Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Laurent PAPAZIAN Réanimation médicale Hôpital Sainte-Marguerite
Doit-on adopter une stratégie diagnostique des pneumonies en réanimation spécifique à " l’immunodéprimé " ? Herpesviruses have an envelope surrounding an icosahedral capsid, approximately 100nm in diameter, which contains the dsDNA genome Laurent PAPAZIAN Réanimation médicale Hôpital Sainte-Marguerite U R

2
Incidence des pneumonies de l’ID
Tx médullaires: 30-60% Tx hépatique: 11-15% Tx cardiaque: 14-38% Tx pulmonaire: 50% Neutropénie: 0,5-10% VIH, cancer…

3
Immunodépression Chimiothérapie Corticoïdes Imurel et Endoxan
Immunité cellulaire et immunité humorale Corticoïdes Altération fonction PNN et macrophages Imurel et Endoxan Inhibition production PNN et lympho Cyclosporine, tacrolimus Modulation fonctions lympho T

4
Autres facteurs Mécaniques Nutrition Colonisation Barrières
Hypoalbuminémie adhésion BGN Altération fonctions PNN Colonisation Oro-pharynx Sinus Estomac

5
Etiologies des pneumonies en hémato-cancéro
Bactéries Communes (SA, Pneumocoque, P. aeruginosa, entérobact, HI) Intra-cellulaires Legionella Chlamydia Mycoplasma Nocardia sp., Actinomyces israeli Mycobactéries
 Intra-cellulaires. Legionella. Chlamydia. Mycoplasma. Nocardia sp., Actinomyces israeli. Mycobactéries.")
6
P. jiroveci Fungiques Virales Aspergilloses Candida (candidémie)
Fusarioses, zygomycetes Histoplasmose, blastomycose, coccidioidomycose Virales Resp: Rhino, Influenza, Parainfluenza, VRS Herpesvirus: HSV, CMV, HVZ, HHV6 Adenovirus

7
Germes, LBA et type de patients
Joos et al. Respir Med 2007

8
Germes, LBA et type de patients
Joos et al. Respir Med 2007

9
Germes, LBA et type de patients
Joos et al. Respir Med 2007

10
Germes, LBA et type de patients
Joos et al. Respir Med 2007

11
Etiologies chez HIV

12
Etiologies en Tx médullaire et chimio lourdes

13
Etiologies en cas de tumeurs solides

15
Cinétique des infections au décours de la Tx médullaire
Soubani A.O. CCM 2006

16
Cinétique des infections au décours de la Tx médullaire
Causes non-infectieuses HR intra-alvéolaire DAH = diffuse alveolar hemorrhage / IPS = idiopathic pneumonia syndrome: symptômes pneumonie mais sans infection documentée / engraftment syndrome = sortie de neutropénie avec aug CK et ALI / BO = bronchiolite oblitérante Soubani A.O. CCM 2006

17
Connaître le type de déficit immunitaire - GdM

18
Pneumonies et Tx médullaire

19
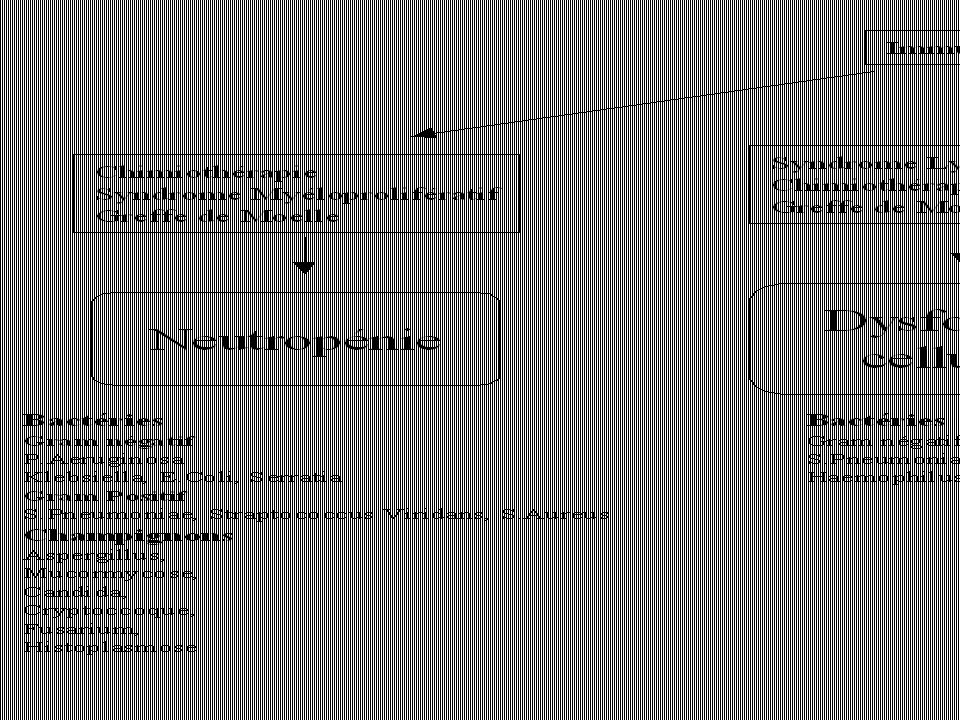
Neutropénie Transplantation Greffe de Moelle 1 Mois 3 Mois 6 Mois
Bactérien Fungique Neutropénie Rejet Chronique Virus Transplantation Greffe de Moelle Virus - Champignons > Autres CMV > P jirovecii Bactéries Virus Respiratoires Temps 1 Mois 3 Mois 6 Mois

20
Pneumocystis BAL Gargarismes: PCR
Coloration de référence: Papanicolaou Gomori (moins sensible) quand Papanicolaou est négatif ? PCR: plus sensible, moins spécifique Gargarismes: PCR
 quand Papanicolaou est négatif PCR: plus sensible, moins spécifique. Gargarismes: PCR.")
21
Le contexte Patient pris en charge en réanimation pour détresse respiratoire et échec de la prise en charge probabiliste

23
Difficultés du diagnostic
Manque de spécificité des signes cliniques et radiologiques "Invasivité" des techniques de diagnostic Traitement anti-infectieux antérieur

24
Diagnostic chez immuno-déprimés,VIH-
Rano et al. Thorax 2001 200 patients

25
Rentabilité LBA dans la vraie vie…
Hémopathie maligne, n = 95 Antibiothérapie à large spectre + anti-fungique LBA contributif: 29/95 BGN, 40% CGP, 35% Mycobactérie, 11% Infection fungique, 11% CMV, 3% Hohenadel et al. Thorax 2001

26
Pneumonie - pas pneumonie ?
99 patients hémato 122 épisodes, 135 LBA Examens « classiques » + PCR: Pneumocystis, CMV, Legionella sp., mycobacteries, Mycoplasma pneumoniae, and Chlamydia pneumoniae Aspergillus antigénémie Hohenthal et al. Eur J Haematol 2005

27
Pneumonie chez le malade hémato
Identification microbienne: 35,6% (48/135) Bactéries cultures quantitatives: 3 (2,2%) cultures spéciales: 4 (3%) Virus respiratoire: 10 (8,2%) PCR Pneumocystis: 21 PCR CMV positive: 18 Aspergillus antigénémie: 7 Modification traitement anti-infectieux: 27 épisodes (22,1%)
 Bactéries. cultures quantitatives: 3 (2,2%) cultures spéciales: 4 (3%) Virus respiratoire: 10 (8,2%) PCR Pneumocystis: 21. PCR CMV positive: 18. Aspergillus antigénémie: 7. Modification traitement anti-infectieux: 27 épisodes (22,1%)")
28
Pneumonie chez le malade hémato
Identification microbienne: 35,6% (48/135) Bactéries cultures quantitatives: 3 (2,2%) cultures spéciales: 4 (3%) Virus respiratoire: 10 (8,2%) PCR Pneumocystis: 21 PCR CMV positive: 18 Aspergillus antigénémie: 7 Modification traitement anti-infectieux: 27 épisodes (22,1%)
 Bactéries. cultures quantitatives: 3 (2,2%) cultures spéciales: 4 (3%) Virus respiratoire: 10 (8,2%) PCR Pneumocystis: 21. PCR CMV positive: 18. Aspergillus antigénémie: 7. Modification traitement anti-infectieux: 27 épisodes (22,1%)")
29
Pneumonie chez le malade hémato
Identification microbienne: 35,6% (48/135) Bactéries cultures quantitatives: 3 (2,2%) cultures spéciales: 4 (3%) Virus respiratoire: 10 (8,2%) PCR Pneumocystis: 21 PCR CMV positive: 18 Aspergillus antigénémie: 7 Modification traitement anti-infectieux: 27 épisodes (22,1%)
 Bactéries. cultures quantitatives: 3 (2,2%) cultures spéciales: 4 (3%) Virus respiratoire: 10 (8,2%) PCR Pneumocystis: 21. PCR CMV positive: 18. Aspergillus antigénémie: 7. Modification traitement anti-infectieux: 27 épisodes (22,1%)")
30
Causes non-infectieuses

31
Rentabilité fibroscopie
104 immunodéprimés non-VIH BW = bronchial washing Jain et al. Chest 2004

32
Contribution OLB: 100% ! Jain et al. Chest 2004

33
Rosen et Narasimhan CCM 2006
DR chez un patient VIH+ Rosen et Narasimhan CCM 2006

34
LBA - BTB Bulpa et al. ERJ 2003

35
Complications… Bulpa et al. ERJ 2003

36
TDM… Pneumonie à Pneumocystis chez VIH. Drain tho en place
Pneumocystis jiroveci (formerly classified Pneumocystis carinii) has always been a major cause of illness and death in patients with HIV infection. Once thought to be a parasite, genomic analysis revealed that P. jiroveci is in fact a fungus that infects only humans, whereas P. carinii is pathogenic only in immunodeficient rats. Despite the change in taxonomy of this pathogen, the term PCP is still acceptable shorthand for Pneumocystis
 has always been a major cause of illness and death in patients with HIV infection. Once thought to be a parasite, genomic analysis revealed that P. jiroveci is in fact a fungus that infects only humans, whereas P. carinii is pathogenic only in immunodeficient rats. Despite the change in taxonomy of this pathogen, the term PCP is still acceptable shorthand for Pneumocystis.")
37
Présentation RX et orientation étiologique
Rosen et Narasimhan CCM 2006

38
Park DR Respir Care 2005

39
Localisation Rouby et al. ARRD 92

40
HSV et patients non-immunodéprimés
Porteous et al. Crit Care Med 84 % oral shedding

41
HSV et patients non-immunodéprimés
Porteous et al. Crit Care Med 84 % oral shedding

42
HSV et patients non-immunodéprimés
Porteous et al. Crit Care Med 84 % oral shedding

45
Critères cliniques Clinical Pulmonary Infection Score
* temperature °C > 36.5 and < 38.4 : 0 point > 38.5 and < 38.9 : 1 point > 39 or < 36 : 2 points * WBC, mm-3 < 4,000 and < 11,000 : 0 point < 4,000 or > 11,000 : 1 point + band forms > 500 = + 1 point * tracheal secretions < 14 + of tracheal secretions = 0 point > 14 + of tracheal secretions = 1 point + purulent secretions = + 1 point * PaO2/FiO2, mmHg > 240 or ARDS = 0 point < 240 and no evidence of ARDS = 1 point * pulmonary radiography no infiltrate = 0 point diffused (or patchy) infiltrate = 1 point localized infiltrate = 2 points * culture of TA (semiquantitative : 0,1,2 or 3 +) pathogenic bacteria cultured < 1 + or no growth = 0 point pathogenic bacteria cultured > 1 = 1 point + same bacteria on Gram stain > 1 + = + 1 point Pugin et al. ARRD 91
 infiltrate = 1 point. localized infiltrate = 2 points. * culture of TA (semiquantitative : 0,1,2 or 3 +) pathogenic bacteria cultured < 1 + or no growth = 0 point. pathogenic bacteria cultured > 1 = 1 point + same bacteria. on Gram stain > 1 + = + 1 point. Pugin et al. ARRD 91.")
46
Luna et al. CCM 2003

47
BAL under fiberscopy technical considerations
oro- or naso-tracheal tube > 7 mm FiO2 = 1, sedation ± curarisation aliquots ( ml) 1st aliquot discarded
 1st aliquot discarded.")
48
BAL under fiberscopy tolerance
Papazian et al. Chest 93 PaO2/FIO2 * p < 0.05

49
Non-directed BAL : clinical studies
n VAP threshold sens. spec. DPC SQ 70% 69% PAC no 100% 75% duodenography BI > 5 73% 96% Ballard % 96%

50
Reproductibilité des examens invasifs
BTP 24% des micro-organismes de part et d’autre du seuil de 103 cfu/ml LBA 33% des micro-organismes de part et d’autre du seuil de 104 cfu/ml Timsit et al. Chest 93 Gerbeaux et al. AJRCCM 98

51
Défaut de sensibilité de la brosse
Johanson et al. ARRD 88

52
Tracheal aspirates diagnostic accuracy
El-Ebiary et al. ARRD 93 * reference : blood or pleural cultures, histology * 54 patients (26 with pneumonia) TA 105 TA 105 PSB 103 PSB 103
 TA TA PSB PSB")
53
Etudes comparatives avec histologie
pour le diagnostic de VAP bactérienne ! sensibilité/spécificité BTP LBA AT Comb CPIS seuil = Torrès AJRCCM 94 36/50 50/ Marquette AJRCCM 95 58/89 47/10067/75 67/75 53/ Chastre AJRCCM 95 82/89 91/ Papazian AJRCCM 95 33/95 50/95 72/80 56/95 44/10067/8072/85

54
Pathogens associated with inadequate antimicrobial treatment
Kollef MH CID 2000

55
Présentation RX J0 J15

56
Groundglass attenuation
J15

57
25 pneumonies à CMV prouvées histologiquement
CMV et VAP Etude rétrospective (n = 2795 patients) SDRA et VM > 7 jours + histologie Exclusion : hémopathie maligne, VIH, corticoïdes au long cours, chimiothérapie Autopsies (n = 60), OLB (n = 26) 25 pneumonies à CMV prouvées histologiquement - CMV seul dans 88% des cas Papazian et al. Anesthesiology 1996
 SDRA et VM > 7 jours + histologie. Exclusion : hémopathie maligne, VIH, corticoïdes au long cours, chimiothérapie. Autopsies (n = 60), OLB (n = 26) 25 pneumonies à CMV prouvées histologiquement. - CMV seul dans 88% des cas. Papazian et al. Anesthesiology")
58
Diagnostic à l’admission
début: 18 j ( ) IgG+ à l’admission 13/18 Diagnostic à l’admission Défaillance respiratoire post-op cancer (oesophage, estomac, poumon) : n = 6 chirurgie cardiaque : n = 4 Péritonite: n = 3 BPCO: n = 5 Coma: n = 4 Méningite: n = 1 Myocardite: n = 1 EP: n = 1
 IgG+ à l’admission 13/18. Diagnostic à l’admission. Défaillance respiratoire post-op. cancer (oesophage, estomac, poumon) : n = 6. chirurgie cardiaque : n = 4. Péritonite: n = 3. BPCO: n = 5. Coma: n = 4. Méningite: n = 1. Myocardite: n = 1. EP: n = 1.")
59
Ventilation mécanique et HSV
Plus âgés et plus souvent ventilés que les immunodéprimés Pas d’herpesvirus dans le LBA de sujets sains 26% des LBA de 132 patients Schuller et al. Am J Med 93 Tarp et al. Eur Respir J 2001 Prellner: 47% burns Prellner et al. Scand J Infect Dis 92

60
Portage HSV-1 chez les patients ventilés
Oro-pharynx et trachée (PCR) 393 patients HSV-1: 27% Corrélation age ou APACHE II – portage HSV-1 Trachée et sang (culture) 95 patients HSV-1: 23% Oro-pharynx (culture) 617 patients HSV-1: 21% Ong et al. J Med Virol 2004 Increased hospital mortality in shedders Cook et al. Crit Care Med 2003 Bruynseels et al. The Lancet 2003
 393 patients. HSV-1: 27% Corrélation age ou APACHE II – portage HSV-1. Trachée et sang (culture) 95 patients. HSV-1: 23% Oro-pharynx (culture) 617 patients. HSV-1: 21% Ong et al. J Med Virol Increased hospital mortality in shedders. Cook et al. Crit Care Med Bruynseels et al. The Lancet")
61
HSV et pathogénicité Patients SDRA: double-aveugle acyclovir-placebo %
Tuxen et al. ARRD 87

62
HSV et pathogénicité Patients SDRA: double-aveugle acyclovir-placebo %
Tuxen et al. ARRD 87

63
Bruynseels et al. The Lancet 2003
HSV et PAV ? Bruynseels et al. The Lancet 2003 mortalité p = 0.003 Weekly mini BAL MLR showed that the difference in mortality was related to disease severity TRT ?

64
Bruynseels et al. The Lancet 2003
HSV et PAV ? Bruynseels et al. The Lancet 2003 mortalité p = 0.45 p = 0.003 Weekly mini BAL MLR showed that the difference in mortality was related to disease severity TRT ?

65
Cytomégalovirus

66
Gerna and Lilleri Herpes 2006
Antigénémie Identifie les GB qui expriment la phosphoprotéine pp65 dans leur noyau Précocité Sensibilité In high-risk SOT recipients (i.e. the HCMV-seronegative), primary HCMV infection was treated on first antigenaemia positivity in blood Gerna and Lilleri Herpes 2006
, primary HCMV infection was treated on first antigenaemia positivity in blood. Gerna and Lilleri Herpes")
67
CMV = HSV ? Cook et al. Crit Care Med 2003 *

68
CMV = HSV ? Cook et al. Crit Care Med 2003 *

69
CMV = HSV ? Cook et al. Crit Care Med 2003 *

70
CMV: signification ? 237 patients: au moins 1 antigénémie
Incidence: 40/237 (17%) Type d’admission: surg,med,trauma Jaber et al. Chest 2005
 Type d’admission: surg,med,trauma. Jaber et al. Chest")
71
Quels malades ? Jaber et al. Chest 2005

72
Morbidité – Mortalité et réanimation
* * * * Mais: + de steroids, + d’IRA et CMV n’est pas FdR indépendant Jaber et al. Chest 2005

73
Tableau “typique”… - Vers la 2ème – 3ème semaine - Fièvre
Détérioration de l’état respiratoire Bactériologie négative - Petite note cholestatique

74
Performance diagnostique
Papazian et al. Anesthesiology 1998

78
Photomicrograph (original magnification, 400; hematoxylin-eosin stain) shows three large nuclei containing eosinophilic inclusion bodies (arrows) within hyperplastic pneumocytes. x 400 HES

79
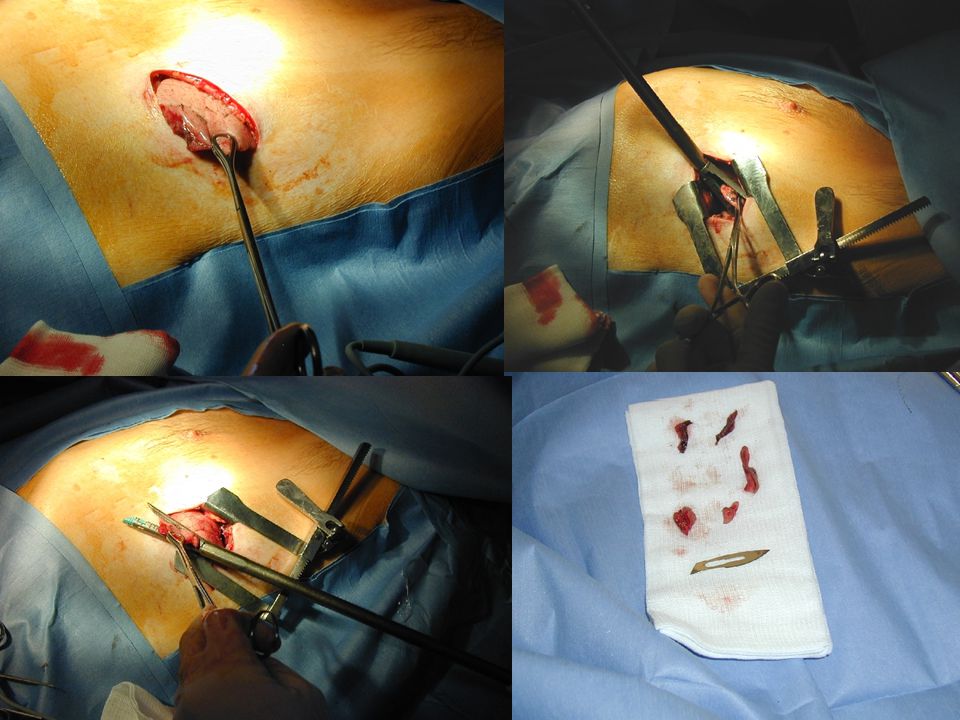
OLB: résultats 100 SDRA 100 OLB

80
OLB et SDRA n PEEP PaO2/FiO2 morbidité
Hill JTCVS bed 6.5 (0 - 15) 84 ( ) 1 air leak 1HR 1inf Ashbaugh AS ? Costa Auler EJRD OR ( ) ? Warner ARRD OR ? ? ? Meduri Chest OR ? ? ? Canver JCVS OR 9 ± ? air leaks 2 PNO Meduri Chest OR ? ? air leak Papazian Anesth bed/OR 10 ± ( ) 5 air leak 1HR PNO Patel Chest OR 10 ± ± death, 1 HR, 12 air leaks
 84 ( ) 1 air leak 1HR 1inf. Ashbaugh AS Costa Auler EJRD 86 5 OR ( ) Warner ARRD OR Meduri Chest 91 7 OR Canver JCVS OR 9 ± 1 6 air leaks 2 PNO. Meduri Chest OR 1 air leak. Papazian Anesth bed/OR 10 ± ( ) 5 air leak 1HR PNO. Patel Chest OR 10 ± ± 61 1 death, 1 HR, 12 air leaks.")
81
Modifications thérapeutiques
n modifications Hill JTCVS % Warner ARRD % Canver JCVS % Papazian Anest % Patel Chest %

82
OLB biopsie contributive biopsie non-contributive
Papazian et al. CCM 2007

83
Mechanical complications

84
New treatment after OLB results
78 patients

85
Photomicrograph (original magnification, x 40; hematoxylin-eosin stain) shows diffuse interstitial and intraalveolar fibroblastic proliferation (arrows) with some mononuclear cell infiltration (diffuse alveolar damage, organizing stage) x 40 HES

86
CMV et fibrose Souris Péritonite Evaluation à 3 semaines CMV –
Réactivation CMV Réactivation CMV + Gancyclovir Boxplot comparison of pulmonary fibrosis in latently infected (CMV), noninfected (CMV), and ganciclovir-treated (CMVGCV) mice 3 wks after cecal ligation and puncture. White belts indicate the median value. Boxes give the range between quartiles (25th and 75th percentiles). Notched black regions are 95% confidence intervals for the medians, and the dots indicate the full range of the distributions. Because distributions of pulmonary fibrosis scores are nonnormal, nonparametric tests were used to discern differences among study groups at day 21. Post hoc comparisons of pairs of groups were made using the Mann-Whitney-Wilcoxon test (nonparametric t-test). CMV reactivation was related to significant increases in pulmonary fibrosis compared with healthy controls after CLP (p ). Blocking CMV reactivation with ganciclovir after CLP appeared to prevent this increased level of fibrosis, as fibrosis was significantly lower in GCV-treated mice than in nontreated mice (p .0002) Cook et al. Crit Care Med 2006
, noninfected (CMV), and ganciclovir-treated (CMVGCV) mice 3 wks after cecal ligation and puncture. White belts indicate the median value. Boxes give the range between quartiles (25th and 75th percentiles). Notched black regions are 95% confidence intervals for the medians, and the dots indicate the full range of the distributions. Because distributions of pulmonary fibrosis scores are nonnormal, nonparametric tests were used to discern differences among study groups at day 21. Post hoc comparisons of pairs of groups were made using the Mann-Whitney-Wilcoxon test (nonparametric t-test). CMV reactivation was related to significant increases in pulmonary fibrosis compared with healthy controls after CLP (p .0007). Blocking CMV reactivation with ganciclovir after CLP appeared to prevent this increased level of fibrosis, as fibrosis was significantly lower in GCV-treated mice than in nontreated mice (p .0002) Cook et al. Crit Care Med")
87
CMV et fibrose Souris Péritonite Evaluation à 3 semaines CMV –
Réactivation CMV Réactivation CMV + Gancyclovir Boxplot comparison of pulmonary fibrosis in latently infected (CMV), noninfected (CMV), and ganciclovir-treated (CMVGCV) mice 3 wks after cecal ligation and puncture. White belts indicate the median value. Boxes give the range between quartiles (25th and 75th percentiles). Notched black regions are 95% confidence intervals for the medians, and the dots indicate the full range of the distributions. Because distributions of pulmonary fibrosis scores are nonnormal, nonparametric tests were used to discern differences among study groups at day 21. Post hoc comparisons of pairs of groups were made using the Mann-Whitney-Wilcoxon test (nonparametric t-test). CMV reactivation was related to significant increases in pulmonary fibrosis compared with healthy controls after CLP (p ). Blocking CMV reactivation with ganciclovir after CLP appeared to prevent this increased level of fibrosis, as fibrosis was significantly lower in GCV-treated mice than in nontreated mice (p .0002) Cook et al. Crit Care Med 2006
, noninfected (CMV), and ganciclovir-treated (CMVGCV) mice 3 wks after cecal ligation and puncture. White belts indicate the median value. Boxes give the range between quartiles (25th and 75th percentiles). Notched black regions are 95% confidence intervals for the medians, and the dots indicate the full range of the distributions. Because distributions of pulmonary fibrosis scores are nonnormal, nonparametric tests were used to discern differences among study groups at day 21. Post hoc comparisons of pairs of groups were made using the Mann-Whitney-Wilcoxon test (nonparametric t-test). CMV reactivation was related to significant increases in pulmonary fibrosis compared with healthy controls after CLP (p .0007). Blocking CMV reactivation with ganciclovir after CLP appeared to prevent this increased level of fibrosis, as fibrosis was significantly lower in GCV-treated mice than in nontreated mice (p .0002) Cook et al. Crit Care Med")
88
CMV et fibrose Souris Péritonite Evaluation à 3 semaines CMV –
Réactivation CMV Réactivation CMV + Gancyclovir Boxplot comparison of pulmonary fibrosis in latently infected (CMV), noninfected (CMV), and ganciclovir-treated (CMVGCV) mice 3 wks after cecal ligation and puncture. White belts indicate the median value. Boxes give the range between quartiles (25th and 75th percentiles). Notched black regions are 95% confidence intervals for the medians, and the dots indicate the full range of the distributions. Because distributions of pulmonary fibrosis scores are nonnormal, nonparametric tests were used to discern differences among study groups at day 21. Post hoc comparisons of pairs of groups were made using the Mann-Whitney-Wilcoxon test (nonparametric t-test). CMV reactivation was related to significant increases in pulmonary fibrosis compared with healthy controls after CLP (p ). Blocking CMV reactivation with ganciclovir after CLP appeared to prevent this increased level of fibrosis, as fibrosis was significantly lower in GCV-treated mice than in nontreated mice (p .0002) Cook et al. Crit Care Med 2006
, noninfected (CMV), and ganciclovir-treated (CMVGCV) mice 3 wks after cecal ligation and puncture. White belts indicate the median value. Boxes give the range between quartiles (25th and 75th percentiles). Notched black regions are 95% confidence intervals for the medians, and the dots indicate the full range of the distributions. Because distributions of pulmonary fibrosis scores are nonnormal, nonparametric tests were used to discern differences among study groups at day 21. Post hoc comparisons of pairs of groups were made using the Mann-Whitney-Wilcoxon test (nonparametric t-test). CMV reactivation was related to significant increases in pulmonary fibrosis compared with healthy controls after CLP (p .0007). Blocking CMV reactivation with ganciclovir after CLP appeared to prevent this increased level of fibrosis, as fibrosis was significantly lower in GCV-treated mice than in nontreated mice (p .0002) Cook et al. Crit Care Med")
89
Other micro-organisms
BAL⊕ 4-fold increase in antibody titer stable increased antibody titer Acanthamoeba, Bosea Water-associated microorganisms Amebal pathogens VAP episodes, n=120 Berger et al. Emerg Infect Dis 2006

90
La Scola et al. Emerg Infect Dis 2005
Mimivirus La Scola et al. Emerg Infect Dis 2005 Transmission electron microscopy: non-enveloped icosahedral virions surrounded by fibrils Mimivirus pour Mimicking Microbes A l’intérieur d’amibes qui vivent dans l’eau Intra-cellulaire obligatoire

91
Co-infections N Série de 338 CAP chez des non-immunodéprimés
De Roux et al. Chest 2004

92
Apport de la biologie moléculaire
Legoff et al. J Clin Microbiol 2005 N Avec Fagon

93
VAP, adequacy of antibiotic therapy and mortality
%

94
Adequate early antibiotic therapy Disease severity
LOD 4 LOD > 4 Clec’h et al. Intensive Care Med 2004 ICU mortality % Inadequate empirical treatment seemed to be associated with a poor prognosis only in patients with Logistic Organ Dysfunction score < or = to 4.

95
Delay in the initiation of appropriate antibiotic treatment
VAP, n=107 P < .01 % Appropriate but delayed antibiotic therapy Iregui et al. Chest 2002

96
Resistant strains even in EOP
Giantsou et al. Intensive Care Med 2005 Micro-organisms responsible for 408 episodes of VAP, % EOP: More surgical patients, more patients who have received previous antibiotics, more corticosteroids Modification of the initial antibiotic therapy: 58% vs. 36%, p < .001

97
Diagnosis = BAL + blood + urine
but initial antibiotherapy = TA !

98
One or two TA per week

99
Conclusions Stratégie diagnostique Stratégie thérapeutique
Any difference ? Stratégie thérapeutique Quelques différences VAP précoce Pn Immuno VAP tardive ? Biologie moléculaire

Présentations similaires
















: données de la littérature Dr S. Alfandari Service de Réanimation et Maladies Infectieuses.>")





