Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Bilan d’hémostase, TCA, Willebrand…
Charles Marc SAMAMA Départements d’Anesthésie-Réanimation CHU Avicenne, Bobigny / CHU Hôtel Dieu, Paris

3
Preoperative hemostatic evaluation Samuel I Rapaport, Blood, 1983
When the whole blood clotting time and the Duke bleeding time were the tests used to screen hemostatic function preoperatively, the question : “Preoperative hemostatic evaluation, which tests, if any” was easy to answer : “do not bother with these insensitive tests, rely on the patient’s history”

4
A simple screening questionnaire
have you ever bled for a long time or developed a swollen tongue or mouth after cutting or biting your tongue, cheek or lip ? do you develop bruises larger than “a silver dollar” without being able to remember when or how you injured yourself ? If so, how big was the largest of these bruises ?

5
A simple screening questionnaire (2)
how many times have you had teeth pulled and what was the longest time that you bled after an extraction ? Has bleeding ever started up again the day after extraction ? what operations have you had, including minor surgery such as skin biopsies ? Was bleeding after surgery ever hard to stop ? Have you ever developed unusual bruising in the skin around an area of surgery or injury ?

6
A simple screening questionnaire (3)
have you had a medical problem within the past 5 yr requiring a doctor’s care ? If so, what was its nature ? what medications including aspirin or any other remedies for headaches, cold, menstrual cramps or other pains have you taken within the past 7-9 days ? has any blood relative had a problem with unusual bruising or bleeding after surgery ? Were blood transfusions required to control this bleeding ? Samuel I Rapaport, Blood, 1983

7
Tests in addition to the history ?
patients may protect against the doctor who fails to take an adequate history some patients give an unreliable history i.e mild bleeding disorders... but excessive abnormality that causes bleeding only after surgery and no surgery or dental extractions before (factor XI deficiency, Willebrand) acquired hemostatic defects (thrombocytopenia)
 acquired hemostatic defects (thrombocytopenia)")
9
Bilan pré-op : la première étude Eika, Scand J Haematol 1978
101 patients, 3 groupes, hémostase pré-opératoire (2 hematologues) pas de risque hémorragique risque hémorragique modéré risque hémorragique élevé saignement intra et post-opératoire, 3 groupes (chirurgien + anesthésiste) saignement habituel ou pas de saignement majoration du saignement hémorragie majeure pre-op vs post-op : pas de corrélation
 pas de risque hémorragique. risque hémorragique modéré. risque hémorragique élevé. saignement intra et post-opératoire, 3 groupes (chirurgien + anesthésiste) saignement habituel ou pas de saignement. majoration du saignement. hémorragie majeure. pre-op vs post-op : pas de corrélation.")
10
TCA + TQ ?? Eisenberg & Coll, Arch.Surg, 1982
480 patients modifications sans anomlie retrouvée à l'interrogatoire ou à l'examen, soit 2,7% 4 allongements non confirmés 9 confirmés opérés : - 8 sans problémes hémorragiques - 1 hémorragie post-op origine mécanique nécessitant réintervention ; TCA normalisé Inutilité du T.Q Faible valeur du T.C.A : 1/480

11
Usual preoperative screening Janvier, Anesthesiology, 1991
prospective study patients screening history, physical examination platelet count, BT, PT, APTT, fibrinogen one prolonged PT and 19 prolonged APTT (0.48%) and only 8 potential bleeding risks : 3 factor XI deficiencies, 1 anti VII , 4 Willebrand diseases 3 positive screening stories /8 usefulness of the screening: 5/4141 (0.12%)
 and only 8 potential bleeding risks : 3 factor XI deficiencies, 1 anti VII , 4 Willebrand diseases. 3 positive screening stories /8. usefulness of the screening: 5/4141 (0.12%)")
14
Leroux et al, Pediatric Anesthesia 2002; 12:118-23
Period 1 (24-months, retrospective study, n = 751): Haemostasis screening undertaken only after family and personal history and physical examination in all patients Period 2 (following 24 months, prospective study, n = 958): Standardized questionnaire. Routine tests (PT, APTT, platelet count) in children who where not yet walking In older children, coagulation tests undertaken as in period 1
: Haemostasis screening undertaken only after family and. personal history and physical examination in all patients. Period 2 (following 24 months, prospective study, n = 958): Standardized questionnaire. Routine tests (PT, APTT, platelet count) in children who where not. yet walking. In older children, coagulation tests undertaken as in period 1.")
15
Leroux et al, Pediatric Anesthesia 2002; 12:118-23
26 significant abnormalities / 1709 children Coagulation tests in 16.2% (period 1) and 78.2% (period 2) of the children, who were not yet walking Routine tests did not improve the diagnosis of haemostasis abnormalities(2.2% from 406 children in period 1 vs 4.1% from 266 children in period 2) Predictive positive value of routine tests (period 2) was 19%, vs 45% for specific tests (period 1) (P < 0.001)
 and 78.2% (period 2) of the children, who were not yet walking. Routine tests did not improve the diagnosis of haemostasis. abnormalities(2.2% from 406 children in period 1 vs 4.1% from. 266 children in period 2) Predictive positive value of routine tests (period 2) was. 19%, vs 45% for specific tests (period 1) (P < 0.001)")
16
When routine testing is performed in nonwalking children,
the screening number increases without leading to a higher number of anaesthetic management changes, suggesting that routine testing does not seem to provide much extra information in the absence of a positive history.

17
Three levels level I : screening history negative, minor surgery no screening tests are recommended

18
Three levels level II : patients whose screening bleeding history raises a possibility of defective hemostasis, patients in whom the procedure may impair hemostasis e.g. cardiac surgery, prostatectomy, patients undergoing procedures in which even minimal postoperative bleeding could be hazardous e.g. neurosurgery : platelet count, (BT or PFA 100), PT, APTT …
, PT, APTT …")
19
Three levels level III : the screening bleeding history leaves one very suspicious or certain of a hemostatic abnormality; the surgery may be minor or minor : specific tests in close collaboration with the hemostasis laboratory

20
Interrogatoire positif = 1 réponse A ou 2 réponses B
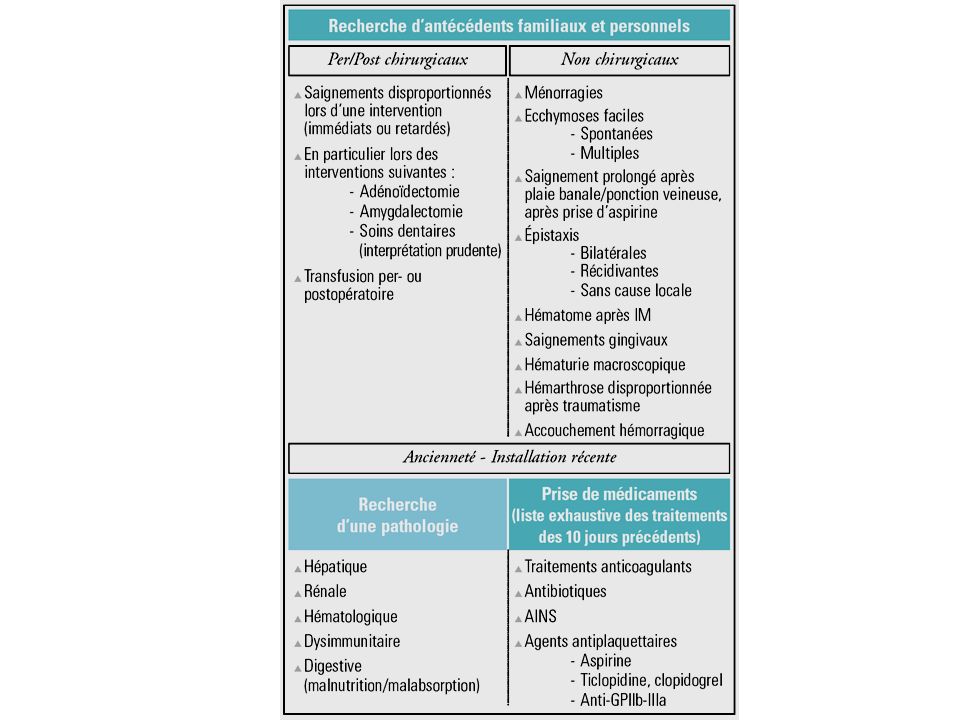
Type A 1- saignement >24H ou transfusion après chirurgie mineure 2- saignement prolongé ou reprise 24H après soins (chir) dentaires 3- aspirine ou AINS < 15 j 4- examen = ecchymoses pétéchies, purpura, malnutrition, exogénose Type B 5 - ATCD familiaux de type A 6- Hématomes spontanés 7- Epistaxis nécessitant contrôle chirurgical 8- saignement > 15 min après ponction veineuse 9- tendance au saignement
 dentaires. 3- aspirine ou AINS < 15 j. 4- examen = ecchymoses pétéchies, purpura, malnutrition, exogénose. Type B. 5 - ATCD familiaux de type A. 6- Hématomes spontanés. 7- Epistaxis nécessitant contrôle chirurgical. 8- saignement > 15 min après ponction veineuse. 9- tendance au saignement.")
23
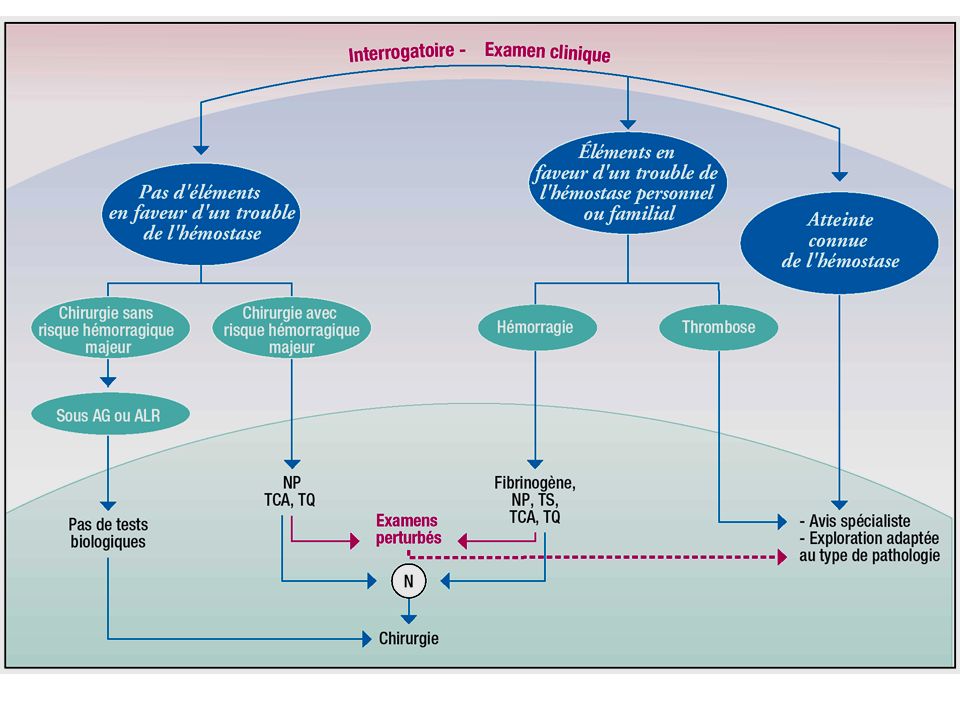
Recommandations ANAES
Interrogatoire positif Enfant avant l ’âge de la marche Interrogatoire impossible Pathologie de la grossesse Pathologies associées à un trouble d ’hémostase Avant chirurgie hémorragique ? Plaquettes, TCA, TP, (Fibrinogène)
")
24
Recos concernant la période préanesthésique SFAR 1991
En fonction des données de l'interrogatoire et de l'examen physique, de l'acte et de l'anesthésie envisagés, ainsi que du degré d'urgence, d'éventuels examens complémentaires sont effectués. Aucune donnée scientifique ou norme réglementaire n'impose la pratique systématique d'examens complémentaires. Seuls, ceux motivés par les données de l'interrogatoire, de l'examen, de l'acte et de l'anesthésie envisagés sont indispensables. Le cas échéant, une consultation spécialisée est demandée.

25
Bilan d ’hémostase chez l ’enfant : Quelles recommandations ?
1992 ANDEM : • clinique et/ou interrogatoire risque hémorragique ? • avant la marche 1993 GEHT : si acte vulnérant TQ, TCA, plaquettes, TS? 1995 American Academy of Otolaryngology. Head and Neck Surgery : étude sélective, si « histoire suggestive » ou si information génétique indisponible 1998 ANAES : inutile si absence d ’antécédents particuliers, sauf si : Enfant avant l ’âge de la marche devant subir un acte de chirurgie majeure Risque chirurgical et enfant jamais opéré Chirurgie ambulatoire exsangue Examens jugés les plus utiles : TCA et numération plaquettaire

27
IIa macrophage or monocyte platelet activated platelet II X TF VIIa Xa
VIII/vWF VIIIa + free vWF TF VIIa Xa V Va IIa macrophage or monocyte Va XI IX VIIa TF XIa platelet IXa X II IIa VIIIa Xa IXa Va XIa activated platelet IX

29
Initiation and First Generation of Thrombin
II X stimulus VII VIIa Xa TF IIa Cell with TF IX VIIa TF IXa

30
Initiation Phase Thrombin IIa (nM) time (min) 20 40 60 80 100 120 140
20 40 60 80 100 120 140 5 10 15 Thrombin IIa (nM) 20 25 30 35 40 45 50 time (min)
 time (min)")
31
Initiation and Amplification
II X VIIIa stimulus VII VIIa Xa Va TF IIa Cell with TF XIa IX VIIa TF IXa platelet Activated platelet

32
Multicellular Model of Coagulation
IXa Xa TF IX X Xa IXa X II IIa CELL WITH TF PLATELET VIIIa Blood Reviews 2003;17:S1-S5

33
Hartwig, Thromb Haemost 1999; 82: 392-398

35
Amplification Phase thrombin IIa (nM) time (min) 20 40 60 80 100 120
20 40 60 80 100 120 140 5 10 15 thrombin IIa (nM) 20 25 30 35 40 45 50 time (min)
 time (min)")
36
Amplification Burst of Thrombin
II X VIIIa VIIa Xa Va TF IIa Cell with TF XIa IX VIIa TF IXa II X Platelet IIa VIIIa Xa XIa IXa Va IX Activated platelet

37
Burst of Thrombin (Propagation Phase)
20 40 60 80 100 120 140 5 10 15 thrombin IIa (nM) 20 25 30 35 40 45 50 time (min)
 time (min)")
38
IIa macrophage or monocyte platelet activated platelet II X TF VIIa Xa
VIII/vWF VIIIa + free vWF TF VIIa Xa V Va IIa macrophage or monocyte Va XI IX VIIa TF XIa platelet IXa X II IIa VIIIa Xa IXa Va XIa activated platelet IX Roberts, Haemophilia 1998

39
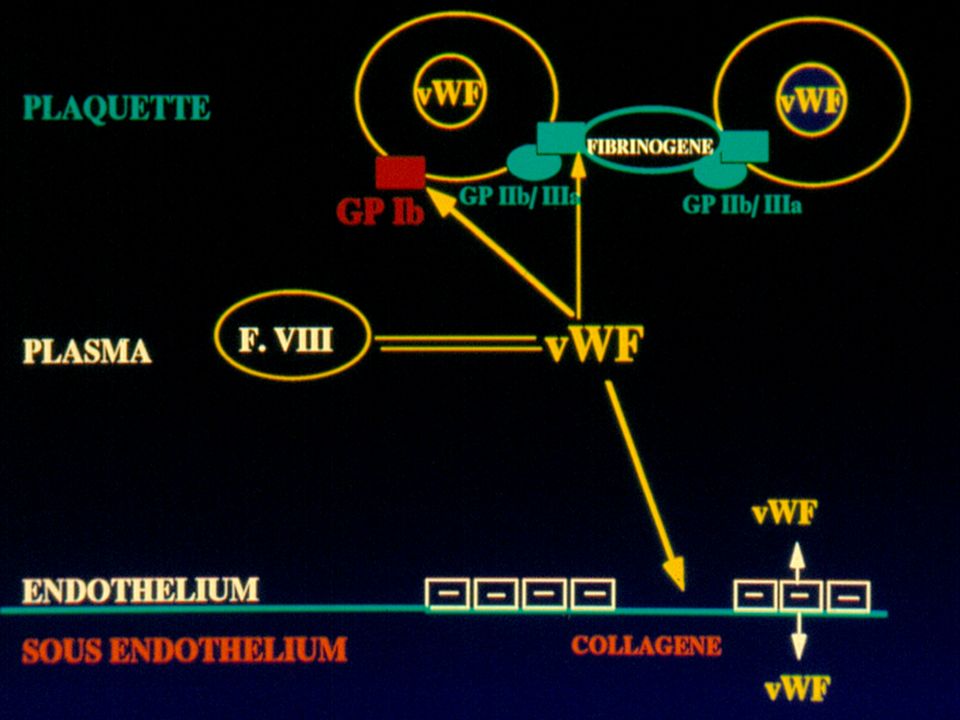
Temps de céphaline + activateur (TCA) Maladie de Willebrand
 Maladie de Willebrand")
40
TCA TP

41
Allongement du TCA Définir un pourcentage du temps du témoin et non un nombre de secondes Anomalie à partir de % Exemple : TCA témoin 30 sec, malade 36 sec ==> allongement de 6 sec soit 20 %

42
TCA allongé : Risque hémorragique ou thrombotique ?

43
Allongement isolé du TCA
Toujours raisonner en fonction de la clinique (interrogatoire +++ traitement) puis rechercher un déficit ou un inhibiteur
 puis. rechercher un déficit ou un inhibiteur.")
44
Recherche d'un anticoagulant circulant
TCA avec plasma du malade + plasma du témoin Allongement non corrigé par le témoin : inhibiteur Correction par le plasma du témoin : déficit

45
Allongement isolé du TCA : Mélange du plasma du malade avec un plasma témoin
Non correction de l'allongement = présence d'un inhibiteur Anticoagulant circulant - antiphospholipide - anti cardiolipine Anticorps antifacteur de la voie endogène (anti VIII, anti IX) risque thrombotique risque hémorragique
 risque thrombotique. risque hémorragique.")
46
Allongement TCA isolé : mélange du plasma du malade avec un plasma témoin
Correction de l'allongement = présence d'un déficit => Dosage cofacteurs XII : allongement important du TCA, courant XI : ATCD hémorragiques ou nuls Fréquent chez les patients septiques pas de risque hémorragique risque hémorragique variable

47
Allongement TCA isolé : Mélange du plasma du malade avec un plasma témoin
Correction de l'allongement = présence d'un déficit => dosages cofacteurs et vWF - hémophilie : histoire hémorragique, sexe masculin F VIII:C ou IX - Willebrand : histoire hémorragique non constante, allongement du TS, vWF Ag diminué, vWF : RCo diminué VIII variable, généralement diminué

48
Pourquoi les hémophiles saignent ils ?
Retard dans la formation du caillot hémostatique Caillot mécaniquement fragile, prématurément détruit thrombine/ antithrombine (nM) 800 700 600 500 400 300 200 100 12 11 1 2 3 4 5 6 7 8 9 10 minutes initiation propagation coagulation sang normal FT pM stabilisation hémophile
 minutes. initiation. propagation. coagulation. sang normal. FT pM. stabilisation. hémophile.")
49
macrophage or monocyte platelet activated platelet II X TF VIIa Xa Va
XI IX VIIa TF XIa platelet IXa II IXa Va XIa activated platelet IX Roberts, Haemophilia 1998

50
IIa macrophage or monocyte platelet activated platelet II X TF VIIa Xa
VIII/vWF VIIIa + free vWF TF VIIa Xa V Va IIa macrophage or monocyte Va XI IX VIIa TF XIa platelet IXa X II IIa VIIIa Xa IXa Va XIa activated platelet IX Roberts, Haemophilia 1998

51
Maladie de Willebrand autosomale, généralement dominante
la plus fréquente des anomalies constitutionnelles de l’hémostase : 1% formes sévères rares : 0,5 à 5,3 par million anomalie quantitative ou qualitative du facteur Willebrand

53
Déficit en F. Willebrand
Prévalence estimée Population générale (type 1++, AD) 1/100 Cas avec risque hémorragique 100/106 (23-113/106) type 1, quantitatif modéré 70-80% plasmatique et plaquettaire type 2, qualitatif 20-30% 2A, 2B, 2M, 2N type 3, quantitatif sévère 3-5/106 plaquettaire et plasmatique Rodeghiero, Haemophilia, 2002, 8, : « vWD : still an intriguing disorder in the era of molecular medicine »
 1/100. Cas avec risque hémorragique. 100/106. (23-113/106) type 1, quantitatif. modéré % plasmatique et plaquettaire. type 2, qualitatif % 2A, 2B, 2M, 2N. type 3, quantitatif. sévère. 3-5/106. plaquettaire et plasmatique. Rodeghiero, Haemophilia, 2002, 8, : « vWD : still an intriguing disorder in the era of molecular medicine »")
54
Maladie de Willebrand : clinique
hétérogène dans son expression clinique, phénotypique et génotypique hémorragies muqueuses : épistaxis, gingivorragies, hémorragies gastro-intestinales, ménorragies hémorragies cutanées : ecchymoses pour des traumatismes minimes hématomes profonds et hémarthroses rares

55
Maladie de Willebrand : diagnostic
histoire hémorragique (inconstante) allongement du TS allongement du PFA allongement du TCA (inconstante) diminution du taux de facteur VIII (++) diminution du taux de vWFR-Co(activité) et vWFAg
 allongement du TS. allongement du PFA. allongement du TCA (inconstante) diminution du taux de facteur VIII (++) diminution du taux de vWFR-Co(activité) et vWFAg.")
56
Maladie de Willebrand :
Diagnostic difficile des formes frustes (patients de groupe O) Savoir reconnaître un variant de maladie de Willebrand Hémorragies importantes TS / PFA ì vWFRCo < vWFAg F VIII ¯ Caractérisation dans des laboratoires spécialisés Pq TS/PFA FVIII vWFAg vWFRCo Agrég.Risto DDAVP N N/ N/ N N/ – N/ – N N N N N – N – Type 1 Type 2A B N Type 3
 Savoir reconnaître un variant de maladie de Willebrand. Hémorragies importantes. TS / PFA ì. vWFRCo < vWFAg. F VIII ¯ Caractérisation dans des laboratoires spécialisés. Pq TS/PFA FVIII vWFAg vWFRCo Agrég.Risto DDAVP. N N/ N/ + N N/ – N/ – N N N N N – N – Type 1. Type 2A. B. N. Type 3.")
57
- maladie de Willebrand taux de FVIII:C <20% ou >20% DDAVP +
Test préalable de réponse au DDAVP - Traitement préventif des hémorragies (intervention chirurgicale, trauma sévère) Traitement curatif des hémorragies ou chirurgie d’urgence ou trauma sévère) taux de FVIII:C <20% ou >20%
 Traitement curatif des. hémorragies. ou chirurgie d’urgence. ou trauma sévère) taux de FVIII:C <20% ou >20%")
58
Première injection de facteur Willebrand
préventif curatif taux de FVIII:C < 20% taux de FVIII:C > 20% taux de FVIII:C < 20% taux de FVIII:C > 20% Première injection de facteur Willebrand 50 UI/kg 30 min avant l’intervention 50 UI/kg 30 min avant l’intervention 50 UI/kg vWF + Facteur VIII (30-40 UI/kg) ou Willstart (50 UI/kg) 50 UI/kg vWF + Facteur VIII (30-40 UI/kg) ou Willstart (50 UI/kg) Intervention programmée : 50 UI/kg de vWF 12 à 24h avant, à renouveler 1h avant
 ou. Willstart. (50 UI/kg) 50 UI/kg vWF. + Facteur VIII. (30-40 UI/kg) ou. Willstart. (50 UI/kg) Intervention programmée : 50 UI/kg de vWF 12 à 24h avant, à renouveler 1h avant.")
59
facteur Willebrand - injections suivantes
objectif : maintien du vWF:RCo à 60% et du VIII:C à 40% facteur Willebrand : UI/kg toutes les 12/24h pendant un à plusieurs jours selon la gravité de l’état clinique et biologique du patient

60
Mannucci P, Thromb Haemost 2001; 86: 149-53

61
Mannucci P, Thromb Haemost 2001; 86: 149-53

62
Willebrand : en pratique
vWF type I : DDAVP et surveillance du VIII si > 20% , ne rien faire de plus si < 20% Willstart® (vWF + FVIII) - rarement nécessaire) péridurale obstétricale : fonction du type de vWF type II ou III : NON type I : OUI si vWF > 50%
 - rarement nécessaire) péridurale obstétricale : fonction du type de vWF. type II ou III : NON. type I : OUI si vWF > 50%")
63
Réfléchir et ne rien faire dans la précipitation…

Présentations similaires




![[number 1-100] There is no rule to the way to remember the names for the numbers 1 to 10 in French so we recommend that you simply practice!](/1/172873/big_thumb.jpg "[number 1-100] There is no rule to the way to remember the names for the numbers 1 to 10 in French so we recommend that you simply practice!>")















