Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Est-ce que la désinfection des mains est un outil efficace pour prévenir les transmissions croisées ? Bertrand Souweine

2
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

3
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

4
Types of Skin Flora Transient flora Resident flora Infectious flora

5
Epiderme superficiel : stratum corneum
effet protecteur contre flore contaminante squammes lipides H20 assure plasticité, perméabilité // hydratation La main joue un rôle important dans la transmission croisée car elle est le principal outil du soignant au contact du patient et de son environnement. La peau qui recouvre la main est une barrière anatomique bâtie comme un mur dont les squames seraient les briques et les lipides le mortier. L ’hydratation de la peau assure sa perméabilité et sa plasticité. Les lipides limitent l ’évaporation et sont indispensables au respect des propriétés fonctionnelles de l ’épiderme. Tous les jours l ’organisme élabore une couche de stratum et en disperse une dans l ’environnement libérant ainsi 107 particules contenant 10% de germes. Une couche produite / 24 heures et qui disparaît en 15 jours ufc/cm2, enchâssés en profondeur 107 particules libérées / j dans air dont 10% contiennent des germes

6
Resident Flora Deeper skin layers
Mainly CNS, coryneform bacteria and micrococci ; fungi (Malassezia); virus usually not resident on the skin More resistant to mechanical removal and stable over time Lower pathogenic potential (not pathogens on intact skin) Colonization resistance Very difficult to eliminate (< 50% decrease in bacteril load after 6 min of handwashing)
; virus usually not resident on the skin. More resistant to mechanical removal and stable over time. Lower pathogenic potential (not pathogens on intact skin) Colonization resistance. Very difficult to eliminate (< 50% decrease in bacteril load after 6 min of handwashing)")
7
Transient Flora Superficial layers; usually not multiply on the skin
Acquired by contact with patient or environment Easily removed by mechanical means S. aureus, GNB or candida or virus

8
Infectious Flora The etiologic agents of actual infections such as abscess, panaritium, paronychia, and infected eczema on the hands S. aureus and β-hemolytic streptococci

9
You may not Realize You Have Germs on Your Hands!
Nurses, doctors and other healthcare workers can contaminate their hands by doing simple tasks, including: Taking a patient’s blood pressure or pulse Assisting patients with mobility Touching the patient’s gown or bed sheets Touching equipment, including bedside rails, over bed tables, IV pumps The photo shows a blood agar plate 24 hrs after an ICU nurse placed her hand on plate”

10
Acquisition de la flore transitoire ou contaminante
temps de soin dépendante Pittet Arch Intern Med 1999 Durée de contact : 16 cfu /mn Port de gants : 3 cfu /mn Dans ce travail qui consiste à évaluer la densité microbienne sur les mains des soignants après activité de soins on voit que la contamination augmente avec la durée du contact et que le port de gants réduit significativement la contamination des mains.

11
Acquisition de la flore transitoire ou contaminante
même après simple contact patient Pittet Arch Intern Med 1999 Cette contamination survient pour tous les types d ’activité au contact des patient y compris des contact direct simple Type d’activité : cfu /mn

12
Clin Microbiol Rev. 2004;17(4):863
:863")
13
Transmission of organisms
Transmission of organisms by hands of health care providers between two patients can result in health care associated infections (HAIs). Adapted from the Swiss Hand Hygiene Campaign
. Adapted from the Swiss Hand Hygiene Campaign.")
14
Clin Microbiol Rev. 2004;17(4):863
:863")
15
Hygiène des mains et contrôle de l’infection
CDC Guideline for HH in healthcare settings Hygiène des mains et contrôle de l’infection Recently Mrs Larson published in a review a table with the 6 publications of hospital based studies which demonstrates significant results between the effect of hand hygiene and risk of infection. They are much methodologic limitations to conduct such a study but despite those problems, they are many evidences for an obvious link between hand hygiene and reduced risk of transmission of nosocomial pathogen

16
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

17
CID 2000;31:136

19
Soap Plain Esterified fatty acids with sodium or potassium hydroxide Mechanical removal of dirt and loosely adherent flora (transient>resident) Antiseptic

20
Chlorhexidine A cationic biguanide
England in 1954; introduced into U.S. in 1970s Chlorhexidine base only minimally soluble in water, but digluconate is water-soluble Exists as acetate (diacetate), gluconate, and hydrochloride salts
, gluconate, and hydrochloride salts.")
21
Mechanism of Action Attach to bacterial cytoplasmic membrane (inner membrane) Precipitation or coagulation of protein and nucleic acids Also to the outer membrane in G(-) and the cell wall in G(+) Also damage the cytoplasmic membrane of yeasts
 and the cell wall in G(+) Also damage the cytoplasmic membrane of yeasts.")
22
Spectrum of Activity Depends on concentration Bacteria
lower: bacteriostatic against GP bacteria, GNB and bacterial spores Bacteria Good activity against G(+), less G(-) and fungi, not spores Dermatophytes: no activity Mycobacteria: limited Virus: good for most enveloped virus, low for naked viruses
, less G(-) and fungi, not spores. Dermatophytes: no activity. Mycobacteria: limited. Virus: good for most enveloped virus, low for naked viruses.")
23
Efficacy Reduce transient bacteria by 2.1 to 3 log10; smaller in resident flora (0.35 to 2.29 log10) Activity is greatly reduced in the presence of organic matter, natural corks, and hand creams containing anionic emulsifying agents Substantial residual activity

24
Resistance If MIC greater than 50 mg/liter Mechanism
Uncommon among G(+) bacteria Yes for G(-), such as E.coli, P.mirabilis (84.6%), P. stuartii, P. aeruginosa, P. cepacia and S. marcescens C. albicans (10.5%) Cross-resistance (+) Mechanism Alternation of inner, outer membrane or the cell wall
 bacteria. Yes for G(-), such as E.coli, P.mirabilis (84.6%), P. stuartii, P. aeruginosa, P. cepacia and S. marcescens. C. albicans (10.5%) Cross-resistance (+) Mechanism. Alternation of inner, outer membrane or the cell wall.")
25
Adverse Effect Temperature greater than 70℃, chlorhexidine may degrade to para-chloraniline (carcinogenic) Conjunctivitis and corneal damage when contacted with eye Ototoxicity Dermatitis is concentration dependent Anaphylactic reactions Avoid direct contact with brain tissue and the meninges

26
Another reason why personnel don’t wash their hands often
Frequent handwashing with soap and water often causes skin irritation and dryness. Skin irritation are more frequently reported when using antiseptic soap In the winter months, some personnel may even develop cracks in their skin that cause bleeding, as seen in the adjacent figure.

27
OBSERVANCE / HYGIENE DES MAINS
Nb d’actions d’hygiène des mains Nb d’indications à l’hygiène des mains

28
Observance basale Soignants 30-40% Médecins 10-20% Autres 10-20%

29
Observance du lavage des mains : revue de la littérature
%

30
Trick, CID 07

31
Reasons Advocated for Poor Handwashing Compliance
Risk factors for Poor Handwashing Compliance Skin irritation from hand hygiene products Inaccessibility of hand hygiene supplies Wearing gloves Hands don’t look dirty Lack of information on the importance of hand hygiene Lack of knowledge of the guidelines Too busy/handwashing takes too long Male vs female Physician vs nurse Wearing gloves Working in ICU Understaffing/overcrowding

32
It takes ICU nurses an average of 62 seconds to go to a sink, wash and dry their hands, and return to patient care activities

33
It takes ICU nurses an average of 62 seconds to go to a sink, wash and dry their hands, and return to patient care activities. In this study the authors measured the contact rates between health care workers and patients in a general ICU and estimated that if handwashing was undertaken for every patient contact, 3 to 4 hours during every 24 h of care would be needed for every patient in the ICU for this activity. If an alcohol-based handrub (ABH) is available at each patient’s bedside, it takes nurses about 15 seconds to clean their hands. It takes ICU nurses an average of 62 seconds to go to a sink, wash and dry their hands, and return to patient care activities The time needed for hand hygiene before and after every contact is about 100 min/patient for direct contacts
 is available at each patient’s bedside, it takes nurses about 15 seconds to clean their hands. It takes ICU nurses an average of 62 seconds to go to a sink, wash and dry their hands, and return to patient care activities. The time needed for hand hygiene before and after every contact is about 100 min/patient for direct contacts.")
34
DUREE DU LAVAGE SIMPLE DES MAINS
Anne Simon

35
Hand as a Vectors of Transmission
Organisms present on the patient’s skin or on inanimate objects Organism must be capable of surviving for at least several minutes on the hands of personnel Handwashing is inadequate or omitted entirely Come in direct contact with another patient, or with an inanimate object

36
Precaution Recontaminated from faucets or by splashes from traps or sinks (P. aeruginosa in the tap water) or from plain soap (both bar and liquid soaps, bar soaps heavier; S. marcescens or Serratia liquefaciens) Outside health care facilities (working hours, before eating, after using restroom), use of soap and water is recommended
 or from plain soap (both bar and liquid soaps, bar soaps heavier; S. marcescens or Serratia liquefaciens) Outside health care facilities (working hours, before eating, after using restroom), use of soap and water is recommended.")
37
Hand hygiene is the most important tool in NI control
Adherence to hand-washing practices remains unacceptable low, rarely exceeding 40%

38
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

39
CID 2000;31:136

40
Poor Kolletchka

41
Ignaz Philipp Semmelweis (1818-1865)
Ignaz Philipp Semmelweis ( ), a Hungarian obstetrician educated at the universities of Pest and Vienna, introduced antiseptic prophylaxis into medicine. In the 1840s, puerperal or childbirth fever, a bacterial infection of the female genital tract after childbirth, was taking the lives of up to 30% of women who gave birth in hospitals. Women who gave birth at home remained relatively unaffected. As assistant professor on the maternity ward of the Vienna General Hospital, Semmelweis observed that women examined by student doctors who had not washed their hands after leaving the autopsy room had very high death rates. When a colleague who had received a scalpel cut died of infection, Semmelweis concluded that puerperal fever was septic and contagious. He ordered students to wash their hands with chlorinated lime before examining patients; as a result, the maternal death rate was reduced from 12% to 1% in 2 years. Nevertheless, Semmelweis encountered strong opposition from hospital officials and left Vienna in 1850 for the University of Pest. As a professor of obstetrics at the University of Pest Hospital, he enforced antiseptic practices and reduced the death rate from puerperal fever to 0.85%. However, Semmelweis findings and publications were resisted by hospital and medical authorities in Hungary and abroad. After a breakdown, he entered a mental hospital in Vienna, where he died of an infection contracted during an operation he had performed. Ignaz Philipp Semmelweis ( )
, a Hungarian obstetrician educated at the universities of Pest and Vienna, introduced antiseptic prophylaxis into medicine. In the 1840s, puerperal or childbirth fever, a bacterial infection of the female genital tract after childbirth, was taking the lives of up to 30% of women who gave birth in hospitals. Women who gave birth at home remained relatively unaffected. As assistant professor on the maternity ward of the Vienna General Hospital, Semmelweis observed that women examined by student doctors who had not washed their hands after leaving the autopsy room had very high death rates. When a colleague who had received a scalpel cut died of infection, Semmelweis concluded that puerperal fever was septic and contagious. He ordered students to wash their hands with chlorinated lime before examining patients; as a result, the maternal death rate was reduced from 12% to 1% in 2 years. Nevertheless, Semmelweis encountered strong opposition from hospital officials and left Vienna in 1850 for the University of Pest. As a professor of obstetrics at the University of Pest Hospital, he enforced antiseptic practices and reduced the death rate from puerperal fever to 0.85%. However, Semmelweis findings and publications were resisted by hospital and medical authorities in Hungary and abroad. After a breakdown, he entered a mental hospital in Vienna, where he died of an infection contracted during an operation he had performed. Ignaz Philipp Semmelweis ( )")
42
hand disinfection with a solution of 4% chlorinated
Death of Kolletchka (Mean) maternal mortality at the First ([white circle]) and Second (•) Imperial Royal Obstetric Departments of the General Hospital in Vienna, A: before the introduction of autopsies; B: after the introduction of autopsies; C: after the establishment of a second department, medical and midwifery students trained jointly at both departments; D: medical students trained only at the first department, where deliveries were directed by doctors; midwifery students trained only at the second department, where deliveries were conducted mainly by midwives; E: introduction of hand disinfection with a solution of 4% chlorinated lime by Semmelweis in May 1847 at both departments; F: maternal mortality after the introduction of hand disinfection. Curr Opin Infect Dis 1998; 11:
 maternal mortality at the First ([white circle]) and Second (•) Imperial Royal Obstetric Departments of the General Hospital in Vienna, A: before the introduction of autopsies; B: after the introduction of autopsies; C: after the establishment of a second department, medical and midwifery students trained jointly at both departments; D: medical students trained only at the first department, where deliveries were directed by doctors; midwifery students trained only at the second department, where deliveries were conducted mainly by midwives; E: introduction of hand disinfection with a solution of 4% chlorinated lime by Semmelweis in May 1847 at both departments; F: maternal mortality after the introduction of hand disinfection. Curr Opin Infect Dis 1998; 11:")
43
Ethanol, Isopropanol, and n-Propanol
Ethanol is introduced in 1888 isopropanol and n-propanol in 1904 Vigorous friction, rinsing with water, and drying with a towel are unnecessary

44
Les produits hydro-alcooliques (PHA)
solutions ou gels séchage rapide désinfection des mains alcool (60-70%) + émollient +/- autre antiseptique péril hydrique friction sans rinçage friction sur mains sèches +++ non visiblement souillées (propres) non poudrées pas de friction de gants
 + émollient +/- autre antiseptique. péril hydrique. friction sans rinçage. friction sur mains. sèches +++ non visiblement souillées (propres) non poudrées. pas de friction de gants.")
45
Mechanism of Action Killing not mechanically remove
Protein denaturation, rapid killing (sec)
")
46
The cell viability of biofilms of S
The cell viability of biofilms of S. epidermidis was determined by staining the bacteria within biofilm with CTC and DAPI. The absence of red cells indicates the loss of respiratory activity by most cells in ethanol treated biofilm. At this point we see that on the basis of in vitro study results, concentrated ethanol is effective for treating experimental biofilm. However, extrapolating these results in clinical practice might be questionable since blood components such as fibrin, or other proteins may interfere with the ability of ethanol to kill biofilm in vivo.

47
Spectrum of Activity Mycobacteria
Excellent in vitro activity against G(+) and G(-) bacteria Virus Good activity against enveloped viruese Nonenveloped viruses require higher concentration (70-80%) Against most fungi Poor or no activity against spores, protozoal oocysts
 and G(-) bacteria. Virus. Good activity against enveloped viruese. Nonenveloped viruses require higher concentration (70-80%) Against most fungi. Poor or no activity against spores, protozoal oocysts.")
48
Etudes expérimentales de l’activité des savons sur les mains contaminées par C. difficile (Barbut F. et coll., Hygiènes, 2003, 5, ) Contamination expérimentale des mains de 14 volontaires Contamination initiale : 4.2 à 4.8 log10 UFC/ml Méthode du jus de gants log 1 min 30 sec P<0.01 P=0.36 P<0.01 Diapositive empruntée a F Barbut

49
Quelle hygiène des mains ?
Faut il bannir les solutions hydro alcooliques? Boyce et al, ICHE 2006 Même constat, -Diminution de l’incidence des ERV et des SARM ( ) vs ( ) -Incidence stable pour Clostridium difficile Gordin et al ICHE 2006
 vs ( ) -Incidence stable pour Clostridium difficile. Gordin et al ICHE")
50
Efficacy The type of alcohol Concentration Contact time Volume used
Whether the hands are wet when the alcohol applied Temperature Organic material

51
Efficacite de l’hygiène des mains sur la flore
Henri Mondor, 1996

52
Clin Microbiol Rev. 2004;17(4):863
:863")
53
Time-Course of Efficacy of Unmedicated Soap and Water and Alcohol-Based Handrub in Reducing the Release of Test Bacteria from Artificially Contaminated Hands Curr Opin Infect Dis Aug;16(4):327
:327.")
54
LIQUID SOAP PREVALUES POVIDONE-IODINE LIQUID SOAP 0.8% CHLORHEXIDINE-
Iog 10 LIQUID SOAP PREVALUES POVIDONE-IODINE LIQUID SOAP 0.8% CHLORHEXIDINE- DETERGENT 4% POVIDONE-IODINE AQU. SOLUTION 10% ISO-PROPANOL 60% HEXACHLOROPHENE- DETERGENT 3% ISO-PROPANOL 70% N-PROPANOL 60% ISO-PROPANOL 70%+ CHLORHEXIDINE 0.5% 60 min

55
Handwashing with plain soap Handwashing with antiseptic detergent
Alcohol-based handrub Before After Alcohol is an established disinfectant. Many in vitro studies have demonstrated that ABH is more effective than either plain soap or antibacterial soaps in reducing the bacterial counts on hands. On this slide you can see culture plates showing growth of germs 24 hours after a nurse placed her hand on the plate, having used three different techniques of hand hygiene. ABH reduced the bacterial counts on hands to a greater extent than washing with plain soaps or detergents containing povidone-iodine. One noticeable exception is clostridium difficile since the spores cannot be destroyed by standard ABH. When caring for a patient harbouring c difficile, handwashing is mandatory for mechanical removal of spores and should be followed by alcoholic hand disinfection after hands have been dried. d’après Pr Bientz, Institut d’hygiène de Strasbourg

56
The technique used for hand cleansing before patient care affected the amount of bacterial contamination Handwashing with plain soap Handwashing with antiseptic detergent On this slide we see that the bacterial contamination of ungloved hands during patient care increased linearly with time and depended on the method of hand cleansing performed before patient care. HCWs who washed their hands with only unmedicated soap and water had higher bacterial counts than those who used hand antisepsis Alcohol-based handrub (ABH)
")
57
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

58
Temps économisé par l’utilisation de la Friction Hydro-Alcoolique
Lavage simple des mains : quitter le lit du patient aller au lavabo, se mouiller les mains se laver les mains (= 30 secondes) se sécher les mains retourner au lit du patient Total 1 min 30 s Friction avec une SHA : au lit du malade durée de friction pour séchage Total 30 s
 se sécher les mains. retourner au lit du patient. Total 1 min 30 s. Friction avec une SHA : au lit du malade. durée de friction pour séchage. Total 30 s.")
59
PLUS RAPIDE Lavage des mains sol. alcoolique
40 à 80 secondes pour effectuer le lavage des mains contre seulement 20 secondes pour une désinfection avec la solution hydro-alcoolique Pour une équipe de 12 personnes en réanimation au cours d ’une journée de 8h de travail : Lavage des mains sol. alcoolique Temps requis 16h 4h Force de travail 17% < 5% Voss A & Widmer AF ICHE 1997;18:205-8

61
Widmer CID 2007

62
Widmer CID 2007

63
Mayo Clin Proc. 2004;79(1):109
:109")
66
15 Jan 2007. Michelle Manhart nude photos are now online
15 Jan Michelle Manhart nude photos are now online. Air Force staff sergeant Michelle Manhart was relieved of her duties for posing nude in Playboy US Air Force sergeant Michelle Manhart gets nude for Playboy february 2007

67
Aviat Space Environ Med. 2007 number of duty days lost
2004 2005 2006 N=56 N=210 ; 2.4% N=78 ; 0.9% N=61 number of duty days lost

68
Effet des SHA sur l’observance
Service de réanimation médicale, 6 mois Observance à l’hygiène des mains Au début: l’observance ne dépasse pas 22%. Cela a permis d’augmenter l’observance d’environ 20% Bischoff et al., Arch Intern Med, 2000

69
Effet des SHA sur l’observance
Évolution selon la catégorie de personnel soignant Maury et al.AJRCCM, 2000

70
There is a negative relationship between hand hygiene compliance and the number of hand hygiene opportunities per hour of patient care when handwashing is used, which is not found when ABH is used.

71
In this study the author reported the effect on adherence to hand hygiene of a multifaceted programme. ABH was available all over the study. Observed hand hygiene practice was measured at baseline in grey and after intervention in blue. On the x axis are shown 8 indications to hand hygiene. As we can see baseline values of hndhygiene complinace with ABH differed widely according to the indications for hand hygiene. The multifaceted programm was asociated with a significant improvement in the adherence to hand hygiene from 40 to 80%, But the effect differed with the opportunities observed.

73
What about ABH for preventing cross transmission?
Despite the paucity of appropriate RCTs there is substantial evidence that hand antisepis reduces the incidence of health care associated infections. Numerous recent studies reported that when dealing with outbreaks related to VRE or other multiresistant organisms, the re-inforcement of ABH use in combination with establishment or re-inforcement of other barrier precautions halted the outbreak. Despite the limitations of these studies, most reports showed a temporal relation between improvement in hand hygiene practices and reduced infection rates.

74
Handwashing is in grey boxes and ABH in black boxes
Handwashing is in grey boxes and ABH in black boxes. The increase in hand hygiene compliance when ABH is available is not related to an increase in handwashing but to the addition of hand hygiene actions undertaken with ABH

75
Several Limitations in Hand Hygiene Compliance Studies
Before / after study Single centre No period randomization Overt observations Differences in the type of opportunities recorded Hawthorne effect Handwashing still performed during the ABH period Multifaceted programme on hand hygiene practice However, several points must be taken into account when assessing the results of these studies. Most of these studies are before / after studies, performed in one centre without period randomization. The observations are overt, the opportunities recorded differ, and the novelty effect cannot be fully excluded since the study periods and follow-up are often short. During the intervention period with ABH introduction, handwashing is still performed, and, in most cases, ABH is introduced in combination with a multifaceted programme for improving hand hygiene practice. Taken together these factors make it difficult to measure the specific impact of ABH on hand hygiene compliance.

76
Effect of Alcohol Handrub on Skin Condition
RCT: HW vs HR 29 nurses Self-reported skin score Epidermal water content Dry Healthy * * Healthy Dry Several studies showed that ABH is associated with a better skin tolerance than handwashing. This was found in self-report questionnaire surveys and in studies where skin condition was assessed by external observers and biometric tests. It has been suggested that among alcohol-based handrubs, gels might be associated with better skin care properties and dermal tolerance. Alcohol-based handrub is less damaging to the skin * , P<0.001 Boyce, Infection Control and Hospital Epidemiology 2000;21:

77
The better skin tolerance observed with ABH compared to handwashing probably contributes to the better acceptability of ABH. As you can seen in this prospective randomized clinical trial, healthcare workers assigned to ABH reported they preferred ABH to handwashing with chlorhexidine. They reported that ABH was easier and faster than handwashing. However, no differences between the two techniques were reported with gloving. Larson EL CCM 2001

78
It has been suggested that among alcohol-based handrubs, gels might be associated with better skin care properties and dermal tolerance. In this study performed in an MICU, self-reported and observed skin tolerance was better in the period when the ABH used was a gel.

79
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

80
Impact de l’utilisation des SHA sur les taux d’IN
Pittet et al., Lancet 2000

81
Impact de l’utilisation des SHA sur l’incidence des SARM
Pittet et coll., Lancet 2000

82
In this prospective observational study carried out by Lucet and coll in Paris over a-6 year period in ICUs with high colonization pressure, we can see a relationship between intoduction of ABH and control of MRSA acquisition ABH introduction

83
Education programme Education programme
Here the results of a prospective controlled cross-over trial performed in two adult ICUs assessing the impact of ABH introduction on the rates of nosocomial infections. Concerning compliance, At baseline nurses exhibited greater hand hygiene compliance than physicians. After the educational programme, in unit A, where ABH was not available, nurses had a higher rate of hand hygiene compliance than physicians. In both units there was a significant increase in hand hygiene compliance during periods when ABH was available. During the periods with ABH, most of hand hygiene actions were performed with ABH. There was a close correlation between hand hygiene compliance and the patient care activities. baseline baseline ABH ABH Education programme Education programme

84
Infection due to MRSA: from 1.67 to 2.77 per 1.000 patient-days
Concerning nosocomial infection, Baseline rates were very low and there was no correlation between hand hygiene compliance and the nosocomial infection rates. The rates of nosocomial infections due to resistant organisms: VRE, MRSA and P aeruginosa were low during the study without significant change over time. Infection due to MRSA: from 1.67 to 2.77 per patient-days Infections due to VRE from 0.35 to 1.36 per patient-days

85
Cannot detect a change is not absence of change
Absence of training programme Very low baseline rates of nosocomial infection Absence of surveillance cultures to detect MRSA/VRE colonization No data on the rates of MRSA/VRE importation Doest it mean that improving compliance with ABH is not efficious for decreasing NI rates? Many reasons may have contributed to this negative results Concerns exist on the bactericidal effect of the hand hygiene gel used. There are ongoing debate on about the efficacy of ABH gel with a an ethnol concentration lower than 80% We don’t know if training in the application of ABH gel was performed The very low baseline rate of NI may have jeopardized the possibilidy of detecting the clinical effect of introducing the gel. Rough calculation were performed and have suggested that even if improvements in hand hygiene compliance were able to decrease NI rates of 50%, this study would have only 20% of chance of demonstrating the effect The acquisition of nosocomial infection represents an accurate surrogate but did not actually reflect cross transmission. Surveillance cultures were not performed and therefore data on ICU acquired colonization are lacking. Such information is needed to estimate the risk for acquiring MRSA since the rates of MRSA/VRE importation are a major determinant of MRSA/VRE transmission.

86
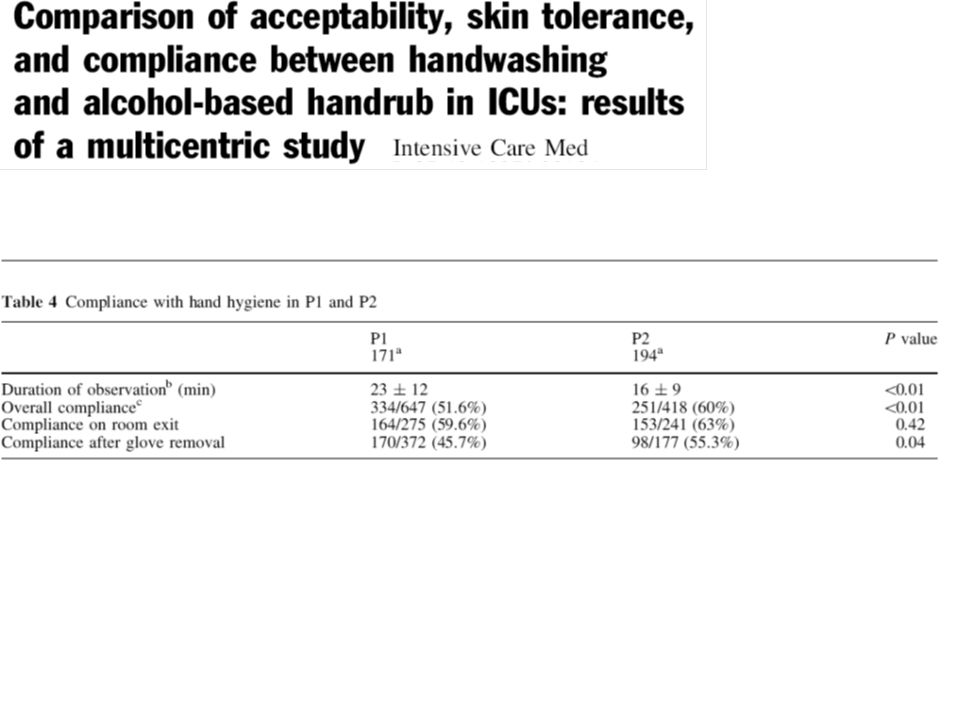
Baseline 59.5% 26% 21% 22.5% Overall compliance Before patient contact After patient contact Correctly performed Intervention 65% 45% 56% 42.6% P 0.46 <0.01 <0.001

88
6 urban sites Here the results of a large australian study aiming at measuring the effect of a multisite multifaceted programme to improve hand hygiene practice in 22 institutions. ABH was available all over the study. The study duration was 2 years. The authors measured hand hygiene complinace, ABH consumption, and the rates of MRSA bcteremia and of MRSA isolated from clinical samples. There was no screening for MRSA colonization.

89
a total of 65 fewer patients developping MRSA bacteremia during the 24-month intervention period
The number of patients with MRSA bacteremia fell significantly from a mean baseline rate of 0.05/per 100 patients discharge per month 24 months before the intervention to 0.02 in the last 3 month of the intervention. This represented a total of 65 fewer patients developping MRSA bacteremia during the 24-month intervention period Similarly was observed a significant decrease in the rates of clinical sample positive to MRSA representing 716 fewer clinical MRSA isolates identified during the 24-month intervention period. Similar findings were observed in the australian statewide roll-out including 75 hospitals with an increase in hand hygiene compliance from 20% to 55% and a reduction in the rates of MRSA isolates and bacteremia.

92
Acceptability of hand hygiene procedures in the 7 units

95
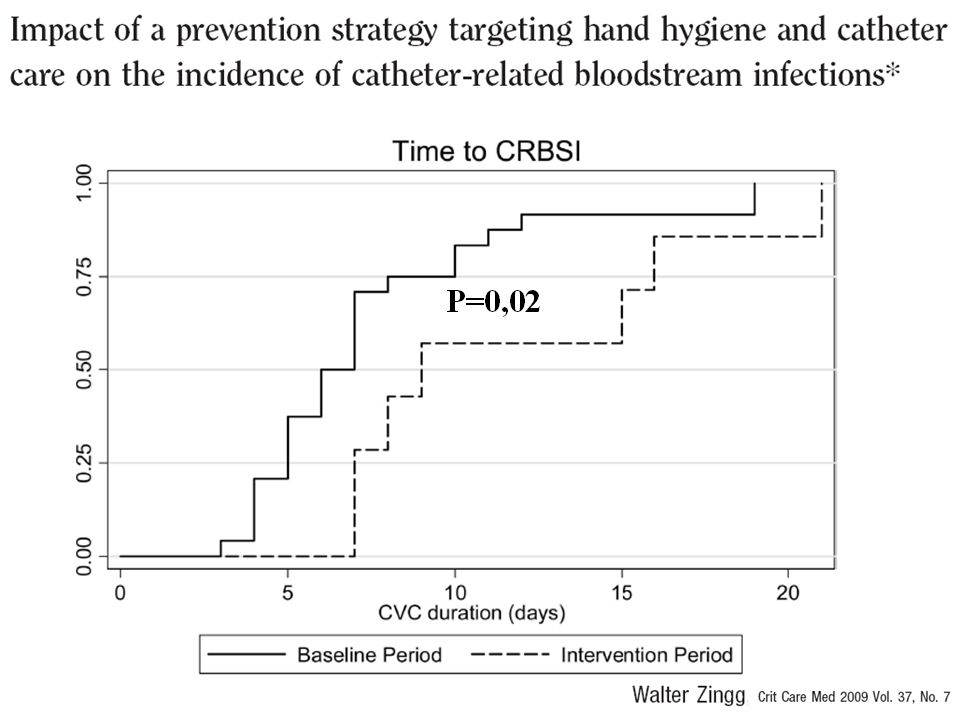
P=0.06

97
Cannot detect a change is not absence of change

98
Plan Flore cutanée et contamination Lavage des mains
Frictions alcoolique Efficacité microbiologique Aspects pratiques Efficacité clinique Conclusion

99
ABH is effective in decreasing NI rates
The causal role of microorganisms on hands in the pathogenesis of NI is extremely well established Traditional soap-and-water hand hygiene is less effective than hand antisepsis Handwashing as frequent as recommended is often impractical and leads to inflammatory skin reactions

100
ABH is effective in decreasing NI rates
ABH is the simplest and least expensive way of achieving good hand hygiene practice and so of preventing health care associated infections and the spread of antimicrobial resistance Multifaceted campaign with education programme, meetings, introduction of ABH, training in application of ABH, reminders, monitoring of compliance, monitoring of NI rate, and surveillance feedback are required to promote hand hygiene and reduce cross transmission in ICUs

101
Avantages de la friction alcoolique
Plus efficace que le lavage avec un savon. Action rapide et réalisation rapide. Ne nécessite pas de lavabo. Actif sur les pathogènes nosocomiaux. Toujours à portée de la main. Moins irritant pour la peau. Moins polluant pour l ’environnement. Favorise l ’observance. Boyce JM.Infect Control Hosp Epidemiol 2000;21: Daschner Fr. Am J Infect Control 2000;28: 386

102
Quand utiliser les SHA? avant tout contact avec un malade, que des gants aient été portés ou non après tout contact avec un malade, que des gants aient été portés ou non entre les soins pour un même malade, que des gants aient été portés ou non après l’ablation des gants

103
Attention L'alcool ne contient pas d'agent nettoyant
Si mains souillées, lavage des mains impératif Si C difficile la FHA est précédée d’un lavage avec séchage

104
MODE D’EMPLOI Délivrer une dose (3ml) dans le creux de la main
Friction des mains jusqu’à évaporation (30 sec.) Paume / paume et paume/dos mains Espaces interdigitaux, ongles, pouce…
 Paume / paume et paume/dos mains. Espaces interdigitaux, ongles, pouce…")
106
Hand Hygiene Clean Care is Safer Care

Présentations similaires











![[number 1-100] There is no rule to the way to remember the names for the numbers 1 to 10 in French so we recommend that you simply practice!](/1/172873/big_thumb.jpg "[number 1-100] There is no rule to the way to remember the names for the numbers 1 to 10 in French so we recommend that you simply practice!>")


 et.>")

 / Information about the study trip to Strasbourg (29th-31st March 2009) Château de.>")










