Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Diabète de T2 et Hypertension : prise en charge du risque CV
Pr Nacer Chraibi Cardiologue

3
Plan Pourquoi le diabétique hypertendu mérite une attention spéciale ;
Comment améliorer le pronostic CV ? Quelles prise en charge thérapeutique ?

4
Pourquoi traiter ? Pandémie diabétique mondiale ;
Fréquence et gravité des complications cardiovasculaires ; Complexité de la physiopathologie, et donc interventions à cibles multiples ; Efficacité de l'intervention thérapeutique ; Réduction des coûts socio-économiques du suivi du diabétique non compliqué ;

5
New Cases of Diabetes Note Y access in thousands of cases = 2,000,000
5 Diabetes Report Card Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; 2012.

7
+ AVC x2-3 Syndromes Coronariens Insuffisance cardiaque Hx10 Fx15 + HVG x2-3

8
Chez le diabétique hypertendu, une augmentation de la PAS ou de la PAD de 5 mmHg augmente le risque cardiovasculaire de 20 à 30 %. Mac Mahon, Lancet 1990 Framingham HTA chez le Diab. 2012 Diabète Seul + HTA Mortalité totale 7 % 30 % Mortalité CV 9 % 25 %

9
HTA et diabète : relations complexes
Facteurs du risque cardiovasculaire : Obésité, (syndome métabolique); tabagisme; dyslipidémie; sédentarité … HTA Diabète Complications cardiovasculaires Complications rénales
; tabagisme; dyslipidémie; sédentarité … HTA. Diabète. Complications. cardiovasculaires. Complications rénales.")
10
physiopathologie

11
Factors Favoring Hypertension in Diabetes
Genetic factors Increased sympathetic tone Endothelial dysfunction associated with hyperglycemia and AGEs, increased free radicals, and altered response to NO Hyperglycemia stimulates intrarenal production of angiotensin II with increased salt and water retention at the proximal tubule

12
Effects of Angiotensin II
Pressor effect Proinflammatory Oxidative stress Salt retention Insulin resistance Through PI3 kinase and downstream Akt pathway Reduction in NO production within endothelium Increases vasoconstriction Increases TGF- production and hepatic fibrosis

13
HTA chez le diabétique, caractéristiques particulières
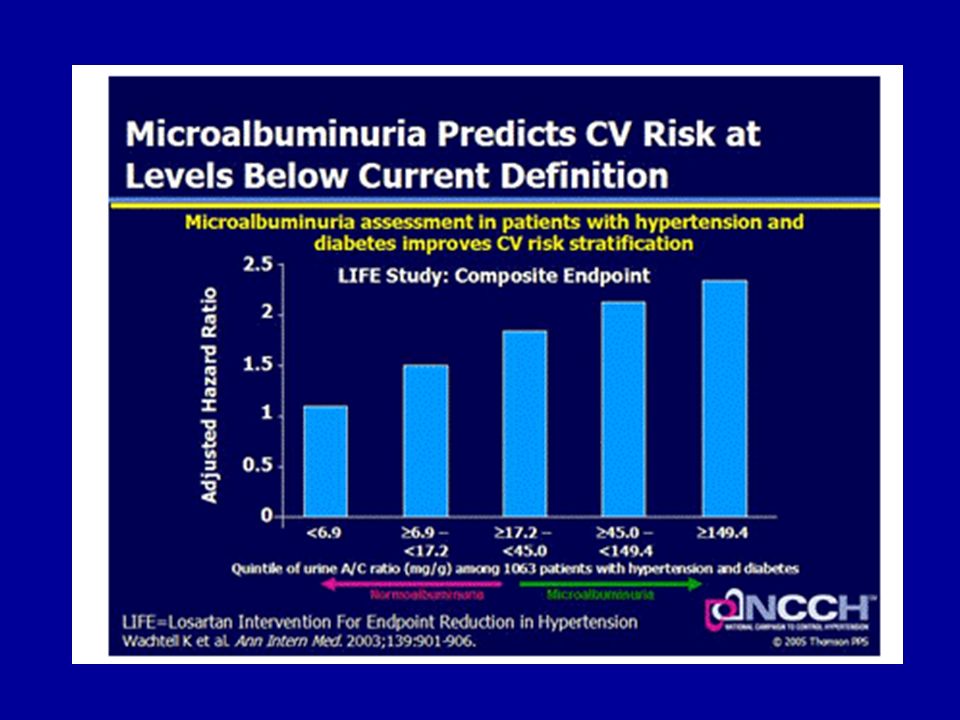
Augmentation de l’incidence de l’HTA systolique Augmentation de la variabilité tensionnelle Hypertension de décubitus et hypotension orthostatique Perte de la chute tensionnelle nocturne : à valeurs de pression diurne identiques, le diabétique a une charge tensionnelle globale plus élevée, et un pronostic plus mauvais; Une prise de médicament le soir est nécessaire L’hypertension est très 昀爀焀甀攀渀琀攀 挀栀攀稀 氀攀猀 瀀愀琀椀攀渀琀猀 搀椀愀戀琀椀焀甀攀猀 攀琀 猀愀 瀀爀 瘀愀氀攀渀挀攀 攀猀琀 攀渀瘀椀爀漀渀 氀攀 搀漀甀戀氀攀 搀攀 挀攀氀氀攀 爀攀渀挀漀渀琀爀攀 挀栀攀稀 氀攀猀 渀 漀渀 搀椀愀戀琀椀焀甀攀猀 ⠀䔀瀀猀琀攀椀渀 攀琀 匀漀眀攀爀猀Ⰰ 㤀㤀㈀⤀⸀ 䐀攀 瀀氀甀猀Ⰰ 氀愀 瀀爀猀攀渀挀攀 搀ᤠ栀礀瀀攀爀琀攀渀猀椀漀渀 愀挀挀爀漀琀 氀攀 爀椀猀焀甀攀 搀樀 攀砀椀猀琀愀渀琀 搀攀 挀漀洀瀀氀椀挀愀琀椀 漀渀猀 挀愀爀搀椀漀瘀愀猀挀甀氀愀椀爀攀猀 愀猀猀漀挀椀 愀甀 搀椀愀戀琀攀 搀攀 琀礀瀀攀 ㈀ ⠀䔀瀀猀琀攀椀渀 攀 琀 匀漀眀攀爀猀Ⰰ 㤀㤀㈀㬀 吀栀攀 䠀礀瀀攀爀琀攀渀猀椀漀渀 椀渀 䐀椀愀戀攀琀攀猀 匀琀甀搀礀 䜀爀漀甀瀀Ⰰ 㤀㤀㌀ 戀⤀⸀ 唀渀攀 琀甀搀攀 搀攀 挀漀栀漀爀琀攀 椀渀挀氀甀愀渀琀 㔀㐀㤀 搀椀愀戀琀椀焀甀攀猀 搀攀 琀礀瀀攀 ㈀ ⠀ 最攀 洀漀礀攀渀 㘀 愀渀猀⤀Ⰰ 愀 洀椀猀 攀渀 瘀椀搀攀渀挀攀 甀渀攀 瀀爀瘀愀氀攀渀挀攀 氀攀瘀攀 搀ᤠ栀礀瀀攀 爀琀攀渀猀椀漀渀Ⰰ 猀甀爀 氀愀 戀愀猀攀 搀ᤠ甀渀攀 瀀爀攀猀猀椀漀渀 愀爀琀爀椀攀氀氀攀 ⠀倀䄀⤀ 洀漀礀攀渀渀攀 攢 㐀 ⼀㤀 洀洀䠀最 瀀攀渀搀愀渀琀 甀渀 猀甀椀瘀椀 搀攀 琀爀漀椀猀 愀渀猀⸀ 㠀 ─ 搀攀猀 瀀愀琀椀攀渀琀猀 漀 渀琀 琀 挀漀渀猀椀搀爀猀 挀漀洀洀攀 栀礀瀀攀爀琀攀渀搀甀猀㨀 氀愀 瀀爀瘀愀氀攀渀挀攀 搀攀 氀ᤠ栀礀瀀攀爀 琀攀渀猀椀漀渀 瘀愀 搀攀 㜀 ─ 挀栀攀稀 氀攀猀 瀀愀琀椀攀渀琀猀 愀礀愀渀琀 甀渀攀 攀砀挀爀琀椀漀渀 搀ᤠ愀氀戀甀 洀椀渀攀 甀爀椀渀愀椀爀攀 渀漀爀洀愀氀攀 ⠀搢 ㌀ 洀最⼀㈀㐀栀⤀ 㤀㌀ ─ 瀀漀甀爀 氀攀猀 瀀愀琀椀攀渀琀猀 愀 瘀攀挀 洀愀挀爀漀愀氀戀甀洀椀渀甀爀椀攀 ⠀攢 ㌀ 洀最⼀㈀㐀栀⤀⸀ 匀攀甀氀猀 㐀 ─ 搀攀猀 瀀愀琀椀攀渀琀猀 漀 渀琀 爀攀甀 甀渀 琀爀愀椀琀攀洀攀渀琀 愀渀琀椀ⴀ栀礀瀀攀爀琀攀渀猀攀甀爀⸀ 䐀攀甀砀 瀀愀琀椀攀渀琀猀 猀甀爀 琀爀 漀椀猀 渀漀渀 琀爀愀椀琀猀 瀀漀甀爀 氀ᤠ栀礀瀀攀爀琀攀渀猀椀漀渀 瀀爀猀攀渀琀愀椀攀渀琀 甀渀攀 栀礀瀀攀爀琀攀 渀猀椀漀渀 猀礀猀琀漀氀椀焀甀攀 椀猀漀氀攀⸀ 䰀愀 瀀爀猀攀渀挀攀 搀ᤠ甀渀攀 洀椀挀爀漀ⴀ愀氀戀甀洀椀渀甀爀椀攀 攀琀, plus encore, d’une macro-albuminurie augmente la probabilité d’observer une HTA chez un DT2 (ref 6). Même parmi les patients traités pour l’hypertension, 92 % de ceux avec normoalbuminurie, 92 % de ceux avec microalbuminurie et 88 % de ceux avec macroalbuminurie correspondaient toujours à la définition d’hypertendus (PA ≥ 140/90 mmHg) avec une PA moyenne de 163/90, 165/88 et 161/92 mmHg dans les trois groupes respectifs. L’hypertension artérielle (HTA) est très fréquente dans le DT2 et apparaît très précocement dans l’histoire du diabète. Diverses enquêtes en France indiquent qu’environ deux DT2 sur trois sont hypertendus. Parmi les hypertendus traités, près de la moitié ont un contrôle tensionnel insuffisant, l’objectif chez le diabétique étant d’amener les chiffres tensionnels à 140/80 mm Hg ou en dessous (réf 7).
. Même parmi les patients traités pour l’hypertension, 92 % de ceux avec normoalbuminurie, 92 % de ceux avec microalbuminurie et 88 % de ceux avec macroalbuminurie correspondaient toujours à la définition d’hypertendus (PA ≥ 140/90 mmHg) avec une PA moyenne de 163/90, 165/88 et 161/92 mmHg dans les trois groupes respectifs. L’hypertension artérielle (HTA) est très fréquente dans le DT2 et apparaît très précocement dans l’histoire du diabète. Diverses enquêtes en France indiquent qu’environ deux DT2 sur trois sont hypertendus. Parmi les hypertendus traités, près de la moitié ont un contrôle tensionnel insuffisant, l’objectif chez le diabétique étant d’amener les chiffres tensionnels à 140/80 mm Hg ou en dessous (réf 7).")
14
1- Le diagnostic précoce du diabète est il possible ?
Prise en charge du risque cardiovasculaire 1- Le diagnostic précoce du diabète est il possible ?

15
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
Criteria for diagnosis of diabetes: DCCT=Diabetes Control and Complications Trial; FPG=fasting plasma glucose; OGTT=oral glucose tolerance test; PG=plasma glucose Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
:S14-S80. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
16
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
Categories of increased risk for development of diabetes (prediabetes): Fasting plasma glucose 100 mg/dl (5.6 mmol/L) to 125 mg/dL (6.9 mmol/L) (impaired fasting glucose [IFG]) 2-hour plasma glucose in 75-g oral glucose tolerance test (OGTT) 140 mg/dL (7.8 mmol/L) to 199 mg/dL (11.0 mmol/L) (impaired glucose tolerance [IGT]) A1C 5.7%-6.4% For each of the tests listed above, risk is continuous, extending below the lower limit of the range and becoming disproportionately greater at higher ends of the range. Both IFG and IGT should be viewed as risk factors for both diabetes and cardiovascular disease. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
: Fasting plasma glucose 100 mg/dl (5.6 mmol/L) to 125 mg/dL (6.9 mmol/L) (impaired fasting glucose [IFG]) 2-hour plasma glucose in 75-g oral glucose tolerance test (OGTT) 140 mg/dL (7.8 mmol/L) to 199 mg/dL (11.0 mmol/L) (impaired glucose tolerance [IGT]) A1C 5.7%-6.4% For each of the tests listed above, risk is continuous, extending below the lower limit of the range and becoming disproportionately greater at higher ends of the range. Both IFG and IGT should be viewed as risk factors for both diabetes and cardiovascular disease. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
17
Pre-Diabetes Diagnosis
Plasma glucose and/or A1C level between normal range and diabetes Estimates for developing diabetes over 5 years range from % Elevated triglycerides and/or low HDL 17 American Diabetes Association (ADA) Professional Practice Committee. Standards of medical care in diabetes Diabetes Care ;36(1): S11-S66.
 Professional Practice Committee. Standards of medical care in diabetes Diabetes Care. 2013;36(1): S11-S66.")
18
2 – Comment identifier le risque cardiovasculaire de manière précoce ?
Prise en charge du risque cardiovasculaire 2 – Comment identifier le risque cardiovasculaire de manière précoce ?

19
Waist/hip ratio and prevalence (%) of HT, diabetes and hypercholesterolemia Morocco NPS 2000
P. HTA P. Diabetes P. Hyperchol. Men < 1, , , ,8 > 1, , , ,9 Women < 0, , , ,6 > 0, , , ,4

20
Cardiovascular Death Risk and Proteinuria In Diabetes
National Kidney Foundation, Am J Kid Dis 39 (Suppl 1): S1-S321
: S1-S321.")
22
Peut on prédire la survenue d’une HTA chez le diabétique ?

24
Prise en charge du risque cardiovasculaire
Les interventions thérapeutiques améliorent elles le pronostic CV ? Prise en charge du risque cardiovasculaire

25
Le contrôle glycémique strict améliore-t-il
Le pronostic cardiovasculaire ? Meta-analysis on tight glycemic control BMJ 2011: based on 13 studies Limited benefits to all cause mortality and cardiovascular-related death Values on both sides of the debate can not be ruled out by this analysis Risk and benefit for microvascular and macrovascular complications - inconclusive Risk of harm with hypoglycemia noted Need for more trials Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, et al. BMJ ;343:d4169 doi: /bmj.d4169. 25

26
Cardiovascular Effects of Intensive Lifestyle Intervention in Type 2 Diabetes The Look AHEAD Research Group N Engl J Med 2013; 369: July 11, 2013

27
The Look AHEAD Research Group. N Engl J Med 2013;369:145-154.
Changes in Weight, Physical Fitness, Waist Circumference, and Glycated Hemoglobin Levels during 10 Years of Follow-up. Figure 1. Changes in Weight, Physical Fitness, Waist Circumference, and Glycated Hemoglobin Levels during 10 Years of Follow-up. Shown are the changes from baseline in overweight or obese patients with type 2 diabetes who participated in an intensive lifestyle intervention (intervention group) or who received diabetes support and education (control group). The reported main effect is the average of all between-group differences after baseline. Means were estimated with the use of generalized linear models for continuous measures. MET denotes metabolic equivalents; asterisks indicate P<0.05 for the between-group comparison. Data from 107 visits during year 11 were not included in the analyses. The Look AHEAD Research Group. N Engl J Med 2013;369:
 or who received diabetes support and education (control group). The reported main effect is the average of all between-group differences after baseline. Means were estimated with the use of generalized linear models for continuous measures. MET denotes metabolic equivalents; asterisks indicate P<0.05 for the between-group comparison. Data from 107 visits during year 11 were not included in the analyses. The Look AHEAD Research Group. N Engl J Med 2013;369:")
28
Cumulative Hazard Curves for the Primary Composite End Point.
The Look AHEAD Research Group. N Engl J Med 2013;369:

32
Prise en charge de hypertension du sujet diabétique

33
Quelles cibles de P.A. ? Framingham : courbe de risque linéaire;
UKPDS : pronostic groupe strict > groupe normal; HOT : groupe <80, vs g <90 vs g<100; ADVANCE : g 135/75 vs g 140/77; consensus sur cible : PAS <130 et PAD <80 mmHg;

34
Effets délétères d’une baisse trop importante
INVEST : cible <130 mmHg Augmentation du risque d’atteinte coronaire et de la mortalité globale; ROADMAP : 4500 diabétiques; NEJM 2011 Olmésartan vs placebo; Groupe tt intensif vs tt normal augmentation mortalité CV; Aucun bénéfice sur les événements CV;

35
Effects of Intensive Blood-Pressure Control in Type 2 Diabetes Mellitus
The ACCORD Study Group N Engl J Med 2010; 362:

36
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585.
Mean Systolic Blood-Pressure Levels at Each Study Visit. Figure 1. Mean Systolic Blood-Pressure Levels at Each Study Visit. I bars indicate 95% confidence intervals. The ACCORD Study Group. N Engl J Med 2010;362:

37
The ACCORD Study Group. N Engl J Med 2010;362:1575-1585.
Kaplan–Meier Analyses of Selected Outcomes. Figure 2. Kaplan–Meier Analyses of Selected Outcomes. Shown are the proportions of patients with events for the primary composite outcome (Panel A) and for the individual components of the primary outcome (Panels B, C, and D). The insets show close-up versions of the graphs in each panel. The ACCORD Study Group. N Engl J Med 2010;362:
 and for the individual components of the primary outcome (Panels B, C, and D). The insets show close-up versions of the graphs in each panel. The ACCORD Study Group. N Engl J Med 2010;362:")
38
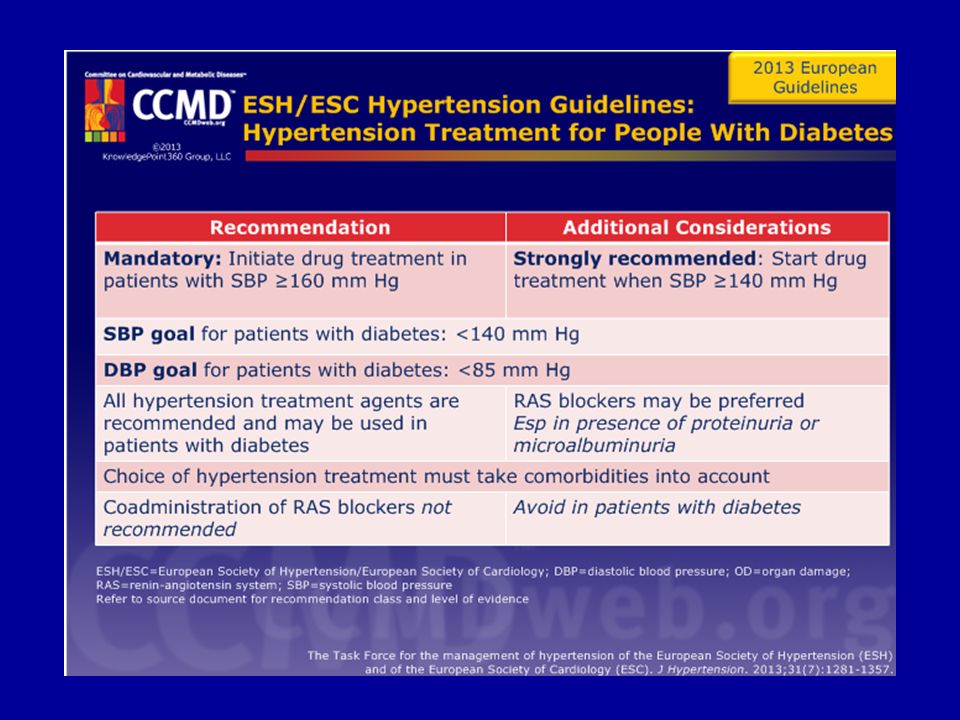
Quelles cibles pour le diabétique hypertendu en 2014?
ESH 2009 80-85 ESH – ESC 2013 < 140 <85 JNC8 <140 <90 ADA 2014 <80

39
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
Blood pressure (BP) screening: measure blood pressure (BP) at every visit. Elevated BP should be confirmed at a separate visit. Treatment targets Systolic blood pressure (SBP) <140 mm Hg for those with diabetes and hypertension; lower SBP targets (eg, <130 mm Hg) may be appropriate in certain patients if target can be achieved without treatment burden Diastolic blood pressure (DBP) <80 mm Hg for persons with diabetes Treatment BP >120/80 mm Hg: advise on lifestyle changes to reduce BP, including weight loss (if overweight), Dietary Approaches to Stop Hypertension (DASH)-style diet (including reducing sodium and increasing potassium intake), moderation of alcohol intake, and increased physical activity BP >140/80 mm Hg: Lifestyle changes to reduce BP Initiation and titration of pharmacologic therapy to achieve BP targets For those with diabetes and hypertension, use either an angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB). If one class is not tolerated, substitute other class . ≥2 agents at maximal doses usually required to achieve BP targets Administer ≥1 agent at bedtime Monitor serum creatinine/estimated glomerular filtration rate and serum potassium if using ACEI, ARB, or diuretic Treatment and targets for pregnant women with diabetes and hypertension /65-79 mm Hg target ACEIs, ARBs contraindicated Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. Any pharmacologic agents discussed are approved for use in the United States by the U.S. Food and Drug Administration (FDA) unless otherwise noted. Consult individual prescribing information for approved uses outside of the United States. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
 screening: measure blood pressure (BP) at every visit. Elevated BP should be confirmed at a separate visit. Treatment targets. Systolic blood pressure (SBP) <140 mm Hg for those with diabetes and hypertension; lower SBP targets (eg, <130 mm Hg) may be appropriate in certain patients if target can be achieved without treatment burden. Diastolic blood pressure (DBP) <80 mm Hg for persons with diabetes. Treatment. BP >120/80 mm Hg: advise on lifestyle changes to reduce BP, including weight loss (if overweight), Dietary Approaches to Stop Hypertension (DASH)-style diet (including reducing sodium and increasing potassium intake), moderation of alcohol intake, and increased physical activity. BP >140/80 mm Hg: Lifestyle changes to reduce BP. Initiation and titration of pharmacologic therapy to achieve BP targets. For those with diabetes and hypertension, use either an angiotensin-converting enzyme inhibitor (ACEI) or angiotensin receptor blocker (ARB). If one class is not tolerated, substitute other class . ≥2 agents at maximal doses usually required to achieve BP targets. Administer ≥1 agent at bedtime. Monitor serum creatinine/estimated glomerular filtration rate and serum potassium if using ACEI, ARB, or diuretic. Treatment and targets for pregnant women with diabetes and hypertension /65-79 mm Hg target. ACEIs, ARBs contraindicated. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. Any pharmacologic agents discussed are approved for use in the United States by the U.S. Food and Drug Administration (FDA) unless otherwise noted. Consult individual prescribing information for approved uses outside of the United States. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
41
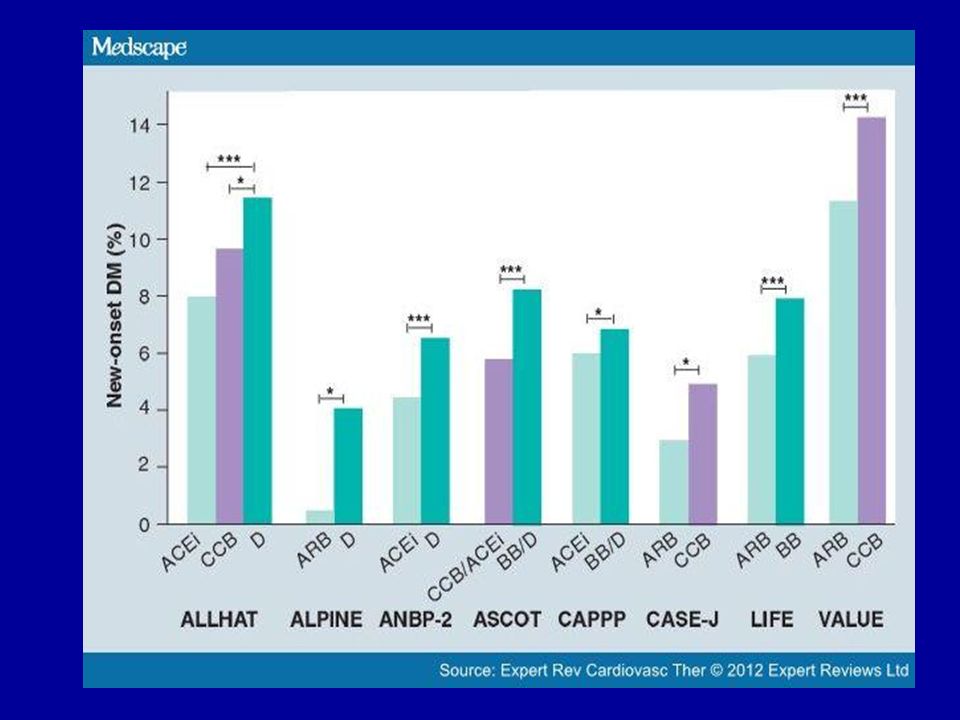
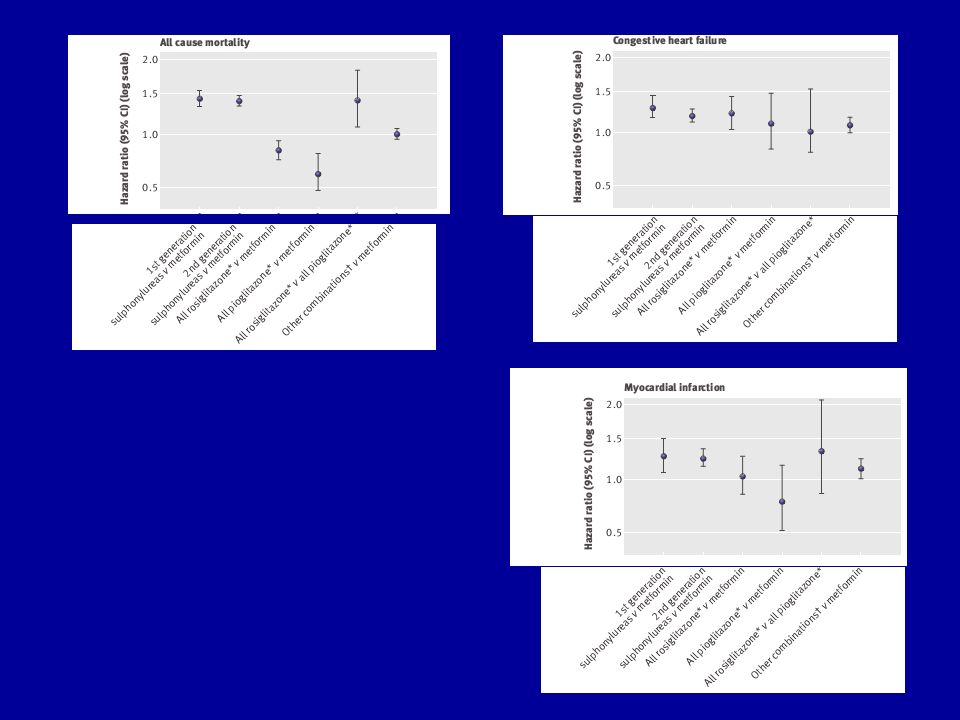
ADO et risque CV

42
Résumé de la PEC Surveillance et dépistage précoce de l’HTA chez le diabétique; Dépistage précoce du diabète et du prédiabète chez les sujets à risque CV et hypertendus ; Le contrôle glycémique strict n’améliore pas le pronostic CV; La prise en charge précoce de l’HTA est favorable sur le pronostic CV; La baisse trop importante de la TA a un effet délétère!

43
Résumé de la PEC Mesures diététiques; Activité physique
Décourager le tabagisme Contrôle de la dyslipidémie; Aspirine Contrôle de l’hypertension ; bithérapie d’emblée (sujet à haut risque CV); Traitement de première ligne : IEC ou ARA II Cible thérapeutique ? : ESH 2013 < 140 et < 85
; Traitement de première ligne : IEC ou ARA II. Cible thérapeutique : ESH 2013 < 140 et < 85.")
44
Conclusions HTA fréquente chez le diabétique
Le SRAA fait le lien entre HTA, syndrome métabolique, dyslipidémie,obésité et diabète; Le pronostic CV dépend de la rapidité de la PEC Les médicaments préférentiels de 1ère ligne sont IEC, ARA II; Mais toutes les familles peuvent être utilisées Il est souvent nécessaire d’associer plusieurs anti-hypertenseurs; prescrire un anti-hypertenseur le soir ;

45
Merci de votre attention

47
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
Aspirin for primary prevention mg/day recommended as primary prevention in patients with type 1 and type 2 diabetes at increased cardiovascular disease (CVD) risk (10-year risk >10%). Includes most men aged >50 yrs or women aged >60 yrs with ≥1 additional major risk factor: family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria Not recommended in low-risk patients (10-year risk <5%; men aged <50 yrs and women aged >60 yrs with no major additional CVD risk factors) since potential for bleeds likely offsets potential benefits Use clinical judgment for treating men <50 years and women <60 years with multiple other risk factors (10-year risk 5%-10%) Aspirin for secondary prevention mg/day recommended in patients with diabetes with CVD history Clopidogrel 75 mg/day recommended for patients with CVD and documented aspirin allergy. Dual antiplatelet therapy is reasonable for ≤1 year after acute coronary syndrome Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. Any pharmacologic agents discussed are approved for use in the United States by the U.S. Food and Drug Administration (FDA) unless otherwise noted. Consult individual prescribing information for approved uses outside of the United States. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
 risk (10-year risk >10%). Includes most men aged >50 yrs or women aged >60 yrs with ≥1 additional major risk factor: family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria. Not recommended in low-risk patients (10-year risk <5%; men aged <50 yrs and women aged >60 yrs with no major additional CVD risk factors) since potential for bleeds likely offsets potential benefits. Use clinical judgment for treating men <50 years and women <60 years with multiple other risk factors (10-year risk 5%-10%) Aspirin for secondary prevention mg/day recommended in patients with diabetes with CVD history. Clopidogrel 75 mg/day recommended for patients with CVD and documented aspirin allergy. Dual antiplatelet therapy is reasonable for ≤1 year after acute coronary syndrome. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. Any pharmacologic agents discussed are approved for use in the United States by the U.S. Food and Drug Administration (FDA) unless otherwise noted. Consult individual prescribing information for approved uses outside of the United States. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
48
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
Measure fasting lipids at least annually in adults with diabetes. Adults with low-risk lipid values (LDL-C <100 mg/dL [2.6 mmol/L], HDL-C >50 mg/dL [1.3 mmol/L], triglycerides <150 mg/dL [1.7 mmol/L]) can be measured every 2 years. Targets No overt CVD: LDL-C <100 mg/dL (2.6 mmol/L) Overt CVD: <70 mg/dL (1.8 mmol/L), with high-dose statin therapy* If targets not achieved on maximal statin therapy: ~30-40% LDL-C reduction from baseline Treatment should include lifestyle modification, focusing on Reduced saturated fat, trans fat, cholesterol intake Increased intake of omega-3 fatty acids, viscous fiber, plant stenols/sterols Weight loss (if indicated) Increased physical activity Statin therapy* and lifestyle changes should be used in those with Overt cardiovascular disease (CVD) No CVD in patients aged >40 years and with ≥1 CVD risk factor (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria) Consider statins in lower-risk patients (no overt CVD, aged <40 years) if LDL-C >100 mg/dL or in presence of multiple CVD risk factors Combination therapy not recommended *Statins contraindicated in pregnancy Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. Any pharmacologic agents discussed are approved for use in the United States by the U.S. Food and Drug Administration (FDA) unless otherwise noted. Consult individual prescribing information for approved uses outside of the United States. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
 can be measured every 2 years. Targets. No overt CVD: LDL-C <100 mg/dL (2.6 mmol/L) Overt CVD: <70 mg/dL (1.8 mmol/L), with high-dose statin therapy* If targets not achieved on maximal statin therapy: ~30-40% LDL-C reduction from baseline. Treatment should include lifestyle modification, focusing on. Reduced saturated fat, trans fat, cholesterol intake. Increased intake of omega-3 fatty acids, viscous fiber, plant stenols/sterols. Weight loss (if indicated) Increased physical activity. Statin therapy* and lifestyle changes should be used in those with. Overt cardiovascular disease (CVD) No CVD in patients aged >40 years and with ≥1 CVD risk factor (family history of CVD, hypertension, smoking, dyslipidemia, or albuminuria) Consider statins in lower-risk patients (no overt CVD, aged <40 years) if LDL-C >100 mg/dL or in presence of multiple CVD risk factors. Combination therapy not recommended. *Statins contraindicated in pregnancy. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. Any pharmacologic agents discussed are approved for use in the United States by the U.S. Food and Drug Administration (FDA) unless otherwise noted. Consult individual prescribing information for approved uses outside of the United States. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
49
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
Exercise programs for adults with diabetes should include the following: ≥150 min/week moderate-intensity aerobic activity (50%–70% maximum heart rate), spread over ≥3 days/week with no more than 2 consecutive days without exercise Resistance training ≥2 times/week (in the absence of contraindications): patients with type 2 diabetes Patients should be evaluated for contraindications (eg, uncontrolled hypertension, severe autonomic or peripheral neuropathy, history of foot lesions, unstable proliferative retinopathy) that would prohibit certain types of exercise before recommending an exercise program. Age and previous level of physical activity should also be considered. Children with diabetes or prediabetes should engage in ≥60 min physical activity/day. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
, spread over ≥3 days/week with no more than 2 consecutive days without exercise. Resistance training ≥2 times/week (in the absence of contraindications): patients with type 2 diabetes. Patients should be evaluated for contraindications (eg, uncontrolled hypertension, severe autonomic or peripheral neuropathy, history of foot lesions, unstable proliferative retinopathy) that would prohibit certain types of exercise before recommending an exercise program. Age and previous level of physical activity should also be considered. Children with diabetes or prediabetes should engage in ≥60 min physical activity/day. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
50
The American Diabetes Association (ADA) released standards of medical care in diabetes for 2014.
With regard to smoking cessation, all patients with diabetes should be advised not to smoke or use tobacco products. Patients should be counseled on smoking prevention and cessation as part of routine care. The level of nicotine dependence should be assessed, and pharmacologic therapy should be offered as appropriate. Refer to source document for full recommendations, including level of evidence rating. American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. January 2014 This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.
:S14-S80. January This slide was created by KnowledgePoint360 Group, LLC, and was not associated with funding via an educational grant or a promotional/commercial interest.")
Présentations similaires



 and associated factors in HIV-infected patients,>")










 Accra - Ghana, 10 – 12 Mars 2009 Trends in remuneration and motivation.>")






