Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Stratégies thérapeutiques des infections à C. difficile en réanimation
Lyon, DESCQ Janvier 2010 Stratégies thérapeutiques des infections à C. difficile en réanimation Jean-François TIMSIT Réanimation médicale CHU Albert Michallon INSERM/UJF U823 Grenoble

2
Pré-requis Responsable de 30% des cas de diarrhée post antibiotiques
Responsable de 50 à 80% des cas de colite associée aux antibiotiques Responsable de 95% des cas de CPM Cause la plus importante de diarrhée nosocomiale d’origine bactérienne Manifestations cliniques très variées: portage asymptomatique, diarrhée modérée à CPM gravissime Rechutes fréquentes

3
Antiobio, antineoplasiques

4
Synergie d’action : toxine A (entérotoxine) et toxine B (cytotoxine)
• Rôle prépondérant de la toxine A – Destruction partielle du cytosquelette – Destruction des jonctions interentérocytaires – Libération de médiateurs de l’inflammation dans la lamina propria • Toxine B – Destruction totale du cytosquelette • Toxine binaire CDT ? Thelestham M., Cur. Topics in Microbiol. and Immuno., 2000, 250, Poxton IR, CMI 2001, 7,

5
Virulence Large clostridial toxines (LCT +++)
Toxine A enterotoxine (tcdA) Toxine B cytotoxine (tcdB) Toxine binaire (ADP ribosyl transferase) CDTa sous-unité enzymatique CDTb sous-unité ligand
 Toxine B cytotoxine (tcdB) Toxine binaire (ADP ribosyl transferase) CDTa sous-unité enzymatique. CDTb sous-unité ligand.")
6
Lancet 2005, 366,

7
Levofloxacin MICs for Current Isolates
Figure 3. Distribution of Minimum Inhibitory Concentrations of Levofloxacin for Current (Obtained after 2000) BI/NAP1 and Non-BI/NAP1 Clostridium difficile Isolates. NEJM, Dec 8, 2005, Vol. 353 (23),
 BI/NAP1 and Non-BI/NAP1 Clostridium difficile Isolates. NEJM, Dec 8, 2005, Vol. 353 (23),")
12
Que se passe t-il? incidence formes graves mortalité attribuable
virulence résistance aux antibiotiques (FQ, EM) récidives après metronidazole
 récidives après metronidazole.")
13
Pepin J et al

14
Actualités des colites pseudomembraneuses
(Pepin et al CMAJ 2004;171:466) Mortalité accrue : : 4.7% 2003 : 13.7% Incidence plus élevée (sujet>65 ans) : : 102 2002 : 210 2003 : 866 Les fluoroquinolones souvent en cause Apparition de résistances au métronidazole Pepin et al CMAJ 2004;171:466
 Mortalité accrue : : 4.7% 2003 : 13.7% Incidence plus élevée (sujet>65 ans) : : : : 866. Les fluoroquinolones souvent en cause. Apparition de résistances au métronidazole. Pepin et al CMAJ 2004;171:466.")
15
Age Specific Incidence and Mortality Attributed to C. difficile
NEJM, Dec 8, 2005, Vol. 353 (23),
,")
16
C. Difficile: Risk of death in the hospital
16,7% (*) matched for sex, age charlson index, LOS Since 2002, an epidemic of Clostridium difficile –associated disease (CDAD) caused by a hypervirulent strain has spread to many hospitals in Quebec. Pépin and colleagues studied the effect of the epidemic on mortality and duration of hospital stay among patients admitted to one hospital during 2003 and They found a high excess mortality among 161 inpatients with nosocomial CDAD compared with 656 matched control subjects. Overall, the CDAD patients spent 10.7 days longer in hospital than the control subjects did. The high attributable mortality represents a dramatic change in the pathogenicity of C. difficile. CMAJ 2005;173(9): Since 2002 an epidemic of Clostridium difficile–associated disease (CDAD) caused by a hypervirulent toxinotype III ribotype 027 strain has spread to many hospitals in Quebec. The strain has also been found in the United States, the United Kingdom and the Netherlands. The effects of this epidemic on mortality and duration of hospital stay remain unknown. We measured these effects among patients admitted to a hospital in Quebec during 2003 and 2004. Methods: We compared mortality and total length of hospital stay among inpatients in whom nosocomial CDAD developed and among control subjects without CDAD matched for sex, age, Charlson Comorbidity Index score and length of hospital stay up to the diagnosis of CDAD in the corresponding case. Results: Thirty days after diagnosis 23.0% (37/161) of the patients with CDAD had died, compared with 7.0% (46/656) of the matched control subjects (p < 0.001). Twelve months after diagnosis, mortality was 37.3% (60/161) among patients with CDAD and 20.6% (135/656) among the control subjects (p < 0.001), for a cumulative attributable mortality of 16.7% (95% confidence interval 8.6%–25.2%). Each case of nosocomial CDAD led, on average, to 10.7 additional days in hospital. Interpretation: This study documented a high attributable mortality among elderly patients with CDAD mostly caused by a hypervirulent strain, which represents a dramatic change in the severity of this infection. ABSTRACT: Cite this article as CMAJ 2005;173(9). DOI: /cmaj 409 death in Quebec (8%) August 2004-August 2005: 8673 cases of C. difficile recorded. Pepin et al – CMAJ 2005; 173:1037
 matched for sex, age charlson index, LOS. Since 2002, an epidemic of Clostridium difficile –associated disease (CDAD) caused by a hypervirulent strain has spread to many hospitals in Quebec. Pépin and colleagues studied the effect of the epidemic on mortality and duration of hospital stay among patients admitted to one hospital during 2003 and They found a high excess mortality among 161 inpatients with nosocomial CDAD compared with 656 matched control subjects. Overall, the CDAD patients spent 10.7 days longer in hospital than the control subjects did. The high attributable mortality represents a dramatic change in the pathogenicity of C. difficile. CMAJ 2005;173(9): Since 2002 an epidemic of Clostridium. difficile–associated disease (CDAD) caused by a hypervirulent. toxinotype III ribotype 027 strain has spread to many. hospitals in Quebec. The strain has also been found in the. United States, the United Kingdom and the Netherlands. The effects of this epidemic on mortality and duration of. hospital stay remain unknown. We measured these effects. among patients admitted to a hospital in Quebec during and Methods: We compared mortality and total length of hospital. stay among inpatients in whom nosocomial CDAD developed. and among control subjects without CDAD matched for sex, age, Charlson Comorbidity Index score and length of hospital. stay up to the diagnosis of CDAD in the corresponding case. Results: Thirty days after diagnosis 23.0% (37/161) of the patients. with CDAD had died, compared with 7.0% (46/656) of. the matched control subjects (p < 0.001). Twelve months after. diagnosis, mortality was 37.3% (60/161) among patients with. CDAD and 20.6% (135/656) among the control subjects (p < 0.001), for a cumulative attributable mortality of 16.7% (95% confidence interval 8.6%–25.2%). Each case of nosocomial. CDAD led, on average, to 10.7 additional days in hospital. Interpretation: This study documented a high attributable. mortality among elderly patients with CDAD mostly caused. by a hypervirulent strain, which represents a dramatic change. in the severity of this infection. ABSTRACT: Cite this article as CMAJ 2005;173(9). DOI: /cmaj death in Quebec (8%) August 2004-August 2005: 8673 cases of C. difficile recorded. Pepin et al – CMAJ 2005; 173:1037.")
20
Figure 1 – Signalements d'infection à Clostridium difficile, par mois, France métropolitaine, avril 2007 à décembre 2008 (N=331)
")
21
Figure 2 (bis) – Souches de C
Figure 2 (bis) – Souches de C. difficile caractérisées par le CNR, par mois, France, avril 2007 à décembre 2008 (N=955)
 – Souches de C. difficile caractérisées par le CNR, par mois, France, avril 2007 à décembre 2008 (N=955)")
22
Figure 3 – Souches de Clostridium difficile caractérisées par le CNR, par région d’origine, France, avril 2007 à décembre 2008 (N=949)
")
23
TRT Cl difficile Réhydratation et arrêt ATB
Pas de modificateurs du transit ou d’anti-secrétoires Metronidazole per os ou vancomycine? Autres traitements? Timing de la chirurgie pour les formes les plus graves? Prévention : Saccharomyces boulardii Immunotherapie Mesure hygiène,manuportage

24
Gravité clinique et poursuite des ATB
Modena S et al. J Clin Gastroenterol 2006; 40: 49-54

25
Impact de l’acidité gastrique sur Clostridium difficile?
Oui: CMAJ Dial S Risk of clostridium difficile diarrhea among hospital inpatients prescribed proton pup inhibitors: cohort and case control studies Oui: Dubberke - CID2007; Bishara et al – JHI 2008 Non: ICAAC D’après J. Pépin, communication orale 539 7 6 5 4 Log10 cfu/ml 3 2 Il existe plusieurs études cas-témoins contradictoires en ce qui concerne le rôle des inhibiteurs de pompes à protons comme facteur favorisant la survenue des colites à Clostridium difficile. Toutes ces études posent le problème de possibles facteurs confondants, ou d’un manque de puissance. Pourtant, il ne s’agit pas d’une question accessoire, car les IPP sont parmi les médicaments les plus prescrits dans le monde : au Québec, 50 % des patients hospitalisés en reçoivent au moins une fois, dans 50 % des cas sans raison valable. Jacques Pépin a présenté une étude fondamentale qui plaide fortement contre une association entre IPP et C. difficile : l’acidité gastrique ne semble avoir aucun impact sur C. difficile. Il n’y a donc pas de raison pour qu’un antiacide, même puissant, représente un surrisque… 1 Temps 0 Après 1 h d’incubation dans du liquide gastrique Après 3 h d’incubation Klebsiella Candida Spores de Clostridium difficile

26
Vancomycine ou metronidazole
CMI90: mg/l La plus haute jamais rapportée: 16 mg/L Metronidazole CMI 2 mg/L Pelaez 2005: 415 souches CMI90 4mg/L CMI > 32:6% cas Mais pas de corrélation bio-clinique Wang et al – Diagn Microbiol Infect Dis 1999; 34:1; Aspevall et al – AAC 2006; 50:1890; Pelaez et al – AAC 2005; 49:1147

27
PK metronidazole Oral Metronidazole IV Metronidazole
Absorption rapide: pic 1-2 h paroi colique Concentration fécale Diarrhée liquide: 9.3 µg/g (range ) Selles moulées:1.2 µg/g (range ) Porteurs asymptomatiques 0 IV Metronidazole 3 patients 6.3 µg/g à 24 µg/g Données cliniques publiées anecdotiques Bolton RP et al – Gut 1986; 27:1169; Dion YM et al – Ann Surg 1980; 192:221; Johnson S et al – Ann Intern Med 1992; 117:297
 Selles moulées:1.2 µg/g (range ) Porteurs asymptomatiques 0. IV Metronidazole. 3 patients 6.3 µg/g à 24 µg/g. Données cliniques publiées anecdotiques. Bolton RP et al – Gut 1986; 27:1169; Dion YM et al – Ann Surg 1980; 192:221; Johnson S et al – Ann Intern Med 1992; 117:297.")
28
PK Vancomycine Oral Vancomycine IV Vancomycine
Pos :125 mg X 4 > 3000 µg/g dans les selles Atteint la valve ileo-caecale en moins de 6 heures En cas d’ileus???? Pic retardé??? Posologies plus élevées IV Vancomycine Pepin J - Clin Infect Dis 2008; 46:1493; Johnson et al – Ann Intern Med 1992; 117:297; Tedesco F – Lancet :226

29
Vancomycine ou metronidazole: ERV?
Durée séjour C3G, FQ ERV C dif + +/- VAN IV VAN Per Os MET + +/-

30
Vancomycine ou metronidazole: ERV?
Quebec, épidemie de C dif O27 vancomycine per os conseillée 2002 2003 2004 ERV 106 275 554 Jette et al- Rapport 2004 Institut national de santé publique du Québec

31
Both Oral Metronidazole and Oral Vancomycin Promote Persistent Overgrowth of Vancomycin-Resistant Enterococci during Treatment of Clostridium difficile-Associated Disease Legend of the figure: FIG. 1. Concentration of VRE in stools of patients with preexisting VRE colonization who were treated with oral metronidazole versus oral vancomycin for C. difficile-associated disease. Day 0, before treatment on day of CDAD diagnosis. For the metronidazole group (n 37), the number of subjects monitored to 1 to 5 days, 6 to 10 days, 11 to 15 days, 16 to 20 days, and 21 to 25 days were 37, 28 (76%), 22 (59%), 19 (51%), and 16 (43%), respectively. For the vancomycin group (n 19), the number of subjects monitored to 1 to 5 days, 6 to 10 days, 11 to 15 days, 16 to 20 days, and 21 to 25 days were 19, 14 (74%), 11 (58%), 11 (58%), and 8 (42%), respectively. The durations of treatment (mean the SD) with metronidazole and vancomycin were and , respectively. Error bars indicate the standard error. For treatment of mild to moderate Clostridium difficile-associated disease (CDAD), oral metronidazole has been recommended as the preferred agent, in part due to concern that vancomycin may be more likely to promote colonization by vancomycin-resistant enterococci (VRE). We performed a prospective observational study to examine the effects of oral metronidazole or vancomycin treatment of CDAD on acquisition and concentration of VRE stool colonization. Before, during, and after 90 courses of CDAD therapy, stool samples were cultured for VRE, and the concentrations were quantified. Eighty-seven subjects (97%) had received antibiotics within the past month. For 56 treatment courses in which preexisting VRE colonization was present, metronidazole (n 37 courses) and vancomycin (n 19 courses), each promoted persistent VRE overgrowth during therapy, and the concentration decreased significantly in both groups by 2 weeks after completion of treatment (P <0.049). For 34 treatment courses in which baseline cultures were negative for VRE, new detection of VRE stool colonization occurred during 3 (14%) of the 22 courses of metronidazole and 1 (8%) of the 12 courses of vancomycin (P 1.0). These results demonstrate that both oral metronidazole and oral vancomycin promote the overgrowth of VRE during treatment of CDAD. New CDAD treatments are needed that are less likely to disrupt the intestinal microflora and promote overgrowth of healthcare-associated pathogens. Al-Nassir WN – AAC 2008; 2403
, the number of subjects monitored to 1 to 5 days, 6 to 10 days, 11. to 15 days, 16 to 20 days, and 21 to 25 days were 37, 28 (76%), 22. (59%), 19 (51%), and 16 (43%), respectively. For the vancomycin. group (n 19), the number of subjects monitored to 1 to 5 days, 6 to. 10 days, 11 to 15 days, 16 to 20 days, and 21 to 25 days were 19, 14. (74%), 11 (58%), 11 (58%), and 8 (42%), respectively. The durations. of treatment (mean the SD) with metronidazole and vancomycin. were and , respectively. Error bars indicate the. standard error. For treatment of mild to moderate Clostridium difficile-associated disease (CDAD), oral metronidazole has. been recommended as the preferred agent, in part due to concern that vancomycin may be more likely to. promote colonization by vancomycin-resistant enterococci (VRE). We performed a prospective observational. study to examine the effects of oral metronidazole or vancomycin treatment of CDAD on acquisition and. concentration of VRE stool colonization. Before, during, and after 90 courses of CDAD therapy, stool samples. were cultured for VRE, and the concentrations were quantified. Eighty-seven subjects (97%) had received. antibiotics within the past month. For 56 treatment courses in which preexisting VRE colonization was present, metronidazole (n 37 courses) and vancomycin (n 19 courses), each promoted persistent VRE overgrowth. during therapy, and the concentration decreased significantly in both groups by 2 weeks after completion of. treatment (P <0.049). For 34 treatment courses in which baseline cultures were negative for VRE, new. detection of VRE stool colonization occurred during 3 (14%) of the 22 courses of metronidazole and 1 (8%) of. the 12 courses of vancomycin (P 1.0). These results demonstrate that both oral metronidazole and oral. vancomycin promote the overgrowth of VRE during treatment of CDAD. New CDAD treatments are needed. that are less likely to disrupt the intestinal microflora and promote overgrowth of healthcare-associated. pathogens. Al-Nassir WN – AAC 2008;")
32
Vancomycine ou metronidazole: coûts?
Vanco suspension orale $ Mais Vanco IV $45 Metronidazole PO 10j $20 VANCOMYCINE 1G PDR LYO INJ : 3.21 VANCOMYCINE 125MG PDR LYO INJ : 1,79 VANCOMYCINE voie orale n’est plus commercialisée FLAGYL 4% SUSP BUV : 3.33 METRONIDAZOLE BBM 0,5% INJ FL 100ML : 0,39 Coûts CHU Grenoble VANCOMYCINE 1G PDR LYO INJ : 3.21€ VANCOMYCINE 125MG PDR LYO INJ : 1,79€ VANCOMYCINE voie orale n’est plus commercialisée FLAGYL 4% SUSP BUV : 3.33€ METRONIDAZOLE BBM 0,5% INJ FL 100ML : 0,39€ …

33
Traitement « classique » de la diarrhée à CD
Standard: Metronidazole per os pendant 7 à 10 jours 400 mg x 3/jour Option: Vancomycine per os, 7 à 10 jours 125 mg x 4/jour Doses plus élevées pour les épisodes sévères Standard (?) pour les patients avec albumine <25 g/l En USI La résistance clinique de CD au metronidazole et à la vancomycine n’est pas rapportée … mais le changement d’antibiotiques est recommandé par certains en cas de persistance des symptômes au delà d’une semaine
 pour les patients. avec albumine <25 g/l. En USI. La résistance clinique de CD au metronidazole et à la vancomycine n’est pas rapportée. … mais le changement d’antibiotiques est recommandé par certains en cas de persistance des symptômes au delà d’une semaine.")
34
Increasing Risk of Relapse after Treatment of Clostridium difficile Colitis in Quebec, Canada
Probabilities of recurrence among patients with Clostridium difficile associated diarrhea treated with only metronidazole, comparing to (top). Treatment with only vancomycin during to (bottom) Clinical Infectious Diseases 2005;40:
. Treatment with only vancomycin during to (bottom) Clinical Infectious Diseases 2005;40:")
35
Traitement des diarrhées à CD : échecs et rechutes/récidives
Aslam S et al. Lancet Infect Dis 2005; 5:

36
Peut-être partiellement liée au clone O27
Clinical Infectious Diseases 2005; 40:1598–1600 - Augmentation du taux de récidive sous metronidazole des études récentes par rapport aux études randomisées anciennes Peut-être partiellement liée à une population plus âgée et plus immunodéprimée Peut-être partiellement liée au clone O27 - Bien que l’efficacité de la vancomycine dans les études récentes semble inchangée Molécule sous surveillance

37
A Comparison of Vancomycin and Metronidazole for the Treatment of Clostridium difficile –Associated Diarrhea, Stratified by Disease Severity Zar – CID 2007 Monocentrique 8 ans 172 inclusions 150 analysables pour le CJP (87%)
")
38
172 inclusions 150 analysables pour le CJP (87%)
A Comparison of Vancomycin and Metronidazole for the Treatment of Clostridium difficile –Associated Diarrhea, Stratified by Disease Severity Monocentrique 8 ans 172 inclusions 150 analysables pour le CJP (87%) * Background. The incidence and severity of Clostridium difficile–associated diarrhea (CDAD) has been increasing, and there have been recent reports of metronidazole treatment failure. Metronidazole is still commonly used as first-line treatment for CDAD but has never been compared with vancomycin in a prospective, randomized, double-blind, placebo-controlled trial. We conducted such a trial, stratifying patients according to disease severity, to investigate whether one agent was superior for treating either mild or severe disease. Methods. From October 1994 through June 2002, patients with CDAD were stratified according to whether they had mild or severe disease based on clinical criteria and were randomly assigned to receive oral metronidazole (250 mg 4 times per day) or oral vancomycin (125 mg 4 times per day) for 10 days. Both groups received an oral placebo in addition to the study drug. Patients were followed up for 21 days to assess cure, treatment failure, relapse, or intolerance. Results. One hundred seventy-two patients were enrolled, and 150 of these patients successfully completed the trial. Among the patients with mild CDAD, treatment with metronidazole or vancomycin resulted in clinical cure in 90% and 98% of the patients, respectively ( ). Among the patients with severe CDAD, treatment with metronidazole or vancomycin resulted in clinical cure in 76% and 97% of the patients, respectively ( ). Clinical symptoms recurred in 15% of the patients treated with metronidazole and 14% of those treated with vancomycin. Conclusions. Our findings suggest that metronidazole and vancomycin are equally effective for the treatment of mild CDAD, but vancomycin is superior for treating patients with severe CDAD. Assessment of efficacy. The primary outcomes assessed were cure, treatment failure, and relapse. Cure was defined as resolution of diarrhea by day 6 of treatment and a negative result of a C. difficile toxin A assay at days 6 and 10 of treatment. Treatment failure was defined as persistence of diarrhea and/ or a positive result of a C. difficile toxin A assay after 6 days of treatment, the need for colectomy, or death after 5 days of therapy. Relapse was defined as recurrence of C. difficile toxin A–positive diarrhea by day 21 after initial cure. Intolerance was defined as the inability or refusal to continue the medication because of adverse reactions. Noncompliance was defined as missing 13 doses of the study medication during the 10 days of therapy for reasons other than intolerance. Lettres: la difference persiste si on tient compte des 13 exclus avant J6… Pas de recherche de O27 Pas de difference sur l’arret des antibiotiques .005 *:Resolution of diarrhea by day 6 of treatment and a negative result of a C. d toxin A assay at days 6 and 10 of treatment Relapse /66(14) 5/69 (7) 14/13 (10) Zar FA et al - CID 2007:45
 * Background. The incidence and severity of Clostridium difficile–associated diarrhea (CDAD) has been increasing, and there have been recent reports of metronidazole treatment failure. Metronidazole is still commonly used as first-line treatment for CDAD but has never been compared with vancomycin in a prospective, randomized, double-blind, placebo-controlled trial. We conducted such a trial, stratifying patients according to disease severity, to investigate whether one agent was superior for treating either mild or severe disease. Methods. From October 1994 through June 2002, patients with CDAD were stratified according to whether they had mild or severe disease based on clinical criteria and were randomly assigned to receive oral metronidazole (250 mg 4 times per day) or oral vancomycin (125 mg 4 times per day) for 10 days. Both groups received an oral placebo in addition to the study drug. Patients were followed up for 21 days to assess cure, treatment failure, relapse, or intolerance. Results. One hundred seventy-two patients were enrolled, and 150 of these patients successfully completed the trial. Among the patients with mild CDAD, treatment with metronidazole or vancomycin resulted in clinical cure in 90% and 98% of the patients, respectively ( ). Among the patients with severe CDAD, treatment with metronidazole or vancomycin resulted in clinical cure in 76% and 97% of the patients, respectively ( ). Clinical symptoms recurred in 15% of the patients treated with metronidazole and 14% of those treated with vancomycin. Conclusions. Our findings suggest that metronidazole and vancomycin are equally effective for the treatment of mild CDAD, but vancomycin is superior for treating patients with severe CDAD. Assessment of efficacy. The primary outcomes assessed. were cure, treatment failure, and relapse. Cure was defined as. resolution of diarrhea by day 6 of treatment and a negative. result of a C. difficile toxin A assay at days 6 and 10 of treatment. Treatment failure was defined as persistence of diarrhea and/ or a positive result of a C. difficile toxin A assay after 6 days. of treatment, the need for colectomy, or death after 5 days of. therapy. Relapse was defined as recurrence of C. difficile toxin. A–positive diarrhea by day 21 after initial cure. Intolerance was defined as the inability or refusal to continue. the medication because of adverse reactions. Noncompliance. was defined as missing 13 doses of the study medication during. the 10 days of therapy for reasons other than intolerance. Lettres: la difference persiste si on tient compte des 13 exclus avant J6… Pas de recherche de O27. Pas de difference sur l’arret des antibiotiques *:Resolution of diarrhea by day 6 of treatment and a negative result of a C. d toxin A assay at days 6 and 10 of treatment. Relapse 9/66(14) 5/69 (7) 14/13 (10) .27. Zar FA et al - CID 2007:45.")
39
Vanco or metronidazole?
Bishara et al- CID 2007:45 (15 December)
")
40
Metronidazole 1360 vs vancomycin 219, both 37
Quebec, , n=1616 Metronidazole 1360 vs vancomycin 219, both 37 Definition: Severe/complicated CDAD death d30, (b) septic shock, (c) megacolon, (d) perforation, or (e) emergency colectomy RF of S-CDAD: age>or=65 yr, male sex, immunosuppression, hospital acquisition, tube feeding, short duration of diarrhea, fever, elevated leukocytosis, or creatinine. Decrease in S-CDAD: (NAP1/O27) Adjusted risk of S-CDAD Vanco:AOR 0.21, 95% CI , P=0.048 Vanco: AOR 0.90, 95% CI , P=0.71 Am J Gastroenterol Dec;102(12): Epub 2007 Sep 26. Comment in: Am J Gastroenterol Dec;102(12): Am J Gastroenterol Aug;103(8):2147; author reply Outcomes of Clostridium difficile-associated disease treated with metronidazole or vancomycin before and after the emergence of NAP1/027. Pépin J, Valiquette L, Gagnon S, Routhier S, Brazeau I. Department of Microbiology and Infectious Diseases, University of Sherbrooke, Sherbrooke, Quebec, Canada. OBJECTIVE: To reassess the comparative efficacy of vancomycin versus metronidazole in the treatment of Clostridium difficile-associated disease (CDAD) after the emergence in 2003 of the hypervirulent NAP1/027 strain. METHODS: A retrospective cohort study was conducted in a tertiary-care Canadian hospital among 1,616 patients treated initially with metronidazole (N=1,360), vancomycin (N=219), or both (N=37), between 1991 and 2006, and followed for 60 days after diagnosis. Primary outcome was severe/complicated CDAD (SC-CDAD) defined as any of: (a) death within 30 days, (b) septic shock, (c) megacolon, (d) perforation, or (e) emergency colectomy. Adjusted odds ratios (AOR) and their 95% confidence intervals (CI) were calculated, stratifying into pre-epidemic ( ) and epidemic ( ) periods. Secondary outcome was recurrence within 60 days. RESULTS: Risk factors for SC-CDAD were the same in both periods: age>or=65 yr, male sex, immunosuppression, hospital acquisition, tube feeding, short duration of diarrhea, fever, elevated leukocytosis, or creatinine. Adjusting for confounders and using metronidazole therapy as baseline, vancomycin therapy was associated with a lower probability of developing SC-CDAD in (AOR 0.21, 95% CI , P=0.048) but not during (AOR 0.90, 95% CI , P=0.71). For both metronidazole and vancomycin, risk of recurrence increased in but decreased in CONCLUSIONS: Loss of superiority of vancomycin over metronidazole coincided with the emergence of NAP1/027. Toxin hyperproduction by NAP1/027 might be such that the disease follows its natural course. Novel therapeutic approaches are needed. The higher risk of recurrence in probably reflected reinfections rather than relapses. Pepin J et al - Am J Gastroenterol Dec;102(12):2781-8
 septic shock, (c) megacolon, (d) perforation, or (e) emergency colectomy. RF of S-CDAD: age>or=65 yr, male sex, immunosuppression, hospital acquisition, tube feeding, short duration of diarrhea, fever, elevated leukocytosis, or creatinine. Decrease in S-CDAD: (NAP1/O27) Adjusted risk of S-CDAD Vanco:AOR 0.21, 95% CI , P= Vanco: AOR 0.90, 95% CI , P=0.71. Am J Gastroenterol Dec;102(12): Epub 2007 Sep 26. Comment in: Am J Gastroenterol Dec;102(12): Am J Gastroenterol Aug;103(8):2147; author reply Outcomes of Clostridium difficile-associated disease treated with metronidazole or vancomycin before and after the emergence of NAP1/027. Pépin J, Valiquette L, Gagnon S, Routhier S, Brazeau I. Department of Microbiology and Infectious Diseases, University of Sherbrooke, Sherbrooke, Quebec, Canada. OBJECTIVE: To reassess the comparative efficacy of vancomycin versus metronidazole in the treatment of Clostridium difficile-associated disease (CDAD) after the emergence in 2003 of the hypervirulent NAP1/027 strain. METHODS: A retrospective cohort study was conducted in a tertiary-care Canadian hospital among 1,616 patients treated initially with metronidazole (N=1,360), vancomycin (N=219), or both (N=37), between 1991 and 2006, and followed for 60 days after diagnosis. Primary outcome was severe/complicated CDAD (SC-CDAD) defined as any of: (a) death within 30 days, (b) septic shock, (c) megacolon, (d) perforation, or (e) emergency colectomy. Adjusted odds ratios (AOR) and their 95% confidence intervals (CI) were calculated, stratifying into pre-epidemic ( ) and epidemic ( ) periods. Secondary outcome was recurrence within 60 days. RESULTS: Risk factors for SC-CDAD were the same in both periods: age>or=65 yr, male sex, immunosuppression, hospital acquisition, tube feeding, short duration of diarrhea, fever, elevated leukocytosis, or creatinine. Adjusting for confounders and using metronidazole therapy as baseline, vancomycin therapy was associated with a lower probability of developing SC-CDAD in (AOR 0.21, 95% CI , P=0.048) but not during (AOR 0.90, 95% CI , P=0.71). For both metronidazole and vancomycin, risk of recurrence increased in but decreased in CONCLUSIONS: Loss of superiority of vancomycin over metronidazole coincided with the emergence of NAP1/027. Toxin hyperproduction by NAP1/027 might be such that the disease follows its natural course. Novel therapeutic approaches are needed. The higher risk of recurrence in probably reflected reinfections rather than relapses. Pepin J et al - Am J Gastroenterol Dec;102(12):")
41
Gerdings et al – Clin Infect Dis 2008; 46:S32
Age > T > 38°3C 1 Alb < 25g/l 1 WBC > 15000/mm3 1 Pseudomembranes 2 ICU 2 *: Total 2 Gerdings et al – Clin Infect Dis 2008; 46:S32

42
Nitazoxanide et diarrhée à CD
Nitrothiazolide CMI mg/l Excrétion de 2/3 dose dans les fèces activité comparable au metronidazole Musher DM et al. CID 2006; 43: 421-7 Après un echec Metronidazole (pas d’amélioration clinique à 14 j): 26/35 réponse au traitement 19/35 guérison Musher DM et al – JAC 2007; Anti helminthique et anti protozoaire
: 26/35 réponse au traitement. 19/35 guérison. Musher DM et al – JAC 2007; Anti helminthique et anti protozoaire.")
43
Nitazoxanide vs Vancomycine
N=49 (27 V;22 N) Response 20/27(74%) V and 17/22(77%) N Day 31 disease free 20/23 (86%) V 17/18 (95%) N Relapse 2 V, vs 1 N Sustained response rates 18/27(67%) V vs. 16 of 22 (73%) N Musher D et al – 48th ICAAC 2008 – K524b
 Response. 20/27(74%) V and 17/22(77%) N. Day 31 disease free. 20/23 (86%) V 17/18 (95%) N. Relapse. 2 V, vs 1 N. Sustained response rates. 18/27(67%) V vs. 16 of 22 (73%) N. Musher D et al – 48th ICAAC 2008 – K524b.")
44
Vancomycine vs Tolevamer
Polymère anionique soluble capable de fixer les toxines A et B Arret de la diarrhée à 48 h: Vanco 500: 73/80 91% Tolevamer 6g: 58/70 83% Tolevamer 3g: 48/72 67% Louie TJ et al. CID 2006; 43:

45
Tolevamer vs Vanco : effets 2aires
Louie TJ et al. CID 2006; 43:

46
Tolevamer (étude phase III)
Phase III : 1100 pts, 300 sites, double aveugle Tolevamer (9g forme liquide) vs Metronidazole (1.5g) et Vancomycine (500mg) (2:1:1) Critère ppal : résolution des diarrhées à CD à J10 528 pat (268T, 125 V, 135 M) Formes sévères: 25%, récurrentes 17% Succès clinique: T 42% (112/268), V 81% (101/125), M 73% (99/135) Récurrence: T 6%, V 18%, M 19% Infériorité vs les 2 antibiotiques de référence Bouza E et al – 18th ECCMID Avr 2008
 vs Metronidazole (1.5g) et Vancomycine (500mg) (2:1:1) Critère ppal : résolution des diarrhées à CD à J pat (268T, 125 V, 135 M) Formes sévères: 25%, récurrentes 17% Succès clinique: T 42% (112/268), V 81% (101/125), M 73% (99/135) Récurrence: T 6%, V 18%, M 19% Infériorité vs les 2 antibiotiques de référence. Bouza E et al – 18th ECCMID Avr")
47
McFarland et al., JAMA; 271, 1913-1918, (1994).
OBJECTIVE--To determine the safety and efficacy of a new combination treatment for patients with Clostridium difficile-associated disease (CDD). The treatment combines the yeast Saccharomyces boulardii with an antibiotic (vancomycin hydrochloride or metronidazole). DESIGN--A double-blind, randomized, placebo-controlled, parallel-group intervention study in patients with active CDD. Patients received standard antibiotics and S boulardii or placebo for 4 weeks, and were followed up for an additional 4 weeks after therapy. Effectiveness was determined by comparing the recurrence of CDD in the two groups using multivariate analysis to control for other risk factors for CDD. SETTING--National referral study of ambulatory or hospitalized patients from three main study coordinating centers. PATIENTS--A total of 124 eligible consenting adult patients, including 64 who were enrolled with an initial episode of CDD, and 60 who had a history of at least one prior CDD episode. Patients who were immunosuppressed due to acquired immunodeficiency syndrome or cancer chemotherapy within 3 months were not eligible. INTERVENTION--Treatment with oral S boulardii (1 g/d for 4 weeks) or placebo in combination with a standard antibiotic. MAIN OUTCOME MEASURE--Recurrence of active CDD. RESULTS--A history of CDD episodes dramatically increased the likelihood of further recurrences. Multivariate analysis revealed that patients treated with S boulardii and standard antibiotics had a significantly lower relative risk (RR) of CDD recurrence (RR, 0.43; 95% confidence interval, 0.20 to 0.97) compared with placebo and standard antibiotics. The efficacy of S boulardii was significant (recurrence rate 34.6%, compared with 64.7% on placebo; P = .04) in patients with recurrent CDD, but not in patients with initial CDD (recurrence rate 19.3% compared with 24.2% on placebo; P = .86). There were no serious adverse reactions associated with S boulardii. CONCLUSIONS--The combination of standard antibiotics and S boulardii was shown to be an effective and safe therapy for these patients with recurrent CDD; no benefit of S boulardii was demonstrated for those with an initial episode of CDD.
. The treatment combines the yeast Saccharomyces boulardii with an antibiotic (vancomycin hydrochloride or metronidazole). DESIGN--A double-blind, randomized, placebo-controlled, parallel-group intervention study in patients with active CDD. Patients received standard antibiotics and S boulardii or placebo for 4 weeks, and were followed up for an additional 4 weeks after therapy. Effectiveness was determined by comparing the recurrence of CDD in the two groups using multivariate analysis to control for other risk factors for CDD. SETTING--National referral study of ambulatory or hospitalized patients from three main study coordinating centers. PATIENTS--A total of 124 eligible consenting adult patients, including 64 who were enrolled with an initial episode of CDD, and 60 who had a history of at least one prior CDD episode. Patients who were immunosuppressed due to acquired immunodeficiency syndrome or cancer chemotherapy within 3 months were not eligible. INTERVENTION--Treatment with oral S boulardii (1 g/d for 4 weeks) or placebo in combination with a standard antibiotic. MAIN OUTCOME MEASURE--Recurrence of active CDD. RESULTS--A history of CDD episodes dramatically increased the likelihood of further recurrences. Multivariate analysis revealed that patients treated with S boulardii and standard antibiotics had a significantly lower relative risk (RR) of CDD recurrence (RR, 0.43; 95% confidence interval, 0.20 to 0.97) compared with placebo and standard antibiotics. The efficacy of S boulardii was significant (recurrence rate 34.6%, compared with 64.7% on placebo; P = .04) in patients with recurrent CDD, but not in patients with initial CDD (recurrence rate 19.3% compared with 24.2% on placebo; P = .86). There were no serious adverse reactions associated with S boulardii. CONCLUSIONS--The combination of standard antibiotics and S boulardii was shown to be an effective and safe therapy for these patients with recurrent CDD; no benefit of S boulardii was demonstrated for those with an initial episode of CDD.")
48
Gerdings et al – Clin Infect Dis 2008; 46:S32
Age > 60 – 1 T > 38°3C – 1 Alb < 25g/l – 1 WBC > 15000/mm3 – 1 Pseudomembranes– 2 ICU - 2 *: Total 2 Gerdings et al – Clin Infect Dis 2008; 46:S32

49
Colites pseudo-membraneuses fulminantes à Clostridium difficile
Étude rétrospective, CHU Sherbrooke et hôpital Maisonneuve-Rosemont (Québec) 165 patients admis en réanimation pour une colite pseudo-membraneuse Mortalité à 30 jours 87/165 (53 %) 38 des 87 décès (44 %) dans les 48 heures suivant l’admission en réanimation Intérêt de la colectomie ? La mortalité des colites à Clostridium difficile ribotype 027 est élevée (27 % au 1er septembre 2006 en France). Une partie de ces décès est directement attribuable au C. difficile, avec des tableaux de choc septique ou de colite fulminante. Le traitement de ces tableaux est mal codifié, notamment en ce qui concerne le traitement chirurgical « de sauvetage » (colectomie). Jacques Pépin a étudié 165 patients consécutifs admis en réanimation pour une colite fulminante à C. difficile. La mortalité de ces formes est très élevée (53 %) et précoce : 44 % des décès surviennent dans les 48 premières heures de réanimation. Lamontagne F et al. Ann Surg 2007; 245:
 165 patients admis en réanimation pour une colite pseudo-membraneuse. Mortalité à 30 jours. 87/165 (53 %) 38 des 87 décès (44 %) dans les 48 heures suivant l’admission en réanimation. Intérêt de la colectomie La mortalité des colites à Clostridium difficile ribotype 027 est élevée (27 % au 1er septembre 2006 en France). Une partie de ces décès est directement attribuable au C. difficile, avec des tableaux de choc septique ou de colite fulminante. Le traitement de ces tableaux est mal codifié, notamment en ce qui concerne le traitement chirurgical « de sauvetage » (colectomie). Jacques Pépin a étudié 165 patients consécutifs admis en réanimation pour une colite fulminante à C. difficile. La mortalité de ces formes est très élevée (53 %) et précoce : 44 % des décès surviennent dans les 48 premières heures de réanimation. Lamontagne F et al. Ann Surg 2007; 245:")
50
Colectomie et CPM age 75 years AOR, 6.5; 95% CI, 1.7–24.3
immunosuppression AOR, 7.9; 95% CI, 2.3–27.2 shock requiring vasopressors AOR, 3.4; 95% CI,1.3– 8.7 leukocytosis 50 X 109/L AOR, 18.6; 95% CI, 3.7–94.7 lactate 5 mmol/L AOR, 12.4; 95% CI, 2.4–63.7 Objectives: To determine whether emergency colectomy reduces mortality in patients with fulminant Clostridium difficile-associated disease (CDAD), and to identify subgroups of patients more likely to benefit from the procedure. Summary Background Data: Many hospitals in Quebec, Canada, have noted since 2003 a dramatic increase in CDAD incidence and in the proportion of cases severe enough to require intensive care unit (ICU) admission. The decision to perform an emergency colectomy remains largely empirical. Methods: Retrospective observational cohort study of 165 cases of CDAD that required ICU admission or prolongation of ICU stay between January 2003 and June 2005 in 2 tertiary care hospitals of Quebec. Multivariate analysis was performed through logistic regression; adjusted odds ratios (AOR) and their 95% confidence intervals (CI) were calculated. The primary outcome was mortality within 30 days of ICU admission. Results: Eighty-seven (53%) cases resulted in death within 30 days of ICU admission, almost half (38 of 87, 44%) within 48 hours of ICU admission. The independent predictors of 30-day mortality were: leukocytosis /L (AOR, 18.6; 95% CI, 3.7–94.7), lactate 5 mmol/L (AOR, 12.4; 95% CI, 2.4–63.7), age 75 years (AOR, 6.5; 95% CI, 1.7–24.3), immunosuppression (AOR, 7.9; 95% CI, 2.3–27.2) and shock requiring vasopressors (AOR, 3.4; 95% CI, 1.3– 8.7). After adjustment for these confounders, patients who had an emergency colectomy were less likely to die (AOR, 0.22; 95% CI, 0.07– 0.67, P ) than those treated medically. Colectomy seemed more beneficial in patients aged 65 years or more, in those immunocompetent, those with a leukocytosis /L or lactate between 2.2 and 4.9 mmol/L. Conclusion: Emergency colectomy reduces mortality in some patients with fulminant CDAD. (Ann Surg 2007;245: 267–272) Emergency colectomy were less likely to die AOR, 0.22; 95%CI, 0.07– 0.67, P =0.008 Lamontagne F et al. Ann Surg 2007; 245:
, and to identify subgroups of patients more likely. to benefit from the procedure. Summary Background Data: Many hospitals in Quebec, Canada, have noted since 2003 a dramatic increase in CDAD incidence and. in the proportion of cases severe enough to require intensive care. unit (ICU) admission. The decision to perform an emergency colectomy. remains largely empirical. Methods: Retrospective observational cohort study of 165 cases of. CDAD that required ICU admission or prolongation of ICU stay. between January 2003 and June 2005 in 2 tertiary care hospitals of. Quebec. Multivariate analysis was performed through logistic regression; adjusted odds ratios (AOR) and their 95% confidence. intervals (CI) were calculated. The primary outcome was mortality. within 30 days of ICU admission. Results: Eighty-seven (53%) cases resulted in death within 30 days. of ICU admission, almost half (38 of 87, 44%) within 48 hours of. ICU admission. The independent predictors of 30-day mortality. were: leukocytosis /L (AOR, 18.6; 95% CI, 3.7–94.7), lactate 5 mmol/L (AOR, 12.4; 95% CI, 2.4–63.7), age 75 years. (AOR, 6.5; 95% CI, 1.7–24.3), immunosuppression (AOR, 7.9; 95% CI, 2.3–27.2) and shock requiring vasopressors (AOR, 3.4; 95% CI, 1.3– 8.7). After adjustment for these confounders, patients who had. an emergency colectomy were less likely to die (AOR, 0.22; 95% CI, 0.07– 0.67, P 0.008) than those treated medically. Colectomy. seemed more beneficial in patients aged 65 years or more, in those. immunocompetent, those with a leukocytosis /L or. lactate between 2.2 and 4.9 mmol/L. Conclusion: Emergency colectomy reduces mortality in some patients. with fulminant CDAD. (Ann Surg 2007;245: 267–272) Emergency colectomy were less likely to die AOR, 0.22; 95%CI, 0.07– 0.67, P = Lamontagne F et al. Ann Surg 2007; 245:")
51
Réponse immunitaire anti-toxine A et Evolution clinique de l’ICD
Maroo P et al. Gastroenterology 2006; 130:

52
Sougioultzis S et al. Gastroenterology 2005; 128: 764-70

53
Mab anti-toxine A vs placebo
Données animales encourageantes (Babcock AAC 2006; 6339) Ac monoclonal anti Cdta 10 mg/kg 1 fois J0 Phase II – Patients traités pour CDAD 29 Mab vs 17 Pb Recurence: 17 vs 18%; NS Anti-toxin B significantly lower in case of recurrence phase II combination anti-toxin A and B ongoing B-1925 Serum Anti-Toxin B Antibody Correlates with Protection from Recurrent Clostridium difficile Associated Diarrhea (CDAD) B. LEAV1, B. BLAIR 1, C. REILLY 1, I. LOWY 2, D. AMBROSINO 1; 1Massachusetts Biologic Lab., Boston, MA, 2Medarex, Inc., Bloomsbury, NJ. Background: Previous studies have demonstrated a correlation between C. difficile anti-toxin A serum antibodies and protection against symptomatic disease and recurrence. Methods:A neutralizing monoclonal antibody (MAb) to C. difficile toxin A (CDA1) developed by MBL and Medarex, Inc. was studied in a phase II, randomized, double blind, placebo-controlled trial in patients receiving standard of care treatment for CDAD. Subjects received a single intravenous infusion of 10mg/kg CDA1 or placebo on day 0 of the study and were evaluated for recurrence of CDAD during the 56 day study period. Serum samples were obtained prior to and after infusion to measure anti-toxin A and B antibody concentrations and specific neutralizing activity. Results: 29 patients received CDA1 and 17 received placebo. Recurrence occurred in 17% in the CDA1 group and 18% in the placebo group with a trend toward delay in time to recurrence in the group treated with CDA1. Geometric mean concentrations by ELISA (0.3 vs. 1.2 µg/ml, P= 0.02) and neutralizing titers (6 vs. 107, P=0.003) of anti-toxin B antibody at day 28 were significantly lower for subjects with recurrence compared to those who did not recur. In a multiple logistic regression analysis both anti-toxin A (trend) and anti-toxin B (P=0.02) correlated with protection from recurrence. Conclusion: In this prospective study, recurrence of CDAD was associated with significantly lower concentrations and neutralizing activity of anti-toxin B antibody. These results are consistent with our data from animal studies that demonstrate that antibodies to both toxins optimally protect against recurrence. A phase II clinical trial with a combination of anti-toxin A and B human MAbs is currently underway in patients with CDAD as adjunctive treatment and for prevention of recurrence. Leav B et al – 48th ICAAC 2008– B-1925 Medarex, Inc
 Ac monoclonal anti Cdta 10 mg/kg 1 fois J0. Phase II – Patients traités pour CDAD. 29 Mab vs 17 Pb. Recurence: 17 vs 18%; NS. Anti-toxin B significantly lower in case of recurrence. phase II combination anti-toxin A and B ongoing. B Serum Anti-Toxin B Antibody Correlates with Protection from Recurrent Clostridium difficile Associated Diarrhea (CDAD) B. LEAV1, B. BLAIR 1, C. REILLY 1, I. LOWY 2, D. AMBROSINO 1; 1Massachusetts Biologic Lab., Boston, MA, 2Medarex, Inc., Bloomsbury, NJ. Background: Previous studies have demonstrated a correlation between C. difficile anti-toxin A serum antibodies and protection against symptomatic disease and recurrence. Methods:A neutralizing monoclonal antibody (MAb) to C. difficile toxin A (CDA1) developed by MBL and Medarex, Inc. was studied in a phase II, randomized, double blind, placebo-controlled trial in patients receiving standard of care treatment for CDAD. Subjects received a single intravenous infusion of 10mg/kg CDA1 or placebo on day 0 of the study and were evaluated for recurrence of CDAD during the 56 day study period. Serum samples were obtained prior to and after infusion to measure anti-toxin A and B antibody concentrations and specific neutralizing activity. Results: 29 patients received CDA1 and 17 received placebo. Recurrence occurred in 17% in the CDA1 group and 18% in the placebo group with a trend toward delay in time to recurrence in the group treated with CDA1. Geometric mean concentrations by ELISA (0.3 vs. 1.2 µg/ml, P= 0.02) and neutralizing titers (6 vs. 107, P=0.003) of anti-toxin B antibody at day 28 were significantly lower for subjects with recurrence compared to those who did not recur. In a multiple logistic regression analysis both anti-toxin A (trend) and anti-toxin B (P=0.02) correlated with protection from recurrence. Conclusion: In this prospective study, recurrence of CDAD was associated with significantly lower concentrations and neutralizing activity of anti-toxin B antibody. These results are consistent with our data from animal studies that demonstrate that antibodies to both toxins optimally protect against recurrence. A phase II clinical trial with a combination of anti-toxin A and B human MAbs is currently underway in patients with CDAD as adjunctive treatment and for prevention of recurrence. Leav B et al – 48th ICAAC 2008– B Medarex, Inc.")
54
Jul 06-April 08, 30 centres, US and Canada Phase II double-blind trial
10 mg CDA-1-10 mg CD-B1 vs Placebo Primary end point: 1st laboratory documented relapse Secondary end-points Number of days to the resolution of the initial episode Failure of ABx initial treatment Level of antibodies Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, 2010 Medarex, Inc
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, Medarex, Inc.")
55
Lowy et al - N Engl J Med 362;3 january 21, 2010
Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, 2010 Medarex, Inc
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, Medarex, Inc.")
56
Lowy et al - N Engl J Med 362;3 january 21, 2010
Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, 2010 Medarex, Inc
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, Medarex, Inc.")
57
« half-life of the terminal portion of the disposition phase was 26±8
« half-life of the terminal portion of the disposition phase was 26±8.4 days for antitoxin A and 22±13 days for antitoxin B » Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, 2010 Medarex, Inc
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, Medarex, Inc.")
58
Lowy et al - N Engl J Med 362;3 january 21, 2010
Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, 2010 Medarex, Inc
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, Medarex, Inc.")
59
Resolution of the 1st episode
No difference in the time of resolution of the 1st episode (at least 5 unformed stools for at least 2 consecutive days) Death 7 (Ab) vs 8 (Pb), p=0.79 Death due to Cdif 0(Ab) vs 2 (Pb), NS
 Death 7 (Ab) vs 8 (Pb), p=0.79. Death due to Cdif 0(Ab) vs 2 (Pb), NS.")
60
Lowy et al - N Engl J Med 362;3 january 21, 2010
Chez les inatients, plus de maladies chronique et colite plutot moins severe… Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, 2010 Medarex, Inc
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) Lowy et al - N Engl J Med 362;3 january 21, Medarex, Inc.")
61
(*) during the 84 days study period
Background New therapies are needed to manage the increasing incidence, severity, and high rate of recurrence of Clostridium difficile infection. Methods We performed a randomized, double-blind, placebo-controlled study of two neutralizing, fully human monoclonal antibodies against C. difficile toxins A (CDA1) and B (CDB1). The antibodies were administered together as a single infusion, each at a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile infection who were receiving either metronidazole or vancomycin. The primary outcome was laboratory-documented recurrence of infection during the 84 days after the administration of monoclonal antibodies or placebo. Results Among the 200 patients who were enrolled (101 in the antibody group and 99 in the placebo group), the rate of recurrence of C. difficile infection was lower among patients treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027 strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial hospitalization for inpatients did not differ significantly between the antibody and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event was reported by 18 patients in the antibody group and by 28 patients in the placebo group (P = 0.09). Conclusions The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) (*) during the 84 days study period Lowy et al - N Engl J Med 362;3 january 21, 2010
 and. B (CDB1). The antibodies were administered together as a single infusion, each at. a dose of 10 mg per kilogram of body weight, in patients with symptomatic C. difficile. infection who were receiving either metronidazole or vancomycin. The primary outcome. was laboratory-documented recurrence of infection during the 84 days after. the administration of monoclonal antibodies or placebo. Results. Among the 200 patients who were enrolled (101 in the antibody group and 99 in the. placebo group), the rate of recurrence of C. difficile infection was lower among patients. treated with monoclonal antibodies (7% vs. 25%; 95% confidence interval, 7 to 29; P<0.001). The recurrence rates among patients with the epidemic BI/NAP1/027. strain were 8% for the antibody group and 32% for the placebo group (P = 0.06); among patients with more than one previous episode of C. difficile infection, recurrence. rates were 7% and 38%, respectively (P = 0.006). The mean duration of the initial. hospitalization for inpatients did not differ significantly between the antibody. and placebo groups (9.5 and 9.4 days, respectively). At least one serious adverse event. was reported by 18 patients in the antibody group and by 28 patients in the placebo. group (P = 0.09). Conclusions. The addition of monoclonal antibodies against C. difficile toxins to antibiotic agents. significantly reduced the recurrence of C. difficile infection. (ClinicalTrials.gov number, NCT ) (*) during the 84 days study period. Lowy et al - N Engl J Med 362;3 january 21,")
63
Rôle des antibiotiques dans la survenue d’infections à C. difficile
Bignardi et al., JHI, 1998

64
Pear, S. M. et. al. Ann Intern Med 1994;120:272-277
Number of cases of Clostridium difficile-associated diarrhea detected each month before and after clindamycin restriction Suzanne Climo and colleages at the VA Medical Center in Tucson Arizona. Figure 1. Number of cases of Clostridium difficile-associated diarrhea detected each month before and after clindamycin restriction. The epidemic period is shown in black bars and the pre- and postepidemic periods by white bars. The dotted horizontal line represents a historical threshold of 2 SD above the mean. The number of type J7 isolates (identified using restriction endonuclease analysis) compared with the number tested are shown below the bars. Pear, S. M. et. al. Ann Intern Med 1994;120:
 compared with the number tested are shown below the bars. Pear, S. M. et. al. Ann Intern Med 1994;120:")
65
TRANSMISSION DE C. DIFFICILE
Manuportée +++ Directe (personnels) ou indirecte (matériels, environnement) Favorisée par : La diarrhée (dissémination du germe) : C. difficile est retrouvé dans 49 % des chambres de patients diarrhéiques vs 29% dans celles de patients non diarrhéiques La résistance des spores dans l'environnement La promiscuité des patients : l'acquisition de C. difficile est rapide (3,2 j) si le patient voisin est porteur La pression antibiotique MacFarland LV, NEJM 1989, 320,
 ou indirecte (matériels, environnement) Favorisée par : La diarrhée (dissémination du germe) : C. difficile est retrouvé dans 49 % des chambres de patients diarrhéiques vs 29% dans celles de patients non diarrhéiques. La résistance des spores dans l environnement. La promiscuité des patients : l acquisition de C. difficile est rapide (3,2 j) si le patient voisin est porteur. La pression antibiotique. MacFarland LV, NEJM 1989, 320,")
66
C. DIFFICILE et ENVIRONNEMENT
Réservoirs Statut du patient CD neg. CD asympt. CD symptom. Total - lits (39%) - vitres (30 %) - sols (36 %) - boutons d'appel (30%) - toilettes (18%) - autres (49%) Total (N=216) 7 (8%) (29%) (49%) 62 (29%) McFarland,NEJM 1989
 - vitres (30 %) - sols (36 %) - boutons d appel (30%) - toilettes (18%) - autres (49%) Total (N=216) 7 (8%) 11 (29%) 44 (49%) 62 (29%) McFarland,NEJM")
67
Effet de la décontamination des chambres à l’eau de Javel® sur la colonisation des surfaces par Clostridium difficile Sommier Table de chevet Téléphone Sonnette Toilettes Poignée de porte Avant le ménage Ménage standard (eau de Javel®) Ménage renforcé 10 20 30 40 50 60 70 Taux de cultures positives Lors de l’épidémie de Clostridium difficile ribotype 027 au Québec, les auteurs de cette étude se sont posé la question de la persistance de C. difficile après une désinfection de la chambre à l’eau de Javel® lors de la sortie des patients infectés. Un lavage « standard » de la chambre par l’équipe paramédicale n’avait que peu d’effet sur la colonisation des surfaces. En revanche, un nettoyage « à fond », effectué de manière spécifique pour les patients infectés par le C. difficile, en laissant les surfaces sécher après application de l’eau de Javel®, permettait de diminuer très significativement le taux de positivité des cultures. À la suite de cette étude, du temps supplémentaire a été attribué aux équipes de ménage pour la désinfection des chambres. ICAAC D’après J. Pépin, communication orale 539
 Ménage renforcé Taux de cultures positives. Lors de l’épidémie de Clostridium difficile ribotype 027 au Québec, les auteurs de cette étude se sont posé la question de la persistance de C. difficile après une désinfection de la chambre à l’eau de Javel® lors de la sortie des patients infectés. Un lavage « standard » de la chambre par l’équipe paramédicale n’avait que peu d’effet sur la colonisation des surfaces. En revanche, un nettoyage « à fond », effectué de manière spécifique pour les patients infectés par le C. difficile, en laissant les surfaces sécher après application de l’eau de Javel®, permettait de diminuer très significativement le taux de positivité des cultures. À la suite de cette étude, du temps supplémentaire a été attribué aux équipes de ménage pour la désinfection des chambres. ICAAC D’après J. Pépin, communication orale 539.")
68
13 C. difficile et Hygiène des mains Pourcentage de réduction bactérienne des quatre produits log Barbut et coll., Hygiènes 2003

69
All with a previous CDAD
Skin contamination 73 patients from long-term facilities 68 patients no signs 5 patients CDAD 78% skin contamination 20% skin contamination All with a previous CDAD 33 patients not carriers 35 patients carriers 60% skin contamination 22 non epidemic 13 O27 Riggs M - SHEA 2007

70
3. dès le diagnostic rapide d’ICD réalisé
1. d’évoquer le diagnostic si diarrhée post-AB ou iléus, douleurs abdominales et d’hyperleucocytose 2. Surveillance active de C. dif si adulte >48h d’hospitalisation (toxines A et B) 3. dès le diagnostic rapide d’ICD réalisé précautions « standard » et précautions complémentaires d’hygiène de type « contact ». notamment de porter une surblouse à manches longues si contacts directs 4. de pratiquer l’hygiène des mains + gants: en entrant:SHA puis gants à UU en sortant: ablation gants + lavage simple mains séchage complet puis SHA
 3. dès le diagnostic rapide d’ICD réalisé. précautions « standard » et précautions complémentaires d’hygiène de type « contact ». notamment de porter une surblouse à manches longues si contacts directs. 4. de pratiquer l’hygiène des mains + gants: en entrant:SHA puis gants à UU. en sortant: ablation gants + lavage simple mains. séchage complet puis SHA.")
71
Dans l’environnement du patient 8. Réduire le réservoir des spores
6. Désinfection fécale 7. d’arrêter l’antibiotique responsable et de débuter systématiquement un traitement par metronidazole(1g/j) en première intention, Dans l’environnement du patient 8. Réduire le réservoir des spores bio nettoyage au moins quotidien des sols et des surfaces impérativement : - un nettoyage complet (détersion, rinçage) avec du matériel à usage unique, terminé par un séchage passif ; - suivi d’une désinfection à l'aide d’une solution d'hypochlorite de sodium à 0,5% de chlore actif, (10 minutes mini) 9. Petit matériel à UU ou (stéthoscope, brassard à tension, thermomètre, flacons d’antiseptique…) maintenu en permanence dans sa chambre jusqu’à la levée des mesures
 en première intention, Dans l’environnement du patient. 8. Réduire le réservoir des spores. bio nettoyage au moins quotidien des sols et des surfaces. impérativement : - un nettoyage complet (détersion, rinçage) avec du matériel à usage unique, terminé par un séchage passif ; - suivi d’une désinfection à l aide d’une solution d hypochlorite de sodium à 0,5% de chlore actif, (10 minutes mini) 9. Petit matériel à UU ou (stéthoscope, brassard à tension, thermomètre, flacons d’antiseptique…) maintenu en permanence dans sa chambre jusqu’à la levée des mesures.")
72
Des mesures générales - d’informer, signalisation claire, isolement géographique chambres individuelles +- cohorting jusqu’à l’arret des diarrhées -limiter les déplacements et les tranferts de maintenir les mesures d’isolement géographique et l’application des précautions « contact » Bactériologie - Isolement des souches si ICD severe + envoi au CNR (O27) - prévenir UHLIN - signalement DDASS et Cclin des formes severes et épidémies - jamais de dépistage systématique, jms de traitement des porteurs sains
 - prévenir UHLIN. - signalement DDASS et Cclin des formes severes et épidémies. - jamais de dépistage systématique, jms de traitement des porteurs sains.")
Présentations similaires

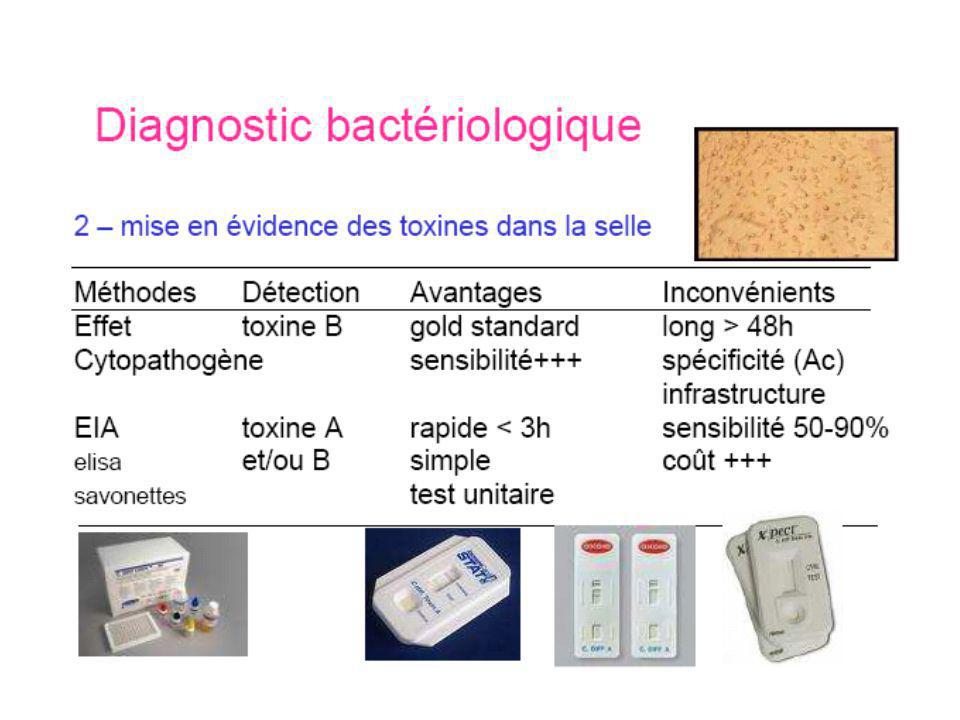
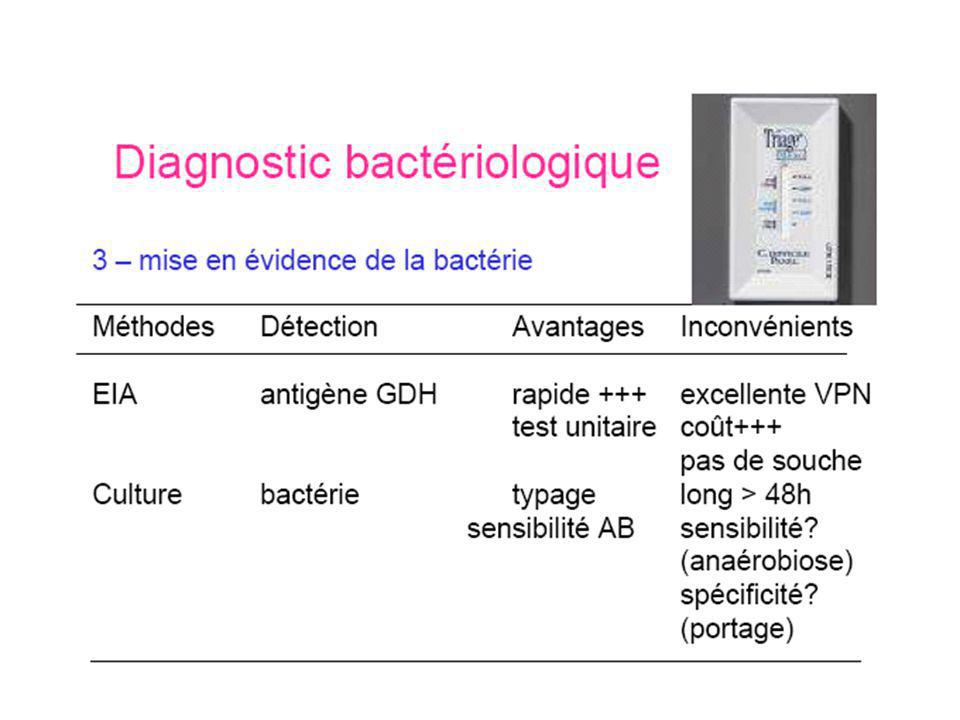
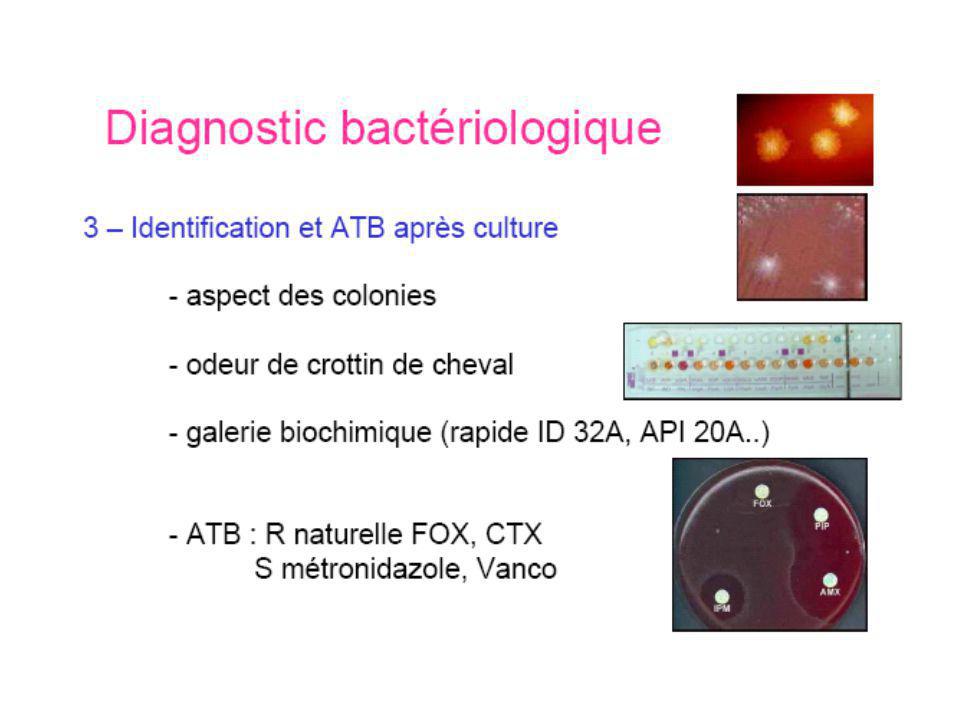
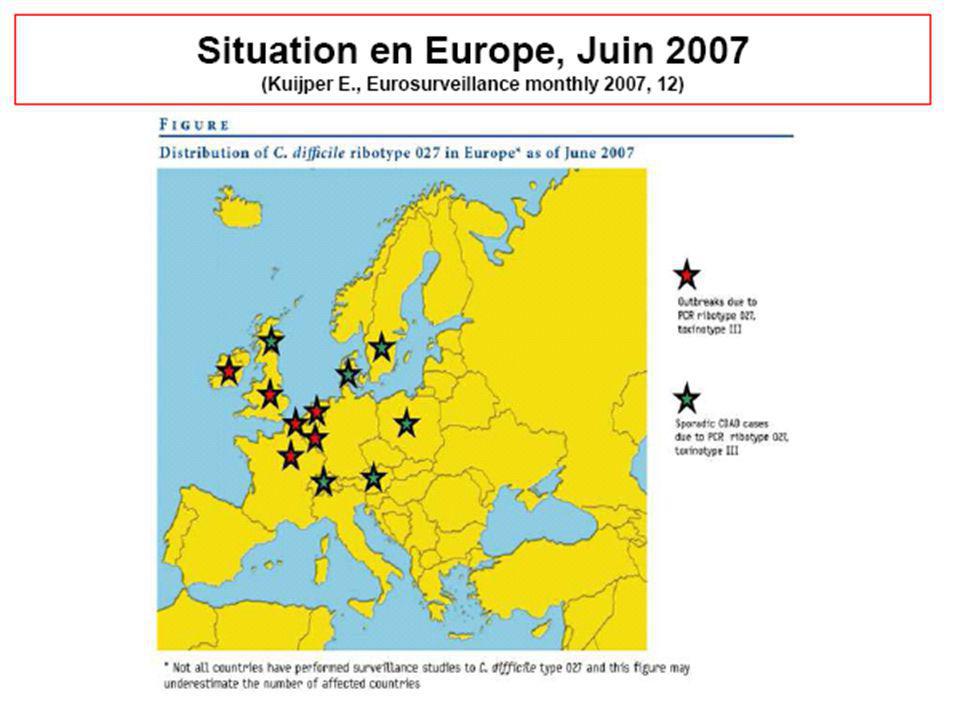

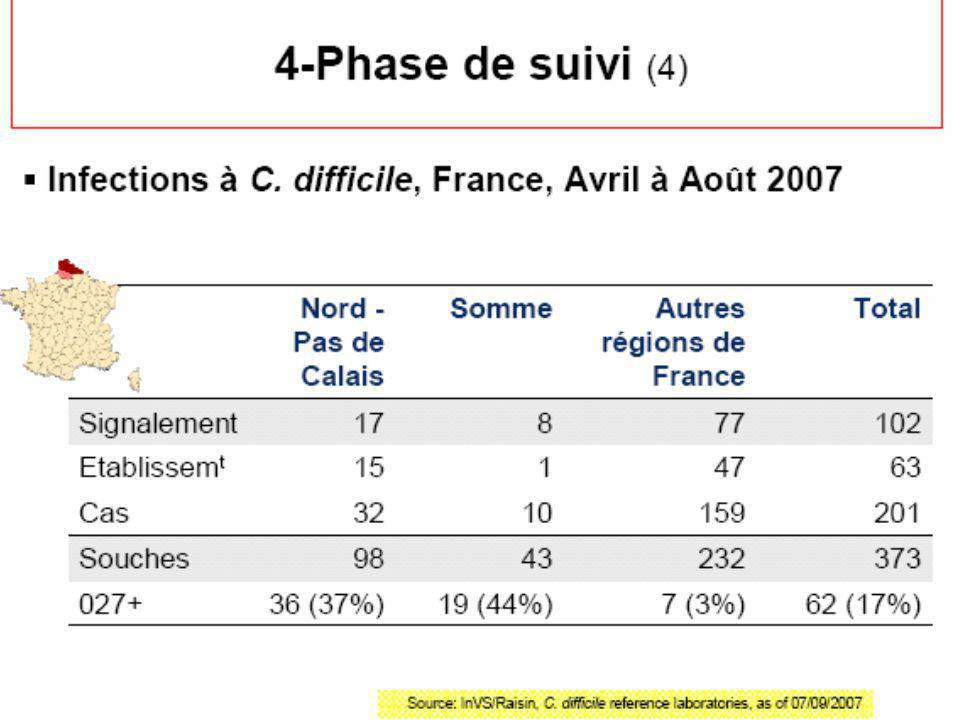






 d ’éradication du SARM en soins de longue durée>")













