Identification: The Core Screening Tools + Hypertriglyceridemic waist Tg>2 mmol/l Waist circumference>90 cm Adapted from Després JP, et al. Baylor College of Medicine Reports on Cardiometabolic Disorders. 2006;1(3):1-10.
/European Association for the Study of Diabetes (EASD) document questioned the relevance of the metabolic syndrome diagnosis. It was suggested that the metabolic syndrome by itself could not appropriately assess global cardiovascular risk, and this criticism is certainly justified. Whether the metabolic syndrome diagnosis adds to global cardiovascular disease risk assessed by traditional risk factors has not been properly examined in the literature. Furthermore, not all patients with metabolic syndrome are characterized by the same clustering abnormalities, and once a diagnosis is established, traditional risk factors are treated by following guidelines. Whether the presence or absence of the metabolic syndrome will modify the therapeutic pharmacological approaches remains an open question at the moment. AHA: American Heart Association. CRP: C-reactive protein. CVD: cardiovascular disease. HDL: high-density lipoprotein. IDF: International Diabetes Federation. LDL: low-density lipoprotein. NCEP ATP III: National Cholesterol Education Program Adult Treatment Panel III. TG: triglycerides. Reference: Adapted from Després JP, Lemieux I, Almeras N, Poirer P. Visceral Adipose Tissue and its Contribution to Global Cardiometabolic Risk. Baylor College of Medicine Reports on Cardiometabolic Risk. 2006;1(3):1-10. Small dense LDL. CRP. Adioponectin. Hypertension. Diabetes. CVD. The Clinical Identification: The Core Screening Tools. + Hypertriglyceridemic waist. Tg>2 mmol/l. Waist circumference>90 cm. Adapted from Després JP, et al. Baylor College of Medicine Reports on. Cardiometabolic Disorders. 2006;1(3):1-10.")
18
Comment dépister les patients à risque de diabète?

19
Dépistage du D2: glycémie à jeun
Un dépistage opportuniste ciblé des sujets de plus de 45 ans ayant (en plus de l’âge) au moins un des marqueurs de risque de diabète suivants : origine non caucasienne et/ou migrant ; marqueurs du syndrome métabolique : excès pondéral mesuré à partir de l’IMC, défini comme > 28 kg/m², hypertension artérielle (pression artérielle systolique > 140 mmHg et/ou pression artérielle diastolique > 90 mmHg et/ou hypertension artérielle traitée) ; HDL-cholestérol < 0,35 g/L (0,9 mmol/L) et/ou triglycérides > 2 g/L (2,3 mmol/L) et/ou dyslipidémie traitée ; antécédents : diabète familial (du premier degré) diabète gestationnel ou enfants de poids de naissance de plus de 4 kg, diabète temporairement induit (consensus d’experts). (HAS, 2003)
 au moins un des marqueurs de risque de diabète suivants : origine non caucasienne et/ou migrant ; marqueurs du syndrome métabolique : excès pondéral mesuré à partir de l’IMC, défini comme > 28 kg/m², hypertension artérielle (pression artérielle systolique > 140 mmHg et/ou pression artérielle diastolique > 90 mmHg et/ou hypertension artérielle traitée) ; HDL-cholestérol < 0,35 g/L (0,9 mmol/L) et/ou triglycérides > 2 g/L (2,3 mmol/L) et/ou dyslipidémie traitée ; antécédents : diabète familial (du premier degré) diabète gestationnel ou enfants de poids de naissance de plus de 4 kg, diabète temporairement induit (consensus d’experts). (HAS, 2003)")
20
La prise en charge hygiéno-diététique est efficace pour diminuer les complications du syndrome métabolique ….ou les bénéfices d’une perte de poids modérée… associée à de l’activité physique Rien de neuf?

21
Syndrome métabolique et risque de diabète
Diabetes Prevention Program (DPP) 3,234 patients with elevated fasting and post-load glucose levels randomized to placebo, metformin (850 mg bid), or lifestyle modification* for 3 years Lifestyle modification reduces the risk of developing DM Placebo Metformin Lifestyle modification 40 30 The Diabetes Prevention Program demonstrated that weight loss and physical activity (averaged to 22 minutes/day) reduced the incidence of diabetes to a greater extent than medication alone. This study, along with the Finish Diabetes Prevention Study, highlight the importance of structured lifestyle modifications in at risk individuals to reduce the risk of developing diabetes. Incidence of DM (%) 20 10 1 2 3 4 Years *Includes 7% weight loss and at least 150 minutes of physical activity per week Knowler WC et al. NEJM 2002;346:
 3,234 patients with elevated fasting and post-load glucose levels randomized to placebo, metformin (850 mg bid), or lifestyle modification* for 3 years. Lifestyle modification reduces the risk of developing DM. Placebo. Metformin. Lifestyle modification The Diabetes Prevention Program demonstrated that weight loss and physical activity (averaged to 22 minutes/day) reduced the incidence of diabetes to a greater extent than medication alone. This study, along with the Finish Diabetes Prevention Study, highlight the importance of structured lifestyle modifications in at risk individuals to reduce the risk of developing diabetes. Incidence of DM (%) Years. *Includes 7% weight loss and at least 150 minutes of physical activity per week. Knowler WC et al. NEJM 2002;346:")
22
Diabetes Prevention Programm (DPP)
Programme du « mode de vie intensif » >7% perte du poids initial et maintien de cette perte Lipides < 25 % >150 minutes par semaine d’activité physique Protocole difficile à appliquer en clinique (16 cs au départ, un coach/patient pendant 24 semaines, suivi: 1 / mois)
")
23
Effets des modifications hygiéno diététiques sur les composantes du syndrome métabolique
Subjects without MetS diagnosis at baseline* Subjects with MetS diagnosis at baseline* ‡ ‡ † † † Effects of intensive lifestyle modification on components of metabolic syndrome (MetS) The intensive lifestyle modification arm of the Diabetes Prevention Program was designed to achieve and maintain a weight reduction of at least 7% through a low-calorie, low-fat diet and to engage in physical activity of moderate intensity, such as brisk walking, for at least 150 minutes per week. The results showed that when compared with the placebo arm, there were benefits for all metabolic syndrome components in subjects with metabolic syndrome at baseline (right) and for all components except low high-density lipoprotein in subjects without metabolic syndrome at baseline (left). Orchard TJ, Temprosa M, Goldberg R, Haffner S, Ratner R, Marcovina S, Fowler S, for the Diabetes Prevention Program Research Group. The effect of metformin and intensive lifestyle intervention on the metabolic syndrome: the Diabetes Prevention Program randomized trial. Ann Intern Med. 2005;142: % Meeting MetS Criteria † † † † *All subjects had an FPG >95 at baseline; †p<0.01; ‡p<0.05 vs. placebo. Waist, waist circumference; HDL, high-density lipoprotein; Trig, triglycerides; FPG, fasting plasma glucose; BP, blood pressure. Orchard TJ, et al. Ann Intern Med. 2005;142:
 The intensive lifestyle modification arm of the Diabetes Prevention Program was designed to achieve and maintain a weight reduction of at least 7% through a low-calorie, low-fat diet and to engage in physical activity of moderate intensity, such as brisk walking, for at least 150 minutes per week. The results showed that when compared with the placebo arm, there were benefits for all metabolic syndrome components in subjects with metabolic syndrome at baseline (right) and for all components except low high-density lipoprotein in subjects without metabolic syndrome at baseline (left). Orchard TJ, Temprosa M, Goldberg R, Haffner S, Ratner R, Marcovina S, Fowler S, for the Diabetes Prevention Program Research Group. The effect of metformin and intensive lifestyle intervention on the metabolic syndrome: the Diabetes Prevention Program randomized trial. Ann Intern Med. 2005;142: % Meeting MetS Criteria. † † † † *All subjects had an FPG >95 at baseline; †p<0.01; ‡p<0.05 vs. placebo. Waist, waist circumference; HDL, high-density lipoprotein; Trig, triglycerides; FPG, fasting plasma glucose; BP, blood pressure. Orchard TJ, et al. Ann Intern Med. 2005;142:")
24
Prévention du diabète Amaigrissement
Les médicaments? Prévention du diabète Amaigrissement

25
Prévention du diabète de type 2: place des interventions pharmacologiques
Essai Journal Description Resultats Finnish Prevention Study (FPS) NEJM / 2001 RHD 58% RR Diabetes Prevention Program (DPP) NEJM / 2002 Metformin 31% RR RHD”Intensives” XENDOS Diabetes Care/ 2004 Orlistat+ RHD 37% RR STOP-NIDDM Lancet / 2002 Acarbose 25% RR TRIPOD Diabetes / 2002 Troglitazone 55% RR DREAM Lancet / 2006 Rosiglitazone 62% RR NEJM / 2006 Ramipril 9% RR (NS) Prevention of type 2 diabetes: Completed trials in impaired glucose tolerance This slide shows a partial listing of intention-to-treat studies examining the effects of both behavioral and pharmacological agents on the incidence of type 2 diabetes in subjects at high-risk for type 2 diabetes (who usually have impaired glucose tolerance [IGT]). In general, lifestyle interventions have been remarkably effective in the prevention of type 2 diabetes averaging a 40-60% treatment effect. In the Diabetes Prevention Program (DPP) study, metformin had a 31% reduction in the risk of type 2 diabetes, and acarbose had a 25% reduction in the risk of type 2 diabetes. Both metformin and acarbose were less than one might expect from the lifestyle intervention. The 3 thiazolidinediones (TZD) trials (DPP, TRIPOD, and DREAM) have shown effects comparable to those seen with lifestyle intervention. However, TZD’s have been reported to have other adverse effects such as weight gain, congestive heart failure, increased fractures, and a possible increase in coronary heart disease. It is clear that the initial choice of therapy for subjects with IGT should be lifestyle intervention. Only in subjects at very high risk of type 2 diabetes, IGT + IFG (slide 34) or IGT + the metabolic syndrome (slide 12) should the addition of a pharmacological agent to lifestyle intervention be considered. DPP = Diabetes Prevention Program TRIPOD = Troglitazone in Prevention of Diabetes DREAM = Diabetes REduction Approaches with ramipril and rosiglitazone Medications References: Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346: Buchanan TA, Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, Ochoa C, Tan S, Berkowitz K, Hodis HN, Azen SP. Preservation of pancreatic beta-cell function and prevention of type 2 diabetes by pharmacological treatment of insulin resistance in high-risk hispanic women. Diabetes 2002;51: Diabetes Prevention Program Research Group. Prevention of type 2 diabetes with troglitazone in the Diabetes Prevention Program. Diabetes 2005;54: The DREAM Trial Investigators. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet 2006;368: DREAM Trial Investigators; Bosch J, Yusuf S, Gerstein HC, Pogue J, Sheridan P, Dagenais G, Diaz R, Avezum A, Lanas F, Probstfield J, Fodor G, Holman RR. Effect of ramipril on the incidence of diabetes. N Engl J Med 2006;355: Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, Keinanen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M, Salminen V, Uusitupa M; Finnish Diabetes Prevention Study Group. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001;344:
 NEJM / RHD. 58% RR. Diabetes Prevention Program (DPP) NEJM / Metformin. 31% RR. RHD Intensives XENDOS. Diabetes Care/ Orlistat+ RHD. 37% RR. STOP-NIDDM. Lancet / Acarbose. 25% RR. TRIPOD. Diabetes / Troglitazone. 55% RR. DREAM. Lancet / Rosiglitazone. 62% RR. NEJM / Ramipril. 9% RR (NS) Prevention of type 2 diabetes: Completed trials in impaired glucose tolerance. This slide shows a partial listing of intention-to-treat studies examining the effects of both behavioral and pharmacological agents on the incidence of type 2 diabetes in subjects at high-risk for type 2 diabetes (who usually have impaired glucose tolerance [IGT]). In general, lifestyle interventions have been remarkably effective in the prevention of type 2 diabetes averaging a 40-60% treatment effect. In the Diabetes Prevention Program (DPP) study, metformin had a 31% reduction in the risk of type 2 diabetes, and acarbose had a 25% reduction in the risk of type 2 diabetes. Both metformin and acarbose were less than one might expect from the lifestyle intervention. The 3 thiazolidinediones (TZD) trials (DPP, TRIPOD, and DREAM) have shown effects comparable to those seen with lifestyle intervention. However, TZD’s have been reported to have other adverse effects such as weight gain, congestive heart failure, increased fractures, and a possible increase in coronary heart disease. It is clear that the initial choice of therapy for subjects with IGT should be lifestyle intervention. Only in subjects at very high risk of type 2 diabetes, IGT + IFG (slide 34) or IGT + the metabolic syndrome (slide 12) should the addition of a pharmacological agent to lifestyle intervention be considered. DPP = Diabetes Prevention Program. TRIPOD = Troglitazone in Prevention of Diabetes. DREAM = Diabetes REduction Approaches with ramipril and rosiglitazone Medications. References: Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med 2002;346: Buchanan TA, Xiang AH, Peters RK, Kjos SL, Marroquin A, Goico J, Ochoa C, Tan S, Berkowitz K, Hodis HN, Azen SP. Preservation of pancreatic beta-cell function and prevention of type 2 diabetes by pharmacological treatment of insulin resistance in high-risk hispanic women. Diabetes 2002;51: Diabetes Prevention Program Research Group. Prevention of type 2 diabetes with troglitazone in the Diabetes Prevention Program. Diabetes 2005;54: The DREAM Trial Investigators. Effect of rosiglitazone on the frequency of diabetes in patients with impaired glucose tolerance or impaired fasting glucose: a randomised controlled trial. Lancet 2006;368: DREAM Trial Investigators; Bosch J, Yusuf S, Gerstein HC, Pogue J, Sheridan P, Dagenais G, Diaz R, Avezum A, Lanas F, Probstfield J, Fodor G, Holman RR. Effect of ramipril on the incidence of diabetes. N Engl J Med 2006;355: Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, Keinanen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M, Salminen V, Uusitupa M; Finnish Diabetes Prevention Study Group. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001;344:")
26
XENDOS: Orlistat associé aux règles hygiéno diététiques
Weight loss with orlistat + lifestyle reduced and maintained weight better than lifestyle alone -3 -6 -9 -12 4-year long randomized control trial of orlistat as an adjunct to lifestyle for the prevention of type 2 diabetes in obese at-risk patients Benefits of medication use can be maintained over long-term period of time. The XENDOS trial was a 4-year long randomized control trial of orlistat as an adjunct to lifestyle for the prevention of type 2 diabetes in at risk population. In this study, a DPP-type intervention was delivered in an effort to prevent type 2 diabetes in at risk population over a 4-year period of time. The intervention alone produced significant weight loss of about 6 kg after 1 year with 3 kg maintained over the 4-year period. The group treated with orlistat plus the behavioral intervention had a mean weight loss of over 10 kg with 5.8 kg maintained over the same period of time. Reference: Torgerson JS, Hauptman J, Boldrin MN, Sjostrom L. XENical in the prevention of diabetes in obese subjects (XENDOS) study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care 2004;27: “DPP-type” Intervention –3.0 kg Placebo + Lifestyle p<0.001 Change in Body Weight (kg) Orlistat + “DPP-type” Intervention–5.8 kg Orlistat + Lifestyle 52 104 156 208 Week Torgerson JS et al. Diabetes Care 2004;27:
 study: a randomized study of orlistat as an adjunct to lifestyle changes for the prevention of type 2 diabetes in obese patients. Diabetes Care 2004;27: DPP-type Intervention –3.0 kg. Placebo + Lifestyle. p< Change in Body Weight (kg) Orlistat + DPP-type Intervention–5.8 kg. Orlistat + Lifestyle Week. Torgerson JS et al. Diabetes Care 2004;27:")
27
Effete de la sibutramine associée aux règles hygiéno diététiques
-2 -4 -6 -8 -10 -12 -14 -16 Sibutramine alone Effects of lifestyle modification and pharmacotherapy are additive This randomized controlled trial by Wadden and colleagues compared the effects of lifestyle modification and sibutramine (15 mg/day) either alone or in combination. There were no differences in weight loss at 1-year weight for participants who received 30 weeks of group-based lifestyle modification alone (6.7 ± 7.9 kg) vs. those who received sibutramine alone (5.0 ± 7.4 kg). Adding brief lifestyle counseling, delivered in eight 10- to 15-minute sessions, to sibutramine resulted in a weight reduction of 7.5 ± 8.0 kg at 1 year. When the 30-week group-based lifestyle modification program was added to sibutramine, however, participants achieved a 1-year weight loss (12.1 ± 9.8 kg) that was nearly double that of either therapy alone. These findings demonstrate that the effects of lifestyle modification and pharmacotherapy are equivalent when used separately, but additive when used in combination. As with behavioral treatment, pharmacological weight loss therapies should be continued long term to facilitate the maintenance of weight loss. In studies of sibutramine and orlistat, significant weight regain has been found upon discontinuation of the drug. Patients should be informed that lack of continued weight loss does not necessarily indicate that the medication has lost its effectiveness, but that the drug is still working to prevent regain. References: Wadden TA, Berkowitz RI, Womble LG, Sarwer DB, Phelan S, Cato RK, Hesson LA, Osei SY, Kaplan R, Stunkard AJ. Randomized trial of lifestyle modification and pharmacotherapy for obesity. N Engl J Med 2005;353: James WPT, Astrup A, Finer N, Hilsted J, Kopelman P, Rössner S, Saris WHM, Van Gaal LF, for the STORM Study Group. Effect of sibutramine on weight maintenance after weight loss: a randomised trial. Lancet 2000;356: Davidson MH, Hauptman J, DiGirolamo M, Foreyt JP, Halsted CH, Heber D, Heimburger DC, Lucas CP, Robbins DC, Chung J, Heymsfield SB. Weight control and risk factor reduction in obese subjects treated for 2 years with orlistat: a randomized controlled trial. JAMA 1999;281: Sjöström L, Rissanen A, Andersen T, Boldrin M, Golay A, Koppeschaar HPF, Krempf M, for the European Multicentre Orlistat Study Group. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. Lancet 1998;352: Lifestyle modificationalone Weight Loss (kg) Sibutramine + brief therapy Combined therapy 3 6 10 18 26 40 52 Weeks Wadden TA et al. N Engl J Med 2005;35:
 either alone or in combination. There were no differences in weight loss at 1-year weight for participants who received 30 weeks of group-based lifestyle modification alone (6.7 ± 7.9 kg) vs. those who received sibutramine alone (5.0 ± 7.4 kg). Adding brief lifestyle counseling, delivered in eight 10- to 15-minute sessions, to sibutramine resulted in a weight reduction of 7.5 ± 8.0 kg at 1 year. When the 30-week group-based lifestyle modification program was added to sibutramine, however, participants achieved a 1-year weight loss (12.1 ± 9.8 kg) that was nearly double that of either therapy alone. These findings demonstrate that the effects of lifestyle modification and pharmacotherapy are equivalent when used separately, but additive when used in combination. As with behavioral treatment, pharmacological weight loss therapies should be continued long term to facilitate the maintenance of weight loss. In studies of sibutramine and orlistat, significant weight regain has been found upon discontinuation of the drug. Patients should be informed that lack of continued weight loss does not necessarily indicate that the medication has lost its effectiveness, but that the drug is still working to prevent regain. References: Wadden TA, Berkowitz RI, Womble LG, Sarwer DB, Phelan S, Cato RK, Hesson LA, Osei SY, Kaplan R, Stunkard AJ. Randomized trial of lifestyle modification and pharmacotherapy for obesity. N Engl J Med 2005;353: James WPT, Astrup A, Finer N, Hilsted J, Kopelman P, Rössner S, Saris WHM, Van Gaal LF, for the STORM Study Group. Effect of sibutramine on weight maintenance after weight loss: a randomised trial. Lancet 2000;356: Davidson MH, Hauptman J, DiGirolamo M, Foreyt JP, Halsted CH, Heber D, Heimburger DC, Lucas CP, Robbins DC, Chung J, Heymsfield SB. Weight control and risk factor reduction in obese subjects treated for 2 years with orlistat: a randomized controlled trial. JAMA 1999;281: Sjöström L, Rissanen A, Andersen T, Boldrin M, Golay A, Koppeschaar HPF, Krempf M, for the European Multicentre Orlistat Study Group. Randomised placebo-controlled trial of orlistat for weight loss and prevention of weight regain in obese patients. Lancet 1998;352: Lifestyle modificationalone. Weight Loss (kg) Sibutramine + brief therapy. Combined therapy Weeks. Wadden TA et al. N Engl J Med 2005;35:")
28
Les espoirs déçus….

29
Effets métaboliques périphériques
Rimonabant : Antagoniste Sélectif des Récepteurs CB1 Effets Centraux et Périphériques CB1 Diminution de l’appétit Réduction de l’apport calorique cerveau Effets centraux Diminution du poids corporel Oxydation des acides gras (muscle, graisse) Rimonabant FFA clairance Effets métaboliques périphériques Restaurateur de la sensibilité à l’insuline Amélioration du métabolisme du glucose métabolisme des lipides - Diminution de l’inflammation CB1 Adipocyte Adiponectine JP Després et al. NEJM 2005, 353,
 Rimonabant. FFA clairance. Effets métaboliques périphériques. Restaurateur de la. sensibilité à l’insuline. Amélioration du. métabolisme du glucose. métabolisme des lipides. - Diminution de l’inflammation. CB1. Adipocyte. Adiponectine. JP Després et al. NEJM 2005, 353,")
30
RIMONABANT

31
IMC > ou 40 IMC > 35 + Co morbidités
La Chirurgie? IMC > ou 40 IMC > 35 + Co morbidités

33
Conduite pratique pour Mme X?

34
Principes du traitement
Complications : NASH, MCV Complications : SAS, arthrose Tabac Defining Global Cardiometabolic Risk The presence of the metabolic syndrome has been shown to increase the relative risk of cardiovascular disease (CVD) by approximately 2-fold. However, increasing the risk of CVD by 2-fold does not necessarily put the patient at high absolute risk of CVD. Physicians have to pay attention to both the traditional risk factors and the metabolic syndrome. More results from prospective studies are needed to address the question of whether the presence of the metabolic syndrome has an impact on the global CVD risk that is assessed solely on the basis of traditional risk factors. Meanwhile, it has been proposed that global cardiometabolic risk is defined as the global CVD risk, resulting from the presence of traditional risk factors, and the features of the metabolic syndrome. Additional prospective studies with measurements of traditional risk factors and various metabolic syndrome features are urgently needed to provide physicians with better risk assessment algorithms. This is particularly important considering the very high prevalence in clinical practice of patients with type 2 diabetes, abdominal obesity, and features of the metabolic syndrome. Hypertension Diabete Obésité abdominale Cholesterol LDL HDL FDR classiques Traiter la cause
 by approximately 2-fold. However, increasing the risk of CVD by 2-fold does not necessarily put the patient at high absolute risk of CVD. Physicians have to pay attention to both the traditional risk factors and the metabolic syndrome. More results from prospective studies are needed to address the question of whether the presence of the metabolic syndrome has an impact on the global CVD risk that is assessed solely on the basis of traditional risk factors. Meanwhile, it has been proposed that global cardiometabolic risk is defined as the global CVD risk, resulting from the presence of traditional risk factors, and the features of the metabolic syndrome. Additional prospective studies with measurements of traditional risk factors and various metabolic syndrome features are urgently needed to provide physicians with better risk assessment algorithms. This is particularly important considering the very high prevalence in clinical practice of patients with type 2 diabetes, abdominal obesity, and features of the metabolic syndrome. Hypertension. Diabete. Obésité abdominale. Cholesterol. LDL. HDL. FDR classiques. Traiter la cause.")
35
Diététique du syndrome métabolique
Obésité: ⇩Calories ⇩Lipides Hypertriglycéridémie et baisse du HDL- < 55% de Glucides ⇩ Fructose, Saccharose ⇧ Fibres Index glycémique bas ⇧ Acides gras mono insaturés McKeown, Diabetes Care February 2004 vol. 27 no

36
Conseils minimaux pour un sujet à risque cardiovasculaire
Poissons: 2 à 3 fois par semaine Éviter la charcuterie, privilégier les viandes maigres Huile d’olive et colza > 2 fruits par jour > 1 plat de légumes par jour > 1 plat de crudités

37
Recommandations des Sociétés Savantes
Exercice aérobie +- intense 50-70 % de la FMT 30 minutes par jour échauffement récupération 5-10 min endurance Conseils pour limiter l’activité: se déplacer à pied, escalier, jardin

38
Comment initier puis maintenir dans le temps les règles hygiéno diététiques?

39
Rôle de l’éducation thérapeutique?
Prise en charge en équipe multidisciplinaire (médecin, IDE, diététique, kinésithérapeute, psychologue) Éducation thérapeutique: En groupe ou individuel Centré sur: Identification des facteurs de risques, Reconnaître les matières grasses, Analyser son comportement alimentaire Mettre en place une activité physique à son niveau Suivi rapproché
 Éducation thérapeutique: En groupe ou individuel. Centré sur: Identification des facteurs de risques, Reconnaître les matières grasses, Analyser son comportement alimentaire. Mettre en place une activité physique à son niveau. Suivi rapproché.")
40
Aide à la motivation….mais aussi aide à l’action!
Partenariat avec des associations d’activités physiques adaptées ! Adams et White, Br J Sports Med 2003;37,106 Brug J Behav NutrAct. 2005;2,2

43
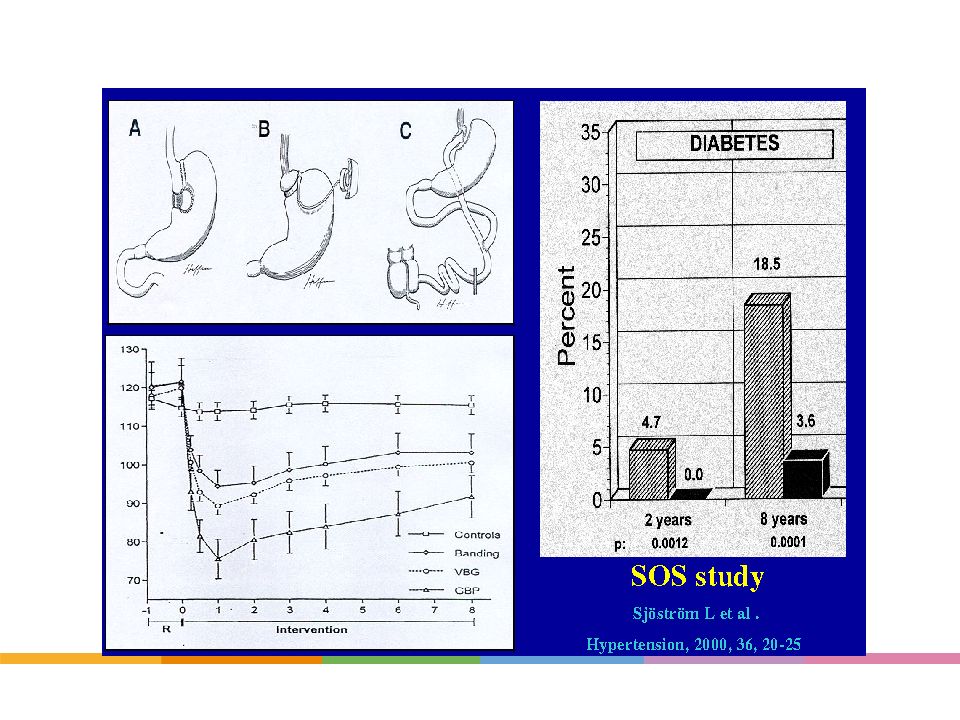
Effect of Bariatric Surgery on Obesity-related Metabolic Complications
Control Surgery 72 62 46 Ratio of Recovery (% of subjects) Effect of bariatric surgery on obesity-related metabolic complications The improvement in diabetes was significant at 10 years when compared to a matched cohort group in the Swedish Obese Subjects (SOS) trial.1 There were also significant improvements in hypertriglyceridemia, hyperuricemia and high molecular weight cholesterol at 10 years. However, the significant improvement in hypertension seen at 2 years was no longer present at 10 years. But in another SOS report, in the 6% of patients who underwent a gastric bypass who had a significantly greater weight loss than purely restrictive procedures, there was a significant improvement in both systolic and diastolic blood pressure at eight years.2 References: Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Eng J Med. 2004;351: Sjöström CD, Peltonen M, Sjöström L. Blood pressure and pulse pressure during long-term weight loss in the obese: the Swedish Obese Subjects (SOS) Intervention Study. Obes Res. 2001;9: 36 34 24 21 21 19 22 13 11 Diabetes Hypertension Hypertriglyceridemia Sjöström: N Engl J Med 2004;351:2683. 43
 Effect of bariatric surgery on obesity-related metabolic complications The improvement in diabetes was significant at 10 years when compared to a matched cohort group in the Swedish Obese Subjects (SOS) trial.1 There were also significant improvements in hypertriglyceridemia, hyperuricemia and high molecular weight cholesterol at 10 years. However, the significant improvement in hypertension seen at 2 years was no longer present at 10 years. But in another SOS report, in the 6% of patients who underwent a gastric bypass who had a significantly greater weight loss than purely restrictive procedures, there was a significant improvement in both systolic and diastolic blood pressure at eight years.2 References: Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Eng J Med. 2004;351: Sjöström CD, Peltonen M, Sjöström L. Blood pressure and pulse pressure during long-term weight loss in the obese: the Swedish Obese Subjects (SOS) Intervention Study. Obes Res. 2001;9: Diabetes. Hypertension. Hypertriglyceridemia. Sjöström: N Engl J Med 2004;351:")
44
Syndrome métabolique et risque de diabète
Finnish Diabetes Prevention Study 522 overweight (mean BMI=31 kg/m2) patients with impaired fasting glucose† randomized to intervention‡ or usual care for 3 years Lifestyle modification reduces the risk of developing DM Intervention Control 23% Patients with the metabolic syndrome can decrease their risk of developing diabetes with a program targeted at weight loss, reduced calorie intake, reduced saturated fat, and increased physical activity (30 minutes/day). 11% % with Diabetes Mellitus †Defined as a glucose >140 mg/dl 2 hours after an oral glucose challenge ‡Aimed at reducing weight (>5%), total intake of fat (<30% total calories) and saturated fat (<10% total calories); increasing uptake of fiber (>15 g/1000 cal); and physical activity (moderate at least 30 min/day) Tuomilehto J et al. NEJM 2001;344:
 patients with impaired fasting glucose† randomized to intervention‡ or usual care for 3 years. Lifestyle modification reduces the risk of developing DM. Intervention. Control. 23% Patients with the metabolic syndrome can decrease their risk of developing diabetes with a program targeted at weight loss, reduced calorie intake, reduced saturated fat, and increased physical activity (30 minutes/day). 11% % with Diabetes Mellitus. †Defined as a glucose >140 mg/dl 2 hours after an oral glucose challenge. ‡Aimed at reducing weight (>5%), total intake of fat (<30% total calories) and saturated fat (<10% total calories); increasing uptake of fiber (>15 g/1000 cal); and physical activity (moderate at least 30 min/day) Tuomilehto J et al. NEJM 2001;344:")
Présentations similaires





![[number 1-100].](/1/172887/big_thumb.jpg "[number 1-100].>")














