Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
SEPSIS - MENINGITIS - MALARIA
Pr. B. Vandercam Consultation Maladies Infectieuses et Tropicales Cliniques Universitaires St-Luc Octobre 2004

2
Sepsis Focus Absence of focus Purpura fulminans
Community acquired sepsis immunocompentent adult Nosocomial sepsis immunocompetent adult IV DU Asplenic (anatomic or functional) Neutropenia Toxic shock syndrome
 Neutropenia. Toxic shock syndrome.")
3
Working definitions associated with sepsis and related disorders

4
Source of infection Anamnesis (pets, travel, household, …)
Physical examination (purpura, scar …) Blood culture Urine culture RX thorax Echo (scan abdo) obstacle abscess collection Echo cardio
 Blood culture. Urine culture. RX thorax. Echo (scan abdo) obstacle abscess collection. Echo cardio.")
5
Activated protein C (- 6 %)
Corticosteroids (low (HC mg/day) - long (5-7d)) Intensive insuline therapy (- 17%) Volume resuscitation (- 15%)
 - long (5-7d)) Intensive insuline therapy (- 17%) Volume resuscitation (- 15%)")
6
Prior medicare database analyses
MEEHAN T. Jama 1997; 278:2080 Mortality increased significantly with delay in first Abx dose > 8 hrs (registration to dose) GLEASON PP. Arch Intern Med 1999, 159:2562 Mortality based on abx (OR) Cephalosporin Cephalosporin + mac Fluoroquinolone
 GLEASON PP. Arch Intern Med 1999, 159:2562 Mortality based on abx (OR) Cephalosporin 1.0. Cephalosporin + mac Fluoroquinolone")
7
Method : review of Medicare database for patients > 65 yrs hospitalized with x-ray confirmed CAP
Period reviewed : July ’98 - March ’99 Patients : PSI score : III - 47 % IV - 24 %

8
Results

9
Skin lesions and systemic infections

10
Purpura fulminans : treatment
Cefotaxime 2 gr q h or Ceftriaxone 2 gr q 12 h Allergy Vanco 1 gr q 12 h Aztreonam 2 gr q 6 h or Moxifloxacin 0,4 gr q 24 h or Levofloxacin 0,5 gr q 12 h

11
Community acquired sepsis - immunocompetent adults
Infecting organisms Enterobacteriacae Staph aureus Strept pneumoniae & spp N. meningitidis Bacteroides spp Treatment Cefotaxime or Ceftriaxone Amoxi clav or cefurox + amino

12
IVDU Infecting organisms Exclude endocarditis Previous antibiotherapy
Staph aureus Exclude endocarditis Previous antibiotherapy Treatment Oxacilline 2 gr q 6 h or Vancomycine 1 gr q 12h Genta 2,5 mg/kg q 12 h

13
Asplenia Overwhelming sepsis Stand by therapy Antibioprophylaxis
Amoxi clav Allergy, travel --> Moxifloxacin, Levofloxacin Vaccination Antibioprophylaxis

14
Asplenia sepsis Infecting organisms Treatment S. pneumoniae
H. influenzae N. meningitidis Capnocytophaga spp Treatment Ceftriaxone or Cefotaxime

15
Nosocomial *sepsis - immunocompetent adult
Infecting organisms Enterobacteriacae S. aureus Strep pneumoniae Bacteroïdes spp P. aeruginosa CNS * readmission - nursing home

16
Nosocomial sepsis Local epidemiology Colonization
Previous antibiotherapy IV line Urinary catheter Invasive procedure

17
Treatment Vancomycin ? Cefotaxime or Ceftriaxone or Pip/tazo + amino
Ceftazidime or Cefepime or Carbapenem amino

18
Sepsis neutropenia Infecting organisms Colonization
Strepto spp CNS S. aureus Enterobacteriacae P. aeruginosa Colonization Previous antibiotherapy

19
Neutropenia « Low risk »
Amoxi clav 2 gr q 6-8 h Cipro 750 q 12 h OR Ceftriaxone 2 gr q 12 h Amikacin mg/kg q 24 h

20
Neutropenia « High risk »
Ceftazidime 2 gr q 8 h Cefepime gr q 8 h Pip/tazo gr q 6 h Imipenem mg q 6 h Meropenem 2 gr q 8 h amino ???

21
Toxic shock syndrome Infecting organisms Treatment Strepto A, B, C,
Staph aureus Treatment Cefazoline 2 gr q 8 h + Clindamycine 600 mg q 8 h

22
Clinical diagnosis Fever sensitivity 85% Menigism 70%
Altered mental status 60% Kernig Sensitivity 5% Specificity 95% Poser la question = y répondre

23
Case presentation 25-year-old man
2-day history of severe headache, fever, neck stiffness 38,3 °C No rash Normal mental status and neurologic examination Pain on neck flexion but able to flex his neck fully No Kernig and Brudzinski signs

24
Contraindications of lumbar puncture
Known or suspected space-occupying lesions with mass effect LP deferred until CT scan Severe uncorrected coagulopathy (INR > 1.5) Trombocytopenia (platelet count < /mm³) Infection at the puncture site (decubitus ulcer) - Glasgow < 13 - Shock
 Trombocytopenia (platelet count < /mm³) Infection at the puncture site (decubitus ulcer) - Glasgow < Shock.")
25
When should a computerized tomography scan precede a lumbar puncture ?
Age over 60 years Immunocompromised state History of primary neurologic disease, head trauma, neurosurgery History of seizure within the past week Altered mental status, cilated or poorly reactive pupils, occular palsy and focal neurologic abnormalities Papilledema, bradycardia, irregular respiration History of cancer Suspicion of brain abscess (endocarditis, bacteremia …) Empiric anti infective therapy without delay
 Empiric anti infective therapy without delay.")
26
CSF examination Gram stain - Ziehl - Ink
Culture (bacteria, fungi, brucella, nocardia …) Bacterial antigens if antibiotherapy Gram or culture negative PCR virus + BK Blood culture 60 % + in acute bacterial meningitis
 Bacterial antigens. if antibiotherapy. Gram or culture negative. PCR virus + BK. Blood culture 60 % + in acute bacterial meningitis.")
27
CSF characteristics in selected neurologic conditions

28
Purpura, petechia N. meningitidis
Cellulitis face S. aureus H. influ VRS, VRI S. pneumoniae Parotitis Mumps Endocarditis S. aureus Septic arthritis S. pneumoniae S. aureus Pregnancy Listeria

29
Acute meningitis treatment
IV line - blood cultures AB + dexa 10 mg within 30 min(*) LP if no contraindication Chest x-ray Delta scan if needed (*) S. pneumoniae : 4 h N. meningitidis : 2 h LCR
 LP if no contraindication. Chest x-ray. Delta scan if needed. (*) S. pneumoniae : 4 h. N. meningitidis : 2 h LCR.")
30
Antibiotherapy Listeria : ampi or CTX
S. pneumoniae : peni i 10% cef 3 i 1% H. influ : vaccination

31
Antibiotherapy dosage
Penetration - bactericide - CMI Cefotax gr -(4 gr) q 4h (ratio 25%) Ceftriaxone 2 gr q 12h (ratio %) Ampi gr q 4h (ratio %) Cefepime (ratio 10%) Ceftazidime (ratio %) Cotrimoxazole (ratio %)
 q 4h (ratio 25%) Ceftriaxone 2 gr q 12h (ratio %) Ampi 2 gr q 4h (ratio %) Cefepime (ratio 10%) Ceftazidime (ratio %) Cotrimoxazole (ratio %)")
32
Antibiotic therapy in meningitis
IV from the beginning to the end … Standard therapy 7 days for N. meningitidis days for S. pneumoniae (14) - 21 days for L. monocytogenes
 - 21 days for L. monocytogenes.")
33
Meningitis : child > 3 months - adults < 50 yrs
Infecting organisms S. pneumoniae N. meningitidis H. influ L. monocytogenes Treatment Cefotaxime + ampicilline Ceftriaxone + ampicilline

34
Meningitis : alcoohol - adults < 50 yrs Cellular immune deficiency - Debilitating illness
Infecting organisms S. pneumoniae L. monocytogenes N. meningitidis Gram negative bacilli Treatment Cefotaxime + ampicilline Ceftriaxone + ampicilline

35
Meningitis : HIV /AIDS Infecting organisms C. neoformans S. pneumoniae
M. tuberculosis L. monocytogenes T. pallidum N. meningitidis HIV

36
Meningitis : cerebrospinal fluid shunt
Infecting organisms Coag neg staph S. aureus Diphteroids Enterobacteriaceae Treatment Vancomycin + cefta

37
Meningitis : after cranial or spinal trauma
Infecting organisms S. pneumoniae H. influ Treatment Cefotaxime or Ceftriaxone

38
Meningitis after cranial or spinal trauma (> 4 days)
Infecting organisms Enterobacteriaceae S. aureus P. aeruginosa S. pneumoniae Treatment Vancomycin + ceftazidime

39
People on the move: demographics year 2003
175 million persons live outside of their country of origin (2,9%) of the world's population Population of concern to UNHCR: 21,6 million Refugees 11,7 million Internally displaced persons: million Rural to urban migration: million/year 1-2 million migrate permanently every year 700 million tourist arrivals/year
 of the world s population. Population of concern to UNHCR: 21,6 million. Refugees 11,7 million. Internally displaced persons: million. Rural to urban migration: million/year. 1-2 million migrate permanently every year. 700 million tourist arrivals/year.")
45
Malaria risk pyramid for 1 month of travel without chemoprophylaxis
Oceania 1:5 Africa 1:50 South Asia 1:250 Southeast Asia 1:2500 South America 1:5000 Mexico and Central America 1:10 000 01643

49
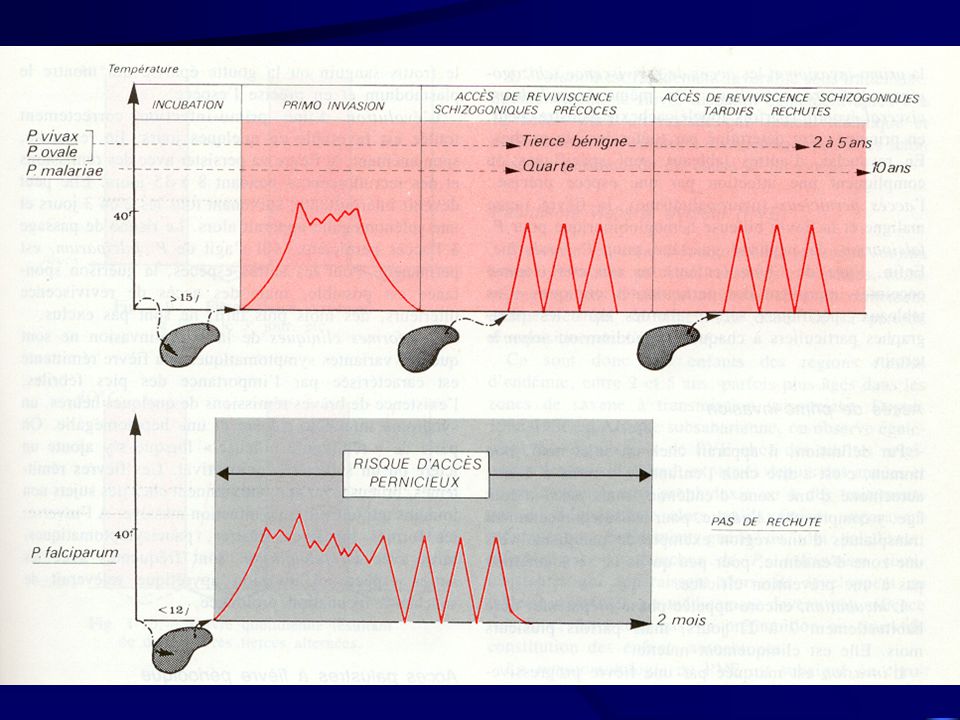
Délai d’apparition de malaria selon espèce
Schwartz NEJM 2003; 349, 1510

50
Malaria en Belgique Institut de Santé Publique-Louis Pasteur

51
Who dies from travelers’ malaria ?
USA & Canada (n = 21) Total (%) No chemo Dealy seeking care Missed by MD Lab misdiagnosis Mistreatment MMWR July 20, 2001 & 1999; 48:SS Kain K et al. CMAJ 2001, 164:
 Total (%) No chemo Dealy seeking care 1 5. Missed by MD Lab misdiagnosis Mistreatment MMWR July 20, 2001 & 1999; 48:SS-1 Kain K et al. CMAJ 2001, 164:")
53
Toute fièvre au retour des tropiques est une malaria jusqu’à preuve du contraire !!

54
Contribution de certaines anomalies biologiques au diagnostic de la malaria
Thrombopénie : 60-85% Si de plus GB N : VPP : 77% VPN : 92% Leucopénie ou GB N : quasi-constante CRP: 100% (mais très peu spécifique) Précoce Très élevé // à parasitémie et à évolution VPN très bonne (probable) si CRP N LDH : (très) sensible : % peu spécifique : 60% haptoglobine : 90% des cas VPN élevée de taux N Intérêt potentiel couplé à CRP
 Précoce. Très élevé // à parasitémie et à évolution. VPN très bonne (probable) si CRP N. LDH : (très) sensible : % peu spécifique : 60% haptoglobine : 90% des cas. VPN élevée de taux N. Intérêt potentiel couplé à CRP.")
59
Malaria à P. falciparum Règles: Vu la provenance essentiellement africaine des souches isolées en Belgique Hospitaliser si: patient non immun patient immun avec > 2% GR et/ou critères de gravité Préférer un traitement à base de quinine (5j ± 2j) si malaria sévère (+ doxycycline)
 si malaria sévère (+ doxycycline)")
60
La parasitémie peut augmenter durant les premières 24h de traitement
(action sur points limités du cycle qui continue à évoluer "malgré" le traitement) Résistance R3 est déterminée à 48h (où diminution de 75% doit être obtenue) La température peut persister pendant 72-96h sans signification péjorative Si haute suspicion de malaria, et GE (-) : répéter x sur 48h
 Résistance R3 est déterminée à 48h (où diminution de 75% doit être obtenue) La température peut persister pendant 72-96h sans signification péjorative. Si haute suspicion de malaria, et GE (-) : répéter x sur 48h.")
61
Traitement de la malaria à P. falciparum sévère
Bihydrochlorate de quinine 500 mg IV (dans 250ml glucosé ED) en 4h/ 3x/j pdt 3-7j 10 mg/kg (soit 8mg/kg de quinine base) 3x/j chez enfant N.B.: si origine S. Est Asiatique (ou si malaria sévère ?) dose charge : 20 mg/kg (donc 1 seule fois) ou (dès que possible/début si pas V /peu critères gravité) Sulfate de quinine: 500 mg per os 3x/j pdt 3-7 jours
 en 4h/ 3x/j pdt 3-7j. 10 mg/kg (soit 8mg/kg de quinine base) 3x/j chez enfant. N.B.: si origine S. Est Asiatique (ou si malaria sévère ) dose charge : 20 mg/kg (donc 1 seule fois) ou (dès que possible/début si pas V /peu critères gravité) Sulfate de quinine: 500 mg per os 3x/j pdt 3-7 jours.")
62
Doxycycline 200 mg/j puis 100 mg/j pdt 6 j ou
+ Doxycycline 200 mg/j puis 100 mg/j pdt 6 j ou Clindamycine 600 mg 3-4x/jour pdt 3-7 j (par exemple, si grossesse)
")
63
P. falciparum (zone A) - P. vivax, P. ovale (*)
Malaria treatment P. falciparum (zone A) - P. vivax, P. ovale (*) Day 1 : nivaquine 600 mg mg Day 2 : 300 mg Day 3 : 300 mg (*) Primaquine 15 mg q 24 h x 14 days
 - P. vivax, P. ovale (*) Day 1 : nivaquine 600 mg mg. Day 2 : 300 mg. Day 3 : 300 mg. (*) Primaquine 15 mg q 24 h x 14 days.")
64
Malaria treatment P. falciparum
Malarone P.O 4 x 3 days (food, milky drink) Quinine sulfate 500 mg q 8 h x 3-7 days Doxy 100 mg q 12h x 7 days Quinine I.V mg/kg over 4 h in 5% dextrose Quinine I.V. 10 mg/kg over 4 h q 8 h + Doxy 100 mg q 12h or Clinda 10 mg/kg q 8h Qt ! Halofantrine ! Mefloquine 2 weeks
 Quinine sulfate 500 mg q 8 h x 3-7 days. + Doxy 100 mg q 12h x 7 days. Quinine I.V mg/kg over 4 h in 5% dextrose. Quinine I.V. 10 mg/kg over 4 h q 8 h. + Doxy 100 mg q 12h or Clinda 10 mg/kg q 8h. Qt ! Halofantrine ! Mefloquine 2 weeks.")
Présentations similaires





















 Accra - Ghana, 10 – 12 Mars 2009 Trends in remuneration and motivation.>")



