Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
ASPIRINE ET GROSSESSE QUE NOUS APPORTE LA LITTERATURE S.UZAN
SERVICE DE GYNECOLOGIE OBSTETRIQUE ET MEDECINE DE LA REPRODUCTION UNITE PROPRE DE RECHERCHE U P R E S EA 2396 PHYSIOLOGIE DE L’IMPLANTATION ET DU DEVELOPPEMENT

2
FACTEURS DE RISQUE DE PE
*ANTECEDENTS DE PE SEVERE ET PRECOCE(34 SA) *DIABETE , HTA CHRONIQUE, NEPHROPATHIE *MALADIE AUTO-IMMUNE * FCS >/= 3 origine vasculaire ou reste bilan negatif *ANTECEDENTS FAMILIAUX DE PE SEVERE *PRIMIPARITE *HTA GRAVIDIQUE , ROLL OVER TEST POSITIF *DOPPLER UTERIN ANORMAL *GROSSESSE MULTIPLE *GROSSESSES > 40 ans , ADOLESCENTES (?)
 *DIABETE , HTA CHRONIQUE, NEPHROPATHIE. *MALADIE AUTO-IMMUNE. * FCS >/= 3 origine vasculaire ou reste bilan negatif. *ANTECEDENTS FAMILIAUX DE PE SEVERE. *PRIMIPARITE. *HTA GRAVIDIQUE , ROLL OVER TEST POSITIF. *DOPPLER UTERIN ANORMAL. *GROSSESSE MULTIPLE. *GROSSESSES > 40 ans , ADOLESCENTES ( )")
3
A COOMARASAMY AND ALL BJOG 110 .pp 882-888 OCTOBRE 2003 PE MPN
INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA: A FRAMEWORK OF CLINICAL DECISION MAKING A COOMARASAMY AND ALL BJOG 110 .pp OCTOBRE 2003 PE ET MPN NOMBRE DE PATIENTES A TRAITER POUR « GAGNER » UNE PE (*) OU UNE MPN (§) PE MPN TOTAL ESSAIS * §----
 OU UNE MPN (§) PE MPN TOTAL ESSAIS ----* §----")
4
INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA:
Danger Potentiel Aspirine +/- Contr.Indic. Antécédents personnels Médicaux ou Obstétricaux. Risque PE ou RCIU Qualité Implantation Intérêt Prescription Aspirine Doppler Utérin 22 s INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA: A FRAMEWORK OF CLINICAL DECISION MAKING A.COOMARASSAMY and al BMJO OCTOBER VOL.10,pp

5
PE ET MPN NOMBRE DE PATIENTES A TRAITER POUR « GAGNER »
UNE PE (*) OU UNE MPN (§) ET SELON LE DOPPLER UTERIN A 22 SA PE MPN TOTAL ESSAIS * §---- DU.P DU.Nl DU.P DU.Nl BAS RISQUE * * § §---- HAUT RISQUE ----* * § §---- A COOMARASAMY AND ALL BJOG 110 .pp OCTOBRE 2003
 OU UNE MPN (§) ET SELON LE DOPPLER UTERIN A 22 SA. PE MPN TOTAL ESSAIS ----* §---- DU.P DU.Nl DU.P DU.Nl BAS RISQUE ----* * § §---- HAUT RISQUE * * § §---- A COOMARASAMY AND ALL BJOG 110 .pp OCTOBRE")
6
Aspirine et Doppler Utérin
Terme dose mg n RR PE : 0,55 (0,32-0,95) RR RCIU :NS Coomarasamy et al Obstet.Gynecol. 98,5,1,2001
 RR RCIU :NS. Coomarasamy et al Obstet.Gynecol. 98,5,1,2001.")
7
Essais publiés après la méta-analyse
Screening with a uterine Doppler in low risk pregnant women followed by low dose aspirin in women with abnormal results : a multicenter randomised controlled trial F. Goffinet et al BJOG, May 2001 Aspirin (100mg) used for prevention of pre-eclampsia in nulliparous women : the Essai Régional Aspirine Mère-Enfant study (Part 1 and 2) D. Subtil et al BJOG, May 2003 Randomized controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks ’ gestation Yu et al Ult. Obst. Gynec, Sept 2003
 used for prevention of pre-eclampsia in nulliparous women : the Essai Régional Aspirine Mère-Enfant study (Part 1 and 2) D. Subtil et al BJOG, May Randomized controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks ’ gestation. Yu et al Ult. Obst. Gynec, Sept")
8
Risque PE ou RCIU Qualité Implantation Danger Potentiel Aspirine
+/- Contr.Indic. Antécédents personnels Médicaux ou Obstétricaux. Risque PE ou RCIU Qualité Implantation Intérêt Prescription Aspirine Autre marqueur « precoce Doppler 12 s ? Marqueur biologique ( VEGF ?) Doppler Utérin 22 sem INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA: A FRAMEWORK OF CLINICAL DECISION MAKING A.COOMARASSAMY and al BMJO OCTOBER VOL.10,pp
 Doppler. Utérin. 22 sem. INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA: A FRAMEWORK OF CLINICAL DECISION MAKING. A.COOMARASSAMY and al BMJO OCTOBER 2003 VOL.10,pp")
9
ANTIPLATELET DRUGS FOR PREVENTION OF PRE-ECLAMPSIA AND ITS CONSEQUENCES: SYSTEMATIC REVIEW
DULEY L and al BMJ 2001 ;322:

10
DULEY L and al BMJ 2001 ;322:

11
ASPIRINE :RATIONNEL *INEFFICACITE DU TRAITEMENT ANTI HYPERTENSEUR
*LESIONS PLACENTAIRES PRECOCES * PREEMINENCE DU PHENOMENE THROMBOTIQUE *DESEQUILIBRE PGI2/TXA2

12
A.A. Saleh et al; Am J Perinatol; Vol 9, N°4, July 1992:311-12
ASPIRINE FAIBLE DOSE Cellule endothéliale PLAQUETTE INHIBITION DE LA CYCLOXYGENASE(CO) AA CO + AA TXA2 CO PGI2 NIVEAUX PGI2 INCHANGES noyau CHUTE DES TAUX DE TXA2 EFFETS DIMINUTION DU VASOSPASME 2. INHIBITION DE L’ AGGREGATION PLAQUETTAIRE ET DU RELARGAGE DU THROMBOXANE A2 A.A. Saleh et al; Am J Perinatol; Vol 9, N°4, July 1992:311-12 Letters to the Editor
 AA. CO. + AA. TXA2. CO. PGI2. NIVEAUX PGI2 INCHANGES. noyau. CHUTE DES TAUX DE TXA2. EFFETS 1. DIMINUTION DU VASOSPASME. 2. INHIBITION DE L’ AGGREGATION PLAQUETTAIRE. ET DU RELARGAGE DU THROMBOXANE A2. A.A. Saleh et al; Am J Perinatol; Vol 9, N°4, July 1992: Letters to the Editor.")
13
UNE HISTOIRE EN QUATRE EPISODES
ASPIRINE UNE HISTOIRE EN QUATRE EPISODES EPISODE TITRE CONSEQUENCES INDICATIONS « 1 » QUESTIONS FAIRE DES ESSAIS HAUT RISQUE , AUTRES?

14
Prevention of pre-eclampsia by early antiplatelet therapy
M. Beaufils ,S. Uzan & al Lancet 1985 Apr 13;1(8433):840-2
:")
15
AGE, PARITY AND OBSTETRIC HISTORY
Anti phospholipids? Thrombophilia? Group A Group B (n = 52) ( n = 50) Age (yr, mean ± SD) ± ± 4. 7 Number With parity > = Number with known HT Number of following complications * Stillbirths (32) (27) IUGR (9) (12) Spont abortions (13) (21) Number with 0 complication 1 complication 2 complications > = Given as number of events, with number of patients in parentheses * M. Beaufils, S. Uzan, Lancet April
 ( n = 50) Age (yr, mean ± SD) ± ± Number With parity > = Number with known HT Number of following complications * Stillbirths 42 (32) 31 (27) IUGR 10 (9) 12 (12) Spont abortions 20 (13) 27 (21) Number with. 0 complication complication complications 5 8. > = Given as number of events, with number of patients in parentheses. * M. Beaufils, S. Uzan, Lancet April")
16
Prevention of FGR with low doses
Aspirin:findings of the Epreda Trial Lancet , S.Uzan,M.Beaufils,G.Breart & al

17
Population à haut risque de PE et RCIU
MATERIEL Population à haut risque de PE et RCIU Comparant l’efficacité de l’ aspirine (150 mg/j), à aspirine plus dipyridamole (225 mg/j), et placebo à 14 – 16 semaines pour la prévention : • Retard de croissance intra utérin (RCIU) • Mort in utéro (MFIU) • Hématome rétro placentaire (HRP) METHODE Essai multicentrique contrôlé en double aveugle Sélection Risque Dose Terme
, à aspirine plus dipyridamole (225 mg/j), et placebo. à 14 – 16 semaines pour la prévention : • Retard de croissance intra utérin (RCIU) • Mort in utéro (MFIU) • Hématome rétro placentaire (HRP) METHODE. Essai multicentrique contrôlé en double aveugle. Sélection. Risque. Dose. Terme.")
18
Réduction « seulement » ACCIDENTS PERCENT

19
POIDS FOETAL percent Dans les formes les plus sévères X2 = 19.14
gms <1000 > 2500 X2 = 19.14 DF 4 P = 007 Placebo 9.8 Traitement 72.4 61.7 percent

20
RETARD DE CROISSANCE INTRA UTERIN
percent P > 0.01 Sur le groupe avec le risque le plus élevé

21
UNE HISTOIRE EN QUATRE EPISODES
ASPIRINE UNE HISTOIRE EN QUATRE EPISODES EPISODE TITRE CONSEQUENCES INDICATIONS « 1» QUESTIONS FAIRE DES ESSAIS HAUT RISQUE , AUTRES? « 2 » ENTHOUSIASME C ’EST LA SOLUTION POUR TOUT LE MONDE

23
N = 302 (Résultats en %) Aspirine Placebo Prématurité spont . 2.7 3.7
Prématurité induite RPM Déclenchement Césarienne Mort in utéro (n) RCIU Poids * P E ** * p = ; ** p = (OCR = 0.29) JC Hauth et al, Am J Obstet. Gynecol, 1993:168:1083
 1 1. RCIU Poids * P E ** * p = 0.08 ; ** p = (OCR = 0.29) JC Hauth et al, Am J Obstet. Gynecol, 1993:168:1083.")
24
TX B2 / Aspirine Serum Tx B2 (pg/ml) Aspirine Placebo
Accouchement J.C Hauth et al, Am; J. Obstet. Gynecol, 1993;168:1883

25
LES ESSAIS A/ CLASP Lancet 1994;343:619-629
B/ Low dose aspirin to prevent pre-eclampsia In women at high risk Sibai Nejm ;338:701-5 C/ A randomised trial of low dose aspirine for primipara in pregnancy Bjog 1998;105: D/ Barbados low dose aspirine study in pregnancy:blasp Bjog 1998:105:

26
UNE HISTOIRE EN QUATRE EPISODES
ASPIRINE UNE HISTOIRE EN QUATRE EPISODES EPISODE TITRE CONSEQUENCES INDICATIONS « 1 » QUESTIONS FAIRE DES ESSAIS HAUT RISQUE , AUTRES? « 2 » ENTHOUSIASME C ’EST LA SOLUTION POUR TOUT LE MONDE « 3 » DEPRESSION TOUT ETAIT FAUX AUCUNE INDICATION

27
B.Sibai American Journal Obstet.& Gynecol. 1998
Aspirin:A Big Disapointment ! B.Sibai American Journal Obstet.& Gynecol. 1998

28
Pourquoi CLASP fut un essai négatif ?
Hétérogénéité Biais de sélection des patientes: « contre-sélection !» Traitement tardif (70% après 21 semaines) Définition de la pré- éclampsie Toutefois dans certains sous groupes , l’ aspirine prévient la PE sévère (Bower et al Br J Obstet Gynaecol 1996;103:625)
 Définition de la pré- éclampsie. Toutefois dans certains sous groupes , l’ aspirine prévient la PE sévère (Bower et al Br J Obstet Gynaecol 1996;103:625)")
29
PE Preterm delivery P = 0.005 Prophylaxis 13 % NS Therap. Reason
Term at entry < 20 > 20 P = 0.005 Prophylaxis 13 % NS Therap. Reason 12 % NS Total Preterm delivery Prophylaxis 12 % Treatment 21 % Total 14 % p = 0.005 CLASP. Lancet 1994;343:

30
UNE HISTOIRE EN QUATRE EPISODES
ASPIRINE UNE HISTOIRE EN QUATRE EPISODES EPISODE TITRE CONSEQUENCES INDICATIONS « 1 » QUESTIONS FAIRE DES ESSAIS HAUT RISQUE , AUTRES? « 2 » ENTHOUSIASME C ’EST LA SOLUTION POUR TOUT LE MONDE « 3» DEPRESSION TOUT ETAIT FAUX AUCUNE INDICATION « 4 » RAISON ANALYSES SELECTION DES INDICATIONS

31
LES FACTEURS INFLUENCANT L’ACTION DE L’ASPIRINE
*TERME DU DEBUT DU TRAITEMENT *LA DOSE * L’ INDICATION :TYPE *L’ INDICATION :SEVERITE

32
Traitement < 13 sa vs plus tard
From Sullivan et al Thromb Haemost 1998;79:743-6 « Too Little Too Late »

33
Méta-analyse (2) Mortalité Périnatale
Leitich H et al Br J Obstet Gynaecol 1997;104:450-59

34
Aspirin dosage Perfusion of isolated cotyledons, 10-5 to 10-4 M ASA.
Concentration of 10-4 M necessary to inhibit TX on the fetal side. A concentration of 10-4 M in maternal blood is obtained only for dosages of at least 100 mg/day. Wang Y et al. 10th ISSHP Meeting, Seattle, 1996

35
Temps de Saignement mn N=187
Succès Echec N=187 Augmentation du TS Technique de IVY A.Dumont,,S.Uzan et al Am.J.Obstet.Gynec 1999,180,135-40

37
Aspirine Dose mg/j 150 100 50 Implant. I ère Inv. 2 nd Inv.

38
Risque PE ou RCIU Qualité Implantation Danger Potentiel Aspirine
+/- Contr.Indic. Antécédents personnels Médicaux ou Obstétricaux. Risque PE ou RCIU Qualité Implantation Intérêt Prescription Aspirine Autre marqueur « precoce Doppler 12 s ? Marqueur biologique ( VEGF ?) Doppler Utérin 22 sem INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA: A FRAMEWORK OF CLINICAL DECISION MAKING A.COOMARASSAMY and al BMJO OCTOBER VOL.10,pp
 Doppler. Utérin. 22 sem. INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA: A FRAMEWORK OF CLINICAL DECISION MAKING. A.COOMARASSAMY and al BMJO OCTOBER 2003 VOL.10,pp")
39
Aspirin for prevention of pre-eclampsia in women with historical risk factors : a systematic review. Obstet. Gynecol. jun 14 trials 12416 women past. Obst.Hist ,Chronic HTA Diabètes renal dis. * Perinatal Death 0,79 * * Pre Eclampsia 0,86 * * Spont. Preterm birth 0,86 * * mean birth weight * * placental abruption 0,98 NS * Egger Test (biases) 0,84 NS
 0,84 NS.")
40
PEUT- ON OBTENIR LA MÊME INFORMATION PLUS TÔT ?
Pour les multipares :Indication …….Antécédents Mais pour les primipares : # 50 % des patientes Valeur Prédictive du Doppler Utérin au 2° Trimestre PEUT- ON OBTENIR LA MÊME INFORMATION PLUS TÔT ?

41
VÉLOCIMÉTRIE UTÉRINE AU 1ER TRIMESTRE
259 patientes « non sélectionnées » consultant dès le 1° trimestre Doppler utérin à 12 puis 22 SA Devenir clinique Uzan M et al

42
Doppler Précoce et prévention de la PE et du RCIU par l’aspirine
Vainio. M et al BJOG Fev 120 patientes à haut risque de PE ou RCIU Antécédents (pers. ou familial) Diabète ,Age Doppler utérin entre W 90 patientes avec 2 Notches Randomisée. Double-aveugle. Prospective. Essai avec Aspirine (50mg vs Placebo)
 Diabète ,Age. Doppler utérin entre W. 90 patientes avec 2 Notches. Randomisée. Double-aveugle. Prospective. Essai avec Aspirine (50mg vs Placebo)")
43
CONCLUSIONS 1/L’ effet de l’aspirine est indiscutable chez des patientes à haut risque pour ce qui concerne la pré– éclampsie,la mortalité périnatale ,la prématurité (en particulier induite et vraisemblablement le rciu 2/Un traitement précoce à une dose efficace (Généralement 100 mg) est nécessaire 3/Certaines indications sont établies Les résultats sont discordants pour d’autres 4/Une prescription précoce basée sur le doppler utérin à 12 sa semble être une voie prometteuse.
 est nécessaire. 3/Certaines indications sont établies. Les résultats sont discordants pour d’autres. 4/Une prescription précoce basée sur le doppler utérin à 12 sa semble être une voie prometteuse.")
44
ASPIRINE: PRINCIPALES INDICATIONS
PROUVEES: Haut risque de récidive de PE ou RCIU Syndrôme des antiphospholipides et autres thrombophilies (thrombocytémies) Indications médicales(neuro,cardio) FIV lors d’un SAPL PROBABLES/POSSIBLES: HTA chronique/Néphropathie chronique Greffe rénale RESULTATS DISCORDANTS: FCS inexpliquées Diabète DU à 22 sa Gémellaires FIV IMPROBABLES: Primipares Grossesses après FIV ARRET ASPIRINE : PE et HELLP PISTES POUR L’AVENIR +++ DOPPER à 12 sa
 Indications médicales(neuro,cardio) FIV lors d’un SAPL. PROBABLES/POSSIBLES: HTA chronique/Néphropathie chronique. Greffe rénale. RESULTATS DISCORDANTS: FCS inexpliquées. Diabète. DU à 22 sa. Gémellaires. FIV. IMPROBABLES: Primipares. Grossesses après FIV. ARRET ASPIRINE : PE et HELLP. PISTES POUR L’AVENIR +++ DOPPER à 12 sa.")
48
Doppler à 12 semaines :60 % avec 2 Notch
PROJET PHRC :Etude Multicentrique sur population « générale » de primipares L.Carbillon,M.Uzan Doppler à 12 semaines :60 % avec 2 Notch ASPIRINE 100 mg /j vs Pas de Traitement Doppler à 22 semaines si absence de notch arrêt ASA Pour Naissances (47O primipares,280 avec 2N 140 traitées (dont 60 jusque 35 semaines ) et non traitées Mais... 50% des futures complications recevront un traitement dès 12 semaines Cette étude paraît aujourd’hui d ’autant plus justifiée que….
 et 140 non traitées. Mais... 50% des futures complications recevront un. traitement dès 12 semaines. Cette étude paraît aujourd’hui d ’autant plus justifiée que….")
49
VÉLOCIMÉTRIE UTÉRINE A LA FIN DU 1ER TRIMESTRE
Adaptation presente Complete Precoce Tardive Partielle Absente 259 patientes population générale

50
VÉLOCIMÉTRIE UTÉRINE A LA FIN DU 1ER TRIMESTRE POIDS DE NAISSANCE
POIDS MOYENS 3373g +/- 521g __________________ 3175g +/- 443g 2637g +/- 786g 2383g +/- 912g 0, 0 1, 0 2, 0 1, 1 2, 1 2, 2 0 Notch % 1 Notch % 2 Notches % Différences significatives

51
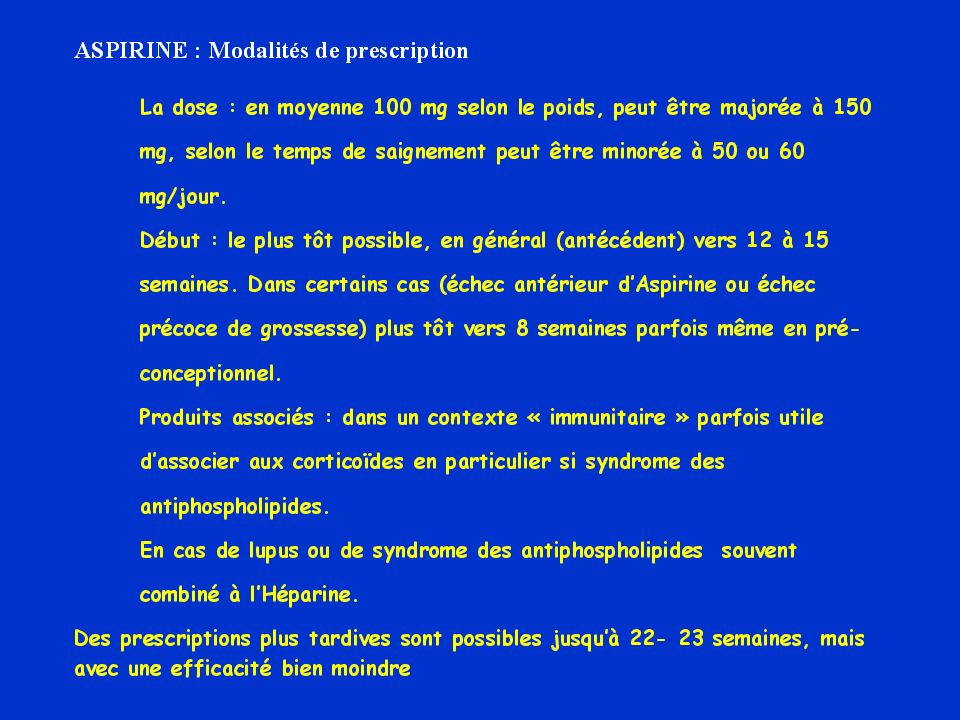
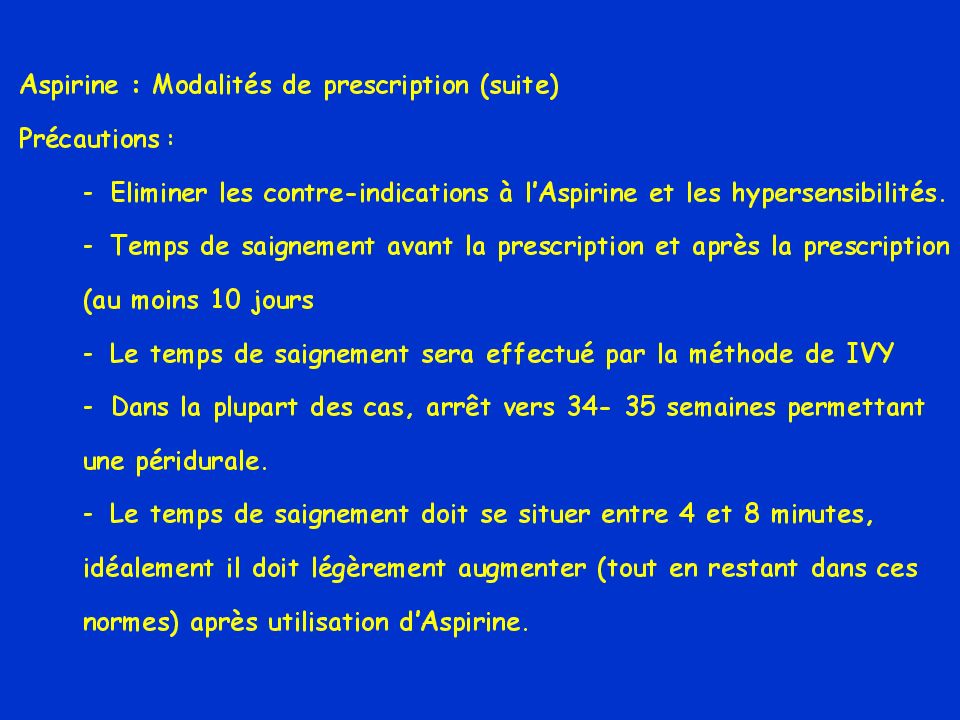
Modalites prescrption

52
INDIVIDUALISING USE OF ASPIRIN TO PREVENT PRE-ECLAMPSIA:
A FRAMEWORK OF CLINICAL DECISION MAKING A.COOMARASSAMY and al BMJO OCTOBER 2003 VOL.10,pp

53
ANTIPLATELET DRUGS FOR PREVENTION OF PRE-ECLAMPSIA AND ITS CONSEQUENCES: SYSTEMATIC REVIEW
DULEY L and al BMJ 2001 ;322:

54
PERINATAL ANTIPLATELET REVIEW OF INTERNATIONAL STUDIES COLLABORATION
PARIS COLLABORATION COORDINATION CENTER CENTRE OF PERINATAL HEALTH SERVICES RESEACH UNIVERSITY OF SYDNEY

55
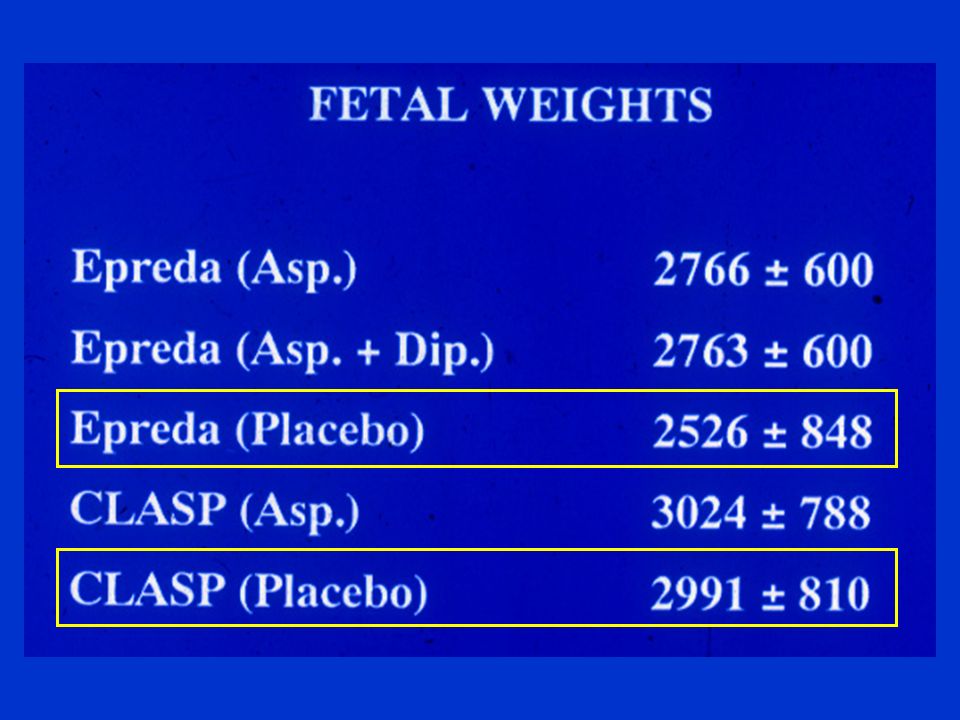
GESTATIONAL AGE AND FETAL PLACENTAL WEIGHTS
Group A Group B p value (n = 48) (n = 45) Duration of pregn. (weeks) < 0.001 Fetal weight (g) < 0.001 Placental weight (g) < 0.01 No of babies < 10th perc < 0.005 No of babies < 3rd perc < 0.005 Pre eclampsia < 0.01 Fet&Neonat loss < 0.01 M Beaufils, S. Uzan, Lancet April 13, 1985
 (n = 45) Duration of pregn. (weeks) < Fetal weight (g) < Placental weight (g) < No of babies < 10th perc < No of babies < 3rd perc. 0 7 < Pre eclampsia 0 6 < Fet&Neonat loss 0 5 < M Beaufils, S. Uzan, Lancet April 13,")
56
If inhibition 50% or more :
TxB2 inhibition If inhibition 50% or more : PE 1.9 vs 5.7% (p = 0.016) IUGR: 2.9 vs 7% (p = 0.023) Prematurity: 5.7 vs 10.7% (p = 0.032) Birthweight: 3314 vs 3121 g (p = ) Hauth et al Amer J Obstet Gynecol 1995;173:578-84) This is no longer found in 1998 (AJOG 1998;179:1193-9)
 IUGR: 2.9 vs 7% (p = 0.023) Prematurity: 5.7 vs 10.7% (p = 0.032) Birthweight: 3314 vs 3121 g (p = ) Hauth et al Amer J Obstet Gynecol 1995;173:578-84) This is no longer found in 1998 (AJOG 1998;179:1193-9)")
57
However, the same authors...
Sibai et al (New Engl J Med 1993;329:1213-8) Nulliparous pts. RR for PE = 0.7 ( ). RR = 0.47 if SBP at inclusion Hauth et al (Amer J Obstet Gynecol 1993; 168: ). Nulliparous pts. OR for PE = 0.29 ( ). OR = 0.16 for « severe » PE. Does it mean that aspirin is efficient in healthy primiparous women with a baseline risk 5%, and inefficient with a risk of 25% ???
 Nulliparous pts. RR for PE = 0.7 ( ). RR = 0.47 if SBP at inclusion Hauth et al (Amer J Obstet Gynecol 1993; 168: ). Nulliparous pts. OR for PE = 0.29 ( ). OR = 0.16 for « severe » PE. Does it mean that aspirin is efficient in healthy primiparous women with a baseline risk 5%, and inefficient with a risk of 25%")
58
Too little, too Late M. h. f. Sullivan et al Am. J
Too little, too Late M.h.f. Sullivan et al Am. J. Aug 1999,181;2: Patients in whom treatment was initiated in the first trimester of pre-gnancy ( 13 w.g) had significantly better outcomes than those in whom treatment was initiated in the second trimester
 had significantly better outcomes than those in whom treatment was initiated in the second trimester.")
59
Meta-analysis: 13 studies (1985-94)
IUGR Leitich H et al Br J Obstet Gynaecol 1997;104:450-59

60
A. Dumont, A Flahault, M. Beaufils,
EFFECT OF ASPIRIN IN PREGNANT WOMEN IS DEPENDENT ON INCREASE IN BLEEDING TIME A. Dumont, A Flahault, M. Beaufils, E. Verdy, & S. Uzan Am J Obstet Gynecol 1999;180:135-40

61
Dumont et al. Retrospective study of 187 consecutive patients treated with aspirin. Classified as "success" or "failure". Multiple variables tested by univariate analysis Multivariate analysis : 2 independant factors associated with "success": Treatment before 17 weeks Increase in bleeding time > 2 min. Am J Obstet Gynec 1999 ;180 :135-40

62
PEUT-ON OBTENIR LA MÊME
INFORMATION PLUS TÔT ?

63
Aspirin Dosage mg/day 150 100 50 Implant. First Tr.Inv. Second.Tr. Invas.

64
VÉLOCIMÉTRIE UTÉRINE A LA FIN DU DU 1ER TRIMESTRE COMPLICATIONS
259 patientes 4,6% 12% 57% 73% % Complications HTA, PE, RCIU, MFIU, HRP

65
Potential harms of Aspirin use in Pregnancy
Studies Study Design Slone Cohort 50282 Congenital Abn. Klebanoff Benendes Cohort 19226 Mean IQ Werler Case-Contol 1381/6966 Cardiac defects Nielsen Cohort 18721

66
Trials published after the meta Analysis
Screening with a uterine Doppler in low risk pregnant women followed by low dose aspirin in women with abnormal results : a multicenter randomised controlled trial F. Goffinet et al BJOG, May 2001 Aspirin (100mg) used for prevention of pre-eclampsia in nulliparous women : the Essai Régional Aspirine Mère-Enfant study (Part 1 and 2) D. Subtil et al BJOG, May 2003 Randomized controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks ’ gestation Yu et al Ult. Obst. Gynec, Sept 2003
 used for prevention of pre-eclampsia in nulliparous women : the Essai Régional Aspirine Mère-Enfant study (Part 1 and 2) D. Subtil et al. BJOG, May Randomized controlled trial using low-dose aspirin in the prevention of pre-eclampsia in women with abnormal uterine artery Doppler at 23 weeks ’ gestation. Yu et al. Ult. Obst. Gynec, Sept")
67
DULEY L and al BMJ 2001 ;322:

68
A.A. Saleh et al; Am J Perinatol; Vol 9, N°4, July 1992:311-12
LOW DOSE ASPIRIN ENDOTHELIAL CELL PLATELET INHIBITION OF CYCLOXYGENASE (CO) AA CO + AA TXA2 CO PG2 INALTERED PG2 LEVELS NUCLEUS DECREASED TXA2 LEVELS NET EFFECT 1. DECREASE VASOSPASM 2. INHIBITION OF PLATELET AGGREGATION AND RELEASE REACTION TXA2 A.A. Saleh et al; Am J Perinatol; Vol 9, N°4, July 1992:311-12 Letters to the Editor
 AA. CO. + AA. TXA2. CO. PG2. INALTERED PG2 LEVELS. NUCLEUS. DECREASED TXA2 LEVELS. NET EFFECT 1. DECREASE VASOSPASM. 2. INHIBITION OF PLATELET AGGREGATION. AND RELEASE REACTION TXA2. A.A. Saleh et al; Am J Perinatol; Vol 9, N°4, July 1992: Letters to the Editor.")
69
BIRTHWEIGHTS percent On the most severe cases X2 = 19.14 DF 4 P = 007
gms <1000 > 2500 X2 = 19.14 DF 4 P = 007 Placebo 9.8 Treatment 72.4 61.7 percent

70
Reduction « only » ACCIDENTS PERCENT

71
FETAL GROWTH RETARDATION
percent P > 0.01 On the group with the highest risk

72
AIM In a selected population at high risk of PE or IUGR Comparing the efficiency of aspirin (150 mg/day), aspirin plus dipyridamole (225 mg/day), and pla-cebo for preventing : • Fetal growth retardation (FGR) • Stillbirth (FD) • Abruptio placentae (AP) METHODS Muticentric, double bind, placebo-controlled trial selection Risk dose
, aspirin plus dipyridamole (225 mg/day), and pla-cebo for preventing : • Fetal growth retardation (FGR) • Stillbirth (FD) • Abruptio placentae (AP) METHODS. Muticentric, double bind, placebo-controlled trial. selection. Risk. dose.")
73
Large Trials in unselected populations
Authors N° Dose Term PE (%) Pla Asp Hauth Sibai Italian Study CLASP ECPPA + Significant difference
 Pla Asp. Hauth Sibai Italian Study CLASP ECPPA Significant difference.")
74
TX B2 / Aspirin Serum Tx B2 (pg/ml) Aspirin Placebo
Delivery J.C Hauth et al, Am; J. Obstet. Gynecol, 1993;168:1883

75
N = 302 (Results in %) Aspirin Placebo Spont. Pret. D. 2.7 3.7
Indicat. Pret. D PRM Labor Ind Cesarean D Fetal Death (n) FGR Birthweight * PreEclampsia ** * p = ; ** p = (OCR = 0.29) JC Hauth et al, Am J Obstet. Gynecol, 1993:168:1083
 1 1. FGR Birthweight * PreEclampsia ** * p = 0.08 ; ** p = (OCR = 0.29) JC Hauth et al, Am J Obstet. Gynecol, 1993:168:1083.")
76
GRANDS ESSAIS POPULATIONS A BAS RISQUE
Auteurs N° Dose Terme PE (%) Pla Asp Hauth Sibai Italian Study CLASP ECPPA + différence significative
 Pla Asp. Hauth Sibai Italian Study CLASP ECPPA différence significative.")
77
Why was CLASP negative ? Heterogeneity Counterselection of patients
Late treatment (70% after 21 weeks) Definition of preeclampsia Ancillary study: aspirin prevented severe PE (Bower et al Br J Obstet Gynaecol 1996;103:625)
 Definition of preeclampsia. Ancillary study: aspirin prevented severe PE (Bower et al Br J Obstet Gynaecol 1996;103:625)")
78
Treatment < 13 weeks vs later
From Sullivan et al Thromb Haemost 1998;79:743-6 « Too Little Too Late »

79
Meta-analysis (2) Perinatal mortality
Leitich H et al Br J Obstet Gynaecol 1997;104:450-59

80
DOPPLER UTERIN:VALEUR PREDICTIVE
K.H.NICOLAÏDES ULTRASOUND 2001;18: Etude multicentrique sur la prédictivité du D.U Pour les naissances survenant avant 32 SA 7851 patientes en population générale entre 22 et 24 sa Mesure de l ’index de pulsatilité moyen et prise en compte de l ’incisure protodiastolique SENSIBILITE de l ’Index pour PE + RCIU = 93% PE ISOLEE =80% RCIU ISOLE =56% SENSIBILITE du Notch bilatéral pour PE et/ou RCIU est IDENTIQUE mais sa VPP est significativement meilleure (10 % vs 5%)
")
81
Early Doppler and prevention of PE and IUGR with aspirin
Vainio. M et al BJOG Fev 120 patients at high risk for PE or IUGR Pastobstet. History (pers. Or familial) Diabetes ,Age Doppler at W 90 patients with 2 Notches rand. Double-blind. Prosp. Trial with Aspirin (50mg vs Placebo)
 Diabetes ,Age. Doppler at W. 90 patients with 2 Notches. rand. Double-blind. Prosp. Trial with Aspirin (50mg vs Placebo)")
82
RISQUES POTENTIELS DE L’ASPIRINE PENDANT LA GROSSESSE
Studies Study Design Slone Cohort 50282 Malformations. Klebanoff Benendes Cohort 19226 QI Werler Case-Contol 1381/6966 Cardiopathies Nielsen Cohort 18721

83
HTA PHYSIOPATHOLOGIE Anomalie de la placentation =Défaut d ’invasion trophoblastique =DU Diminution Q utéro placentaire Ischémie placentaire Retentissement fœtal Retentissement maternel SFC= RCIU+OLIGO libération toxines placentaires DO puis DC Altération endothélium vasc * Microangiopathie Thrombotique HTA Rein=protéinurie augmentation résistances vasc Foie=Microthromboses(HELLP) déséquilibre PGI2 et TXA2 Cerveau=Microangiopathie thrombotique Réaction de préservation du Crise Eclampsie débit utéro-placentaire * Troubles de la coagulation CIVD + Thrombopénie
 déséquilibre PGI2 et TXA2. Cerveau=Microangiopathie thrombotique Réaction de préservation du. Crise Eclampsie débit utéro-placentaire. * Troubles de la coagulation. CIVD + Thrombopénie.")
84
DEFINITIONS HTA GRAVIDIQUE PS >= 140 mmHg PD >=90 mmHg
Après 20 sa 10% des grossesses PRE ECLAMPSIE +/- Oedèmes HTAG + Prot >= 0,3 g/l (O,5 /j) 1,5 à 3 % des grossesses Srt 3eme T , I gest , Récidive possible 25% . A distinguer: *HTA chronique préexistant à la grossesse qui peut se compliquer de protéinurie= PE surajoutée *Néphopathie antérieure à la grossesse *HTA labile
 1,5 à 3 % des grossesses. Srt 3eme T , I gest , Récidive possible 25% . A distinguer: *HTA chronique préexistant à la grossesse. qui peut se compliquer de protéinurie= PE surajoutée. *Néphopathie antérieure à la grossesse. *HTA labile.")
85
FACTEURS DE RISQUE DE PE
*ATCD familiaux ou personels de PE *Age maternel > 38 ans *Pathologie maternelle:Obésité,HTA Ch,Néphropathie Ch, SAPL, Hypercholestérolémie,Diabète type I *Grossesses multiples *Nulliparité,Changement de procréateur,Courte durée d’exposition au sperme (utilisation prolongée de préservatifs)
")
86
FACTEURS DE GRAVITE DE LA PE
SIGNES CLINIQUES *SF:Céphalées, Phosphènes , Acouphènes, Douleur épigastrique *SPh: HTA >= 160/110 Aggravations oedèmes =prise de poids Oligurie ROT vifs SIGNES BIOLOGIGUES *Protéinurie > 1G/L *Créatinémie qui s ’éléve *Uricémie > 360µmol/L *Thrombopénie < /mm3 *Hémolyse(schyzocytes,Haptoglobine ,LDH > 600ui) *Cytolyse hépatique(transaminases à 3N) SIGNES ECHOGRAPHIQUES *RCIU *Oligoamnios *DO et DC pathologiques
 *Cytolyse hépatique(transaminases à 3N) SIGNES ECHOGRAPHIQUES. *RCIU. *Oligoamnios. *DO et DC pathologiques.")
87
COMPLICATIONS DE LA PRE-ECLAMPSIE
*MATERNELLES Une des causes de décès maternel L’I.Placentaire est le primum movens avec un retentissement maternel et fœtal à des degrès divers Le Tt est étiologique=Arrêt de la grossesse et évacuation du placenta ECLAMPSIE: 1% des pré-éclampsies HRP:DPPNI Urgence maternelle et fœtale :Pn vital en jeu pour les deux HELLP Syndrôme: Haemolysis, elevated Enzyme Liver,Low Platelet count. C’est une micro-angiopathie thrombotique 10% des PE sévères Mortalité maternelle:2 à 10% et fœtale 10 à 50% *FŒTALES SFC: Rciu et oligoamnios SFA: MFIU et Prématurité induite

88
PLACE DES ULTRA-SONS EN OBSTETRIQUE
1/Rythme cardiaque fœtal :Rythme base,Variabilité,Réactivité, Absence de décélérations 2/Echographie: Biométrie,Morphologie,Placenta, Liquide amniotique 3/Doppler *Utérin:Reflet de la placentation *Ombilical:Représente le potentiel de croissance fœtale *Cérébral:Reflet des phénomènes de redistribution C ’est la mise en place des phénomènes d ’épargne

89
NL= 6 à 10 3 à 5 = Indication à Accouchement 0= urgence périnatale
SCORE DE MANNING Echographie 20 à 30’ et RCF = 20 à 30’ Mouvements respiratoires(thoraco-abdominaux) Mouvements fœtaux globaux Tonus actif Réativité du RCF Quantité de liquide amniotique NL =2 Suspect=1 Patho=0 NL= 6 à à 5 = Indication à Accouchement 0= urgence périnatale
 Mouvements fœtaux globaux. Tonus actif. Réativité du RCF. Quantité de liquide amniotique. NL =2 Suspect=1 Patho=0. NL= 6 à 10 3 à 5 = Indication à Accouchement 0= urgence périnatale.")
90
POINTS FORTS HTA Rôle initiateur de l ’ischémie utéro-placentaire
L ’insuffisance placentaire est responsable de l ’HTA Complications maternelles: Eclampsie,HRP,HELLP fœtales:RCIU,MFIU,Prématurité induite +++CORTICOTHERAPIE DE MATURATION AVANT 34 SA Traitement:Arrêt de la grossesse = le seul efficace *Hospitalisation en niveau pédiatrique adapté au poids et terme *Repos au lit en DLG *Régime normosodé *Corticothérapie prénatale *Tt antihypertenseur prudent NI TROP VITE et NI TROP FORT Inhibiteurs calciques:Nicadipine=LOXEN Alpha et Beta Bloquants=Trandate Diutétiques et IEC sont C/I *Surveillance maternelle et fœtale :signes gravité = Extraction

91
COLONISATION TROPHOBLASTIQUE

92
DOPPLER UTERIN NORMAL

93
DOPPLER UTERIN PATHOLOGIQUE

94
Artère Ombilicale

95
Partie inférieure du corps avec les membres Tube digestif et viscères
Organes préservés lors de souffrancesfoetales Surrénales Cerveau Coeur Organes sacrifiés lors de souffrances fœtales Reins Partie inférieure du corps avec les membres Tube digestif et viscères

96
ARTERE CEREBRALE MOYENNE

Présentations similaires



















 % de la.>")
 Nombres (1-100).>")