Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Insuffisance Rénale Chronique
Médicaments et Insuffisance Rénale Chronique Prof. M. Jadoul Cliniques Universitaires St. Luc Université Catholique de Louvain 1200 Bruxelles

2
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? 5. I.R.C.: médicaments à prescrire? 6. Quelques précautions

3
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? 5. I.R.C.: médicaments à prescrire? Quelques précautions

4
1. Insuffisance rénale chronique (IRC) ?
anamnèse (nycturie, prurit, …) taille des reins (AUS, écho) Biologies, examens d ’urines antérieurs (préop, autres labos, …) Aiguë ou subaiguë si débit urinaire = 0 Cl. créat. = 0 même si créat. = 2.5 mg / dl si doute : contrôle biologique précoce (+ examen d ’urines !)
 taille des reins (AUS, écho) Biologies, examens d ’urines antérieurs (préop, autres labos, …) Aiguë ou subaiguë. si débit urinaire = 0. Cl. créat. = 0 même si créat. = 2.5 mg / dl. si doute : contrôle biologique précoce. (+ examen d ’urines !)")
5
2. Sévérité de l ’IRC ? Clearance ? • U x V P
• Formule de Cockroft - Gault 140 - âge (années) x Poids (kg) 72 x créat. plasm. (mg / dl) Ex : créatinine plasm. : 2 mg/dl femme : 80 ans - 60 kg - clearance : 21 ml/min - homme : 25 ans - 90 kg - clearance : 72 ml/min (récolte de 24 h …) Poids sec ! (sans oedèmes) x 0.85 (F)
 x Poids (kg) 72 x créat. plasm. (mg / dl) Ex : créatinine plasm. : 2 mg/dl. femme : 80 ans - 60 kg - clearance : 21 ml/min - homme : 25 ans - 90 kg - clearance : 72 ml/min. (récolte de 24 h …) Poids sec ! (sans. oedèmes) x 0.85 (F)")
6
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? 5. I.R.C.: médicaments à prescrire? Quelques précautions

8
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? I.R.C.: médicaments à prescrire? Quelques précautions

9
Spironolactone : risque d ’hyperkaliémie !
Number of admissions year p value to hospital (Mantel Haenszel x2) Hyperkalaemia Taking spironolactone for card. reason for cirrhosis No spironolactone Hypercalcaemia All admissions Georges B, Beguin C, Jadoul M. Lancet 2000 ; 355 :
 Hyperkalaemia. Taking spironolactone. for card. reason for cirrhosis No spironolactone Hypercalcaemia All admissions Georges B, Beguin C, Jadoul M. Lancet 2000 ; 355 :")
10
Hyperkaliémie sous spironolactone pour indication cardio (n = 17 en 1996-97)
K médian : 8 mmol / l ! Hémodialyse en urgence n = 4 Décès n = 1 Facteurs de risque ? Créatinine > 2 mg / dl n = 15 Dose Spiron. ≥ 100 mg n = 14 IEC n = 15

11
Kaplan-Meier Analysis of the Probability of Survival
among Patients in the Placebo Group and Patients in the Spironolactone Group Figure 1. Kaplan-Meier Analysis of the Probability of Survival among Patients in the Placebo Group and Patients in the Spironolactone Group. The risk of death was 30 percent lower among patients in the spironolactone group than among patients in the placebo group (P<0.001). Pitt, B. et al. N Engl J Med 1999;341:
. Pitt, B. et al. N Engl J Med 1999;341:")
12
Who Were Receiving ACE Inhibitors
Rate of Prescriptions for Spironolactone among Patients Recently Hospitalized for Heart Failure Who Were Receiving ACE Inhibitors Figure 1. Rate of Prescriptions for Spironolactone among Patients Recently Hospitalized for Heart Failure Who Were Receiving ACE Inhibitors. Each bar shows the observed spironolactone-prescription rate per 1000 patients during one four-month interval. The line beginning in the second interval of 1999 shows projected prescription rates derived from interventional autoregressive integrated moving-average (ARIMA) models, with I bars representing the 95 percent confidence intervals. Juurlink, D. N. et al. N Engl J Med 2004;351:
 models, with I bars representing the 95 percent confidence intervals. Juurlink, D. N. et al. N Engl J Med 2004;351:")
13
Rate of Hospital Admission for Hyperkalemia among Patients Recently Hospitalized for Heart Failure Who Were Receiving ACE Inhibitors Figure 2. Rate of Hospital Admission for Hyperkalemia among Patients Recently Hospitalized for Heart Failure Who Were Receiving ACE Inhibitors. Each bar shows the rate of hospital admission for hyperkalemia per 1000 patients during one four-month interval. The line beginning in the second interval of 1999 shows projected admission rates for hyperkalemia derived from interventional ARIMA models, with I bars representing the 95 percent confidence intervals. Juurlink, D. N. et al. N Engl J Med 2004;351:

14
IR : médicaments à proscrire
Spironolactone : CI si clearance < 40ml/min jamais sans furosémide suivi régulier kaliémie AINS (même les COX-2 sélectifs) Biguanides (acidose lactique)
 Biguanides (acidose lactique)")
15
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? 5. I.R.C.: médicaments à prescrire? 6. Quelques précautions

16
Métabolisme des médicaments (M) en IRC
absorption : normale (?) liaison à l ’albumine : en IRC, réduite pour M anioniques (ex. phénytoïne) donc : fraction libre du M augmentée distribution : selon volume de distribution (V ; l / kg) V = fonction - du poids (oedèmes !) - de la répartition plasma - tissus
 liaison à l ’albumine : en IRC, réduite pour. M anioniques (ex. phénytoïne) donc : fraction libre du M augmentée. distribution : selon volume de distribution. (V ; l / kg) V = fonction - du poids (oedèmes !) - de la répartition plasma - tissus.")
17
Volume de distribution (V)
bas si M surtout distribué dans le plasma ex. bêtalactamines l / kg AINS l / kg élevé si M à forte liaison tissulaire, concentration sélective dans tissus ex. colchicine, prednisolone l / kg cyclosporine l / kg

18
Adaptation de la posologie des médicaments en IRC (I)
Dose d ’attaque * but : taux thérapeutique d’ emblée ex. digoxine, diphantoïne, … * fonction du volume de distribution du médicament (V) * donc habituellement normale en IRC (augmentée si oedèmes +++)
 * donc habituellement normale en IRC. (augmentée si oedèmes +++)")
19
Adaptation de la posologie des médicaments en IRC (II)
Dose d ’entretien : * élimination rénale ++, diminuer dose d ’entretien ou augmenter intervalle entre les doses ex. Sotalol 40 mg/j (au lieu de 160) * élimination hépatique sans élimination rénale (métabolites !), dose =
 * élimination hépatique sans élimination rénale (métabolites !), dose =")
20
Dose d ’entretien inchangée en IRC
anticalciques, métoprolol nitrés héparine, AVK clonidine, guanfacine,moxonidine doxycycline, oxacilline statines oméprazole corticoides, tamoxifène, cyclosporine, tacrolimus

21
Dose d ’entretien réduite en IRC (I)
Clearance ml/min (sujet âgé, créat. 1,5 - 2) * cardio : sotalol % aténolol % acébutolol 50 % * gastro anti-H % domperidone 66 %
 * cardio : sotalol 33 % aténolol 50 % acébutolol 50 % * gastro anti-H2 50 % domperidone 66 %")
22
Dose d ’entretien réduite en IRC (II)
Clearance ml/min (sujet âgé, créat. 1,5 - 2) anticoagulants héparines BPM % rhumato colchicine 50 % allopurinol 50 % méthotrexate % anti-infectieux acyclovir 33 % quinolones % SNC codéine-morphine 66 % lithium 66 %
 anticoagulants héparines BPM % rhumato colchicine 50 % allopurinol 50 % méthotrexate 50 % anti-infectieux acyclovir 33 % quinolones 50-75% SNC codéine-morphine 66 % lithium 66 %")
23
Sources disponibles - Compendium pharmaceutique Néphrologue
à (réponse endéans 24 h) - Livres ou handbooks sur le sujet (ACP)
 - Livres ou handbooks sur le sujet (ACP)")
24
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? I.R.C.: médicaments à prescrire? Quelques précautions

25
Diabète I Lewis et al. NEJM 1993; 329,

26
Néphropathies non-diab.avec protéinurie

27
Brenner et al. N Engl J Med 2001; 345: 861-869
Diabète II Brenner et al. N Engl J Med 2001; 345:

28
Lewis et al. N Engl J Med 2001; 345: 851-860
Diabète II Irbesartan Amlodipine Placebo Lewis et al. N Engl J Med 2001; 345:

29
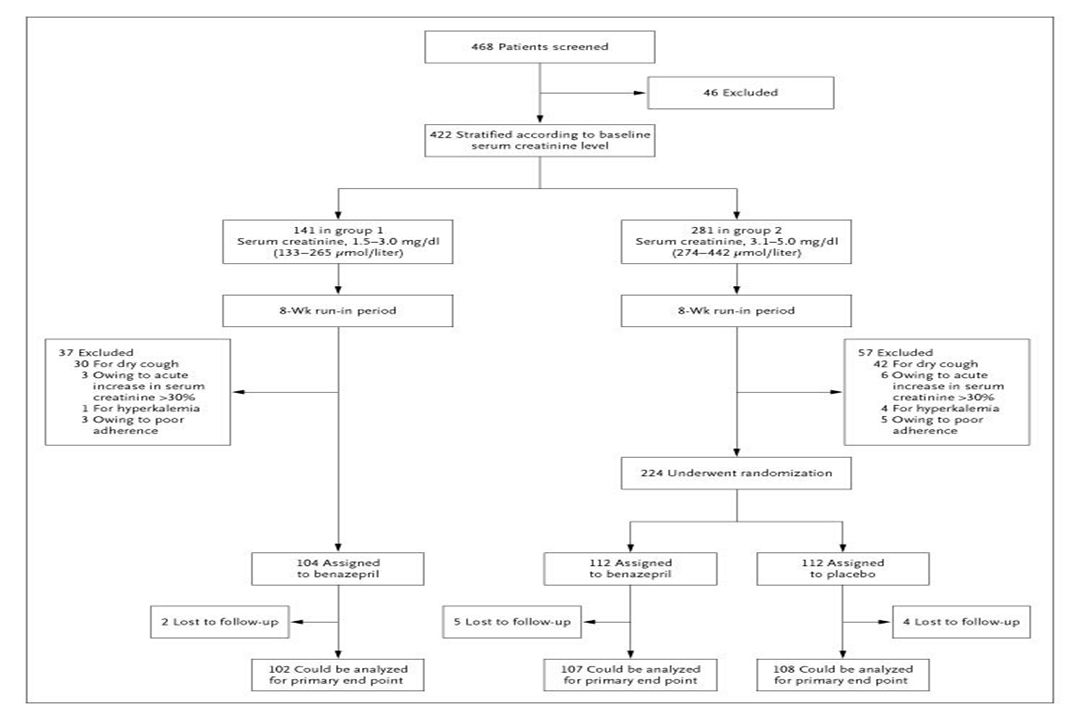
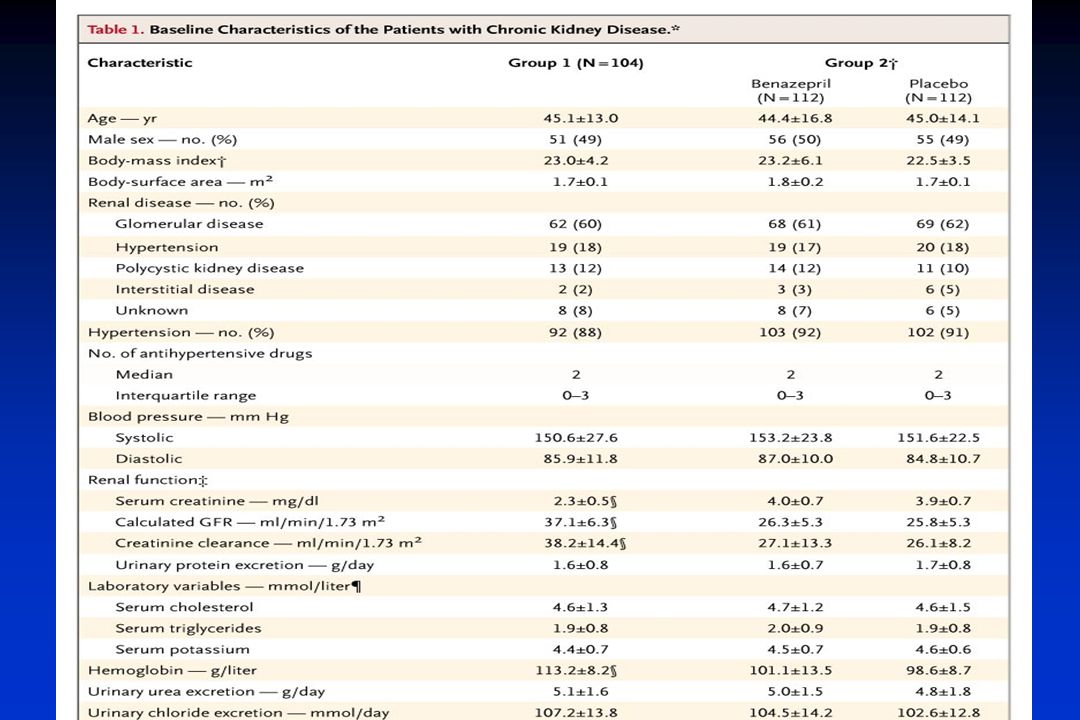
Efficacy and Safety of Benazepril for
Advanced Chronic Renal Insufficiency Fan Fan Hou, M.D., Ph.D., Xun Zhang, M.D., Guo Hua Zhang, M.D., Ph.D., Di Xie, M.D., Ping Yan Chen, M.D., Wei Ru Zhang, M.D., Ph.D., Jian Ping Jiang, M.D., Min Liang, M.D., Ph.D., Guo Bao Wang, M.D., Zheng Rong Liu, M.D. and Ren Wen Geng, M.D. N Engl J Med Volume 354;2: January 12, 2006

32
Kaplan-Meier Estimates of the Percentage of Patients Not Reaching the Primary Composite End Point of a Doubling of the Serum Creatinine Level, End-Stage Renal Disease, or Death

33
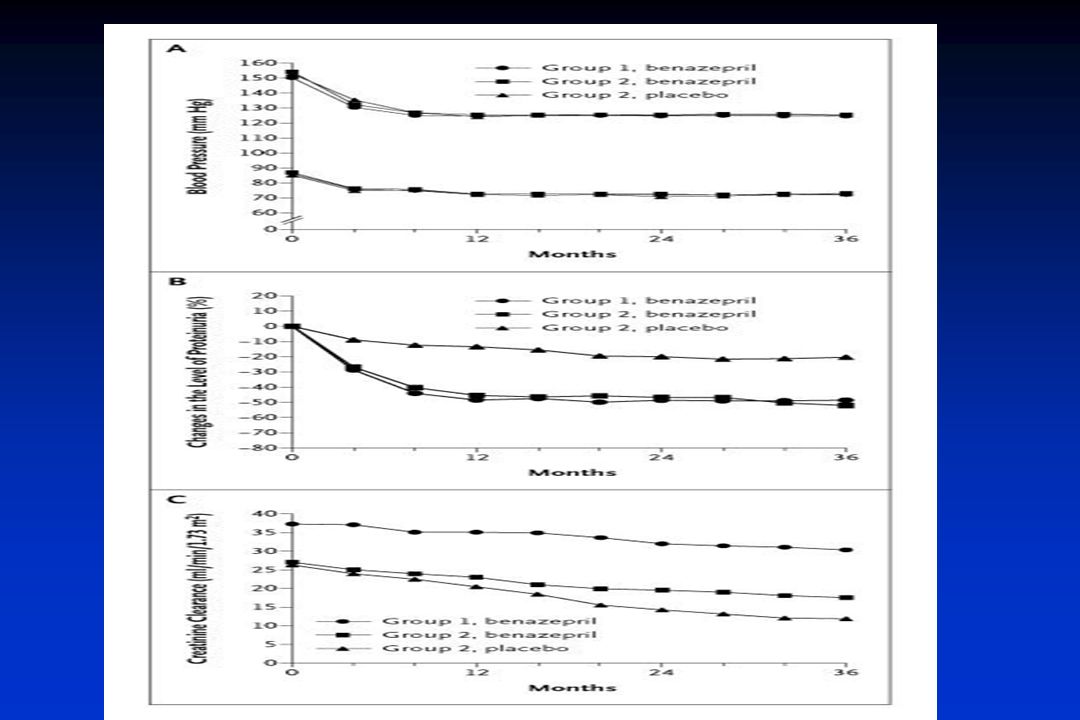
Use of Conventional Antihypertensive Medications at Baseline and during Study Treatment
Hou, F. et al. N Engl J Med 2006;354:

35
Adverse Events after Randomization
Hou, F. et al. N Engl J Med 2006;354:

36
Efficacy and variability of the anti-proteinuric effect of ACEI by lisinopril
Protéinuria, g / 24 h Low salt Low salt High salt Low salt methyldopa lisinopril lisinopril lisinopril Heeg et al. Kidney Int 1989; 36:

37
Buter et al. Nephrol Dial Transplant 1998; 13: 1682-1685

38
IEC et I.R. Start IEC —> créatinine augmente —> stop IEC ??

39
IEC : stop si hausse créatinine ?
créatinine < 3 mg/dl , qui augmente de < 30 % : association +++ avec préservation GFR Bakris et al. Arch Int Med 2000; 160:

40
Hyperkaliémie sous IEC/sartan (I)
Hyperkaliémie vraie? - délai prélèvement- analyse? - hémolyse? - confirmée malgré précautions de prélèvement? sévère? (> 5.8 mmol/l) Rappels diététiques - sels de régime - fruits secs, bananes, fruits, chocolat, café soluble,....
 Rappels diététiques. - sels de régime. - fruits secs, bananes, fruits, chocolat, café soluble,....")
41
Hyperkaliémie sous IEC/sartan (II)
Arrêt AINS , même COX-2 Corriger acidose éventuelle (Vichy 1-2 v/j) IEC + sartan: stop ou réduction 1 des 2 IEC ( sartan) + spironolactone: stop spironolactone IEC ou sartan en monothérapie: - dose IEC/sartan - ajouter furosémide Si persiste, rajouter kayexalate sodique 15 g/2 j per os
 IEC + sartan: stop ou réduction 1 des 2. IEC ( sartan) + spironolactone: stop spironolactone. IEC ou sartan en monothérapie: - dose IEC/sartan. - ajouter furosémide. Si persiste, rajouter kayexalate sodique 15 g/2 j per os.")
42
Plan Questions face à toute insuffisance rénale (I.R.)
Médicaments à incriminer? 3. I.R.C. : médicaments à proscrire ? 4. I.R.C. : médicaments à adapter ? 5. I.R.C.: médicaments à prescrire? 6. Quelques précautions

43
Serum creatinine (mg/dl)
Saline Mannitol and Saline Furosemide and Saline Serum creatinine (mg/dl) Before angiography 48 Hr later Before angiography 48 Hr later Before angiography 48 Hr later Solomon et al. NEJM 1994; 331:
 Before. angiography. 48 Hr. later. Before. angiography. 48 Hr. later. Before. angiography. 48 Hr. later. Solomon et al. NEJM 1994; 331:")
44
Serum creatinine (mg/dl) Saline and Acetylcysteine
Before administration of contrast agent 48 Hr later Before administration of contrast agent 48 Hr later Saline Saline and Acetylcysteine Tepel et al. NEJM 2000 ; 343:

45
Prévention de la toxicité du contraste
Arrêt des diurétiques 48 H avant l’examen Eau de Vichy Célest. 1Litre per os la veille de l’examen (si possible) Avertir le radiologue/cardiologue de l’IRC (choix et dose du produit de contraste ) Acétylcystéine :métaanalyses contradictoires ne dispense pas de ci-dessus
 Avertir le radiologue/cardiologue de l’IRC (choix et dose du produit de contraste ) Acétylcystéine :métaanalyses contradictoires. ne dispense pas de ci-dessus.")
46
Summary Recommendations of Interventions Commonly Used to Reduce the Risk of Contrast-Medium-Induced Nephropathy Table 2. Summary Recommendations of Interventions Commonly Used to Reduce the Risk of Contrast-Medium-Induced Nephropathy. Barrett, B. J. et al. N Engl J Med 2006;354:

47
Conclusion Face à une insuffisance rénale,
s’interroger - sur les médicaments à incriminer proscrire (spironolactone !) adapter (accumulation …) prescrire (IEC..) - sur les préacutions à prendre
 adapter (accumulation …) prescrire (IEC..) - sur les préacutions à prendre.")
Présentations similaires











>")







