Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
SDRA: quelle place pour l’AREC ?
2
Evolution mortalité Phua et al. AJRCCM 2009
A decrease in ARDS mortality was only seen in observational studiesfrom1984to Mortality did not decreasebetween 1994 (when a consensus definition was published) and 2006, and is lower in RCTs than observational studies.
 and 2006, and is. lower in RCTs than observational studies.")
3
Correction de l’hypoxémie Préservation du parenchyme pulmonaire

5
Etude européenne ALIVE
PaO2/FIO2 et mortalité Etude européenne ALIVE 78 ICU, 10 pays, 6522 admissions, 401 SDRA 63% 41% Brun-Buisson et al. ICM 2004

6
Effets délétères ventilation mécanique
Dreyfuss et Saumon AJRCCM 98 Figure 1. Normal Rat Lungs and Rat Lungs after Receiving High-Pressure Mechanical Ventilation at a Peak Airway Pressure of 45 cm of Water. After 5 minutes of ventilation, focal zones of atelectasis were evident, in particular at the left lung apex. After 20 minutes of ventilation, the lungs were markedly enlarged and congested; edema fluid filled the tracheal cannula. Adapted from Dreyfuss et al.8 with the permission of the publisher.

7
SDRA, VM et pronostic SDRA décès MOF VM

8
Décompartementalisation
LBA plasma T0 T1 T2 T0 T1 T2 Ranieri et al. JAMA 99 Baisse aussi dans le LBA de il1, il6 et tnf + il6 dans plasma dans groupe protectif Baisse aussi de l’IL6 dans NIH 36 h à peu près après rando Décompartementalisation

9
Optimisation du réglage du ventilateur

10
Ventilation protectrice: modèle idéal

11
SDRA = NIH ? NIH NEJM 2000

12
LOBAIRE: pas de recrutement
DIFFUS: recrutement

13
LOBAIRE: pas de recrutement
DIFFUS: recrutement

14
Recrutement, surdistension, mécanique ventilatoire et PEEP
Viera et coll. AJRCCM 99 Avec LIP Sans LIP aération aération

15
Vt, PEEP et recrutement PEEP recrutement dérecrutement
Gattinoni et al. AJRCCM 95 recrutement dérecrutement PEEP

16
Vt, PEEP et recrutement PEEP recrutement dérecrutement
Gattinoni et al. AJRCCM 95 recrutement dérecrutement PEEP

17
Mercat et al. JAMA 2008

18
ALVEOLI ARDSnet NEJM 2004

19
O’Meade et al. JAMA 2008

20
Recrutement = mortalité ?
Gattinoni et al. NEJM 2006

22
A ce stade Optimisation du réglage du respirateur Curariser DV NO
Défaillance VD Echec DV Réévaluer dose Eau et sel Raisonnable

23
BTTF

24
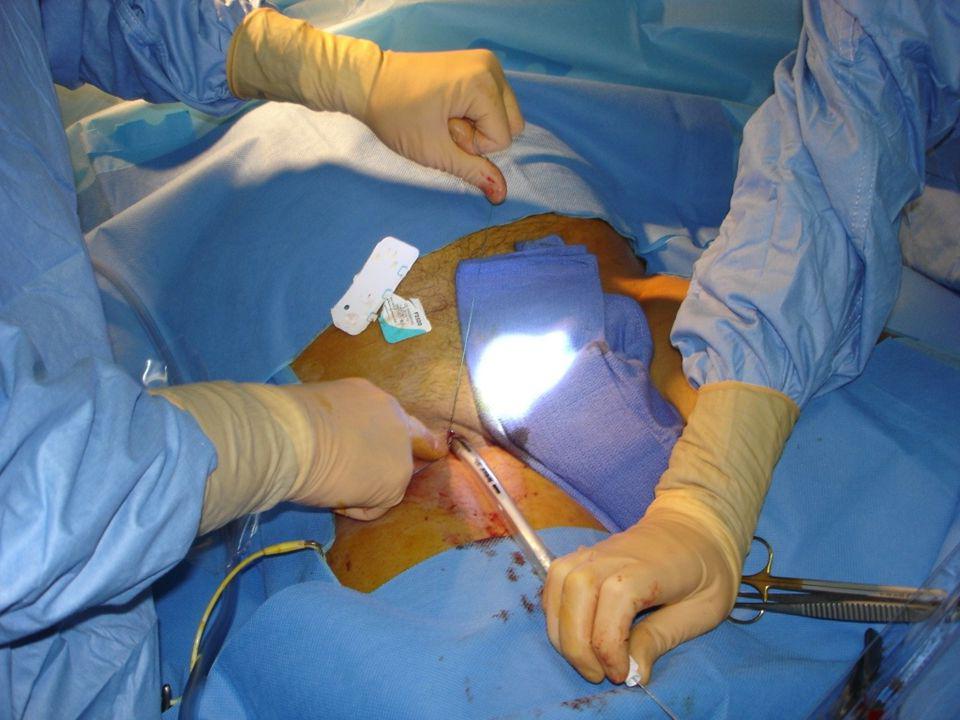
ECMO périphérique ECMO centrale

25
ECMO V V = Suppléance respiratoire Voies fémorales ou jugulaires
Pompe Arrivée Air et O2 Oxygénateur CO2 Voies fémorales ou jugulaires Canules veineuses

26
ECMO CO2 Canules : veineuse et artérielle
ECMO V A = Suppléance cardio respiratoire Pompe Arrivée Air et O2 Oxygénateur CO2 Voies fémorales ou jugulaires Canules : veineuse et artérielle Shunt de revascularisation du membre canulé

27
Collaboration multidisciplinaire
ECMO Collaboration multidisciplinaire Équipe chirurgie cardiaque disponible 24/24h C Chirurgien IBODE Perfusioniste

30
Adapter ECMO et Ventilateur
Débit: vitesse de pompe FIO2 (Oxygénation) Balayage (élimination CO2) Vt < 4 ml/kg FR cycles /min PEP cmH2O CO2 Vitesse Débit Console de l’ECMO Gazométries artérielle et veineuse (SvO2) Lactates Coloration circuit CEC
 Balayage (élimination CO2) Vt < 4 ml/kg. FR cycles /min. PEP cmH2O. CO2. Vitesse. Débit. Console de l’ECMO. Gazométries artérielle et veineuse (SvO2) Lactates. Coloration circuit CEC.")
31
ECMO Sevrage Diminution des paramètres de CEC
Débit, vitesse de pompe, FIO2, balayage Reprise ventilation mécanique FR, Vt , PEEP, FIO2 Retrait des canules

32
Assistance respiratoire extra-corporelle
Inclusion: Fast entry criteria= PaO2 < 50 > 2h avec FiO2 1.0 et PEEP > 5 Slow entry criteria= PaO2 < 50 > 12h avec FiO2>0.6 et PEEP > 5 ; maximal therapy > 48h Exclusion: durée de la VM > 7j CI aux anticoagulants, lésions cérébrales irréversibles, pathologie pulmonaire chronique sévère, immunosuppression, maladie terminale, défaillance multi viscérale Zapol et al. JAMA 79

33
En 1974… US NIH Zapol JAMA étude contrôlée multicentrique
90 patients randomisés entre VM conventionnelle +/- ECMO Mortalité 92 vs 90% mais: mortalité ds le groupe contrôle élevée (malades trop graves?) Plusieurs centres inexpérimentés Remplissage excessif, Vt élevé, anticoagulation+++ Veino-Artériel Durée de VM prolongée avant ECMO The first randomized trial20 comparing patients in nine medical centers treated with ECMO or conventional ventilation was published in The survival rate in both groups was 10%, and no significant difference in mortality was observed between patients receiving ECMO or conventional ventilation. ECMO proponents today point out that this study was performed in the early days of the field, using techniques that are not standard today. For instance, venoarterial (VA) access was used in this study,
 Plusieurs centres inexpérimentés. Remplissage excessif, Vt élevé, anticoagulation+++ Veino-Artériel. Durée de VM prolongée avant ECMO. The first randomized trial20 comparing patients. in nine medical centers treated with ECMO or. conventional ventilation was published in The. survival rate in both groups was 10%, and no. significant difference in mortality was observed between. patients receiving ECMO or conventional. ventilation. ECMO proponents today point out that. this study was performed in the early days of the. field, using techniques that are not standard today. For instance, venoarterial (VA) access was used in. this study,")
34
En 1994, Morris AJRCCM VM (pression contrôlée) Vs VM + ECMO (ECCO2-R)
ETUDE INTERROMPUE après analyse intermédiaire sur 40 patients Pas de différence significative sur la survie (42% vs 33%) Mais mode ventilatoire non uniforme ds le groupe ECMO, Pplat élevée Haut niveau de survie ds le groupe contrôle Faible débit de l’ECMO Beaucoup de complications hémorragiques (inexpérience ?) A second randomized trial21 of 40 patients in 1994 looked at extracorporeal carbon dioxide removal instead of true ECMO. It too showed no significant difference in survival rate between groups (with conventional ventilation, 42%; with ECMO, 33%; p 0.8), although the low blood flow associated with this method (1 to 2 L/min) is inadequate to provide meaningful blood oxygenation.
 Mais mode ventilatoire non uniforme ds le groupe ECMO, Pplat élevée. Haut niveau de survie ds le groupe contrôle. Faible débit de l’ECMO. Beaucoup de complications hémorragiques (inexpérience ) A second randomized. trial21 of 40 patients in 1994 looked at extracorporeal. carbon dioxide removal instead of true. ECMO. It too showed no significant difference in. survival rate between groups (with conventional. ventilation, 42%; with ECMO, 33%; p 0.8), although. the low blood flow associated with this. method (1 to 2 L/min) is inadequate to provide. meaningful blood oxygenation.")
35
Survie: modification // évolutions technologiques

36
Type de membrane Silicone: + résistantes
Fibres microporeuses (polypropylène): + performantes et mieux tolérées Fuite plasma Changements quotidiens Microfibres microporeuses en polymethylpentene Quadrox D MEDOS Novalung Dideco
: + performantes et mieux tolérées. Fuite plasma. Changements quotidiens. Microfibres microporeuses en polymethylpentene. Quadrox D. MEDOS. Novalung. Dideco.")
37
Progrès techniques Surfaces pré-héparinées Canules percutanées

38
Aspects pratiques TCA 1,5 Objectif: 40-50% du débit cardiaque
2 abords veineux afférents si Hyperdébit Hypoxémie très sévère

39
Complications Thrombopénie Hémolyse Activation C GB
Thrombopénie par aggrégation plaquettaire

40
Relation PAM, diamètre canule - débit
Müller et al. Eur Respir J 2009 19 Fr 17 Fr 15 Fr Blood flow through the iLA averaged 1.59¡0.52 L?min-1 with 15-Fr cannulae. With 17-Fr cannulae, blood flow was 1.94¡0.35 L?min-1 and with 19-Fr cannulae it was 2.22¡0.45 L?min-1 (p,0.001).
.")
41
N = 180

42
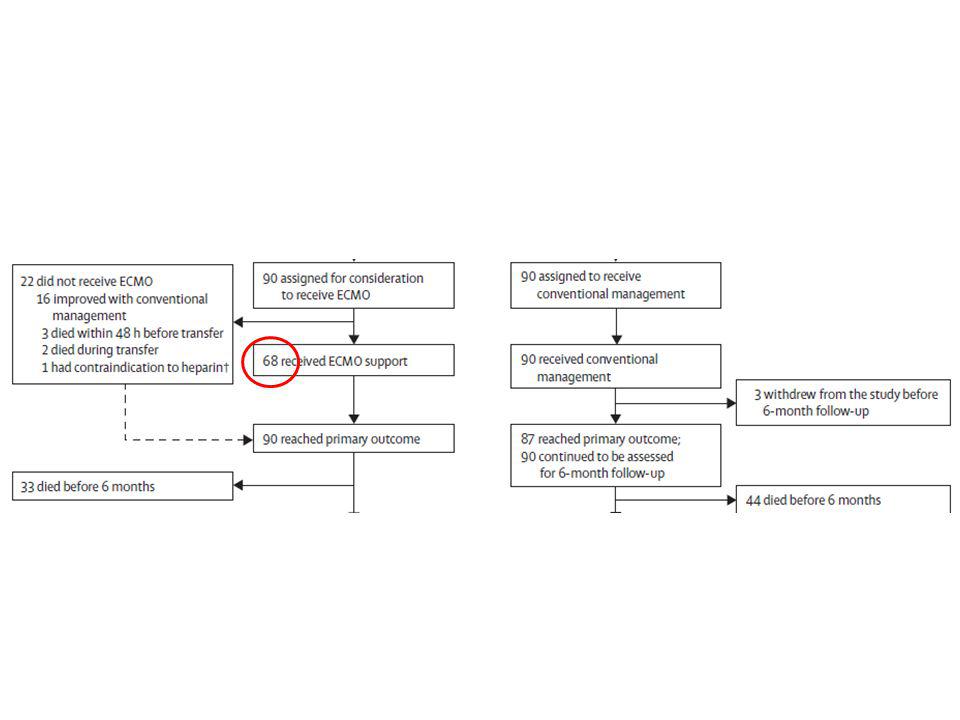
Critères d’inclusion

44
Résultat P = 0.03 68 of 90 patients who were
randomized to receive ECMO actually received this therapy, predominantly due to the improvement of a subset of patients prior to arriving at the ECMO center.

46
Pronostic Hemmila et al. Ann Surg 2004
Ann Arbor Equipe Hirschl et Bartlett Hemmila et al. Ann Surg 2004

47
Interventional Lung Assist
Novalung® sans pompe Canule artérielle Canule veineuse + large de 2 Fr Membrane en polymethylpentene TCA 1,5 PAM > 70 mmHg Efficacité PaCO2 +++ Efficacité PaO2 + O2 12 l/min

48
Müller et al. Eur Respir J 2009
Efficacité ELA Müller et al. Eur Respir J 2009 This rise in Pa,O2, according to the law of Dalton, is caused mainly by a reduction of alveolar PCO2 and a concomitant increase in alveolar PO2.

49
“Therefore, according to the current data, interventional lung assist should probably not be used in patients with the most severely impaired oxygenation or in patients with reduced cardiac output.” Müller et al. Eur Respir J 2009 “ In haemodynamically unstable patients requiring high doses of vasopressors (noradrenaline 0.4 μg/kg/minute or higher) or in patients with severe hypoxaemic ARDS, a pump-driven ECMO is still the rescue measure of choice.” Zimmermann et al. Crit Care 2009
 or in patients with severe hypoxaemic ARDS, a pump-driven ECMO is still the rescue measure of choice. Zimmermann et al. Crit Care")
50
“Optimisation” stratégie
36 patients (4,5 ans) : LIS > 2,5 et critères ECMO stratégie TDM diurétiques ou HF “ Qs pulmonaire” mode ventilatoire (Vt, PIM et Pmoy le plus bas possible avec recrutement alvéolaire correct) ± hypercapnie TGI shunt PEEP, i/e NO 15 ppm DV almitrine Guinard et al. Chest 97
 : LIS > 2,5 et critères ECMO. stratégie. TDM. diurétiques ou HF. Qs pulmonaire mode ventilatoire. (Vt, PIM et Pmoy le plus bas possible avec recrutement alvéolaire correct) ± hypercapnie. TGI. shunt. PEEP, i/e. NO 15 ppm. DV. almitrine. Guinard et al. Chest 97.")
51
ECCO2R “Optimisation” R : PaO2/FiO2 > 100 pendant au moins 6 h NR
PaCO2 non-maitrisable détérioration mécanique ventilatoire Guinard et al. Chest 97 ECCO2R

52
Transport sous ECMO Unité Mobile Transport internes : Bloc, scanner…
Transport interhospitalier: UMAC-AREC Unité Mobile Assistance Circulatoire et Assistance Respiratoire Extra Corporelle L

53
Le petit manuel du parfait ARDSologue
Limiter la iatrogénie Réduction volume courant Plusieurs profils de patients Approche globale Ajuster la PEEP en fonction de la présentation morphologique Limiter pression de plateau Curariser tôt mais brièvement Eviter dérecrutement Limiter les objectifs d’oxygénation Le reste…

54
Linden et al. Acta Anaesthesiol Scand 2009
Que sont-ils devenus ? 12-50 mois après ECMO Reprise activité: 76% TDM Opacités réticulées: 76% Opacités en verre dépoli: 24% Normal: 14% Etendue des anomalies: 10% du parenchyme Linden et al. Acta Anaesthesiol Scand 2009 Mean values of all lung spirometry tests were in the lower normal interval. Ten patients had normal spirometry. Signs of a mild obstructive disorder (FEV1o80%) was observed in nine of 21 patients (43%), in combination with a mild restrictive pattern (TLCo80%) in three patients. Long time on ECMO was associated with reduced TLC (Po0.05). The exercise tests also showed mean performance values in the lower normal interval with nine patients (43%) performingo80% of predicted. Sixteen patients interrupted the exercise due to leg fatigue and only five due to dyspnea. A slight drop in SpO2 after work was noted in seven patients. DLCO was reduced in 13 of 20 patients (65%).
 was observed in nine of 21 patients. (43%), in combination with a mild restrictive pattern. (TLCo80%) in three patients. Long time on. ECMO was associated with reduced TLC (Po0.05). The exercise tests also showed mean performance. values in the lower normal interval with. nine patients (43%) performingo80% of predicted. Sixteen patients interrupted the exercise due to leg. fatigue and only five due to dyspnea. A slight drop. in SpO2 after work was noted in seven patients. DLCO was reduced in 13 of 20 patients (65%).")
55
“Optimisation” Facteurs de mauvais pronostic à l’inclusion PaCO2
analyse univariée PaCO2 DVA avant arrivée Nb défaillances viscérales SAPS II réponse à l’optimisation analyse multivariée Guinard et al. Chest 97

56
“Optimisation” NR : Nb de défaillances viscérales p < 0,05
Guinard et al. Chest 97 NR : Nb de défaillances viscérales p < 0,05

57
ECMO périphérique ECMO centrale

58
Déterminants de l’efficacité sur l’oxygénation
The influence of a) blood flow, b) arterial oxygen saturation (Sa,O2) and c) haemoglobin content on oxygen transfer through the interventional lung assist device (iLA). The oxygen transfer capacity of the iLA depended on Sa,O2 (r ), the blood flow through the device (r50.43) and the haemoglobin content of blood (r50.23; each p,0.01; fig. 4a–c). The capacity of the iLA to remove carbon dioxide increased with higher Pa,CO2 (r50.34, p,0.01), higher sweep gas flow (r50.27, p,0.01) and higher blood flow through the device (r50.23, p,0.01; fig. 5a–c). No correlation was found to haemoglobin content of blood (data not shown).
 blood flow, b) arterial oxygen saturation (Sa,O2) and c) haemoglobin content on oxygen transfer through the interventional lung assist. device (iLA). The oxygen. transfer capacity of the iLA depended on Sa,O2 (r ), the. blood flow through the device (r50.43) and the haemoglobin. content of blood (r50.23; each p,0.01; fig. 4a–c). The capacity of the iLA to remove carbon dioxide increased. with higher Pa,CO2 (r50.34, p,0.01), higher sweep gas flow. (r50.27, p,0.01) and higher blood flow through the device. (r50.23, p,0.01; fig. 5a–c). No correlation was found to. haemoglobin content of blood (data not shown).")
59
Zimmermann et al. Br J Anaest 2006
Efficacité ILA Zimmermann et al. Br J Anaest 2006 (at fractional inspired concentration of oxygen = 1.0) before, after flight, on admission at the ICU (iLA-1) and 24 h (iLA-24) after starting iLA. *P<0.05.
 before, after flight, on admission at. the ICU (iLA-1) and 24 h (iLA-24) after starting iLA. *P<0.05.")
60
Patients à haut risque hémorragique
Huang et al. Resuscitation 2009

61
Interventions durant AREC
2 DC seulement

62
Modification paramètres de VM
Zimmermann et al. Crit Care 2009 51 patients from multiple aetiologies meeting ARDS-criteria prospective multicentre randomised trial (ClinicalTrials NCT ).
.")
Présentations similaires



>")

















