Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
avant 2000 1000 hypertensive patients 940 essential hypertension
60 secondary hypertension 50 renal hypertension 5 reno-vascular hypertension 5 endocrine hypertension 2 pheochromocytomas 2 primary hyperaldosteronism 1 other endocrine cause

2
Pourquoi s’intéresser aux causes endocriniennes d’hypertension ?
Les mécanismes étiopathogéniques d’ hypertension endocrinienne sont aussi impliqués dans l’hypertension essentielle activation de l’axe rénine-angiotensine-aldostérone hyperactivité du système adréno-sympathique L’hypertension endocrinienne est sous-diagnostiquée ! hyperaldostéronisme primaire fréquent bcp de phéochromocytomes restent longtemps occultes incidentalome et syndrome de Cushing infraclinique

3
Adrenal incidentaloma
multicentric italian study ( Mantero et al, JCEM, 2000 ) : incidentalomas + hormonal work-up - malignant and symptomatic tumors excluded non-secreting tumor % subclinical Cushing’s syndrome (SCS) 9,2 % “silent” pheochromocytoma 4,2 % primary hyperaldosteronism 1,6 % 15 % HTA
 : incidentalomas + hormonal work-up. - malignant and symptomatic tumors excluded. non-secreting tumor 85 % subclinical Cushing’s syndrome (SCS) 9,2 % silent pheochromocytoma 4,2 % primary hyperaldosteronism 1,6 % 15 % HTA.")
4
après 2000 1000 hypertensive patients < 900 essential hypertension
> 100 secondary hypertension 50 renal hypertension 5 reno-vascular hypertension 60 endocrine hypertension 3 pheochromocytomas 50 primary hyperaldosteronism 7 other endocrine causes

5
I. Hyperaldostéronisme primaire

6
L’ hyperaldostéronisme primaire “classique” de 1965 à 2000 :
le syndrome de Conn HTA souvent sévère, résistante à un traitement classique comportant au moins 2 anti-hypertenseurs hypokaliémie spontanée (ou facilement inductible par diurétiques ou régime riche en sel) + kaliurie > 30 mEq/24 h hyperaldostéronisme non suppressible par une surcharge sodée ou l’administration d’un minéralocorticoïde suppression de l’axe rénine-angiotensine (ARP ou R )
 + kaliurie > 30 mEq/24 h. hyperaldostéronisme non suppressible par une surcharge sodée ou l’administration d’un minéralocorticoïde. suppression de l’axe rénine-angiotensine (ARP ou R )")
7
Hyperaldostéronisme : primaire ou secondaire ?
Hyperaldostéronisme secondaire (++) activité rénine plasmatique (ARP) < 1 ng/ml/heure rapport aldo (ng/dl) / ARP > 30 (50) Nle ou > 2 ng/ml/heure < 20 test de surcharge saline aldo > 0,25 nmol/L ou 10 ng/dl (2 litres de physio / 4 heures) aldo < 0,25 nmol/l ou 10 ng/dl test au captopril pas de modification du taux d’aldostérone (50 mg per os) aldostérone
 activité rénine plasmatique (ARP) < 1 ng/ml/heure. rapport aldo (ng/dl) / ARP. > 30 (50) Nle ou > 2 ng/ml/heure. < 20. test de surcharge saline. aldo > 0,25 nmol/L ou 10 ng/dl. (2 litres de physio / 4 heures) aldo < 0,25 nmol/l ou 10 ng/dl. test au captopril. pas de modification du taux d’aldostérone. (50 mg per os) aldostérone.")
8
L’hyperaldostéronisme primaire (AP) revisité depuis l’an 2000 :
une prévalence accrue… plusieurs publications récentes montrent une prévalence de 5 à 20% d’AP dans une population de patients hypertendus (dépistage par le rapport aldostérone / rénine plasmatique) Lim et al, Lancet, 1999, 353: 40 Loh et al, JCEM, 2000, 85: 2854 Fardella et al, JCEM, 2000, 85: 1863… l’hypokaliémie n’est présente que dans moins de 50% des cas ! dépistage justifié si HTA (sévère) avec normokaliémie imagerie surrénalienne souvent négative !
 Lim et al, Lancet, 1999, 353: 40. Loh et al, JCEM, 2000, 85: Fardella et al, JCEM, 2000, 85: 1863… l’hypokaliémie n’est présente que dans moins de 50% des cas ! dépistage justifié si HTA (sévère) avec normokaliémie. imagerie surrénalienne souvent négative !")
9
Diagnostic de l’hyperaldostéronisme primaire
dépistage : rapport aldostérone (ng/dl) (N : ) activité rénine plasmatique (ng/ml/h) (N: 0,2 – 5) Si > aldo > 10 ng/dl (0,30 nmol/l) : forte suspicion Si > aldo > 15 ng/dl (0,40 nmol/l) : diagnostique Ce rapport varie peu avec la position, le moment du prélèvement, l’ingestion de sel, … Et les médicaments anti-hypertenseurs ??
 (N : ) activité rénine plasmatique (ng/ml/h) (N: 0,2 – 5) Si > 30 + aldo > 10 ng/dl (0,30 nmol/l) : forte suspicion. Si > 50 + aldo > 15 ng/dl (0,40 nmol/l) : diagnostique. Ce rapport varie peu avec la position, le moment du prélèvement, l’ingestion de sel, … Et les médicaments anti-hypertenseurs")
10
C. Seifarth et al.Clin. Endocrinol.,2002, 57 : 457
aldostérone C. Seifarth et al.Clin. Endocrinol.,2002, 57 : 457

11
C. Seifarth et al.Clin. Endocrinol.,2002, 57 : 457
rénine C. Seifarth et al.Clin. Endocrinol.,2002, 57 : 457

12
Rapport aldostérone/rénine
C. Seifarth et al.,Clin. Endocrinol.,2002, 57 : 457

13
Diagnostic de l’hyperaldostéronisme primaire
rapport aldostérone (ng/dl) activité rénine plasmatique (ng/ml/h) Valide si : - éventuelle hypokaliémie corrigée - apport en NaCl normal - diurétiques, -bloquants, AINS arrêtés depuis 4 semaines Faux + (rapport ) Faux – (rapport ) -bloquants, clonidine diurétiques, spironolactone, IEC et Sartans AINS hypokaliémie Insuffisance rénale HTA réno-vasculaire ou maligne Patients âgés grossesse déplétion en NaCl
 activité rénine plasmatique (ng/ml/h) Valide si : - éventuelle hypokaliémie corrigée. - apport en NaCl normal. - diurétiques, -bloquants, AINS arrêtés depuis 4 semaines. Faux + (rapport ) Faux – (rapport ) -bloquants, clonidine diurétiques, spironolactone, IEC et Sartans. AINS hypokaliémie. Insuffisance rénale HTA réno-vasculaire ou maligne. Patients âgés grossesse. déplétion en NaCl.")
14
Diagnostic de l’hyperaldostéronisme primaire
confirmation : rapport aldo / ARP très élevé > hyperaldostéronisme > 15 ng/dl tests de surcharge saline régime riche en NaCl – 3 jours (+ apports en KCl) (Mayo clinic) aldostéronurie J 3 > 14 µg/24h avec Na urinaire > 200 mEq/24h sérum physiologique 2 litres / 4 heures iv aldostérone plasmatique > 10 ng/dl ou 0,25 nmol/l tests de suppression captopril (50 mg per os) fludrocortisone (0,1 mg/6h – 4 jours) aldo > 6 ng/dl ou 0,15 nmol/l
 (Mayo clinic) aldostéronurie J 3 > 14 µg/24h avec Na urinaire > 200 mEq/24h. sérum physiologique 2 litres / 4 heures iv. aldostérone plasmatique > 10 ng/dl ou 0,25 nmol/l. tests de suppression. captopril (50 mg per os) fludrocortisone (0,1 mg/6h – 4 jours) aldo > 6 ng/dl ou 0,15 nmol/l.")
15
Causes d’hyperaldostéronisme primaire
“APA” adénome surrénalien unilatéral 35% () R/ chirurgical “BAH” hyperplasie (nodulaire) bilatérale 64% () R/ médical Formes familiales % type I – “GRA” – hyperaldostéronisme suppressible par les glucocorticoïdes – diagnostic génétique (UCL) R/ glucocorticoïdes type II – gène non encore identifié
 R/ chirurgical. BAH hyperplasie (nodulaire) bilatérale 64% () R/ médical. Formes familiales 1% type I – GRA – hyperaldostéronisme suppressible par les glucocorticoïdes – diagnostic génétique (UCL) R/ glucocorticoïdes. type II – gène non encore identifié.")
16
Adénome ou hyperplasie ?

17
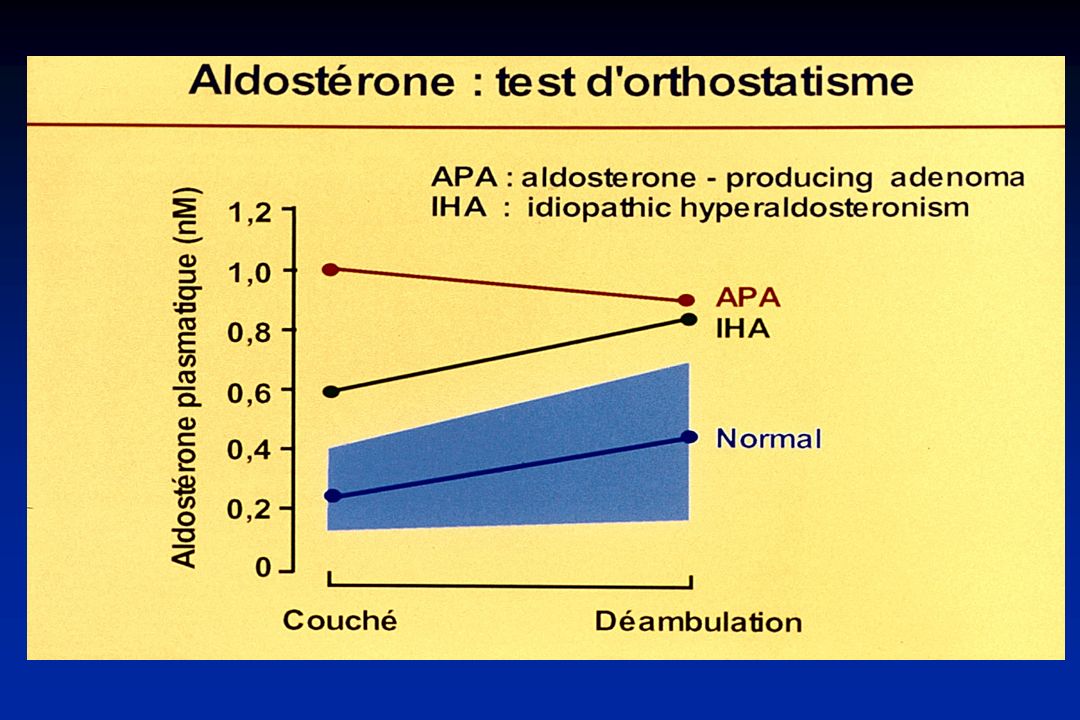
hyperaldostéronisme primaire : APA ou BAH ?
1. Test de posture Sensibilité 80% Spécificité > 95% Aldostérone ou Aldostérone de > 33% 2. Imagerie (CT – IRM) Sensibilité 70% Spécificité 66% Adénome unilatéral (1 – 2 cm) Hyperplasie bilatérale ou surrénales normales 3. Cathétérisme des veines surrénaliennes Sensibilité 90% Spécificité % Gradient de latéralisation Gradient faible ou absent
 Sensibilité 70% Spécificité 66% Adénome unilatéral. (1 – 2 cm) Hyperplasie bilatérale. ou surrénales normales. 3. Cathétérisme des veines surrénaliennes. Sensibilité 90% Spécificité 95-99% Gradient de latéralisation. Gradient faible ou absent.")
19
hyperaldostéronisme primaire : APA ou BAH ?
Test de posture Sensibilité 80% Spécificité 95% Aldostérone ou Aldostérone de > 33% Imagerie (CT – IRM) Sensibilité 70% Spécificité 66% Adénome unilatéral (si > 1 cm) Hyperplasie bilatérale ou surrénales normales Cathétérisme des veines surrénaliennes Sensibilité 90% Spécificité % Gradient de latéralisation Gradient faible ou absent
 Sensibilité 70% Spécificité 66% Adénome unilatéral. (si > 1 cm) Hyperplasie bilatérale. ou surrénales normales. Cathétérisme des veines surrénaliennes. Sensibilité 90% Spécificité 95-99% Gradient de latéralisation. Gradient faible ou absent.")
20
Mr G.DM. : CT Scan abdominal
surrénale gauche Adénome surrénalien droit 9 x 1,3 cm

21
Hyperaldostéronisme primaire
IRM abdominale montrant une hyperplasie surrénalienne bilatérale

22
hyperaldostéronisme primaire : APA ou BAH ?
Test de posture Sensibilité 80% Spécificité 95% Aldostérone ou Aldostérone de > 33% Imagerie (CT – IRM) Sensibilité 70% Spécificité 66% Adénome unilatéral (1 – 2 cm) Hyperplasie bilatérale ou surrénales normales Cathétérisme des veines surrénaliennes Sensibilité 90% Spécificité % Gradient de latéralisation Gradient faible ou absent
 Sensibilité 70% Spécificité 66% Adénome unilatéral. (1 – 2 cm) Hyperplasie bilatérale. ou surrénales normales. Cathétérisme des veines surrénaliennes. Sensibilité 90% Spécificité 95-99% Gradient de latéralisation. Gradient faible ou absent.")
23
Cathétérisme des veines surrénaliennes
Cortisol (nM) Aldo ( nM) Aldo/Cortisol V.C I. partie supérieure 349 1.86 0.5 V.C.I. hauteur A. rénales 403 2.21 V.C. I. partie inférieure 402 2.02 V. rénale G proximale 437 2.44 V. rénale G distale 431 2.24 V. surrénalienne G 15 095 5.5 0.03 V. surrénalienne Dr 1735 33 1.9 V. rénale polaire Dr 446 1.43 0.3 V. rénale Dr 424 2.27
 Aldo ( nM) Aldo/Cortisol. V.C I. partie supérieure V.C.I. hauteur A. rénales V.C. I. partie inférieure V. rénale G proximale V. rénale G distale V. surrénalienne G V. surrénalienne Dr V. rénale polaire Dr V. rénale Dr")
24
Monsieur G. DM. : cathétérisme des veines surrénaliennes (rapports cortisol /aldo)
Gradient ipsilatéral 1.9 / 0.5 = 3.8 (> 2) Gradient controlatéral 0.03 / 0.5 = 0.06 (< 1) 1.9 0.5 V.C.I. suprarénale v. surr. droite 0.03 0.3 v. rénale polaire D v. surr. gauche 0.5 0.5 0.5 0.5 v. rénale D v. rénale G 0.5 V.C.I. infrarénale Gradient de latéralisation 1.9 / 0.03 = 63 ( > 4)
 Gradient controlatéral 0.03 / 0.5 = 0.06 (< 1) V.C.I. suprarénale. v. surr. droite v. rénale polaire D. v. surr. gauche v. rénale D. v. rénale G V.C.I. infrarénale. Gradient de latéralisation. 1.9 / 0.03 = 63 ( > 4)")
25
+ APA BHA Hyperaldostéronisme primaire ? chirurgie R/ médical
Si jeune âge, antéc. familiaux + : exclure GRA Test de posture + Imagerie (CT / IRM) ? Dans tous les autres cas aldostérone debout + adénome unilatéral chez patient < 40 ans Cathétérisme des veines surrénaliennes Pas de gradient G-ipsi > 2 G-contro < 1 G-latér > 5 APA BHA chirurgie R/ médical
 Dans tous les autres cas. aldostérone debout. + adénome unilatéral. chez patient < 40 ans. Cathétérisme des veines surrénaliennes. Pas de gradient. G-ipsi > 2. G-contro < 1. G-latér > 5. APA. BHA. chirurgie. R/ médical.")
26
M. Stowasser et R.D. Gordon.
Primary aldosteronism Best Practice & Research Clin Endocrinology and Metabolism 2003;

27
II. Phéochromocytome

28
Main effects of catecholamines on the cardio-vascular system
Dopamine a 1- receptors (vascular bed) + Sympathetic nervous system Norepinephrine potent vasoconstriction (300 pg/ml) Adrenal medulla Epinephrine tachycardia inotropic effect (30 pg/ml) b 1- receptors (heart) Dopamine vasodilation b 2 - receptors (vascular bed) DA-receptors (vascular bed) vasodilation
 + Sympathetic nervous. system. Norepinephrine. potent. vasoconstriction. (300 pg/ml) Adrenal. medulla. Epinephrine. tachycardia. inotropic effect. (30 pg/ml) b 1- receptors. (heart) Dopamine. vasodilation. b 2 - receptors. (vascular bed) DA-receptors. (vascular bed) vasodilation.")
29
Pheochromocytoma a rare tumor ...
considered as a rare cause of hypertension ( %) only 1 pheochromocytoma discovered in 100 investigations for paroxystic HTA
 only 1 pheochromocytoma discovered in 100 investigations for paroxystic HTA.")
30
Pheochromocytoma … but underdiagnosed !
4-8% of incidentally-discovered adrenal masses 50% of the cases are normotensive between spells 75% of pheos discovered at autopsy remain undiagnosed before death (Mayo Clinic Series)
")
31
Pheochromocytoma : the rule of 10%
10% of pheochromocytomas ... are incidentally discovered are extra-adrenal (« paragangliomas ») are multiple / bilateral are or will become malignant occur in children are familial (probably more …) will recur
 are multiple / bilateral. are or will become malignant. occur in children. are familial (probably more …) will recur.")
32
Pheochromocytoma : clinical symptoms
paroxysmal (50%) or persistent (50%) hypertension - often severe and refractory to treatment - headaches 70% - abdominal pain 25% - perspirations 65% - chest pain 20% - palpitations 65% - weakness 20% - pallor 45% - dyspnea 20% - nausea 35% - weight loss 15% - tremor 30% - visual disturbances 15% - anxiety 30% - polyuria, polydipsia 10% spells of any of the following symptoms : « pheo’s triad »
 or persistent (50%) hypertension - often severe and refractory to treatment. - headaches 70% - abdominal pain 25% - perspirations 65% - chest pain 20% - palpitations 65% - weakness 20% - pallor 45% - dyspnea 20% - nausea 35% - weight loss 15% - tremor 30% - visual disturbances 15% - anxiety 30% - polyuria, polydipsia 10% spells of any of the following symptoms : « pheo’s triad »")
33
Pheochromocytoma : clinical symptoms
spontaneous spells or spells provoked by exercise, twisting, turning, straining, micturition, coitus, surgical procedure, delivery, abortion, …. frequency of spells : 1 every 2-3 months 25 every day ! duration of spells : usually 1 to 30 minutes

34
who should be screened for?
Pheochromocytoma : who should be screened for? paroxysmal or markedly fluctuating hypertension “spells” of any symptoms + hypertension pheo’s triad [headaches + sweating + palpitations] refractoriness to conventional anti-hypertensive treatment (orthostatic) hypotension alternating with hypertension paradoxical hypertensive response to beta-blockers adrenal incidentaloma personal history of a predisposing disease (von-Hippel-Lindau, MEN2, neurofibromatosis, …) familial history of pheochromocytoma, MEN2 syndrome, ...
 hypotension alternating with hypertension. paradoxical hypertensive response to beta-blockers. adrenal incidentaloma. personal history of a predisposing disease. (von-Hippel-Lindau, MEN2, neurofibromatosis, …) familial history of pheochromocytoma, MEN2 syndrome, ...")
35
Pheochromocytoma : how to screen ?
Biochemical test reference value sensitivity specificity urinary NMN + MN > 1.2 mg/24h 90-95% 98% urinary NE + E > 200 µg/24 h 80-85% 98% urinary VMA > 11 mg/24h 30-35% % urinary NE + E > 200 µg/24h or urinary NMN + MN > 1.2 mg/24h plasma NE + E > 1000 pg/ml 88-90% 90% > 2000 pg/ml low 100% 98% 98% In most cases, urinary mets + cats are diagnostic No test has 100% sensitivity + 100% specificity !

36
value of fractionated plasma metanephrines
Pheochromocytoma : value of fractionated plasma metanephrines Sensitivity = 99% specificity = 85% pheo controls pheo controls May be useful if high suspicion A. Sawka et al., JCEM, 2003

37
Pheochromocytoma : the clonidine suppression test
Pheochromocytoma (n=10) Non-pheochromocytoma (n=15) 20000 10000 8000 6000 4000 2000 Plasma norepinephrine (pg/ml) 1000 800 600 400 200 100 Basal Post-clonidine
 Non-pheochromocytoma (n=15) Plasma norepinephrine (pg/ml) Basal. Post-clonidine.")
38
Pheochromocytoma : how to localize ?
Sensitivity Specificity CT-Scan 97% 70% MRI 99% 80% 131I-MIBG 80% 100% 111In-octreoscan 70% 95% PET-Scan ? ? (FDG, fluorodopamine)
")
39
magnetic resonance imaging
Pheochromocytoma : magnetic resonance imaging T1-weighed image T2-weighed image

40
Pheochromocytoma : 131-I MIBG Scanning
Posterior Lateral R R Ant

41
Familial pheochromocytoma
multiple endocrine neoplasia type II (MEN IIa, MEN IIb) von Hippel-Lindau disease (VHL type 2) von Recklinghausen’s neurofibromatosis hereditary paraganglioma familial isolated pheochromocytoma
 von Hippel-Lindau disease (VHL type 2) von Recklinghausen’s neurofibromatosis. hereditary paraganglioma. familial isolated pheochromocytoma.")
42
Clinical suspicion of pheochromocytoma high low - - - - -
2-fold increase U-cats U-mets > 1.2 mg/24 h positive clonidine test ( plasma mets) - 24h-urinary mets+cats - clonidine test - (plasma mets) 24h-urinary mets+cats + + - - Other causes of spells? recheck after a spell do a provocative test ? + Abdominal MRI / CT 131I-MIBG + - - negative Pheochro- mocytoma + Other causes of spells? Whole body MRI octreo-scan PET-scan - Other causes of hypercate- cholaminemia Preparation + surgery
 - 24h-urinary mets+cats. - clonidine test. - (plasma mets) 24h-urinary mets+cats Other causes of spells recheck after a spell. do a provocative test + Abdominal MRI / CT. 131I-MIBG negative. Pheochro- mocytoma. + Other causes of spells Whole body MRI. octreo-scan. PET-scan. - Other causes of hypercate- cholaminemia. Preparation. + surgery.")
43
Maiter D. Pheochromocytoma: a paradigm for catecholamine-mediated hypertension Acta Clin Belg, 2004, 59:

Présentations similaires
>")

 and associated factors in HIV-infected patients,>")
















