Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Traitement des candidoses en réanimation
Annecy 25 Mai 2009 Traitement des candidoses en réanimation Jean-François Timsit Réanimation médicale CHU Albert Michallon UJF/INSERM U823 Grenoble, France

2
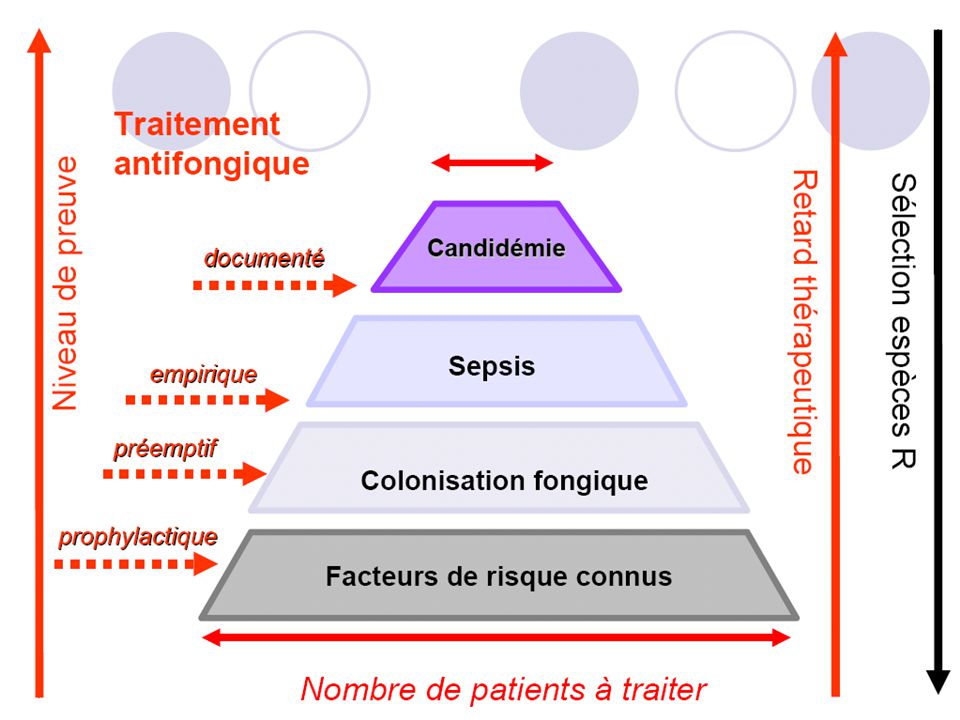
Il faut traiter vite et bien
Augmentation du nombre de molécules Les principales études cliniques Qui traiter en réanimation? Optimisation PK/PD, doses élevées associations

3
Epidemiology of sepsis in the US
Martin et al. NEJM (2003) 348;
 348;")
4
Epidemiology of Candidaemia in Europe
C. albicans – C. glabrata – C. parapsilosis – C. tropicalis 60.5% % % % Tortorano et al.,EJCMID 2004, 23:317

5
Nosocomial Bloodstream Infections in US Hospitals: 1995-2002
% BSI % Crude Mortality Rank Pathogen BSI per 10,000 admissions Total (n=20,978) ICU (n=10,515) Non-ICU 1. CoNS 15.8 31.3 35.9 26.6 20.7 25.7 13.8 2. S aureus 10.3 20.2 16.8 23.7 25.4 34.4 18.9 3. Enterococcus spp 4.8 9.4 9.8 9.0 33.9 43.0 24.0 4. Candida spp 4.6 10.1 7.9 39.2 47.1 29.0 5. E coli 2.8 5.6 3.7 7.6 22.4 16.9 6. Klebsiella spp 2.4 4.0 5.5 27.6 37.4 20.3 7. P aeruginosa 2.1 4.3 4.7 3.8 38.7 47.9 8. Enterobacter spp 1.9 3.9 3.1 26.7 32.5 18.0 9. Serratia spp 0.9 1.7 1.3 27.4 17.1 10. A baumannii 0.6 1.6 34.0 43.4 16.3 BSI=blood stream infection. Surveillance and Control of Pathogens of Epidemiologic Importance (SCOPE) study. Wisplinghoff H, et al. Clin Infect Dis. 2004;39:
 ICU. (n=10,515) Non-ICU. 1. CoNS S aureus Enterococcus spp Candida spp E coli Klebsiella spp P aeruginosa Enterobacter spp Serratia spp A baumannii BSI=blood stream infection. Surveillance and Control of Pathogens of Epidemiologic Importance (SCOPE) study. Wisplinghoff H, et al. Clin Infect Dis. 2004;39:")
6
Nosocomial BSI in ICU OR=8.83
Background. Overall rates of bloodstream infection (BSI) are often used as quality indicators in intensive care units (ICUs). We investigated whether ICU-acquired BSI increased mortality (by 10%) after adjustment for severity of infection at ICU admission and during the pre-BSI stay. Methods. We conducted a matched, risk-adjusted (1:n), exposed-unexposed study of patients with stays longer than 72 h in 12 ICUs randomly selected from the Outcomerea database. Results. Patients with BSI after the third ICU day (exposed group) were matched on the basis of risk-exposure time and mortality predicted at admission using the Three-Day Recalibrated ICU Outcome (TRIO) score to patients without BSI (unexposed group). Severity was assessed daily using the Logistic Organ Dysfunction (LOD) score. Of 3247 patients with ICU stays of 13 days, 232 experienced BSI by day 30 (incidence, 6.8 cases per 100 admissions); among them, 226 patients were matched to 1023 unexposed patients. Crude hospital mortality was 61.5% among exposed and 36.7% among unexposed patients ( ). Attributable mortality P ! was 24.8%. The only variable associated with both BSI and hospital mortality was the LOD score determined 4 days before onset of BSI (odds ratio [OR], 1.10; 95% confidence interval [CI], 1.03–1.16; Pp.0025). The adjusted OR for hospital mortality among exposed patients (OR, 3.20; 95% CI, 2.30–4.43) decreased when the LOD score determined 4 days before onset of BSI was taken into account (OR, 3.02; 95% CI, 2.17–4.22; P ! .0001). The estimated risk of death from BSI varied considerably according to the source and resistance of organisms, time to onset, and appropriateness of treatment. Conclusions. When adjusted for risk-exposure time and severity at admission and during the ICU stay, BSI was associated with a 3-fold increase in mortality, but considerable variation occurred across BSI subgroups. Focusing on BSI subgroups may be valuable for assessing quality of care in ICUs. Garrouste-Orgeas et al – Clin Infect Dis – 2006; 42:1118
 are often used as quality indicators in intensive care. units (ICUs). We investigated whether ICU-acquired BSI increased mortality (by 10%) after adjustment for. severity of infection at ICU admission and during the pre-BSI stay. Methods. We conducted a matched, risk-adjusted (1:n), exposed-unexposed study of patients with stays longer. than 72 h in 12 ICUs randomly selected from the Outcomerea database. Results. Patients with BSI after the third ICU day (exposed group) were matched on the basis of risk-exposure. time and mortality predicted at admission using the Three-Day Recalibrated ICU Outcome (TRIO) score to. patients without BSI (unexposed group). Severity was assessed daily using the Logistic Organ Dysfunction (LOD) score. Of 3247 patients with ICU stays of 13 days, 232 experienced BSI by day 30 (incidence, 6.8 cases per 100. admissions); among them, 226 patients were matched to 1023 unexposed patients. Crude hospital mortality was. 61.5% among exposed and 36.7% among unexposed patients ( ). Attributable mortality P ! was 24.8%. The. only variable associated with both BSI and hospital mortality was the LOD score determined 4 days before onset. of BSI (odds ratio [OR], 1.10; 95% confidence interval [CI], 1.03–1.16; Pp.0025). The adjusted OR for hospital. mortality among exposed patients (OR, 3.20; 95% CI, 2.30–4.43) decreased when the LOD score determined 4. days before onset of BSI was taken into account (OR, 3.02; 95% CI, 2.17–4.22; P ! .0001). The estimated risk of. death from BSI varied considerably according to the source and resistance of organisms, time to onset, and. appropriateness of treatment. Conclusions. When adjusted for risk-exposure time and severity at admission and during the ICU stay, BSI. was associated with a 3-fold increase in mortality, but considerable variation occurred across BSI subgroups. Focusing on BSI subgroups may be valuable for assessing quality of care in ICUs. Garrouste-Orgeas et al – Clin Infect Dis – 2006; 42:1118.")
7
Retard à la mise en route des antifongiques en Réanimation
Les patients avec instauration précoce du traitement (≤ 48 h) ont une probabilité de survie supérieure à celle des patients traités tardivement (> 48 h) Nolla-Salas J et al. Intensive Care Med 1997; 23: Le retard à l’instauration du traitement est un facteur prédictif indépendant de mortalité (odds ratio 1,52 ; p < 0,05) Garey KW et al. Clin Infect Dis 2006; 43: 46 épisodes de candidémie
 ont une probabilité de survie supérieure à celle des patients traités tardivement (> 48 h) Nolla-Salas J et al. Intensive Care Med 1997; 23: Le retard à l’instauration du traitement est un facteur prédictif indépendant de mortalité (odds ratio 1,52 ; p < 0,05) Garey KW et al. Clin Infect Dis 2006; 43: épisodes de candidémie.")
8
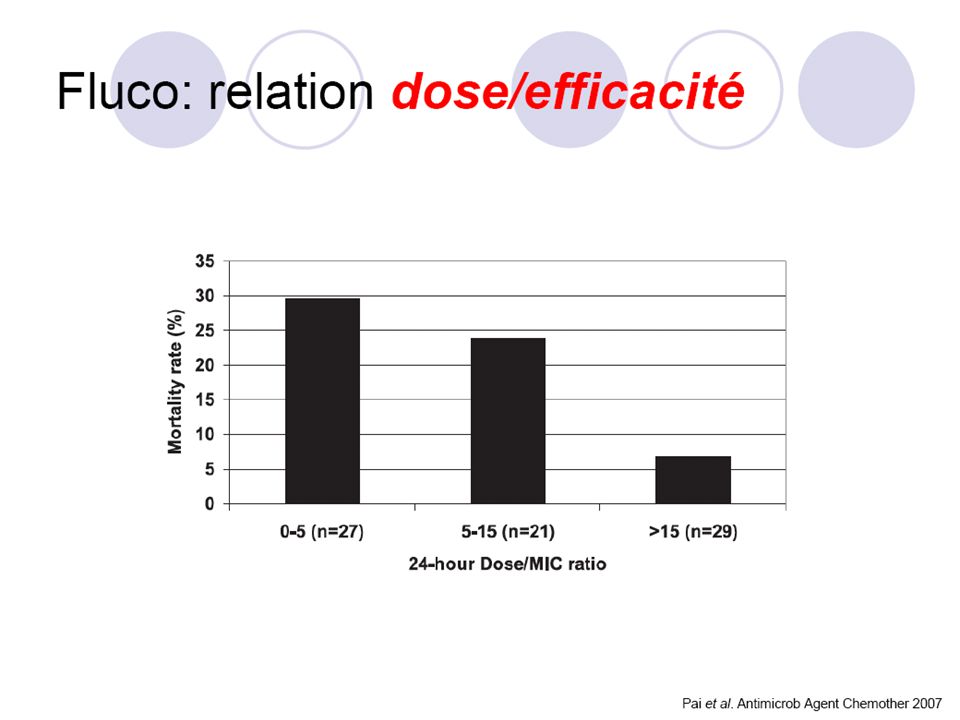
Délai entre la 1ère hémoculture et le début des antifongiques
n = 157 épisodes de candidémie 3 facteurs indépendants de mortalité : Score Apache II Antibiothérapie préalable Retard au traitement antifongique : traitement préemptif ? Morrell M et al. AAC 2005; 49:

9
Faudrait-il retirer les cathéters en Réanimation ?
206 épisodes de candidémie 272 épisodes de candidémie % 70 p < 0,0001 60 p < 0,001 50 40 30 20 Post hoc analysis of a randomized study comparing fluconazole and amphotericine B 10 Ablation du KT KT laissé en place Mortalité Durée de fongémie diminuée Mortalité diminuée Rex RH et al. Clin Infect Dis 1995; 21: Weinberger M et al. J Hosp Infect 2005; 61:

10
Il faut traiter vite et bien
Augmentation du nombre de molécules Les principales études cliniques Qui traiter en réanimation? Optimisation PK/PD, doses élevées associations

11
Prise en charge des candidoses invasives de l’adulte
CONSENSUS 2004 Prise en charge des candidoses invasives de l’adulte 11 11

12
Prise en charge des candidoses invasives de l’adulte
CONSENSUS 2004 Prise en charge des candidoses invasives de l’adulte 12 12

13
13

14
14

15
2009 Amb. liposomale ABLC Posaconazole Caspofungine Voriconazole
Flucytosine Fluconazole Itraconazole Anidulafungine, Micafungine Amphotéricine B

16
Inh la synth du 1,3 D glucane
rupture de la paroi instabilité osmotique et lyse cellulaire Liaison avec l’ergosterol de la membrane cytoplasmique permeabilité Mais affinité au cholesterol des cell. humaines Inhibition de la synth. De la C14- d methylase ergosterol stérols toxiques capté par la cytosine perméase Transformé en 5 FU (cytosine désaminase) altération de l’ARN
 altération de l’ARN.")
17
Spectre des antifongiques
Polyènes Fluco Itraco Vorico Candines C. albicans + C. krusei – C. glabrata C. parapsilosis

18
“Résistance” croisée entre azolés sur des isolats de C
“Résistance” croisée entre azolés sur des isolats de C. glabrata sur hémocultures (n = 149) VRZ (µg/ml) 0,03 0,06 0,12 0,25 0,5 1 2 4 ≥ 8 ≤ 0,12 6 8 15 21 16 20 32 ≥ 64 3 14 10 FCZ (µg/ml) Lortholary O et al. AAC 2007; 51:
 VRZ (µg/ml) 0,03. 0,06. 0,12. 0,25. 0, ≥ 8. ≤ 0, ≥ FCZ (µg/ml) Lortholary O et al. AAC 2007; 51:")
19
Antifungal susceptibility testing in candidemia :
in vitro / clinical correlation

20
Polyenes

21
Ambisome vs Amp B 687 neutropénies fébriles
% * * * * p < 0,001, ° p < 0, Walsh et al. NEJM 1999

22
Coprescription avec des agents néphrotoxiques
% de toxicité rénale 50% p<0,05 45% p<0,001 Amphotéricine B 0,6 mg/kg/j (n = 344) 45,4 % 40% 40,5 % 35% 30% 30,0 % AmBisome® 3 mg/kg/j (n = 343) 25% 20% p<0,05 22,3 % 15% 15,2 % 10% 5% 6,3 % 0% 0 ou 1 médicaments > 2 médicaments > 3 médicaments *Néphrotoxicité définie par une augmentation de la créatinine ≥ à 2x la valeur de base Walsh. N Engl J Med Dossier d’AMM Déc 99.
 45,4 % 40% 40,5 % 35% 30% 30,0 % AmBisome® 3 mg/kg/j. (n = 343) 25% 20% p<0,05. 22,3 % 15% 15,2 % 10% 5% 6,3 % 0% 0 ou 1 médicaments. > 2 médicaments. > 3 médicaments. *Néphrotoxicité définie par une augmentation de la créatinine ≥ à 2x la valeur de base. Walsh. N Engl J Med Dossier d’AMM Déc 99.")
23
Ambisome vs Abelcet Etude PRM tolérance 264 patients, 3 bras Ambi
3 mg/kg 5 mg/kg Abelcet Frissons 18,8 23,5 79,5 Fièvre 19,8 57,7 Créat x 2 14,1 14,8 42,3 Arrêt TT 12,9 12,3 32,1 Wingard et al. CID 2000

24
Candines

25
5346 souches USA (2000-2006) CMI50 / CMI90 :
CAS : 0,03 / 0,25 µg/ml MICA : 0,015 / 1 µg/ml AND : 0,06 / 2 µg/ml 99 % des isolats inhibés par ≤ 2 µg/mL quelque soit la candine émergence de résistance exceptionnelle (Mutant fks) Selection de souches moins sensibles? Aucune variation géographique Pfaller MA et al. 47th ICAAC 2007; M-552.
 Selection de souches moins sensibles Aucune variation géographique. Pfaller MA et al. 47th ICAAC 2007; M-552.")
26
Caspofongine:Sensibilité de 400 souches de candidémies
(NCCLS, RPMI 1640) Organisme (nb isolats) CMI extrêmes CMI 90 C. albicans (206) 0, ,5 0,125 C. glabrata (77) 0,03 - 0,5 0,25 C. tropicalis (54) 0,03 - 0,25 C. parapsilosis (40) 0,03 - 2 1 C. krusei (17) 0, C. spp (6 : 3 C. lusitaniae, 1 C. rugosa, 1 C. famata, 1 C. guilliermondii) 0,015 - > 8 Marco et al. Diagn Microbiol Infect Dis 1998;31:33-37
 Organisme (nb isolats) CMI extrêmes. CMI 90. C. albicans (206) 0, ,5. 0,125. C. glabrata (77) 0,03 - 0,5. 0,25. C. tropicalis (54) 0,03 - 0,25. C. parapsilosis (40) 0, C. krusei (17) 0, C. spp (6 : 3 C. lusitaniae, 1 C. rugosa, 1 C. famata, 1 C. guilliermondii) 0,015 - > 8. Marco et al. Diagn Microbiol Infect Dis 1998;31:")
27
Candines:relation CMI/efficacité?
???Compliqué, incomplètement connu Break point <= 2 mg/l (RPMI) Dans les modèles animaux (C albicans/souris) efficacité liée à AUC/CMI (200) et Pic sur CMI (5) Louie et al - ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Dec. 2005, p. 5058–5068 CMI différente en présence et en l’absence de sérum Paderu et al - ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, June 2007, p. 2253–2256 Efficacité identique in vivo (souris) a dose identiques CMI mesurée non liée à l’efficacité clinique chez l’homme Pfaller et al - JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2008, p. 2620–2629 Technique de référence (RPMI) mettant difficilement en évidence les rares mutants résistants (Fks1) Desnos-Ollivier et al - ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Sept. 2008, p. 3092–3098
 Dans les modèles animaux (C albicans/souris) efficacité liée à AUC/CMI (200) et Pic sur CMI (5) Louie et al - ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Dec. 2005, p. 5058–5068. CMI différente en présence et en l’absence de sérum. Paderu et al - ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, June 2007, p. 2253–2256. Efficacité identique in vivo (souris) a dose identiques. CMI mesurée non liée à l’efficacité clinique chez l’homme. Pfaller et al - JOURNAL OF CLINICAL MICROBIOLOGY, Aug. 2008, p. 2620–2629. Technique de référence (RPMI) mettant difficilement en évidence les rares mutants résistants (Fks1) Desnos-Ollivier et al - ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Sept. 2008, p. 3092–3098.")
28
Comparaison des échinocandines
Posologie (mg/j) Cmax (µg/ml) ASC0-24h (mg•h/l) t1/2ß (h) CL (ml/min/kg) Vdss Caspofungine 50 (70 à J1) 9,9 93,5 9-11 12 ml/min - Micafungine 10,1 16,4 15-17 0,3 ml/min/kg 0,39 l/kg Anidulafungine 100 (200 à J1) 7,5 110,3 25,6 16 ml/min 30-50 l Kim R et al. Expert Opin Pharmacother 2007; 8:
 Cmax. (µg/ml) ASC0-24h (mg•h/l) t1/2ß. (h) CL (ml/min/kg) Vdss. Caspofungine. 50 (70 à J1) 9,9. 93, ml/min. - Micafungine ,1 16, ,3 ml/min/kg. 0,39 l/kg. Anidulafungine. 100 (200 à J1) 7,5. 110,3. 25,6. 16 ml/min l. Kim R et al. Expert Opin Pharmacother 2007; 8:")
29
Caspofungine Posologie (AMM)
Pour un patient dont le poids > 80 kg Dose de charge à J1 70 mg Puis maintien de la posologie de 70 mg/jour Posologie

30
Pharmacology: Metabolism, Elimination, and Protein Binding
Source A (WPC), p 9, §XIXb-3, ¶1, L1-2 (metabolism), §XIXb-4, ¶1, L1-3 (elimination), §XIXb-2, ¶1, L6-7 (protein binding) p 6, §XII, ¶1, L3 (dialyzable) 5/Dodds Ashley, p S31, Table 2, L1 (bioavailability) 1/Mycamine, p 1, C1, ¶12, L1 (metabolism), C1, ¶14, L1-3 (elimination), C1, ¶11, L1 (protein binding) C1, ¶19, L1 (dialyzable) 2/Eraxis PI, 2007, p 3, ¶1, L1, ¶2, L1 (metabolism), ¶3, L2-4 (elimination); p 2, ¶3, L3 (protein binding) p 4, ¶6, L5 (dialyzable) Pharmacology: Metabolism, Elimination, and Protein Binding Caspofungin Micafungin Anidulafungin Metabolism Hepatic metabolism by hydrolysis and N-acetylation Spontaneous nonhepatic chemical degeneration Hepatic metabolism by arylsulfatase and catechol-O-methyl-transferase Nonhepatic chemical degradation Elimination/ excretion Urine 41% Feces 34% Urine + feces 82.5% Feces 71% Urine <1% Feces ≈30% Protein Binding 97% >99% There are differences in the metabolism and elimination fo all 3 echinocandins. The primary metabolic mechanism for caspofungin is mediated by hepatic enzymes with some chemical degradation as a secondary mode. Anidulafungin primarily undergoes spontaneous chemical degradation.1,2 Hepatic metabolism by arylsulfatase and catechol-O-methyl-transferase is the reported mode of metabolism for micafungin and there are 5 metabolites of micafungin. Is this metabolism somehow implicated in the different pre-clincial data seen with micafungin? No one knows. There are significant differences in the elimination pathways for the echinocandins. Caspofungin is excreted in approximately equal proportions via the urine and feces; micafungin and anidulafungin are primarily excreted via the feces.1,2 Protein binding for the echinocandins ranges from 97% for caspofungin to over 99% for micafungin and anidulafungin.1,2 Protein binding for anidulafungin was previously reported as 84%.3 The clinical significance of protein binding account for the ability to use lower doses of caspofungin.4 If asked… Oral bioavailability is poor (<5%) for all of the echinocandins,5 and therefore these drugs must be administered parenterally.6 None of the echinocandins is dialyzable.1,2,7 Source A (WPC), p 9, §XIXb-3, ¶1, L1-2 1/Mycamine, p 1, C1, ¶12, L1 2/Eraxis PI, 2007, p 3, ¶1, L1, ¶2, L1 §XIXb-4, ¶1, L1-3 p 1, C1, ¶14, L1-3 p 3, ¶3, L2-4 §XIXb-2, ¶1, L6-7 p 1, C1, ¶11, L1 2/Eraxis PI, 2007, p 3, ¶3, L3 3/Eraxis PI, 2006, p 2, ¶3, L3 4/Theuretzbacher, p 808, C1, ¶3, L19-28 5/Dodds Ashley, p S31, Table 2, L1 6/Wagner, p 165, C1, ¶3, L1-3 p 6, §XII, ¶1, L3 (dialyzable) p 1, C1, ¶19, L1 (dialyzable) p 4, ¶6, L5 (dialyzable) 7/Morrison, p 326, C1, L2 Adapted from Micafungin US Prescribing Information; Anidulafungin US Prescribing Information; Dodds Ashley ES, et al. Clin Infect Dis. 2006;43:S28–S39. References Mycamine™ (micafungin sodium) For Injection. US Prescribing Information, Astellas Pharma US, Inc., June 2006. Eraxis™ (anidulafungin) For Injection. US Prescribing Information, Roerig Division of Pfizer Inc, February 2007. Eraxis™ (anidulafungin) For Injection. US Prescribing Information, Roerig Division of Pfizer Inc, March 2006. Theuretzbacher U. Pharmacokinetics/pharmacodynamics of echinocandins. Eur J Clin Microbiol Infect Dis. 2004;23:805–812. Dodds Ashley ES, Lewis R, Lewis JS, el al. Pharmacology of systemic antifungal agents. Clin Infect Dis. 2006;43:S28–S39. Wagner C, Graninger W, Presterl E, Joukhadar C. The echinocandins: comparison of their pharmacokinetics, pharmacodynamics and clinical applications. Pharmacology. 2006;78:161–177. Morrison VA. Echinocandin antifungals: review and update. Expert Rev Anti Infect Ther. 2006;4:325–342.
, p 9, §XIXb-3, ¶1, L1-2 (metabolism), §XIXb-4, ¶1, L1-3 (elimination), §XIXb-2, ¶1, L6-7 (protein binding) p 6, §XII, ¶1, L3 (dialyzable) 5/Dodds Ashley, p S31, Table 2, L1 (bioavailability) 1/Mycamine, p 1, C1, ¶12, L1 (metabolism), C1, ¶14, L1-3 (elimination), C1, ¶11, L1 (protein binding) C1, ¶19, L1 (dialyzable) 2/Eraxis PI, 2007, p 3, ¶1, L1, ¶2, L1 (metabolism), ¶3, L2-4 (elimination); p 2, ¶3, L3 (protein binding) p 4, ¶6, L5 (dialyzable) Pharmacology: Metabolism, Elimination, and Protein Binding. Caspofungin. Micafungin. Anidulafungin. Metabolism. Hepatic metabolism by hydrolysis and N-acetylation Spontaneous nonhepatic chemical degeneration. Hepatic metabolism by arylsulfatase and catechol-O-methyl-transferase. Nonhepatic chemical degradation. Elimination/ excretion. Urine 41% Feces 34% Urine + feces 82.5% Feces 71% Urine <1% Feces ≈30% Protein Binding. 97% >99% There are differences in the metabolism and elimination fo all 3 echinocandins. The primary metabolic mechanism for caspofungin is mediated by hepatic enzymes with some chemical degradation as a secondary mode. Anidulafungin primarily undergoes spontaneous chemical degradation.1,2. Hepatic metabolism by arylsulfatase and catechol-O-methyl-transferase is the reported mode of metabolism for micafungin and there are 5 metabolites of micafungin. Is this metabolism somehow implicated in the different pre-clincial data seen with micafungin No one knows. There are significant differences in the elimination pathways for the echinocandins. Caspofungin is excreted in approximately equal proportions via the urine and feces; micafungin and anidulafungin are primarily excreted via the feces.1,2. Protein binding for the echinocandins ranges from 97% for caspofungin to over 99% for micafungin and anidulafungin.1,2. Protein binding for anidulafungin was previously reported as 84%.3. The clinical significance of protein binding account for the ability to use lower doses of caspofungin.4. If asked… Oral bioavailability is poor (<5%) for all of the echinocandins,5 and therefore these drugs must be administered parenterally.6. None of the echinocandins is dialyzable.1,2,7. Source A (WPC), p 9, §XIXb-3, ¶1, L1-2. 1/Mycamine, p 1, C1, ¶12, L1. 2/Eraxis PI, 2007, p 3, ¶1, L1, ¶2, L1. §XIXb-4, ¶1, L1-3. p 1, C1, ¶14, L1-3. p 3, ¶3, L2-4. §XIXb-2, ¶1, L6-7. p 1, C1, ¶11, L1. 2/Eraxis PI, 2007, p 3, ¶3, L3. 3/Eraxis PI, 2006, p 2, ¶3, L3. 4/Theuretzbacher, p 808, C1, ¶3, L /Dodds Ashley, p S31, Table 2, L1. 6/Wagner, p 165, C1, ¶3, L1-3. p 6, §XII, ¶1, L3 (dialyzable) p 1, C1, ¶19, L1 (dialyzable) p 4, ¶6, L5 (dialyzable) 7/Morrison, p 326, C1, L2. Adapted from Micafungin US Prescribing Information; Anidulafungin US Prescribing Information; Dodds Ashley ES, et al. Clin Infect Dis. 2006;43:S28–S39. References. Mycamine™ (micafungin sodium) For Injection. US Prescribing Information, Astellas Pharma US, Inc., June Eraxis™ (anidulafungin) For Injection. US Prescribing Information, Roerig Division of Pfizer Inc, February Eraxis™ (anidulafungin) For Injection. US Prescribing Information, Roerig Division of Pfizer Inc, March Theuretzbacher U. Pharmacokinetics/pharmacodynamics of echinocandins. Eur J Clin Microbiol Infect Dis. 2004;23:805–812. Dodds Ashley ES, Lewis R, Lewis JS, el al. Pharmacology of systemic antifungal agents. Clin Infect Dis. 2006;43:S28–S39. Wagner C, Graninger W, Presterl E, Joukhadar C. The echinocandins: comparison of their pharmacokinetics, pharmacodynamics and clinical applications. Pharmacology. 2006;78:161–177. Morrison VA. Echinocandin antifungals: review and update. Expert Rev Anti Infect Ther. 2006;4:325–342.")
31
Anidulafungine chez l’insuffisant hépatique
Vazquez JA et al. Clin Ther 2005; 27:

32
Préparation et stabilité des echinocandines
Caspofungine Micafungine Anidulafungine Dilution Volume de perfusion total Incompatibilité Stockage (produit reconstitué) Autre NaCl 0,9 % ou ringer-lactate 250 ml D-glucose 48 heures 2 - 8°C NaCl ou D-glucose 100 ml 24 heures 25°C Protéger de la lumière Eau PPI*/éthanol 280 ml Contient 6 g d’alcool pour 100 mg d’anidula • Dilution - La caspofungine est facilement soluble dans l'eau et le méthanol (Rapp RP. Pharmacotherapy 2004) et n'a pas besoin de diluant alcool pour la reconstitution (diluant : eau stérile pour préparations injectables,ou eau pour préparations injectables avec du parahydroxybenzoate de méthyle et du parahydroxybenzoate de propyle ou eau pour préparations injectables avec de l'alcool benzylique à 0,9 %). La caspofungine n’étant pas stable dans les diluants contenant du D-glucose, on ne peut pas utiliser ce type de diluants. La micafungine est soluble dans l’eau, dans une solution isotonique de chlorure de sodium, et peu soluble dans l'alcool (diluant : solution pour injection de NaCl 0,9% ou de D-glucose à 5 %). (Astellas Pharma US, Inc., December 2005) L'anidulafungine est insoluble dans l'eau et a donc besoin d'un diluant spécial pour la reconstitution (diluant : alcool déshydraté à 20 % dans de l’eau pour préparation injectable). (Pfizer Inc, March 2006) La quantité d'alcool est d'environ 6 g pour une dose de 100 mg d'anidulafungine. • Conservation - La caspofungine reconstituée peut être conservée à 25° C ou moins pendant 24 h avant la préparation de la solution. La solution diluée de caspofungine peut être conservée au réfrigérateur, entre 2 et 8 °C, pendant 48 heures. La micafungine reconstituée ou diluée peut être conservée à température ambiante,37 pendant 24 h. C’est une molécule sensible à la lumière. (Astellas Pharma US, Inc., December 2005) L’anidulafungine reconstituée peut être conservée à température ambiante. La solution reconstituée doit être conservée à 25 °C, avec des excursions autorisées entre 15 °C et 30 °C. La solution reconstituée doit ensuite être diluée et utilisée dans les 24 heures. (Pfizer Inc, March 2006) * Pour préparation injectable Adapté de : Caspofungin EMEA Product Information ; Micafungin US Prescribing Information ; Anidulafungin EMEA Product Information Information.
 Autre. NaCl 0,9 % ou ringer-lactate. 250 ml. D-glucose. 48 heures °C. NaCl ou D-glucose. 100 ml. 24 heures. 25°C. Protéger de la lumière. Eau PPI*/éthanol. 280 ml. Contient 6 g d’alcool pour 100 mg d’anidula. • Dilution. - La caspofungine est facilement soluble dans l eau et le méthanol (Rapp RP. Pharmacotherapy 2004) et n a pas besoin de diluant alcool pour la reconstitution (diluant : eau stérile pour préparations injectables,ou eau pour préparations injectables avec du parahydroxybenzoate de méthyle et du parahydroxybenzoate de propyle ou eau pour préparations injectables avec de l alcool benzylique à 0,9 %). La caspofungine n’étant pas stable dans les diluants contenant du D-glucose, on ne peut pas utiliser ce type de diluants. La micafungine est soluble dans l’eau, dans une solution isotonique de chlorure de sodium, et peu soluble dans l alcool (diluant : solution pour injection de NaCl 0,9% ou de D-glucose à 5 %). (Astellas Pharma US, Inc., December 2005) L anidulafungine est insoluble dans l eau et a donc besoin d un diluant spécial pour la reconstitution (diluant : alcool déshydraté à 20 % dans de l’eau pour préparation injectable). (Pfizer Inc, March 2006) La quantité d alcool est d environ 6 g pour une dose de 100 mg d anidulafungine. • Conservation. - La caspofungine reconstituée peut être conservée à 25° C ou moins pendant 24 h avant la préparation de la solution. La solution diluée de caspofungine peut être conservée au réfrigérateur, entre 2 et 8 °C, pendant 48 heures. La micafungine reconstituée ou diluée peut être conservée à température ambiante,37 pendant 24 h. C’est une molécule sensible à la lumière. (Astellas Pharma US, Inc., December 2005) L’anidulafungine reconstituée peut être conservée à température ambiante. La solution reconstituée doit être conservée à 25 °C, avec des excursions autorisées entre 15 °C et 30 °C. La solution reconstituée doit ensuite être diluée et utilisée dans les 24 heures. (Pfizer Inc, March 2006) * Pour préparation injectable. Adapté de : Caspofungin EMEA Product Information ; Micafungin US Prescribing Information ; Anidulafungin EMEA Product Information Information.")
33
Azoles

34
Fluconazole QS… Dose de charge 12 mg/kg/j Dose élevée si SDD Espacement des rythme d’administration si IR Foie++

36
Voriconazole (Vfend)
Triazolé à spectre large Indications : Aspergilloses invasives et infections graves à Candida (y compris C. krusei) résistant au fluconazole Posologie (IV) : 6 mg/kg x 2 pendant 24 h puis 4 mg/kg x 2 Biodisponibilité orale absolue : 96 % (200 mg x 2/j) Elimination par métabolisation hépatique et excrétion urinaire Privilégier la voie orale en cas d’insuffisance rénale
 résistant au fluconazole. Posologie (IV) : 6 mg/kg x 2 pendant 24 h puis 4 mg/kg x 2. Biodisponibilité orale absolue : 96 % (200 mg x 2/j) Elimination par métabolisation hépatique et excrétion urinaire. Privilégier la voie orale en cas d’insuffisance rénale.")
37
Voriconazole (Vfend)
Effets 2re: Tr de la vision, éruption, tr digestifs transaminase (surdosage) Interaction: Rifampicine Cmax et ASC de 93 et 96% CI (carbamazepine, phenobarbital) Surveillance tacrolimus et ciclosporine ( taux) Accumulation de midazolam Adaptation de posologie: Insuffisance hépatique: Cirrhose child C (même dose de charge, puis 2mg/kg X 2) Insuffisance rénale: Accumulation du véhicule IV SBECD (conséquences???). Pas d’adaptation de posologie si HD (HF??)
 Interaction: Rifampicine Cmax et ASC de 93 et 96% CI. (carbamazepine, phenobarbital) Surveillance tacrolimus et ciclosporine ( taux) Accumulation de midazolam. Adaptation de posologie: Insuffisance hépatique: Cirrhose child C (même dose de charge, puis 2mg/kg X 2) Insuffisance rénale: Accumulation du véhicule IV SBECD (conséquences ). Pas d’adaptation de posologie si HD (HF )")
38
Il faut traiter vite et bien
Augmentation du nombre de molécules Les principales études cliniques Optimisation PK/PD, doses élevées associations Qui traiter en réanimation?

39
Réponse au fluconazole dans les essais cliniques
Rex et al Phillips et al Rex et al FCZ (400 mg) n = 103 AmB n = 103 FCZ (400 mg) n = 42 AmB n = 42 FCZ (800 mg) n = 107 FCZ + AmB n = 112 Les taux de réponse au fluconazole varient de 56 % à 70 % Rex JH et al. NEJM 1994; 331: Phillips P et al. Eur J Clin Microbiol Infect Dis 1997; 16: Rex JH et al. Clin Infect Dis 2003; 36:
 n = 103. AmB n = 103. FCZ (400 mg) n = 42. AmB n = 42. FCZ (800 mg) n = 107. FCZ + AmB n = 112. Les taux de réponse au fluconazole varient de 56 % à 70 % Rex JH et al. NEJM 1994; 331: Phillips P et al. Eur J Clin Microbiol Infect Dis 1997; 16: Rex JH et al. Clin Infect Dis 2003; 36:")
40
Etude randomisée en double aveugle: candidoses invasives
Stratification sur Apache II (moyenne 15) et présence neutropénie (11%) Caspo: 70 mg à J1 puis 50 mg/j ou Amb (0,6- 1 mg/kg/j) au minimum 10 jours Critère principal: Efficacité en fin de traitement IV 239 pts inclus, 224 en ITT modifiée Candidémies: 181/224 Mora-Duarte J et al. NEJM 2002.
 et présence neutropénie (11%) Caspo: 70 mg à J1 puis 50 mg/j ou Amb (0,6- 1 mg/kg/j) au minimum 10 jours. Critère principal: Efficacité en fin de traitement IV. 239 pts inclus, 224 en ITT modifiée. Candidémies: 181/224. Mora-Duarte J et al. NEJM")
41
Caspofungine versus amphotéricine B dans la candidose invasive
Différence de12.7 % (CI 95: à 26.0) p=0.09 41 Mora-Duarte J et al. NEJM 2002; 347: 41
 p= Mora-Duarte J et al. NEJM 2002; 347:")
42
Caspofungine versus amphotéricine B dans la candidose invasive
Effets indésirables liés au traitement 42 Mora-Duarte J et al. NEJM 2002; 347: 42

43
fluconazole per os (400 mg/j) après 10 jours de traitement IV
NEJM 2007; 356: Etude randomisée, multicentrique, en double aveugle, de non-infériorité, 245 patients fluconazole per os (400 mg/j) après 10 jours de traitement IV Anidulafungine IV 200 mg à J1 Puis : 100 mg/j Fluconazole IV 800 mg à J1 Puis : 400 mg/j 43 43
 après 10 jours de traitement IV. Anidulafungine IV. 200 mg à J1. Puis : 100 mg/j. Fluconazole IV. 800 mg à J1. Puis : 400 mg/j")
44
Anidulafungine versus fluconazole dans la candidose invasive
Table 1. Characteristics of the Modified Intention-to-Treat Population. * mITT : all patients who received at least one dose of study medication and had a positive culture for candida species within 96 hours before enrollment. Reboli AC et al. NEJM 2007; 356: 44 44

45
Anidulafungine versus fluconazole dans la candidose invasive
Table 1. Characteristics of the Modified Intention-to-Treat Population. 45 Reboli AC et al. NEJM 2007; 356: 45

46
Anidulafungine versus fluconazole dans la candidose invasive
Table 1. Characteristics of the Modified Intention-to-Treat Population. 46 Reboli AC et al. NEJM 2007; 356: 46

47
Réponse globale (clinique + µbiologique),
à la fin du traitement IV, dans la population en ITTm p < 0.02 Reboli AC et al. NEJM 2007; 356: 47

48
Anidulafungine versus fluconazole dans la candidose invasive
Table 1. Characteristics of the Modified Intention-to-Treat Population. 48 Reboli AC et al. NEJM 2007; 356: 48

49
Lancet 2007; 369: 1519–27 49

50
Protocol Objective Design Main inclusion criteria
Efficacy and safety of micafungin vs liposomal amphotericin B (Ambisome®, L-AMB) in patients with invasive candidiasis (IC) or candidemia Design Double-blind, randomised (1:1), non-inferiority study [δ= 15%] in patients ≥ 16 years Main inclusion criteria Non-neutropenic and neutropenic (< 500 cells/µl) patients Clinical and microbiological evidence of IC or candidemia (all Candida species) Primary efficacy endpoint Overall treatment success at end of therapy (EOT) in the per protocol set (PPS) as determined by investigator Overall treatment success: clinical (complete or partial) and mycological (eradication or presumed eradication) response * Patients treated for hepatosplenic candidiasis, Candida osteomyelitis or Candida endocarditis max. treatment 4 weeks Kuse E, at al. Lancet 2007. 50
 in patients with invasive candidiasis (IC) or candidemia. Design. Double-blind, randomised (1:1), non-inferiority study [δ= 15%] in patients. ≥ 16 years. Main inclusion criteria. Non-neutropenic and neutropenic (< 500 cells/µl) patients. Clinical and microbiological evidence of IC or candidemia (all Candida species) Primary efficacy endpoint. Overall treatment success at end of therapy (EOT) in the per protocol set (PPS) as determined by investigator. Overall treatment success: clinical (complete or partial) and mycological (eradication or presumed eradication) response. * Patients treated for hepatosplenic candidiasis, Candida osteomyelitis or Candida endocarditis max. treatment 4 weeks. Kuse E, at al. Lancet")
51
Study Duration and Treatment
Micafungin (100 mg/day) i.v., N=264 Follow-up Patients Randomized 1:1 AmBisome (3 mg/kg/day) i.v., N=267 Follow-up Treatment 2–4 weeks Post Treatment 12 weeks EVR, early virological response; ETVR, end-treatment virological response; SVR, sustained virological response. Day 1 EOT EOS† Dose adjustments permitted under predefined conditions Dose increase to 200 mg/day for micafungin or 5 mg/kg/day for L-AMB Dose decrease by 50% due to nephrotoxicity – only for L-AMB †EOS, end of study. Kuse E, at al. Lancet 2007. 51
 i.v., N=264. Follow-up. Patients Randomized 1:1. AmBisome (3 mg/kg/day) i.v., N=267. Follow-up. Treatment. 2–4 weeks. Post Treatment. 12 weeks. EVR, early virological response; ETVR, end-treatment virological response; SVR, sustained virological response. Day 1. EOT. EOS† Dose adjustments permitted under predefined conditions. Dose increase to 200 mg/day for micafungin or 5 mg/kg/day for L-AMB. Dose decrease by 50% due to nephrotoxicity – only for L-AMB. †EOS, end of study. Kuse E, at al. Lancet")
52
Study Population 531 adult patients were randomized and received at least 1 dose of study drug (intent-to-treat population, ITT) 264 received micafungin (ITT) Safety population 267 received L-AMB (ITT) Safety population Confirmed candidemia or IC Assessment for overall treatment success at EOT ≥ 5 doses of study drug No prohibited antifungal medication Intent to treat population (ITT): patients who were randomized and received at least one dose of study drug – Safety population Per Protocol Set (PPS): patients who had confirmed diagnosis of IC or candidaemia, had an assessment of overall treatment success at EOT, received at least 5 doses of study drug and did not receive prohibited antifungal medication – Primary efficacy population Modified intent to treat population (MITT): patients who had a confirmed diagnosis of IC or candidaemia and received at least one dose of study drug – Secondary efficacy population Reasons why patients were excluded from PPS: Candidaemia /IC not confirmed (mica 17, ambi 20), < 5 doses of study drug (mica 24, ambi 33), no assessment of overall success at EOT (mica 42, ambi 55), prohibited medication (mica 4, ambi 2): There could be more than one reason PPS = Primary efficacy population PPS = Primary efficacy population Kuse E, at al. Lancet 2007. 52
 Safety population. 267 received L-AMB (ITT) Safety population. Confirmed candidemia or IC. Assessment for overall treatment success at EOT. ≥ 5 doses of study drug. No prohibited antifungal medication. Intent to treat population (ITT): patients who were randomized and received at least one dose of study drug – Safety population. Per Protocol Set (PPS): patients who had confirmed diagnosis of IC or candidaemia, had an assessment of overall treatment success at EOT, received at least 5 doses of study drug and did not receive prohibited antifungal medication – Primary efficacy population. Modified intent to treat population (MITT): patients who had a confirmed diagnosis of IC or candidaemia and received at least one dose of study drug – Secondary efficacy population. Reasons why patients were excluded from PPS: Candidaemia /IC not confirmed (mica 17, ambi 20), < 5 doses of study drug (mica 24, ambi 33), no assessment of overall success at EOT (mica 42, ambi 55), prohibited medication (mica 4, ambi 2): There could be more than one reason. PPS = 202 Primary efficacy population. PPS = 190 Primary efficacy population. Kuse E, at al. Lancet")
53
Baseline Characteristics
ITT population Micafungin N = 264 L-AMB N = 267 ICU 135 (51.1%) 135 (50.6%) Ventilation 89 (33.7%) 99 (37.1%) Dialysis 34 (12.9%) 23 (8.6%) CVC 223 (84.5%) 241 (80.1%) Neutropenia 28 (10.5%) Apache II score (mean ± SD) 15.8 ± 8.47 15.6 ± 8.16 Apache II score > 20 66 (27.5%) 56 (24.0%) Kuse E, at al. Lancet 2007. 53
 135 (50.6%) Ventilation. 89 (33.7%) 99 (37.1%) Dialysis. 34 (12.9%) 23 (8.6%) CVC. 223 (84.5%) 241 (80.1%) Neutropenia. 28 (10.5%) Apache II score. (mean ± SD) 15.8 ± ± Apache II score > (27.5%) 56 (24.0%) Kuse E, at al. Lancet")
54
Overall Treatment Success† at EOT (PPS)
†Overall treatment success defined as clinical and mycological response Kuse E, at al. Lancet 2007. 54

55
Treatment Success by Species at EOT (PPS)
† †C. guilliermondii, C. famata, C. lusitaniae, C. dubliniensis, C. inconspicua, C. rugosa. Kuse E, at al. Lancet 2007. 55

56
Micafungine versus amphotéricine B liposomale dans la candidémie et la candidose invasive
Effets indésirables * p < 0,05 L-AMB Micafungine 56 Kuse ER et al. Lancet 2007; 369: 56

57
Treatment Discontinuation Due to Adverse Events (ITT)
Micafungin n = 264 L-AMB n = 267 Overall AEs 60 (22.7%) 72 (27.0%) Drug-related AEs 13 (4.9%) 24 (9.0%) Drug-related SAEs 3 (1.1%) 11 (4.1%) (S)AE: (serious) adverse event Micafungin: bradycardia (1), leucopenia (1), hepatitis (1) L-AMB: renal failure (4), creatinine increase (1), infusion-related reactions (4), cardiac arrest (1), hepatitis (1) Kuse E, at al. Lancet 2007. 57
 72 (27.0%) Drug-related AEs. 13 (4.9%) 24 (9.0%) Drug-related SAEs. 3 (1.1%) 11 (4.1%) (S)AE: (serious) adverse event. Micafungin: bradycardia (1), leucopenia (1), hepatitis (1) L-AMB: renal failure (4), creatinine increase (1), infusion-related reactions (4), cardiac arrest (1), hepatitis (1) Kuse E, at al. Lancet")
58
Micafungin vs Caspofungin
Pappas et al Clin Infect Dis 2007

59
Résumé efficacité May 2009 Optimisation? Associations? Fluco =Ampho B
C krusei, Toxicité renale Ampho B = AmbL sauf toxicité++ VRZ= AmphoB puis Fluco Cas>Amb? meilleure efficacité ou moindre toxicité?, C parapsilosis? Anidula>Fluco? En particulier sur C albicans et C tropicalis (parapsilosis idem) Micafungin = Caspofungin Micafungin = AmbL Plus de toxicité (impact pronostic?) Optimisation? Associations?
 Micafungin = Caspofungin. Micafungin = AmbL. Plus de toxicité (impact pronostic ) Optimisation Associations")
60
Caspofungine (concentration in ICU)
40 SICU patients Dosage résiduel tous les jours 47 à 108 kg CSP 70mg puis 50mg/j Taux Bas si poids haut HD,HF,Mars Albumine basse MethylPrednisolone Min-max 25 et 75th perc. N’guyen et al – JAC 2007

61
Concentration de caspofongine en réanimation
ICU * (n=8) Non ICU (n=21) P CSP dose (mg/kg/d) 0.65 ( ) 0.7 ( ) NS Days of ttx 16 (6-32) 13 (4-31) Serum alb g/L 22 (16-35) 32 (24-35) <0.01 Peak CSP mg/L 4 ( ) 5.9 ( ) 24h-AUC CSP 28.6 ( ) 41.2 ( ) (*) SAPS II=41, 6/8 Pam<70mmHg Pascual AA et al (Lausanne) – ICAAC 2007
 Non ICU (n=21) P. CSP dose (mg/kg/d) 0.65 ( ) 0.7 ( ) NS. Days of ttx. 16 (6-32) 13 (4-31) Serum alb g/L. 22 (16-35) 32 (24-35) <0.01. Peak CSP mg/L. 4 ( ) 5.9 ( ) 24h-AUC CSP ( ) 41.2 ( ) (*) SAPS II=41, 6/8 Pam<70mmHg. Pascual AA et al (Lausanne) – ICAAC")
62
Caspo haute dose? A SUIVRE: Betts et al – 48th ICAAC Oct 2008
Etude pilote en greffe de moelle 64 malades 70 mg/j puis 50mg/j vs 34 malades 100 mg/j Pas de différences d’effets secondaires Survie sans maladie (en faveur des HD p=0.09) DC toute cause (p=0.63) Safdar et al – BMT 2007; 39:157 A SUIVRE: Betts et al – 48th ICAAC Oct 2008 200 patients randomisés double aveugle Pas d’effet secondaires Tendance à une efficacité un peu supérieure et moins de réciidives
 DC toute cause (p=0.63) Safdar et al – BMT 2007; 39:157. A SUIVRE: Betts et al – 48th ICAAC Oct patients randomisés double aveugle. Pas d’effet secondaires. Tendance à une efficacité un peu supérieure et moins de réciidives.")
63
Liposomal amphotericin b as initial therapy for invasive mould infections: a randomized trial comparing a high loading dose regimen with standard dosing (AmBiLoad Trial). Loading regimen: AmBisome 10 mg/kg/day x 14 days→ AmBisome 3 mg/kg/day Patients Randomized 1:1 N=339 Standard regimen: AmBisome 3 mg/kg/day x 14 days→ AmBisome 3 mg/kg/day Cornely O. et al. CID 15 May 2007

64
Favorable Overall Response: No Significant Differences between Treatment Groups
No differences are statistically significant

65
AmBiLoad Trial: Safety [ITT Population]
No unusual or previously unreported safety signals were seen in either treatment arm Drug discontinuations more frequent in 10 mg/kg/d arm Higher rates of serum creatinine (>2x baseline) and hypokalemia in 10 mg/kg/d arm Serum creatinine, 14% 3mg/kg, 31% 10mg/kg Hypokalemia, 16% 3mg/kg, 30% 10mg/kg Safety profiles for each treatment group comparable to previously reported safety data for AmBisome
![AmBiLoad Trial: Safety [ITT Population]](http://slideplayer.fr/slide/1580221/4/images/65/AmBiLoad+Trial%3A+Safety+%5BITT+Population%5D.jpg "No unusual or previously unreported safety signals were seen in either treatment arm. Drug discontinuations more frequent in 10 mg/kg/d arm. Higher rates of serum creatinine (>2x baseline) and hypokalemia in 10 mg/kg/d arm. Serum creatinine, 14% 3mg/kg, 31% 10mg/kg. Hypokalemia, 16% 3mg/kg, 30% 10mg/kg. Safety profiles for each treatment group comparable to previously reported safety data for AmBisome.")
66
PK/PD voriconazole 181 dosages 52 patients
Background. Voriconazole is the therapy of choice for aspergillosis and a new treatment option for candidiasis. Liver disease, age, genetic polymorphism of the cytochrome CYP2C19, and comedications influence voriconazole metabolism. Large variations in voriconazole pharmacokinetics may be associated with decreased efficacy or with toxicity. Methods. This study was conducted to assess the utility of measuring voriconazole blood levels with individualized dose adjustments. Results. A total of 181 measurements with high-pressure liquid chromatography were performed during 2388 treatment days in 52 patients. A large variability in voriconazole trough blood levels was observed, ranging from 1 mg/L (the minimum inhibitory concentration at which, for most fungal pathogens, 90% of isolates are susceptible) in 25% of cases to 15.5 mg/L (a level possibly associated with toxicity) in 31% of cases. Lack of response to therapy was more frequent in patients with voriconazole levels 1 mg/L (6 [46%] of 13 patients, including 5 patients with aspergillosis, 4 of whom were treated orally with a median dosage of 6 mg/kg per day) than in those with voriconazole levels 11 mg/L (15 [12%] of 39 patients; ). Blood levels 11 Pp.02 mg/L were reached after increasing the voriconazole dosage, with complete resolution of infection in all 6 cases. Among 16 patients with voriconazole trough blood levels 15.5 mg/L, 5 patients (31%) presented with an encephalopathy, including 4 patients who were treated intravenously with a median voriconazole dosage of 8 mg/kg per day, whereas none of the patients with levels 5.5 mg/L presented with neurological toxicity (Pp.002). Comedication with omeprazole possibly contributed to voriconazole accumulation in 4 patients. In all cases, discontinuation of therapy resulted in prompt and complete neurological recovery. Conclusions. Voriconazole therapeutic drug monitoring improves the efficacy and safety of therapy in severely ill patients with invasive mycoses. Voriconazole is the first choice therapy for i 181 dosages 52 patients
 in 25% of cases to 15.5 mg/L (a level possibly associated with toxicity) in 31% of cases. Lack of. response to therapy was more frequent in patients with voriconazole levels 1 mg/L (6 [46%] of 13 patients, including 5 patients with aspergillosis, 4 of whom were treated orally with a median dosage of 6 mg/kg per day) than in those with voriconazole levels 11 mg/L (15 [12%] of 39 patients; ). Blood levels 11 Pp.02 mg/L were. reached after increasing the voriconazole dosage, with complete resolution of infection in all 6 cases. Among 16. patients with voriconazole trough blood levels 15.5 mg/L, 5 patients (31%) presented with an encephalopathy, including 4 patients who were treated intravenously with a median voriconazole dosage of 8 mg/kg per day, whereas. none of the patients with levels 5.5 mg/L presented with neurological toxicity (Pp.002). Comedication with. omeprazole possibly contributed to voriconazole accumulation in 4 patients. In all cases, discontinuation of therapy. resulted in prompt and complete neurological recovery. Conclusions. Voriconazole therapeutic drug monitoring improves the efficacy and safety of therapy in severely. ill patients with invasive mycoses. Voriconazole is the first choice therapy for i. 181 dosages. 52 patients.")
67
VRZ dosages Pascual A - Clinical Infectious Diseases 2008; 46:201–11
Background. Voriconazole is the therapy of choice for aspergillosis and a new treatment option for candidiasis. Liver disease, age, genetic polymorphism of the cytochrome CYP2C19, and comedications influence voriconazole metabolism. Large variations in voriconazole pharmacokinetics may be associated with decreased efficacy or with toxicity. Methods. This study was conducted to assess the utility of measuring voriconazole blood levels with individualized dose adjustments. Results. A total of 181 measurements with high-pressure liquid chromatography were performed during 2388 treatment days in 52 patients. A large variability in voriconazole trough blood levels was observed, ranging from 1 mg/L (the minimum inhibitory concentration at which, for most fungal pathogens, 90% of isolates are susceptible) in 25% of cases to 15.5 mg/L (a level possibly associated with toxicity) in 31% of cases. Lack of response to therapy was more frequent in patients with voriconazole levels 1 mg/L (6 [46%] of 13 patients, including 5 patients with aspergillosis, 4 of whom were treated orally with a median dosage of 6 mg/kg per day) than in those with voriconazole levels 11 mg/L (15 [12%] of 39 patients; ). Blood levels 11 Pp.02 mg/L were reached after increasing the voriconazole dosage, with complete resolution of infection in all 6 cases. Among 16 patients with voriconazole trough blood levels 15.5 mg/L, 5 patients (31%) presented with an encephalopathy, including 4 patients who were treated intravenously with a median voriconazole dosage of 8 mg/kg per day, whereas none of the patients with levels 5.5 mg/L presented with neurological toxicity (Pp.002). Comedication with omeprazole possibly contributed to voriconazole accumulation in 4 patients. In all cases, discontinuation of therapy resulted in prompt and complete neurological recovery. Conclusions. Voriconazole therapeutic drug monitoring improves the efficacy and safety of therapy in severely ill patients with invasive mycoses. Voriconazole is the first choice therapy for i Pascual A - Clinical Infectious Diseases 2008; 46:201–11
 in 25% of cases to 15.5 mg/L (a level possibly associated with toxicity) in 31% of cases. Lack of. response to therapy was more frequent in patients with voriconazole levels 1 mg/L (6 [46%] of 13 patients, including 5 patients with aspergillosis, 4 of whom were treated orally with a median dosage of 6 mg/kg per day) than in those with voriconazole levels 11 mg/L (15 [12%] of 39 patients; ). Blood levels 11 Pp.02 mg/L were. reached after increasing the voriconazole dosage, with complete resolution of infection in all 6 cases. Among 16. patients with voriconazole trough blood levels 15.5 mg/L, 5 patients (31%) presented with an encephalopathy, including 4 patients who were treated intravenously with a median voriconazole dosage of 8 mg/kg per day, whereas. none of the patients with levels 5.5 mg/L presented with neurological toxicity (Pp.002). Comedication with. omeprazole possibly contributed to voriconazole accumulation in 4 patients. In all cases, discontinuation of therapy. resulted in prompt and complete neurological recovery. Conclusions. Voriconazole therapeutic drug monitoring improves the efficacy and safety of therapy in severely. ill patients with invasive mycoses. Voriconazole is the first choice therapy for i. Pascual A - Clinical Infectious Diseases 2008; 46:201–11.")
68
Objectifs d’une association
Objectifs Pertinence (Candida) Elargir le spectre Large pour la plupart des molécules (mais quelques “trous”) Obtenir une synergie AmB + 5FC (les autres ?) Réduire le risque de résistance Phénomène peu fréquent Réduire le risque de toxicité AmB + 5FC Améliorer la diffusion tissulaire Azolés +++, 5FC « efficacité prouvée de la bithérapie dans les infections bactériennes?… »
 Elargir le spectre Large pour la plupart des molécules (mais quelques trous ) Obtenir une synergie AmB + 5FC (les autres ) Réduire le risque de résistance Phénomène peu fréquent. Réduire le risque de toxicité AmB + 5FC. Améliorer la diffusion tissulaire Azolés +++, 5FC. « efficacité prouvée de la bithérapie dans les infections bactériennes … »")
69
Etudes in vitro des associations antifongiques sur Candida sp

70
Et la flucytosine… ? Test de sensibilité in vitro : C. albicans 97 % ; C. glabrata 99 % ; C. krusei 5 % (1) Quand associer la flucytosine ? [+ AmB] Pour certaines localisations (méningite, endocardite, infection urinaire, ± oeil ± os) (2) Rôle de la caspofungine + 5FC dans les candidoses sévères ? (péritonite, endocardite) (3) 1) Pfaller MA et al. AAC 2002; 46: 2) Recommandations de l’IDSA ; Pappas PG et al. CID 2004; 38: 3) Choukroun G et al. Transplantation 2006; 82: MYCENDO study France.
 (2) Rôle de la caspofungine + 5FC dans les candidoses sévères (péritonite, endocardite) (3) 1) Pfaller MA et al. AAC 2002; 46: ) Recommandations de l’IDSA ; Pappas PG et al. CID 2004; 38: ) Choukroun G et al. Transplantation 2006; 82: MYCENDO study France.")
71
Ampho B + fluco vs fluco + placebo
Candidémies chez les non-neutropéniques Critères AmB + F F + P p (107) (104) Succès 68 % 56 % 0,045* Mortalité J NS Echec fungique ,02 Créatinine ,02 * J30 en Logrank : NS D’après Rex et al. Clin Infect Dis 2003;
 (104) Succès 68 % 56 % 0,045* Mortalité J NS. Echec fungique ,02. Créatinine ,02. * J30 en Logrank : NS. D’après Rex et al. Clin Infect Dis 2003;")
72
« Les recommandations françaises sont d’associer la flucytosine à l’AmB dans les endocardites, les méningites et les endophtalmies, en raison de sa bonne diffusion [8]. L’IDSA recommande l’association AmB plus flucytosine dans les mêmes situations que le consensus français, mais aussi dans les candiduries et les atteintes sévères intraabdominales [9,39].
![« Les recommandations françaises sont d’associer la flucytosine à l’AmB dans les endocardites, les méningites et les endophtalmies, en raison de sa bonne diffusion [8].](http://slideplayer.fr/slide/1580221/4/images/72/%C2%AB+Les+recommandations+fran%C3%A7aises+sont+d%E2%80%99associer+la+flucytosine+%C3%A0+l%E2%80%99AmB+dans+les+endocardites%2C+les+m%C3%A9ningites+et+les+endophtalmies%2C+en+raison+de+sa+bonne+diffusion+%5B8%5D..jpg "L’IDSA recommande l’association AmB plus flucytosine dans les mêmes situations que le consensus français, mais aussi dans les candiduries et les atteintes sévères intraabdominales [9,39]..")
73
Haut risque de C. glabrata ou krusei ?
Traitement empirique Traitement des candidoses invasives Recommandations IDSA 2008 A mettre en œuvre en fonction : Evaluation clinique des facteurs de risque ou/et Marqueurs sériques de candidose invasive ou/et Culture positive Traitement empirique Oui Non fluconazole echinocandine Pré-exposition azolé ? Haut risque de C. glabrata ou krusei ? L’amphotéricine B et ses formulations lipidiques sont des alternatives en cas d’intolérance ou de non disponibilité des autres traitements

74
Candidémies - suite Traitement des candidoses invasives Recommandations IDSA 2008
Réévaluation du traitement Stabilité clinique Oui Non Connaissance du germe C. parapsilosis C. lusitaniae ou autre germe C. glabrata Sensibilité au fluconazole Oui Non fluconazole echinocandine Durée du traitement : 2 semaines après stérilisation hémocultures et résolution des symptômes Voriconazole non recommandé en 1è intention. A réserver à certains cas précis, relais oral ou tt de C. krusei

75
Il faut traiter vite et bien
Augmentation du nombre de molécules Les principales études cliniques Optimisation PK/PD, doses élevées associations Qui traiter en réanimation?

76
Empirical Therapy In the febrile non-neutropenic patient?
Early treatment is theoretically attractive IDSA Guidelines “The specific basis for selecting non-neutropenic patients who should receive empiric antifungal therapy is unclear, but should be based on at least one of the following: clinical assessment of risk factors, serologic markers for invasive candidiasis, and/or culture data from non-sterile sites (BIII).” My rules Antibiotics, lines, no other source, and… Colonized somewhere with Candida I don’t distinguish sites: anywhere works for me The more sites or fungus the better (see work of Pittet) Prophylaxis? Even hazier Rex summary of the IDSA guidelines 2008
. My rules. Antibiotics, lines, no other source, and… Colonized somewhere with Candida. I don’t distinguish sites: anywhere works for me. The more sites or fungus the better (see work of Pittet) Prophylaxis Even hazier. Rex summary of the IDSA guidelines")
78
Fongiday® Elie Azoulay, Hervé Dupont, Jean-Paul Stahl, Alexis Tabah, Philippe Montravers, Olivier Lortholary, Bertrand Guidet, Jean-François Timsit. INSERM/UJF U 823 Grenoble Attaché de recherche: Loïc Ferrand Biostatisticien : Adrien Français Soutien : Pfizer

79
Descriptif de la base 169 centres 2047 patients 1893 sans TAF
154 (7.5%) avec un TAF 2032 suivi J28 ok (99.3%) 79
 avec un TAF suivi J28 ok. (99.3%) 79.")
80
Candida Score Candida score TAF - (n=1893) TAF + (n=154)
(99.6) 2 (0.4) (98.3) 8 (1.7) (92.7) 25 (7.3) (87.6) 43 (12.4) (83.0) 46 (17.0) (55.9) 30 (44.1) Test de tendance p<10-4 80
 2 (0.4) (98.3) 8 (1.7) (92.7) 25 (7.3) (87.6) 43 (12.4) (83.0) 46 (17.0) 5 38 (55.9) 30 (44.1) Test de tendance p<")
81
Molécules utilisées le jour J
Sans les 16 champignons filamenteux Fluconazole 67.9% Voriconazole 2.9% Caspofongine 22.6% Anidulafongine 0.7% Ambisome 5.1% Abelcet Traitement basé sur l’antifongigramme ? 27% 81

82
Motif de prescription des antifongiques à Fongiday après révision du comité (sans les 16 champignons) 20% des motifs révisés Curatif sur infection documentée 27.5% Empirique basée sur une suspicion clinique de candidémie 18.1% Neutropénie fébrile 10.9% Prophylactique basée sur des facteurs de risque de candidémie 17.4% Précoce ou préemptive basée sur une colonisation à Candida 34.8% Du fait d'une instabilité hémodynamique du patient 13% Autre raison 5.1% 82

83
Traitement tardif préjudiciable Pas de moyen fiables de diagnostic
Traitement préemptif? question de plus en plus fréquente, pas de réponse… Traitement tardif préjudiciable Pas de moyen fiables de diagnostic HC tardives voir négatives Tests diagnostiques nouveaux peu convaincant 13 B –D glucane Platelia- Manane / Antimanane PCR

84
Facteurs de risque de candidémie
Antibiothérapie à spectre large Immunodépression (neutropénie, chimiothérapie, GDM, corticoïdes) Cathéter central, nutrition parentérale Insuffisance rénale, dialyse Chirurgie abdominale majeure Brûlure > 50 % Traumatisme grave Sévérité des patients de réanimation Colonisation 2 sites Rex & Sobel Clin Infect Dis 2001; 32: 1191
 Cathéter central, nutrition parentérale. Insuffisance rénale, dialyse. Chirurgie abdominale majeure. Brûlure > 50 % Traumatisme grave. Sévérité des patients de réanimation. Colonisation 2 sites. Rex & Sobel Clin Infect Dis 2001; 32:")
85
1655 patients non neutropéniques > 7 jours (73 ICUs, Espagne)
Leon et al - Eur J Clin Microbiol Infect Dis- Aout 2008 1655 patients non neutropéniques > 7 jours (73 ICUs, Espagne) 852 colonisés (52%) (Unifocal 379 patients (43.9%), multifocal 485 patients (56.1%)) 92 infections prouvées (5.5%) (55 candidémies, 6 endophtalmie, 25 ponction site stérile) The purpose of this paper is to determine the incidence of fungal colonization and infection in non-neutropenic critically ill patients and to identify factors favoring infection by Candida spp. A total of 1,655 consecutive patients (>18 years of age) admitted for >/=7 days to 73 medical-surgical Spanish intensive care units (ICUs) participated in an observational prospective cohort study. Surveillance samples were obtained once a week. One or more fungi were isolated in different samples in 59.2% of patients, 94.2% of which were Candida spp. There were 864 (52.2%) patients with Candida spp. colonization and 92 (5.5%) with proven Candida infection. In the logistic regression analysis risk factors independently associated with Candida spp. infection were sepsis (odds ratio [OR] = 8.29, 95% confidence interval [CI] ), multifocal colonization (OR = 3.49, 95% CI ), surgery (OR = 2.04, 95% CI ), and the use of total parenteral nutrition (OR = 4.37, 95% CI ). Patients with Candida spp. infection showed significantly higher in-hospital and intra-ICU mortality rates than those colonized or non-colonized non-infected (P < 0.001). Fungal colonization, mainly due to Candida spp., was documented in nearly 60% of non-neutropenic critically ill patients admitted to the ICU for more than 7 days. Proven candidal infection was diagnosed in 5.5% of cases. Risk factors independently associated with Candida spp. infection were sepsis, multifocal colonization, surgery, and the use of total parenteral nutrition.
 852 colonisés (52%) (Unifocal 379 patients (43.9%), multifocal 485 patients (56.1%)) 92 infections prouvées (5.5%) (55 candidémies, 6 endophtalmie, 25 ponction site stérile) The purpose of this paper is to determine the incidence of fungal colonization and infection in non-neutropenic critically ill patients and to identify factors favoring infection by Candida spp. A total of 1,655 consecutive patients (>18 years of age) admitted for >/=7 days to 73 medical-surgical Spanish intensive care units (ICUs) participated in an observational prospective cohort study. Surveillance samples were obtained once a week. One or more fungi were isolated in different samples in 59.2% of patients, 94.2% of which were Candida spp. There were 864 (52.2%) patients with Candida spp. colonization and 92 (5.5%) with proven Candida infection. In the logistic regression analysis risk factors independently associated with Candida spp. infection were sepsis (odds ratio [OR] = 8.29, 95% confidence interval [CI] ), multifocal colonization (OR = 3.49, 95% CI ), surgery (OR = 2.04, 95% CI ), and the use of total parenteral nutrition (OR = 4.37, 95% CI ). Patients with Candida spp. infection showed significantly higher in-hospital and intra-ICU mortality rates than those colonized or non-colonized non-infected (P < 0.001). Fungal colonization, mainly due to Candida spp., was documented in nearly 60% of non-neutropenic critically ill patients admitted to the ICU for more than 7 days. Proven candidal infection was diagnosed in 5.5% of cases. Risk factors independently associated with Candida spp. infection were sepsis, multifocal colonization, surgery, and the use of total parenteral nutrition.")
86
Facteurs de risque de candidose invasive
Léon et al – Crit Care Med 2006

87
Clinical prediction rule validation on a retrospective international cohort Ostrosky-Zeichner – 48th ICAAC- M 1853

88
Clinical prediction rule validation on a retrospective international cohort Ostrosky-Zeichner – 48th ICAAC- M 1853 CPR CPR + Col Abdominal surg. Se 86% 66% 80% Sp 65% 88% 75% PPV 3% 8% 4% NPV 99% % patients with IC 4.7% 9.3% % patients treated 35.5% 12.7% 25.7% % patients captured 83% 67%

89
Conclusion Patients de plus en plus à risque
Beaucoup de traitement plutôt plus efficace sur les candidémies Candidémie très rare Traitement préemptif fréquent mais avec une fort taux de sur-traitement Aucune étude ne permet de prouver son intérêt en réanimation

Présentations similaires











 Biomarqueurs IHC (n = 412) Séquençage (n = 418) 200 patients évaluables pour les facteurs pronostiques cliniques et biologiques Comparaison.>")







