Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Mécanismes de résistance aux antibiotiques/ Interprétation de l’antibiogramme
J.L. Mainardi Unité Mobile de Microbiologie Clinique Hôpital Européen Georges Pompidou Université Paris V René Descartes Paris

2
Mécanisme de résistance lié au mode d’action de l’antibiotique
Généralités (1) Mécanisme de résistance lié au mode d’action de l’antibiotique Colimycine 2 Béta-lactamines Glycopeptides Fosfomycine 4 Aminosides-Macrolides Tétracyclines-acide fusidique Linézolide- chloramphénicol Quinolones Rifampicine, sulfamides
 Mécanisme de résistance lié au mode d’action de l’antibiotique. Colimycine. 2. Béta-lactamines. Glycopeptides. Fosfomycine. 4. Aminosides-Macrolides. Tétracyclines-acide fusidique Linézolide- chloramphénicol. Quinolones. Rifampicine, sulfamides.")
3
Généralités (2) La résistance est soit naturelle soit acquise
4 grands mécanismes de résistance Enzymatique : le plus fréquent Modification de la cible Imperméabilité Efflux

4
Généralités (3) La résistance naturelle est caractéristique d’une espèce ou d’un genre ou d’un groupe Bactéries à Gram+ : colistine (structure) acide nalidixique (cible) Bactéries à Gram- : vancomycine (structure) Anaérobie : aminosides (imperméabilité) Genre Klebsiella : amoxicilline, ticarcilline, Pipéracilline (pénicillinase) Espèce E. faecalis : Céphalosporines (tous les entérocoques)- lincomycine-Clindamycine
 acide nalidixique (cible) Bactéries à Gram- : vancomycine (structure) Anaérobie : aminosides (imperméabilité) Genre Klebsiella : amoxicilline, ticarcilline, Pipéracilline (pénicillinase) Espèce E. faecalis : Céphalosporines (tous les entérocoques)- lincomycine-Clindamycine.")
5
Antibiotiques actifs sur la paroi bactérienne
1) Béta-lactamines 2) Glycopeptides 3) Fosfomycine
 Béta-lactamines 2) Glycopeptides 3) Fosfomycine.")
6
Gram + Gram - Acides lipoteicoiques Acides teicoiques

7
Structure du peptidoglycane

8
Synthèse du peptidoglycane
Glycosyltransférase Transpeptidase PLP PLP

9
Protéines de liaison à la pénicilline
Classe A glycosyltransférase Plp transpeptidase Classe B non catalytique Plp transpeptidase

10
Action des béta-lactamines
PLP PLP Arrêt de la synthèse du peptidoglycane Béta-lactamine Inactivation de la PLP

11
Résistance aux béta-lactamines
Peptido BETA- LACTAMASE Membrane interne Cytoplasme

12
Résistance aux béta-lactamines
Peptidoglycane PLP mutée PLP Normale PLP mutée BETA LACTAMASE MODIFICATION DE CIBLE Membrane interne Cytoplasme

13
Résistance aux béta-lactamines
IMPERMEABILITE Porine modifiée Membrane externe (Gram-) Peptido PLP Normale PLP mutée BETA LACTAMASE MODIFICATION DE CIBLE Membrane interne Cytoplasme
 Peptido. PLP Normale. PLP mutée. BETA LACTAMASE. MODIFICATION DE CIBLE. Membrane interne. Cytoplasme.")
14
Résistance aux béta-lactamines
IMPERMEABILITE Membrane externe (gram-) Porine modifiée Peptido PLP Normale PLP mutée BETA LACTAMASE EFFLUX MODIFICATION DE CIBLE Membrane interne Cytoplasme
 Porine. modifiée. Peptido. PLP Normale. PLP mutée. BETA LACTAMASE. EFFLUX. MODIFICATION DE CIBLE. Membrane interne. Cytoplasme.")
15
Action des glycopeptides
Arrêt de la transpeptidation D-Ala5-D-Ala4 Glycopeptide PLP Arrêt de la synthèse du peptidoglycane

16
O C l H N 3 2 X Vancomycine D-Ala4-D-Ala5

17
Résistance aux glycopeptides
D-lactate or D-serine en 5ème position Van A, Van B, Van C Glycopeptide Modification de la cible PLP

18
Action de la fosfomycine
Peptidoglycane Cytoplasme Fosfomycine Enz Précurseur du peptidoglycane 1 Précurseur du peptidoglycane 2

19
Résistance à la fosfomycine
Peptidoglycane Mutation Cytoplasme Fosfomycine Enz Précurseur 1 Précurseur 2

20
Antibiotiques actifs sur la synthèse des protéines
1) Aminosides 2) Macrolides-lincosamides 3) Cyclines 4) Chloramphénicol 5) Ac. Fusidique 6) Linézolide
 Aminosides 2) Macrolides-lincosamides 3) Cyclines 4) Chloramphénicol 5) Ac. Fusidique 6) Linézolide.")
21
Fonctionnement du ribosome
ARN23S + ARN5S + protéines ARN16S + protéines

22
Sites de fixation des antibiotiques
Macrolides Lincosamides Synergistines Aminosides 16S 23S Cyclines Chloramphénicol Linézolide

23
Résistance aux ATB actifs sur la synthèse protéique
Modification de la cible par mutation Méthylation du ribosome pour les macrolides Production d’une enzyme Enzymes détruisant les aminosides Efflux Macrolides Tétracyclines

24
Antibiotiques actifs sur la synthèse des acides nucléiques
1) Quinolones 2) Rifampicine 3) Sulfamides - triméthroprime
 Quinolones 2) Rifampicine 3) Sulfamides - triméthroprime.")
25
Action des quinolones ADN Quinolone
Sous- unité A des Gyrases et topoisomérases ADN Quinolone Sous- unité B des Gyrases et topoisomérases

26
Résistance aux quinolones
Le plus fréquent : modification de la cible (gyrase et topoisomérase) Efflux Protection de la cible: protéines Qnr Inactivation enzymatique: Aminoside acétyltransférase
 Efflux. Protection de la cible: protéines Qnr. Inactivation enzymatique: Aminoside acétyltransférase.")
27
Action sulfamides, triméthoprime et rifampicine
Précurseur 1 DHPS Précurseur 2 Précurseur 3 DHFR ADN Précurseur 4 ARN polymérase transcription ADN Purines ARN

28
Action sulfamides, triméthoprime et rifampicine
Précurseur 1 DHPS Sulfamides Précurseur 2 Rifampicine Précurseur 3 Trimethop. DHFR ADN Précurseur 4 ARN polymérase transcription ADN Purines ARN

29
Résistance aux sulf., triméth. et rifampicine
Précurseur 1 Mutation DHPS Sulfamides Précurseur 2 Rifampicine Précurseur 3 Triméthop. DHFR ADN Précurseur 4 ARN polymérase transcription ADN Purines ARN

30
Support de la résistance
Gènes portés par des chromosomes Gènes portés par des plasmides Gènes portés par des transposons Conséquences Transmission de bactéries à bactéries (plasmide et transposon) Émergence de la résistance Résistance multiple +++ par différents mécanismes pour une classe d’antibiotique et par différents mécanismes pour des classes différentes: bactéries multirésistantes
 Émergence de la résistance. Résistance multiple +++ par différents mécanismes pour une classe d’antibiotique et par différents mécanismes pour des classes différentes: bactéries multirésistantes.")
31
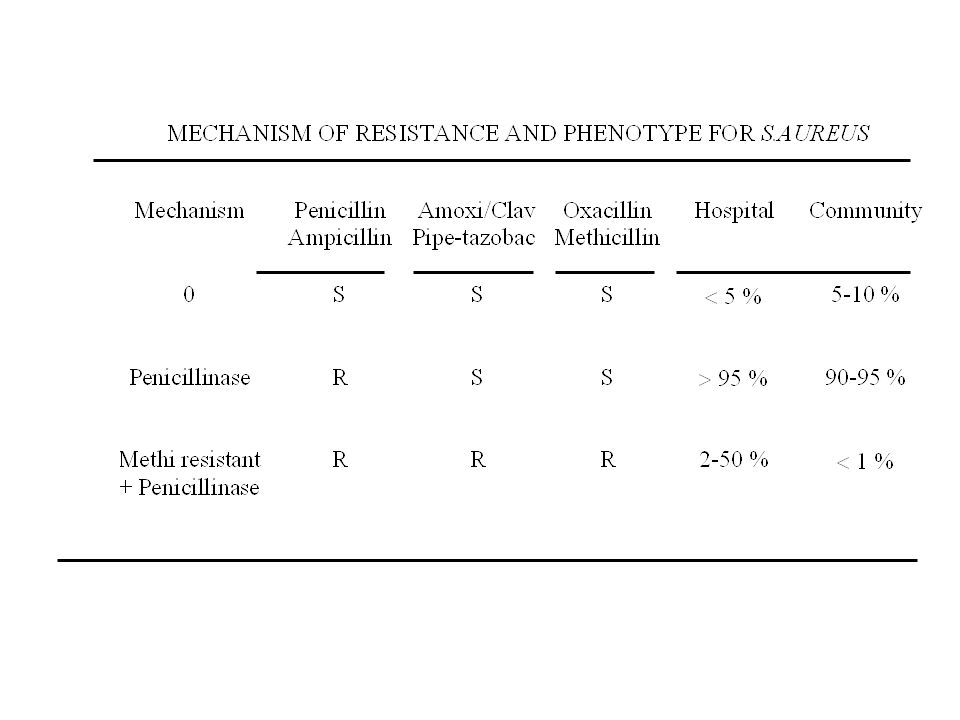
A 50-year old man developed a nosocomial pneumonia
A 50-year old man developed a nosocomial pneumonia. An empiric treatment with piperacillin is begun. The microbiological results of the protected brush specimen showed: UFC/ml of Staphylococcus aureus Penicillin: R Piperacillin: S Oxacillin (methicillin): S All the other antibiotics: S What do you think about this antibiogramme ?: * True * False
: S. All the other antibiotics: S. What do you think about this antibiogramme : * True. * False.")
32
ANSWER * FALSE - Impossible antibiogramme - Strain penicillin resistant = piperacillin resistant due to the production of penicillinase. - The activity is restored in presence of b-lactamase inhibitor as clavulanic acid or tazobactam

33
What do you think about this antibiogramme ?: * True * False
A 40 year-old man, with a mechanical mitral prosthesis, presented a catheter-related infection with positive blood cultures due to Staphylococcus aureus: Penicillin R Oxacillin (methicillin) R Imipenem S Kanamycin R Tetracycline R Vancomycin R All the other antibiotics are resistant What do you think about this antibiogramme ?: * True * False
 R. Imipenem S. Kanamycin R. Tetracycline R. Vancomycin R. All the other antibiotics are resistant. What do you think about this antibiogramme : * True. * False.")
34
ANSWER * FALSE - Impossible antibiogramme because: - Oxacillin R due to the acquisition of additional PBP2a with a low affinity for methicillin - Oxacillin R = imipenem R - Oxacillin R = resistant to all b-lactams - Is the strain really resistant to vancomycin ? (GISA ? High level resistance to vancomycin)
")
36
Clinical isolates with decreased susceptibility to vancomycin
1996: Japan (Hiramatsu et al, JAC 1997) MIC: 8 µg/ml vanco, 16 µg/ml teicoplanin Heterogeneous resistance : 10-6 (Lancet, 1997) 1.3 to 20% in Japanese hospitals Since 1997: USA, United-kingdom, France, Spain, and many other countries In Europe: true incidence not known but seems lower (0.5 to 1.5 %) in absence of outbreak (Schmitz et al.,1999; Chesneau et al., 2000; Marchese et al ; 2000; Reverdy et al., 2001) Diapo 5 concerning Title , you know the first description by Hiramatsu of a strain isolated form a sternal abcess in a patient previously treated with vancomycin. The MIC were ..... One year later, he described the existence of strains which showed hetereginieus resistance to vancomycin. This strain appears susceptible to vancomycin when standard MICs are performed but contained a population eible to grow at a concentration > to 4 µg/ml of vancomycin at a freqwency about 10-6 was a ..... Theses hetereginieus vancomycin resistant strains represent about 1.3 % to 20% of the MRSA strains isolated in japanise hospital Since this date, clinical isolates with decreased susceptibility to vancomycin have been reported in
 MIC: 8 µg/ml vanco, 16 µg/ml teicoplanin. Heterogeneous resistance : 10-6 (Lancet, 1997) 1.3 to 20% in Japanese hospitals. Since 1997: USA, United-kingdom, France, Spain, and many other countries. In Europe: true incidence not known but seems lower (0.5 to 1.5 %) in absence of outbreak. (Schmitz et al.,1999; Chesneau et al., 2000; Marchese et al ; 2000; Reverdy et al., 2001) Diapo 5 concerning Title , you know the first description by Hiramatsu of a strain isolated form a sternal abcess in a patient previously treated with vancomycin. The MIC were One year later, he described the existence of strains which showed hetereginieus resistance to vancomycin. This strain appears susceptible to vancomycin when standard MICs are performed but contained a population eible to grow at a concentration > to 4 µg/ml of vancomycin at a freqwency about 10-6 was a Theses hetereginieus vancomycin resistant strains represent about 1.3 % to 20% of the MRSA strains isolated in japanise hospital. Since this date, clinical isolates with decreased susceptibility to vancomycin have been reported in")
37
Clinical isolates with decreased susceptibility to teicoplanin
MICs: 8-16 µg/ml for teicoplanin/ 2-4 for vancomycin 1988:Brunet et al (Eur J Clin Microbiol, 1990) 1989: Kaatz et al (J Infect Dis, 1990), Vedel et al (Eur J Clin Microbiol, 1990) : Mainardi et al (J Infect Dis, 1995) Diapo 3: In fact, the problem of GISA is not a new phenomena because clinical isolates with decreased susceptibility to teicoplanin have been described by ……. The MICs for the clinical isolates This strain could be considered susceptible to vancomycin according to the breakpoint but in fact the MICs are higher than the foully glycopeptide susceptible strains.
 1989: Kaatz et al (J Infect Dis, 1990), Vedel et al (Eur J Clin Microbiol, 1990) : Mainardi et al (J Infect Dis, 1995) Diapo 3: In fact, the problem of GISA is not a new phenomena because clinical isolates with decreased susceptibility to teicoplanin have been described by ……. The MICs for the clinical isolates This strain could be considered susceptible to vancomycin according to the breakpoint but in fact the MICs are higher than the foully glycopeptide susceptible strains.")
38
Le risque majeur chez S. aureus
Infection with vancomycin-resistant Staphylococcus aureus containing the vanA resistance gene CMI de la vancomycin: 1024 µg/ml Présence du gène vanA Présence de E. faecalis avec gène VanA Sensibilité aux : Chloramphénicol, Linézolide, Minocycline, SynercidR, triméthoprime-sulfaméthoxazole Chang et al, N Engl J Med 2003;348:

39
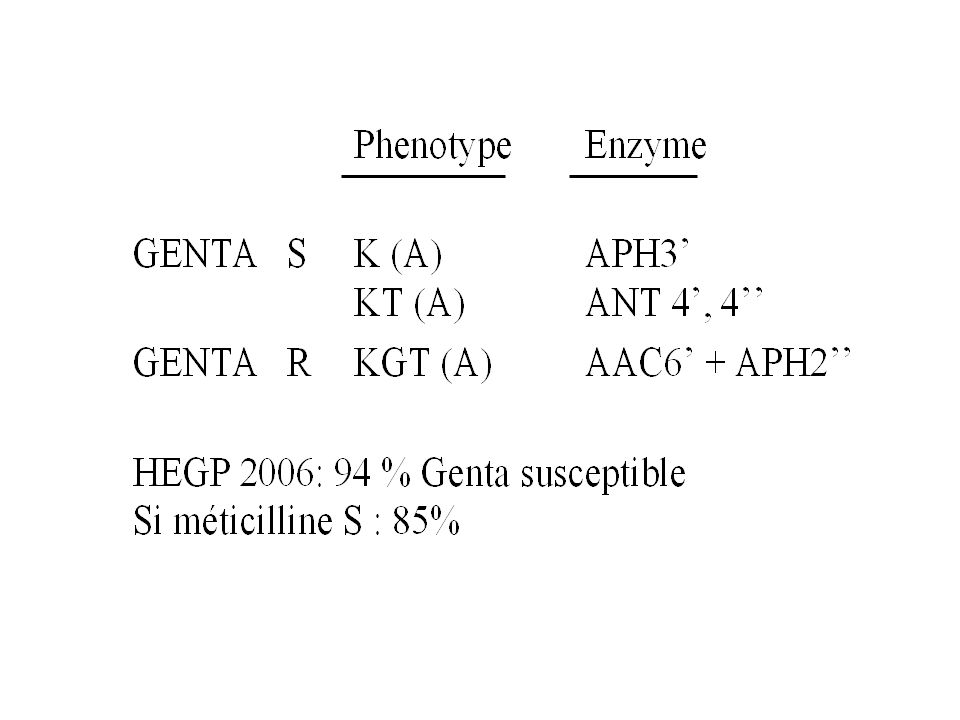
What do you think about this antibiogramme of Staphylococcus aureus ?
Oxacillin (methicillin) R Kanamycin R Gentamicin S Tobramycin R Amikacin S Netilmicin S * True ? * False ?
 R. Kanamycin R. Gentamicin S. Tobramycin R. Amikacin S. Netilmicin S. * True * False")
40
ANSWER * FALSE - Impossible phenotype because: - Kanamycin resistant = Amikacin resistant

41
What do you think about this antibiogramme of Staphylococcus aureus ?
Oxacillin R Kanamycin R Gentamicin R Tobramycin R Amikacin R Netilmicin S * True ? * False ?

42
ANSWER * FALSE - Impossible phenotype because: - Gentamicin resistant = resistant to all aminoglycosides, except streptomycin

44
A methicillin-resistant strain of Staphylococcus aureus is interpreted as:
Pefloxacin R Ciprofloxacin S Norfloxacin S Is it true ? or false ?

45
ANSWER * FALSE - Impossible phenotype because: - Cross-resistance for all fluoroquinolones in S. aureus - Alterations of the same target (DNA gyrase)
")
46
What is the percentage of S
What is the percentage of S. aureus resistant to fluoroquinolones in hospital ? - 10 % - 30 % - 60 % - 90 %

47
ANSWER - Hospital :depending the percentage of methicillin resistance - 20 à 30% in France

48
What is the percentage of S
What is the percentage of S. aureus resistant to fluoroquinolones in the community ? - < 10 % - 30 % - 60 % - 90 %

49
ANSWER - Community: < 10%

50
SARM-communautaire

51
What do you think about this antibiogramme of Enterococcus faecalis ?
Amoxicillin S Cephalotin (1ère génération) S Gentamicin S Erythromycin S Clindamycin R Vancomycin S Is it true or false ?
 S. Gentamicin S. Erythromycin S. Clindamycin R. Vancomycin S. Is it true or false")
52
ANSWER: - FALSE - Impossible phenotype because : - Enterococci are naturally resistant to cephalosporins - Enterococci are naturally resistant to aminoglycosides (low level: MIC µg/ml) - True concerning the clindamycin
 - True concerning the clindamycin.")
53
Among these different bacteria species, which of these are naturally resistant to vancomycin ?
Enterococcus faecium Enterococcus gallinarium Enterococcus casseliflavus Enterococcus faecalis Escherichia coli

54
ANSWER Enterococcus gallinarium Enterococcus caselliflavius Escherichia coli

55
- Normal C-terminal amino acid of the pentapeptide chain of the peptidoglycan: D-alanine Vanco S
- Modification of this amino acid: resistance to vancomycin VanA, VanB : D-lactate (MIC 16 µg/ml) VanC : D-serine (MIC = 8 µg/ml) -VanC : detection on the antibiogramme: : not easy ! - MICs of vancomycin > MICs of teicoplanin - Necessity to identify the species (E.gallinarium)
 VanC : D-serine (MIC = 8 µg/ml) -VanC : detection on the antibiogramme: : not easy ! - MICs of vancomycin > MICs of teicoplanin. - Necessity to identify the species (E.gallinarium)")
56
Chaîne pentapeptidique
Vanco Vanco S D-Ala Chaîne pentapeptidique Vanco R Vanco D-Ser ou D-lactate

57
Streptococcus pneumoniae
What do you think about this resistant phenotype ? Penicillin R Chloramphenicol S Cotrimoxazole S Tetracycline S Erythromycin S Is it possible ? - Yes ? - Not ?

58
ANSWER - Yes - Possible phenotype because some strains present an isolated resistance to penicillin

59
Streptococcus pneumoniae
The frequency of resistance is: - Tetracycline 30 % - Erythromycin 53 % - Chloramphenicol 11 % - Cotrimoxazole 33 % - Fosfomycine 4 % - Rifampin 0,5 % CNRP Rapport d’activité 2004

60
Concernant la résistance aux bêta-lactamines chez les pneumocoques
-L’imipénème est toujours plus actif que l’amoxicilline? -Dans une méningite pourrait on utiliser l’imipénème , le méropénème? -Les céphalosporines de troisième génération peuvent être moins actives que l’amoxicilline

61
Concernant la résistance oux bêta-lactamines chez pneumocoque
-L’imipénème est toujours plus actif que l’amoxicilline? Oui -Dans une méningite pourrait on utiliser l’imipénème , le meropénème? Meropénème pourquoi pas hors AMM??? -Les céphalosporines de troisième génération peuvent être moins sensibles que l’amoxicilline Oui CRO: 8/32 Peni 0.25/2-4 Moralité: Antibiogramme et CMI

62
Que pensez vous de cet antibiogramme chez S. pneumoniae ?
Erythromycin/Roxythomycin (C14) R R Azithromycin (C15) R S Spiramycine /Josamycine (C16) R S Clindamycin R S Télithromycin S S Vrai ou faux ?
 R R. Azithromycin (C15) R S. Spiramycine /Josamycine (C16) R S. Clindamycin R S. Télithromycin S S. Vrai ou faux")
63
MLSb Mef efflux France 51% 3-5 % Italy % Usa % Macrolides 14, 15 R R Macrolides 16 R S Lincosamides R S Ketolides S S Streptogramin (A + B) S S
 S S.")
64
Ciprofloxacine Péfloxacine Lévofloxacine Ofloxacine Moxifloxacine
Chez S. pneumoniae quel est l’ordre d’activité croissante des différentes fluoroquinolones ? Ciprofloxacine Péfloxacine Lévofloxacine Ofloxacine Moxifloxacine

65
Chez S. pneumoniae quel est l’ordre d’activité croissante
des différentes fluoroquinolones ? Péfloxacine 8 Ciprofloxacine 2 Ofloxacine 1/2 Lévofloxacine /1 Moxifloxacine

66
Les mécanismes de R aux quinolones sont ils liés à la présence de:
Une ou plusieurs enzymes détruisant les Fqs ? Mutation(s) dans la cible avec diminution d’affinité ? Efflux ?
 dans la cible avec diminution d’affinité Efflux")
67
Les mécanismes de R sont ils liés à la présence de:
Une ou plusieurs enzymes détruisant les Fqs ? Bifunctional acetyltransferase : AAC(6’)-Ib-cr Confers reduced susceptibility to aminoglycosides and fluoroquinolones (MIC of ciprofloxacin increased 3 fold) (Robicsek et al. Nat Med 2006) Mutation(s) dans la cible avec diminution d’affinité ? ADN Gyrase Efflux-perméabilité ? Oui
-Ib-cr. Confers reduced susceptibility to aminoglycosides and fluoroquinolones (MIC of ciprofloxacin increased 3 fold) (Robicsek et al. Nat Med 2006) Mutation(s) dans la cible avec diminution d’affinité ADN Gyrase. Efflux-perméabilité Oui.")
68
Cephalotin (1st generation cephalosporin) S Piperacillin S
A 30 year-old woman is treated for a pyelonephritis due to klebsiella pneumoniae. The antibiogramme is : Ampicillin R Ticarcillin R Cephalotin (1st generation cephalosporin) S Piperacillin S The patient is treated by piperacillin, the fever persist, and the white blood count is /mm3. Are you surprised ? - YES ? - NO ?
 S. Piperacillin S. The patient is treated by piperacillin, the fever persist, and the white blood count is /mm3. Are you surprised - YES - NO")
69
ANSWER - No - Impossible phenotype because: - K. pneumoniae harbor a natural chromosomal penicillinase for which piperacillin is a substrate

70
Cephalotin (1st generation cephalosporin) S
A protected brush specimen yield with > 103 UFC/ml of Enterobacter cloacae during a nosocomial pneumonia. The antibiogramme is: Ampicillin R Ticarcillin S Cephalotin (1st generation cephalosporin) S A treatment with cephalotin is begun because the patient is allergic to penicillin. The evolution is bad. Are you surprised ? -YES ? - NO ?
 S. A treatment with cephalotin is begun because the patient is allergic to penicillin. The evolution is bad. Are you surprised -YES - NO")
71
ANSWER - NO, the phenotype is impossible because E. cloacae produce a natural chromosomal cephalosporinase. - Ampicillin and 1st generation cephalosporins are natural substrates for the cephalosporinase

73
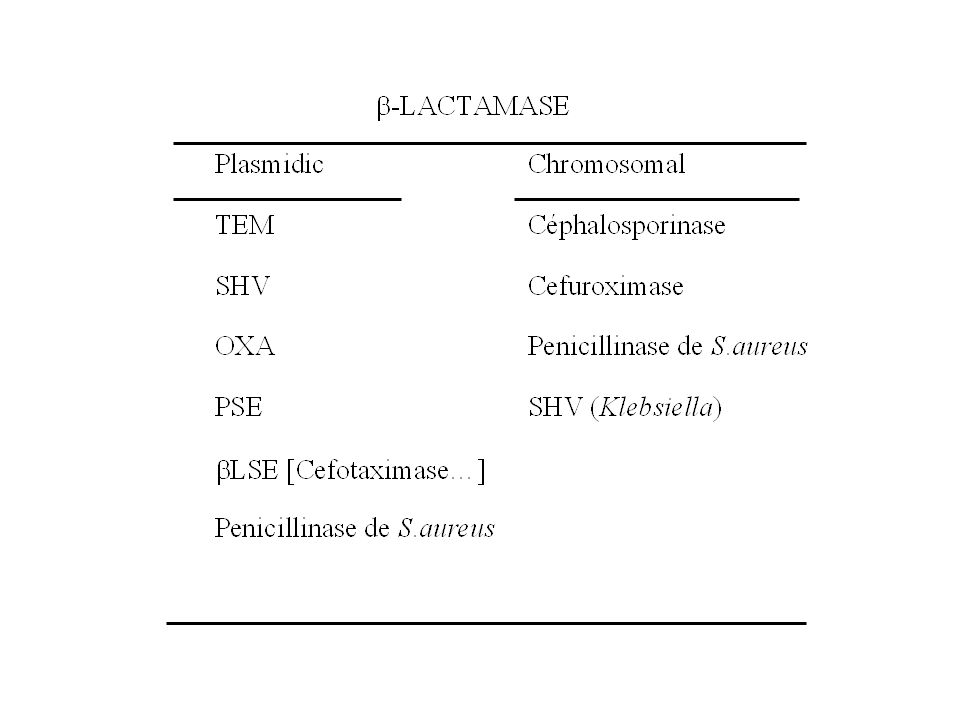
-lactamases most frequently present in clinical isolates
Penicillinases Natural : klebsiella TEM Enterobacteria Plasmidic : SHV ++ Cephalosporinases Natural : E. cloacae Citrobacter Serratia Pseudomonas Plasmidic: yes, but rare C P

74
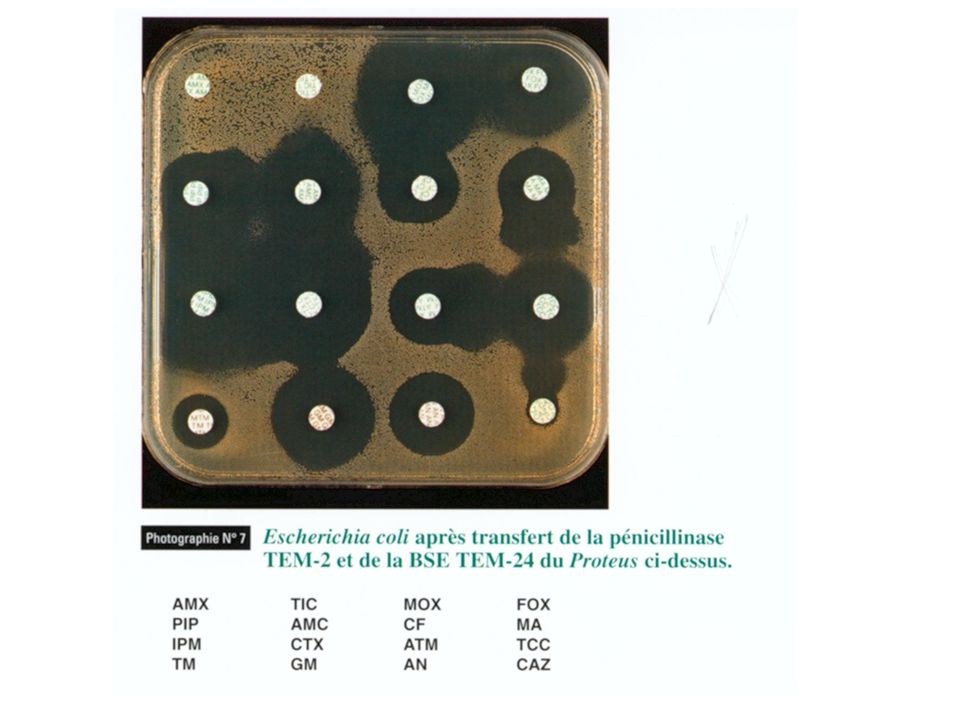
What do you think about this antibiogramme ? Ampicillin R
E. COLI What do you think about this antibiogramme ? Ampicillin R Ticarcillin R Cephalotin (1st generation cephal) I Amoxicillin- clavulanic acid I Possible ? - YES - NO
 I Amoxicillin- clavulanic acid I. Possible - YES. - NO.")
75
ANSWER : - YES - Possible: the strain hyperproduces a penicillinase

76
Cephalotin (1st generation cephalosporin) S
E. COLI Ampicillin R Ticarcillin R Cephalotin (1st generation cephalosporin) S Amoxicillin- clavulanique acid R Possible ? -YES ? - NO ?
 S. Amoxicillin- clavulanique acid R. Possible -YES - NO")
77
Possible: IRT (inhibitor resistant TEM) strain
ANSWER Possible: IRT (inhibitor resistant TEM) strain
 strain.")
78
TEM IRT Mutation I I

82
The antibiogramme of a Pseudomonas aeruginosa strain responsible for a nosocomial urinary tract infection is as follow: Ticarcillin S Piperacillin S Ceftazidime S Imipenem I Is it possible ? - YES or - NO

83
ANSWER : - Possible phenotype - Resistance to imipenem due to the association of the loss of one specific porin (D2) and the production of cephalosporinase
 and the production of cephalosporinase.")
85
of Pseudomonas aeruginosa
IMIPENEM S CEFTAZIDIME S R S Cepase Cepase IMI CEFTA 12 to 20 % of the strains of Pseudomonas aeruginosa

86
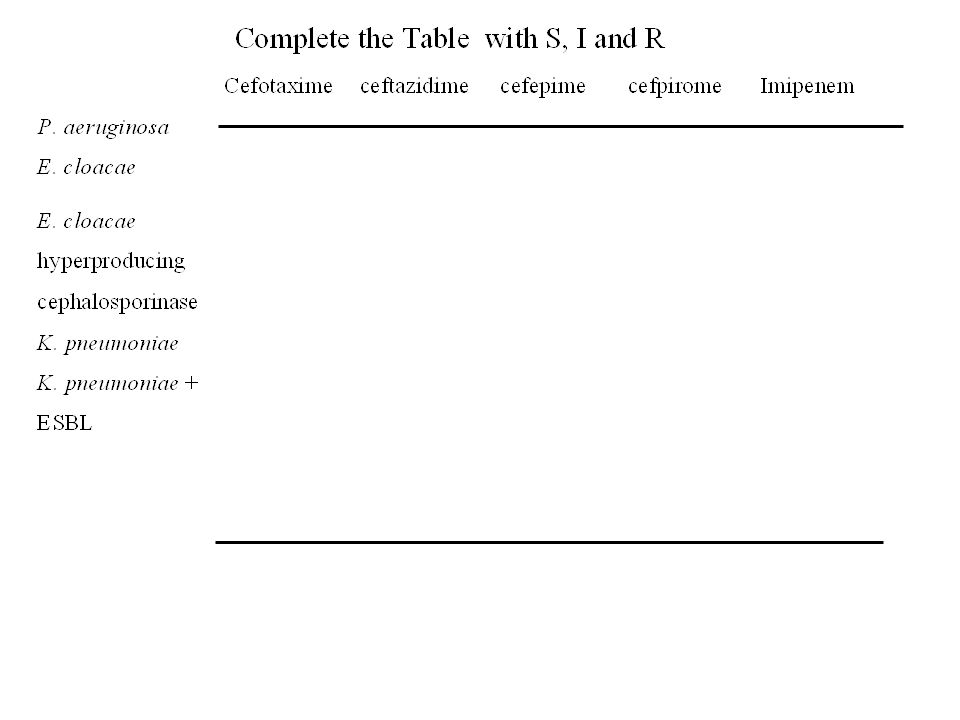
Complete by susceptible (S), Intermediate (I) or Resistant (R)
the different phenotypes of resistance in P. aeruginosa TIC PIP CAZ AZT IMP Wild type Penicillinase Cephalosporinase hyperproducing Non enzymatic resistance (eflux) Loss of porin D2
 Loss of porin D2.")
87
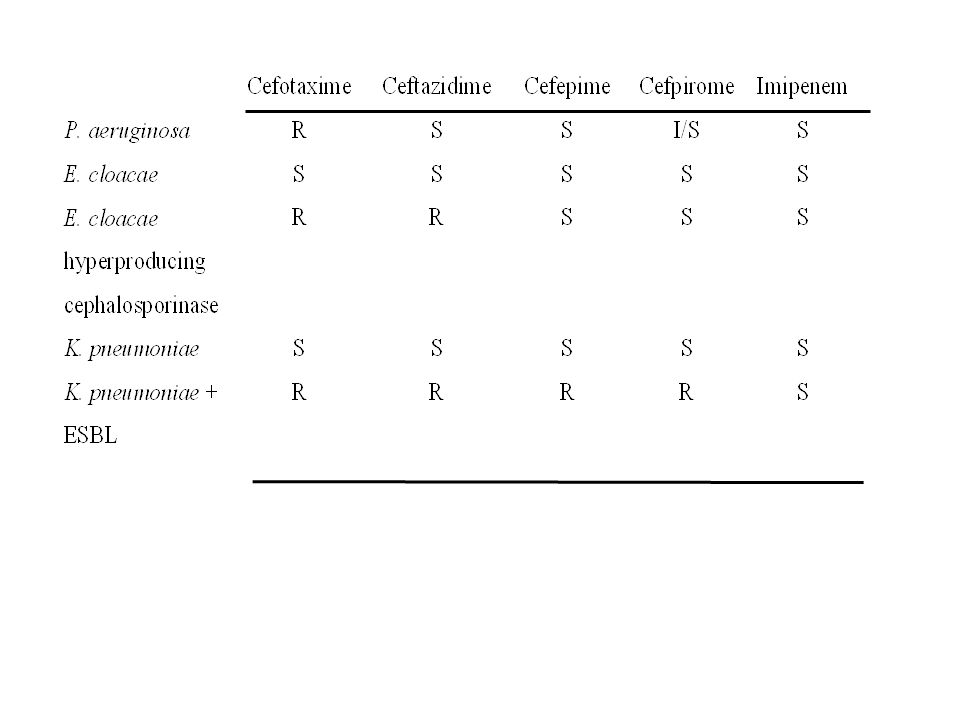
Phenotypes of resistance in P. aeruginosa
TIC PIP CAZ AZT IMP S S S S S Wild type R R S S S Penicillinase R R I/R I/R S Cephalosporinase hyperproducing I S S I S Non enzymatic resistance (eflux) S S S S I Loss of porin D2
 S. S. S. S. I. Loss of porin D2.")
88
Existe t’il des bêta-lactamases détruisant l’imipenème ??
Non? Pourquoi? Oui? Quelles espèces

89
Carbapénèmases dans le monde
Classes A. NMC-A SME-1 SME-2 SME-3 IMI-1 KPC-1 GSE-1 France U.K U.S.A South Africa (E. cloacae) (S. marcescens) (K. pneumoniae) (P. aeruginosa) B. IMP-1 IMP-2 IMP3 VIM-1 VIM-2 (épidémie) Japon Italie Chine Grèce (A. baumanii) (P.aeru., K. pneumoniae) D. OXA Belgique Singapour Portugal
 (S. marcescens) (K. pneumoniae) (P. aeruginosa) B. IMP-1. IMP-2. IMP3. VIM-1. VIM-2. (épidémie) Japon. Italie. Chine. Grèce. (A. baumanii) (P.aeru., K. pneumoniae) D. OXA. Belgique. Singapour. Portugal.")
90
Est-ce vrai ? : les Bacteroides fragilis sont toujours sensibles à l’imipénème ? les Bacteroides fragilis sont toujours sensibles au métronidazole ? les Bacteroides fragilis sont toujours sensibles à la clindamycine ? les Bacteroides fragilis sont généralement sensibles à l’amoxicilline ?

91
% de Résistance chez B. fragilis
l’imipénème < 5% % métronidazole % clindamycine 25 % l’amoxicilline % Augmentin en 1980 / < 10 % actuellement

Présentations similaires

















>")

