Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Hépatites chroniques B et C: épidémiologie et traitement
Vendredi 13 novembre Hépatites chroniques B et C: épidémiologie et traitement Dr Karine Lacombe SMIT, Hôpital Saint-Antoine, AP-HP, France. UPMC, Paris VI Inserm UMR-S707

2
Plan du cours Hépatite chronique C Hépatite chronique B
Épidémiologie Traitement Hépatite chronique B Particularités des co-infections VIH-hépatites

3
Hépatite C chronique

4
Propriétés virologiques
Classification taxonomique famille des Flaviviridae, genre Hepacivirus (seul membre connu aujourd’hui) Structure des virions diamètre de 55 à 65 nm. Constituées de trois structures (ext. vers int.) enveloppe lipidique (avec 2 glycoprotéines E1 et E2) capside protéique (polymérisation de la protéine de capside C) génome viral (constitué d'une molécule d'ARN simple brin)
 Structure des virions. diamètre de 55 à 65 nm. Constituées de trois structures (ext. vers int.) enveloppe lipidique (avec 2 glycoprotéines E1 et E2) capside protéique (polymérisation de la protéine de capside C) génome viral (constitué d une molécule d ARN simple brin)")
5
Les génotypes du VHC- définition
Groupes phylogéniques résultant de l’évolution darwinienne du virus au cours des âges. Ils regroupent l’ensemble des types et sous-types isolés dans le monde 6 principaux types numérotés de 1 à 6 Différence entres les types : 31 à 34% de la séquence nucléotidique et environ 30% de la séquence amino-acidique Une centaine de sous-types Identifiés par une lettre minuscule après le chiffre (ex : 1a…) Différence entre les sous-types : 20 à 23 % de la séquence nucléotidique
 Différence entre les sous-types : 20 à 23 % de la séquence nucléotidique.")
6
Génotypes: distribution mondiale
Afrique de l’ouest : types 1 et 2 Grande diversité des sous-types Existence de sous-types non retrouvés ailleurs Asie du sud-est, Indonésie : type 1 prédominant Mais nombreux sous-types du type 3 Types intermédiaires (3 à 6) également rencontrés (génotype 6a: essentiellement présent à Hong-Kong) Egypte et Afrique centrale : 4a Afrique du sud : 5a En Afrique de l’Ouest, les types 1 et 2 sont prédominants et caractérisés par une grande diversité de leurs sous-types, dont la majorité ne sont rencontrés dans aucune autre région du monde (20-22). De très nombreux sous-types du type 3 sont rencontrés en Asie du Sud-Est et en Indonésie, mais le type 1 y reste prédominant. Les types intermédiaires, classés au sein des types 3 et 6, sont également rencontrés dans ces régions (23-25). Le génotype 4a prédomine en Egypte et en Afrique centrale, tandis que le génotype 5a est trouvé exclusivement en Afrique du Sud (26, 27). Le génotype 6a est présent essentiellement à Hong Kong et dans les régions avoisinantes de Chine continentale (28-30). Dans les pays industrialisés, les génotypes les plus prévalents sont les sous-types 1a, 1b, 2a, 2b, 2c, 3a et 4a (18, 31-35). En Europe de l’Ouest, et plus particulièrement en France, le génotype 1 (sous-types 1a et 1b) est responsable de 60 à 65 % des infections, tandis qu’environ 20 % des malades sont infectés par le génotype 3a. Les autres génotypes (2a, 2c et 4a) sont responsables des cas restants (18, 31, 32). Avant l’identification du VHC et l’utilisation de tests sérologiques pour la qualification des dons de sang, le génotype 1b a été principalement transmis par la transfusion sanguine, alors que les génotypes 1a et 3a ont largement diffusé chez les usagers de drogues par voie veineuse (18). Au cours des 10 dernières années, la proportion de génotypes 1a et 3a a augmenté par rapport au génotype 1b (Figure 2), car l’usage de drogues par voie veineuse est aujourd’hui la première cause de transmission du VHC, responsable d’environ 70 % des nouveaux cas (31). La prévalence du génotype 4a s’accroît également au sein de la population des usagers de drogues.
 également rencontrés. (génotype 6a: essentiellement présent à Hong-Kong) Egypte et Afrique centrale : 4a. Afrique du sud : 5a. En Afrique de l’Ouest, les types 1 et 2 sont prédominants et caractérisés par une grande diversité de leurs sous-types, dont la majorité ne sont rencontrés dans aucune autre région du monde (20-22). De très nombreux sous-types du type 3 sont rencontrés en Asie du Sud-Est et en Indonésie, mais le type 1 y reste prédominant. Les types intermédiaires, classés au sein des types 3 et 6, sont également rencontrés dans ces régions (23-25). Le génotype 4a prédomine en Egypte et en Afrique centrale, tandis que le génotype 5a est trouvé exclusivement en Afrique du Sud (26, 27). Le génotype 6a est présent essentiellement à Hong Kong et dans les régions avoisinantes de Chine continentale (28-30). Dans les pays industrialisés, les génotypes les plus prévalents sont les sous-types 1a, 1b, 2a, 2b, 2c, 3a et 4a (18, 31-35). En Europe de l’Ouest, et plus particulièrement en France, le génotype 1 (sous-types 1a et 1b) est responsable de 60 à 65 % des infections, tandis qu’environ 20 % des malades sont infectés par le génotype 3a. Les autres génotypes (2a, 2c et 4a) sont responsables des cas restants (18, 31, 32). Avant l’identification du VHC et l’utilisation de tests sérologiques pour la qualification des dons de sang, le génotype 1b a été principalement transmis par la transfusion sanguine, alors que les génotypes 1a et 3a ont largement diffusé chez les usagers de drogues par voie veineuse (18). Au cours des 10 dernières années, la proportion de génotypes 1a et 3a a augmenté par rapport au génotype 1b (Figure 2), car l’usage de drogues par voie veineuse est aujourd’hui la première cause de transmission du VHC, responsable d’environ 70 % des nouveaux cas (31). La prévalence du génotype 4a s’accroît également au sein de la population des usagers de drogues.")
7
Génotypes: distribution mondiale
Pays industrialisés : 1a, 1b, 2a, 2b, 2c, 3a et 4a France : type 1 (60 à 65% des contaminations) Sous-type 1a (usage de drogue IV) et 1b (transfusions sanguines) 3a : 20% des malades (usage de drogue IV) Dans les pays industrialisés, les génotypes les plus prévalents sont les sous-types 1a, 1b, 2a, 2b, 2c, 3a et 4a (18, 31-35). En Europe de l’Ouest, et plus particulièrement en France, le génotype 1 (sous-types 1a et 1b) est responsable de 60 à 65 % des infections, tandis qu’environ 20 % des malades sont infectés par le génotype 3a. Les autres génotypes (2a, 2c et 4a) sont responsables des cas restants (18, 31, 32). Avant l’identification du VHC et l’utilisation de tests sérologiques pour la qualification des dons de sang, le génotype 1b a été principalement transmis par la transfusion sanguine, alors que les génotypes 1a et 3a ont largement diffusé chez les usagers de drogues par voie veineuse (18). Au cours des 10 dernières années, la proportion de génotypes 1a et 3a a augmenté par rapport au génotype 1b (Figure 2), car l’usage de drogues par voie veineuse est aujourd’hui la première cause de transmission du VHC, responsable d’environ 70 % des nouveaux cas (31). La prévalence du génotype 4a s’accroît également au sein de la population des usagers de drogues.
 Sous-type 1a (usage de drogue IV) et 1b (transfusions sanguines) 3a : 20% des malades (usage de drogue IV) Dans les pays industrialisés, les génotypes les plus prévalents sont les sous-types 1a, 1b, 2a, 2b, 2c, 3a et 4a (18, 31-35). En Europe de l’Ouest, et plus particulièrement en France, le génotype 1 (sous-types 1a et 1b) est responsable de 60 à 65 % des infections, tandis qu’environ 20 % des malades sont infectés par le génotype 3a. Les autres génotypes (2a, 2c et 4a) sont responsables des cas restants (18, 31, 32). Avant l’identification du VHC et l’utilisation de tests sérologiques pour la qualification des dons de sang, le génotype 1b a été principalement transmis par la transfusion sanguine, alors que les génotypes 1a et 3a ont largement diffusé chez les usagers de drogues par voie veineuse (18). Au cours des 10 dernières années, la proportion de génotypes 1a et 3a a augmenté par rapport au génotype 1b (Figure 2), car l’usage de drogues par voie veineuse est aujourd’hui la première cause de transmission du VHC, responsable d’environ 70 % des nouveaux cas (31). La prévalence du génotype 4a s’accroît également au sein de la population des usagers de drogues.")
8
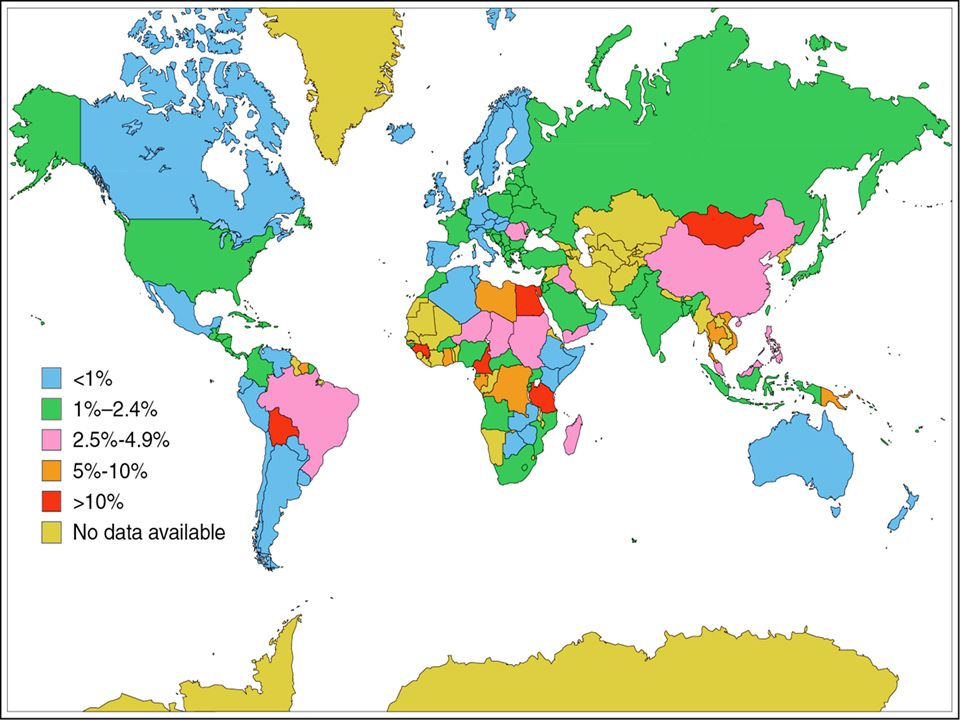
Prévalence mondiale de l’infection par le VHC
Environ 3% de la population mondiale 170 millions d’individus Variations géographiques (gradient Nord/Sud) : - 0,5 % Pays du Nord - 1,8 % USA - 2,0 % Pays méditerranéens - 15,0 % Égypte 1- Di Bisceglie AM: Hepatitis C. Lancet 1998;351: 2- Alter MJ: Epidemiology of hepatitis C. Hepatology 1997;26:62S-65S. 3- Roudot-Thoraval F: Épidémiologie de l’hépatite C. Médecine/Sciences 2002;18:
 : - 0,5 % Pays du Nord. - 1,8 % USA. - 2,0 % Pays méditerranéens. - 15,0 % Égypte. 1- Di Bisceglie AM: Hepatitis C. Lancet 1998;351: Alter MJ: Epidemiology of hepatitis C. Hepatology 1997;26:62S-65S. 3- Roudot-Thoraval F: Épidémiologie de l’hépatite C. Médecine/Sciences 2002;18:")
10
Estimations de la prévalence de l’infection par le VHC en France (InVS – CPAM 2005)
Séro-prévalence 0.86 % [0.66 – 1.10] de la population, soit à personnes dont 80% virémiques (ARN-VHC +). Variation selon facteurs socio-démographiques : - sexe : H=0.73% F=0.99% - précarité : CMU=2.65% - pays de naissance : M. Orient=11.28% Variation selon situations à risque : - UDIV : 55.48% - drogue voie nasale : 8.93% - transfusion < 1992 : 3.60% - tatouage : 2.23% - piercing : 1.66%
. Variation selon facteurs socio-démographiques : - sexe : H=0.73% F=0.99% - précarité : CMU=2.65% - pays de naissance : M. Orient=11.28% Variation selon situations à risque : - UDIV : 55.48% - drogue voie nasale : 8.93% - transfusion < 1992 : 3.60% - tatouage : 2.23% - piercing : 1.66%")
11
Histoire naturelle de l’infection par le VHC
Contamination VHC (n=1000) Clairance « spontanée » (n= ) ALAT normales (n= ) 0-5% Cirrhose (n=40-260) Hépatite chronique (n= ) Hépatite minime (n=90-360) 0-5% 10-30% Hépatite modérée/sévère (n= ) 1-3% par an 4% par an Décès par maladie hépatique après 5 ans (n= 0-40) à 5 ans 1-17% CHC après 5 ans (n= 2-40) Complications sévères après 5 ans (n=8-100) 1- de Lédinghen V: Histoire naturelle de l’infection par le virus de l’hépatite C. Gastroenterol Clin Biol 2002;26:B9-B22.
 Clairance « spontanée » (n= ) ALAT normales. (n= ) 0-5% Cirrhose. (n=40-260) Hépatite chronique. (n= ) Hépatite minime. (n=90-360) 0-5% 10-30% Hépatite modérée/sévère. (n= ) 1-3% par an. 4% par an. Décès par maladie hépatique après 5 ans. (n= 0-40) à 5 ans 1-17% CHC après 5 ans. (n= 2-40) Complications sévères après 5 ans. (n=8-100) 1- de Lédinghen V: Histoire naturelle de l’infection par le virus de l’hépatite C. Gastroenterol Clin Biol 2002;26:B9-B22.")
12
Répartition par modalités de découverte des patients nouvellement pris en charge pour hépatite C en France en 2001 Autre circonstance de découverte Démarche diagnostique Fortuite (bilan de santé, don de sang, bilan pré-transfusionnel) (anomalie des tests hépatiques, complication de cirrhose, bilan d’un carcinome hépato-cellulaire) (dont asthénie) Facteur de risque 16,5% 41,1% 17,6% 24,8% 11- BEH 16-17/2003
 (anomalie des tests hépatiques, complication de cirrhose, bilan d’un carcinome hépato-cellulaire) (dont asthénie) Facteur de risque. 16,5% 41,1% 17,6% 24,8% 11- BEH 16-17/2003.")
13
Facteurs de contamination suspectés chez les patients nouvellement pris en charge pour hépatite C en France en 2001 : Facteurs de risque suspectés Femmes (n=1699) Hommes (n=2204) n (%) Transfusion avant 1991 634 (38.8) 502 (23.7) Utilisation de drogue voie IV 340 (21.0) 1003 (47.4) Utilisation de drogue voie nasale 94 (6.2) 306 (15.7) Exposition professionnelle* 84 (5.5) 42 (2.1) Exposition nosocomiale** 357 (22.6) 323 (15.8) Autre facteur*** 257 (15.7) 364 (17.1) Aucun facteur retrouvé 245 (14.7) 280 (13.0) * médical et paramédical n=145 **dialyse, chirurgies, endoscopies ***acupuncture, injections diverses, piercing, conjoint VHC positif 11- BEH 16-17/2003
 Hommes (n=2204) n (%) Transfusion avant (38.8) 502 (23.7) Utilisation de drogue voie IV. 340 (21.0) 1003 (47.4) Utilisation de drogue voie nasale. 94 (6.2) 306 (15.7) Exposition professionnelle* 84 (5.5) 42 (2.1) Exposition nosocomiale** 357 (22.6) 323 (15.8) Autre facteur*** 257 (15.7) 364 (17.1) Aucun facteur retrouvé. 245 (14.7) 280 (13.0) * médical et paramédical n=145. **dialyse, chirurgies, endoscopies. ***acupuncture, injections diverses, piercing, conjoint VHC positif. 11- BEH 16-17/2003.")
14
Incidence de l’infection à VHC (USA), Effets dans le temps du dépistage chez les donneurs de sang 95 2 4 6 8 10 12 14 16 18 84 85 86 87 88 89 90 91 92 93 94 nb cas/ années Tests indirects (ALAT, Ag HBc) Ac anti-VHC 1ère génération 2ème génération 3- Alter MJ: Epidemiology of hepatitis C. Hepatology 1997 ; 26 : 62S-65S.
 Ac anti-VHC. 1ère génération. 2ème génération. 3- Alter MJ: Epidemiology of hepatitis C. Hepatology 1997 ; 26 : 62S-65S.")
15
Conclusions L’infection par le VHC touche quelques 170 millions d’individus dans le monde et plus d’un demi-million en France. Prédominante par le passé, la source transfusionnelle est actuellement supplantée quantitativement par la toxicomanie IV. La régression de l’endémie passe à la fois par le dépistage des sujets potentiellement infectés et par des mesures de prévention en direction des populations les plus à risque de nouvelles infections, notamment les usagers de drogues.

16
Objectifs du traitement
Primaire Eradiquer le virus Secondaires Prévenir la progression vers la cirrhose Reduire l’incidence du CHC Réduire le besoin d’une transplantation Améliorer la survie Chronic infection with hepatitis C virus (HCV) can lead to cirrhosis, liver cancer, and liver failure. However, unlike HIV or hepatitis B, hepatitis C is a disease that is curable in many cases. The primary goal of HCV treatment is to rid the body of HCV. The ultimate goals of treatment of chronic hepatitis C are to prevent progression to cirrhosis, delay or prevent the development of complications of cirrhosis, such as hepatocellular carcinoma, reduce the need for liver transplantation, and, ultimately, extend survival. Antiviral therapy favorably impacts the natural history of the disease. Achieving and maintaining no detectable virus in the serum has been associated with improvements in the condition of the liver, a decreased risk of progression to cirrhosis, and a decreased risk of negative clinical outcomes. In addition, it has been observed that, at least in some patients, treatment may significantly reduce the rate of liver disease progression independent of achieving a sustained virologic response (SVR). Davis GL, et al. J Hepatol. 1995;22(suppl 1): Lindsay KL. Hepatology. 1997;26(suppl 1):71S-77S. 16
 can lead to cirrhosis, liver cancer, and liver failure. However, unlike HIV or hepatitis B, hepatitis C is a disease that is curable in many cases. The primary goal of HCV treatment is to rid the body of HCV. The ultimate goals of treatment of chronic hepatitis C are to prevent progression to cirrhosis, delay or prevent the development of complications of cirrhosis, such as hepatocellular carcinoma, reduce the need for liver transplantation, and, ultimately, extend survival. Antiviral therapy favorably impacts the natural history of the disease. Achieving and maintaining no detectable virus in the serum has been associated with improvements in the condition of the liver, a decreased risk of progression to cirrhosis, and a decreased risk of negative clinical outcomes. In addition, it has been observed that, at least in some patients, treatment may significantly reduce the rate of liver disease progression independent of achieving a sustained virologic response (SVR). Davis GL, et al. J Hepatol. 1995;22(suppl 1): Lindsay KL. Hepatology. 1997;26(suppl 1):71S-77S. 16.")
17
Traitements ayant une AMM dans le traitement de l’hépatite C
Bithérapie associant: Interferon alfa (injections sous-cutanées) Interferon alfa 2a\alfa 2b\consensus interferon alfa -1 Pegylated interferon alfa 2a\alfa 2b Ribavirine (comprimés) Currently, there are several therapies approved by the US Food and Drug Administration and European regulatory authorities for the treatment of hepatitis C. These include standard interferon alfa in the form of interferon alfa-2a, interferon alfa-2b, and consensus interferon. However, the majority of patients are treated with long-acting pegylated interferon (peginterferon). Pegylation reduces the clearance of interferon allowing for weekly dosing by subcutaneous injection. Two pegylated interferon alfa preparations are available: pegylated interferon alfa-2a administered at a fixed dose and pegylated interferon alfa-2b administered at a weight-based dose. Although these medications can be used alone, it is typically recommended to use them in conjunction with ribavirin tablets, as this has been associated with marked improvements in response rates. The current standard of care for patients with chronic HCV infection is a combination of pegylated interferon and ribavirin which has no clinically significant interactions with methadone and has been studied broadly in the IDU population. 17
 Interferon alfa 2a\alfa 2b\consensus interferon alfa -1. Pegylated interferon alfa 2a\alfa 2b. Ribavirine (comprimés) Currently, there are several therapies approved by the US Food and Drug Administration and European regulatory authorities for the treatment of hepatitis C. These include standard interferon alfa in the form of interferon alfa-2a, interferon alfa-2b, and consensus interferon. However, the majority of patients are treated with long-acting pegylated interferon (peginterferon). Pegylation reduces the clearance of interferon allowing for weekly dosing by subcutaneous injection. Two pegylated interferon alfa preparations are available: pegylated interferon alfa-2a administered at a fixed dose and pegylated interferon alfa-2b administered at a weight-based dose. Although these medications can be used alone, it is typically recommended to use them in conjunction with ribavirin tablets, as this has been associated with marked improvements in response rates. The current standard of care for patients with chronic HCV infection is a combination of pegylated interferon and ribavirin which has no clinically significant interactions with methadone and has been studied broadly in the IDU population. 17.")
18
Mécanismes d’action des molécules
Interféron alfa Inhibe l’entrée du virus dans les cellules Inhibe la réplication virale Augmente l’activité des cellules T cytotoxiques Augmente l’activité des cellules NK Ribavirine Active contre les virus à ARN Pas d’activité antivirale en monothérapie mais diminue les ALAT Diminue le risque de rechute en fin de traitement en combinaison avec l’IFN Mécanisme précis d’action non connu Interferon alfa The mechanisms of action of interferon alfa and ribavirin are poorly defined. Interferons are a family of naturally occurring proteins produced and secreted by cells in response to viral infections. However, the exact way in which interferon works in hepatitis C is not fully understood. It is believed to have a wide range of biological effects that may include: inhibition of viral entry into cells, inhibition of viral replication, enhancement of cytotoxic T-cell activity, and stimulation of cytolytic T-cell activity. Importantly, since interferon alfa does not work directly on the virus, but rather via the host immune system, resistance to this drug has not been observed. Ribavirin Ribavirin is an oral guanosine analogue, which is active against many RNA viruses. Interestingly, ribavirin used alone does not exert any potent anti-HCV effect, but it is associated with improvement in serum alanine aminotransferase (ALT). The addition of ribavirin to interferon was a major breakthrough in the treatment of HCV as it nearly doubles the eradication rate of the virus, primarily by reducing the rate of virologic relapse after stopping treatment. Ribavirin’s mechanism of action is not well understood, although the most recent data suggest that it may increase the mutation rate of the HCV RNA and force it into error catastrophe. Further research is needed to better understand how this drug works. 18
. The addition of ribavirin to interferon was a major breakthrough in the treatment of HCV as it nearly doubles the eradication rate of the virus, primarily by reducing the rate of virologic relapse after stopping treatment. Ribavirin’s mechanism of action is not well understood, although the most recent data suggest that it may increase the mutation rate of the HCV RNA and force it into error catastrophe. Further research is needed to better understand how this drug works. 18.")
19
Advantages of Pegylated Interferon alfa
Polyethylene glycol (peg) is bound to interferon Delays clearance of interferon Maintains higher blood levels of interferon Once-weekly injection Avoids “peaks and troughs” of 3-times-weekly dosing Less fatigue and malaise No drug-drug interaction with methadone Pharmacokinetics Peg-IFN alfa-2a SC once weekly T1/2 80 hours 20,000 15,000 1000 Peg-IFN -2b SC once weekly T1/2 40 hours pg/mL Pegylation of interferon, which is the attachment of a small polyethylene glycol molecule to interferon alfa, has greatly improved the efficacy of interferon. The primary advantage of pegylation is that it reduces the clearance of the drug by the kidneys, resulting in higher blood concentrations. This in turn maintains antiviral pressure and increases clinical efficacy. As a result, pegylation allows for the convenience of once-weekly injections with fewer peaks and troughs in plasma concentrations than the 3-times-weekly injections of nonpegylated alfa interferon. Both peginterferon alfa-2a and peginterferon alfa-2b have improved pharmacokinetic profiles compared with conventional interferon alfa. The half-life of peginterferon alfa-2a is 80 hours, or twice that of peginterferon alfa-2b, which is 40 hours. However, peginterferon alfa-2b appears to be a more potent inhibitor of HCV replication in vitro. Both agents have been shown to have approximately twice the efficacy of standard interferon preparations in clinical trials and, when combined with ribavirin, similar efficacy in the treatment of chronic hepatitis C. Pegylation of interferon has also led to improvements in tolerability with less fatigue and malaise compared with standard interferon. Importantly for HCV-infected individuals who are drug users, a recent study has shown that there is no drug-drug interaction between methadone and pegylated interferon alfa-2a. 100 IFN TIW T1/ hours 10 1 10 20 40 60 80 100 120 140 160 180 Hours 19
 is bound to interferon. Delays clearance of interferon. Maintains higher blood levels of interferon. Once-weekly injection. Avoids peaks and troughs of 3-times-weekly dosing. Less fatigue and malaise. No drug-drug interaction with methadone. Pharmacokinetics. Peg-IFN alfa-2a. SC once weekly T1/2 80 hours. 20, , Peg-IFN -2b SC once weekly T1/2 40 hours. pg/mL. Pegylation of interferon, which is the attachment of a small polyethylene glycol molecule to interferon alfa, has greatly improved the efficacy of interferon. The primary advantage of pegylation is that it reduces the clearance of the drug by the kidneys, resulting in higher blood concentrations. This in turn maintains antiviral pressure and increases clinical efficacy. As a result, pegylation allows for the convenience of once-weekly injections with fewer peaks and troughs in plasma concentrations than the 3-times-weekly injections of nonpegylated alfa interferon. Both peginterferon alfa-2a and peginterferon alfa-2b have improved pharmacokinetic profiles compared with conventional interferon alfa. The half-life of peginterferon alfa-2a is 80 hours, or twice that of peginterferon alfa-2b, which is 40 hours. However, peginterferon alfa-2b appears to be a more potent inhibitor of HCV replication in vitro. Both agents have been shown to have approximately twice the efficacy of standard interferon preparations in clinical trials and, when combined with ribavirin, similar efficacy in the treatment of chronic hepatitis C. Pegylation of interferon has also led to improvements in tolerability with less fatigue and malaise compared with standard interferon. Importantly for HCV-infected individuals who are drug users, a recent study has shown that there is no drug-drug interaction between methadone and pegylated interferon alfa-2a IFN TIW. T1/2 2-3 hours Hours. 19.")
20
Recommandations de traitement
Stade F2 ou complications extra-hépatiques Peg-IFN + RBV plus efficace que IFN + RBV oupeg-IFN seul Génotype 1 Peg-IFN 180µg/j ou 1,5µg/kg/s + RBV mg/j → 48 semaines Génotype 2 or 3 Peg-IFN 180µg/j ou 1,5µg/kg/s + RBV mg/ mg/j → 24 semaines But du traitement = RVS Définie comme: PCR HCV indétectable 24 semaines après la fin du traitement PCR HCV quantitative avec seuil de sensibilité < 50 IU/mL In 2002, the NIH consensus panel recommended peginterferon alfa-2a or alfa-2b, each combined with ribavirin, as the standard care for the treatment of patients with HCV infection. It recommended that persons infected with HCV genotype 1 receive peginterferon alfa-2a 180 µg subcutaneously weekly or peginterferon alfa-2b 1.5 µg/kg weekly plus ribavirin dosed according to body weight at 1000 or 1200 mg/day, typically given orally twice daily. The duration of treatment for genotype 1 should be 48 weeks. Patients with genotypes 2 or 3, which are easier to treat, should receive the same dose of peginterferon, but only 800 mg/day of ribavirin, and 24 weeks of treatment appear sufficient in these patients. The goal of HCV treatment is an SVR, currently the best indicator of viral eradication. Sustained virologic response is defined as the absence of detectable HCV RNA in the serum 24 weeks after the end of HCV treatment using an assay with a lower limit of detection of 50 IU/mL or less. 20

21
Définitions virologiques de la réponse au traitement: marqueurs précoces
Non réponse Échec d’atteinte de l’indétectabilité durant tout le suivi sous traitement RVR HCV RNA indétetable à S4 RVP (EVR) ≥ 2 log10 baisse de l’HCV RNA à S12 Null Response Baisse HCV RNA < 2 log10 IU/mL à S12 Réponse viro partielle ≥ 2 log10 baisse de l’HCV RNA à S12, mais HCV RNA détectable à S24 Primarily, the response to therapy is defined by the decline of HCV viremia levels in persons starting therapy with peginterferon and ribavirin. A person who is nonresponsive to treatment is a person who fails to achieve an undetectable HCV RNA level at any time point during therapy. A rapid virologic response (RVR) is defined as the achievement of an undetectable HCV RNA level (ie, less than 50 IU/mL) by Week 4 of therapy. An early virologic response (EVR) is defined as greater than a 2 log10 reduction from baseline in HCV RNA by Week 12 or an undetectable HCV RNA level by Week 12. Week 12 is an important time point because individuals who have a null response (ie, who fail to achieve a 2 log10 reduction) by that time are highly unlikely to achieve an SVR to therapy. In these cases, current consensus guidelines recommend discontinuation of treatment. A partial virologic responder is a person who has achieved a 2 log10 reduction from baseline by Week 12 but continues to have detectable HCV RNA by Week 24. This person is also unlikely to achieve an SVR but does have more antiviral activity than a null responder. Pawlotsky JM. Hepatology. 2002;36(suppl 1):S65-S73. Sethi A, et al. Clin Liver Dis. 2005;9: 21
 ≥ 2 log10 baisse de l’HCV RNA à S12. Null Response. Baisse HCV RNA < 2 log10 IU/mL à S12. Réponse viro partielle. ≥ 2 log10 baisse de l’HCV RNA à S12, mais HCV RNA détectable à S24. Primarily, the response to therapy is defined by the decline of HCV viremia levels in persons starting therapy with peginterferon and ribavirin. A person who is nonresponsive to treatment is a person who fails to achieve an undetectable HCV RNA level at any time point during therapy. A rapid virologic response (RVR) is defined as the achievement of an undetectable HCV RNA level (ie, less than 50 IU/mL) by Week 4 of therapy. An early virologic response (EVR) is defined as greater than a 2 log10 reduction from baseline in HCV RNA by Week 12 or an undetectable HCV RNA level by Week 12. Week 12 is an important time point because individuals who have a null response (ie, who fail to achieve a 2 log10 reduction) by that time are highly unlikely to achieve an SVR to therapy. In these cases, current consensus guidelines recommend discontinuation of treatment. A partial virologic responder is a person who has achieved a 2 log10 reduction from baseline by Week 12 but continues to have detectable HCV RNA by Week 24. This person is also unlikely to achieve an SVR but does have more antiviral activity than a null responder. Pawlotsky JM. Hepatology. 2002;36(suppl 1):S65-S73. Sethi A, et al. Clin Liver Dis. 2005;9:")
22
Schéma de réponse 7 Nonresponder 6 Null responder 5
Peg-IFN + RBV 7 Nonresponder 6 Null responder 5 HCV RNA (log10 IU/mL) 2 log10 decline Partial responder 4 A graph showing the patterns of virologic response is extremely helpful when treating patients. Initiation of therapy results in a characteristic biphasic decline in viral load. The first phase of rapid decline in HCV RNA levels is due to interferon’s inhibition of the release of virions. The slower second phase decline appears to be related to the reduction in the rate of infection of new hepatocytes combined with an increased death rate of infected hepatocytes. A nonresponder will exhibit no decrease in viral load from baseline. A null responder will have a minimal drop in HCV RNA—for example, between 1-2 log10 IU/mL within 1 or 2 days but no further decrease thereafter. These individuals never achieve an undetectable viral load. Slow-partial responders are defined as having a rapid first-phase decline followed by a gradual second-phase decrease in viral levels. Finally, a rapid virologic responder will have rapid first- and second-slope viral declines with viral levels becoming undetectable soon after initiation of therapy (ie, by Week 4). Patients who achieve an RVR are more likely of achieving an SVR with standard duration of therapy, with a very low risk of virologic relapse. The goal of therapy is to achieve a rapid viral reduction. Hepatitis C virus viremia should be assessed at baseline, Week 4, Week 12, and Week 24 to assess virologic response. Individuals who fail to achieve a 2 log10 reduction from baseline at week 12 may discontinue therapy because they have a low likelihood of SVR. Individuals whose HCV RNA level remains detectable after 24 weeks of therapy may also stop therapy, as they are unlikely to respond. 3 Limit of detection 2 Rapid responder 1 1 2 3 7 14 21 28 84 (12 weeks) Days on Treatment 22
 2 log10 decline. Partial responder. 4. A graph showing the patterns of virologic response is extremely helpful when treating patients. Initiation of therapy results in a characteristic biphasic decline in viral load. The first phase of rapid decline in HCV RNA levels is due to interferon’s inhibition of the release of virions. The slower second phase decline appears to be related to the reduction in the rate of infection of new hepatocytes combined with an increased death rate of infected hepatocytes. A nonresponder will exhibit no decrease in viral load from baseline. A null responder will have a minimal drop in HCV RNA—for example, between 1-2 log10 IU/mL within 1 or 2 days but no further decrease thereafter. These individuals never achieve an undetectable viral load. Slow-partial responders are defined as having a rapid first-phase decline followed by a gradual second-phase decrease in viral levels. Finally, a rapid virologic responder will have rapid first- and second-slope viral declines with viral levels becoming undetectable soon after initiation of therapy (ie, by Week 4). Patients who achieve an RVR are more likely of achieving an SVR with standard duration of therapy, with a very low risk of virologic relapse. The goal of therapy is to achieve a rapid viral reduction. Hepatitis C virus viremia should be assessed at baseline, Week 4, Week 12, and Week 24 to assess virologic response. Individuals who fail to achieve a 2 log10 reduction from baseline at week 12 may discontinue therapy because they have a low likelihood of SVR. Individuals whose HCV RNA level remains detectable after 24 weeks of therapy may also stop therapy, as they are unlikely to respond. 3. Limit of detection. 2. Rapid responder (12 weeks) Days on Treatment. 22.")
23
Définitions virologiques de la réponse au traitement: marqueurs finaux
RFT (ETR) HCV RNA indétectable en fin de traitement Échappement virologique Baisse de l’ HCV RNA à des niveaux indétectables puis rebond virologique malgré la poursuite du traitement RVS (SVR) Négativité de l’HCV RNA 24 semaines après la fin du traitement Rechute RFT puis rebond viral avant la RVS A treatment response is defined as an undetectable HCV RNA level at the end of treatment. Virologic breakthrough refers to a decline in HCV RNA levels below detectable levels followed by a return to detectable levels at any time during therapy. As mentioned earlier, SVR is defined as the absence of detectable HCV RNA in the serum at Week 24 after the end of treatment. Currently, SVR is the best indicator of effective treatment. A relapse is the re-emergence of detectable HCV RNA after the discontinuation of therapy, suggesting that some virus was still present when treatment was discontinued. Pawlotsky JM. Hepatology. 2002;36(suppl 1):S65-S73. Sethi A, et al. Clin Liver Dis. 2005;9: 23
 HCV RNA indétectable en fin de traitement. Échappement virologique. Baisse de l’ HCV RNA à des niveaux indétectables puis rebond virologique malgré la poursuite du traitement. RVS (SVR) Négativité de l’HCV RNA 24 semaines après la fin du traitement. Rechute. RFT puis rebond viral avant la RVS. A treatment response is defined as an undetectable HCV RNA level at the end of treatment. Virologic breakthrough refers to a decline in HCV RNA levels below detectable levels followed by a return to detectable levels at any time during therapy. As mentioned earlier, SVR is defined as the absence of detectable HCV RNA in the serum at Week 24 after the end of treatment. Currently, SVR is the best indicator of effective treatment. A relapse is the re-emergence of detectable HCV RNA after the discontinuation of therapy, suggesting that some virus was still present when treatment was discontinued. Pawlotsky JM. Hepatology. 2002;36(suppl 1):S65-S73. Sethi A, et al. Clin Liver Dis. 2005;9:")
24
Schéma de rechute 7 Breakthrough 6 Relapse 5 2 log10 decline 4
Peg-IFN + RBV 7 Breakthrough 6 Relapse 5 2 log10 decline 4 HCV RNA (log10 IU/mL) 3 An end-of-treatment response for genotypes 2 and 3 is defined as an undetectable viral load at the end of 24 weeks of therapy, whereas an end-of-treatment response for genotype 1 is an undetectable viral load at Week 48. An SVR occurs when an undetectable viral load is maintained 24 weeks after the end of treatment. To detect potential viral relapses, viral loads should be assessed at Weeks 12 and 24 after discontinuation of therapy. Virologic relapse is typically associated with an increase in serum ALT and a resurgence of HCV viral load, often to baseline levels. An SVR is associated with normal serum ALT and no detectable virus. 2 SVR Limit of detection 1 ETR (G1/2) ETR (G3/4) 6 12 18 24 30 36 42 48 54 60 66 72 78 Weeks 24
 3. An end-of-treatment response for genotypes 2 and 3 is defined as an undetectable viral load at the end of 24 weeks of therapy, whereas an end-of-treatment response for genotype 1 is an undetectable viral load at Week 48. An SVR occurs when an undetectable viral load is maintained 24 weeks after the end of treatment. To detect potential viral relapses, viral loads should be assessed at Weeks 12 and 24 after discontinuation of therapy. Virologic relapse is typically associated with an increase in serum ALT and a resurgence of HCV viral load, often to baseline levels. An SVR is associated with normal serum ALT and no detectable virus. 2. SVR. Limit of. detection. 1. ETR (G1/2) ETR (G3/4) Weeks. 24.")
25
Facteurs prédictifs de RVS
Baseline Factor SVR Rates Peg-IFN alfa-2a + RBV OR Peg-IFN alfa-2b + RBV HCV RNA, %[1,2] < 2 x 106 copies/mL 62-78 > 2 x 106 copies/mL 42-53 Genotype, %[1,2] 2 or 3 76-82 1 42-46 Genotype 1 and high viral load, % 30-41 Liver histology, %[1,2] Stage 0-2 55-57 Stage 3-4 41-44 Age[1,2] Older age, lower SVR* Weight[1,2] Higher weight, lower SVR* Race, %[3,4] Black 19-28 White 52 It is important to note that the most powerful predictor of virologic response to peginterferon plus ribavirin is the HCV genotype. Patients infected with genotype 1 have a 42% to 46% probability of response after 48 weeks of therapy with pegylated interferon plus ribavirin, whereas response rates of 76% to 82% can be expected after only 24 weeks of treatment for patients with genotype 2 or 3. Of particular note, individuals with HCV genotype 1 and a high viral load—defined as greater than 800,000 IU/mL or 2 million copies/mL—have only a 30% to 41% response rate, whereas HCV viral load does not affect response in patients with genotypes 2 and 3. For individuals with bridging fibrosis or cirrhosis, known as stage 3 or 4 fibrosis, the response rate is approximately 10% lower compared with patients with less liver disease. However, it is important to note that these individuals do respond to therapy and treatment should not be deferred. Body weight also appears to be a predictor of virologic response, with a marginally lower virologic response for patients who weigh more. Although the exact reasons for this are not clear, some research suggests that it may be related to insulin resistance or to the effect of obesity and steatosis on liver biopsy. Patient ethnicity or race is an important predictor of treatment response; black patients have a markedly reduced response rate compared with caucasian or white patients. In one study, 52% of white patients responded to treatment compared with only 19% to 28% of those who were black. Reasons for the different responses among people of different racial backgrounds are unclear, but race has been a powerful predictor of response across many studies. *Logistic regression analysis: P ≤ .002 1. Manns MP, et al. Lancet. 2001;358: Fried MW, et al. N Engl J Med ;347: Muir AJ, et al. N Engl J Med. 2004;350: Conjeevaram HS, et al. Gastroenterology. 2006;131: 25

26
Effets secondaires fréquents (≥ 10% of Patients)
Adverse Event, % Peginterferon alfa-2a/b + Ribavirin Injection-site reaction 23-75 Fatigue/asthenia 65-66 Pyrexia (fever) 41-46 Rigors 25-48 Pain 10 Nausea/vomiting 14-43 Abdominal pain 8-13 Diarrhea 11-22 Leukopenia 6-14 Anemia 11-12 Neutropenia 26-27 Anorexia 24-32 Weight decrease 10-29 Right upper quadrant pain 12 Myalgia 40-56 Some of the most common adverse events during a standard course of HCV therapy are listed on this and the following slide. This table is based on the prescribing information for the 2 pegylated interferon alfa agents in combination with ribavirin in registrational trials that were performed in the general population. Rates of adverse events in studies of HCV treatment in the IDU patient population suggest that these rates are similar, but there are not enough data to definitively state this. Injection-site reactions, nausea and vomiting, cytopenia, fatigue, and a cluster of symptoms commonly described as flu-like symptoms are some of the most commonly associated adverse events with HCV therapy in the general population.
 Rigors Pain. 10. Nausea/vomiting Abdominal pain Diarrhea Leukopenia Anemia Neutropenia Anorexia Weight decrease Right upper quadrant pain. 12. Myalgia Some of the most common adverse events during a standard course of HCV therapy are listed on this and the following slide. This table is based on the prescribing information for the 2 pegylated interferon alfa agents in combination with ribavirin in registrational trials that were performed in the general population. Rates of adverse events in studies of HCV treatment in the IDU patient population suggest that these rates are similar, but there are not enough data to definitively state this. Injection-site reactions, nausea and vomiting, cytopenia, fatigue, and a cluster of symptoms commonly described as flu-like symptoms are some of the most commonly associated adverse events with HCV therapy in the general population.")
27
Peginterferon alfa-2a/b + Ribavirin
Adverse Event, % Peginterferon alfa-2a/b + Ribavirin Arthralgia 22-34 Musculoskeletal pain 21 Headache 43-62 Dizziness 14-21 Resistance mechanism disorders 12-18 Irritability/anxiety/nervousness 33-47 Insomnia 30-40 Depression 20-31 Concentration impaired 10-17 Dyspnea 13-26 Cough 10-23 Pharyngitis 12 Alopecia 28-36 Pruritus 19-29 Dermatitis/rash 16-24 Dry skin 10-24 Neuropsychiatric and cutaneous adverse events also occur in a significant proportion of patients treated for HCV. These events will be discussed in more detail later in the presentation. PEG-Intron [package insert]. Kenilworth, NJ: Schering Corp; July Pegasys [package insert]. Nutley, NJ: Roche Pharmaceuticals; May 2005.

28
Effets secondaires hématologiques
Anemia Neutropenia Thrombocytopenia Definition Hemoglobin < 12 g/dL > 3 g/dL decrease in Hb Absolute neutrophil count (ANC) < 750 cells/mL Platelets < 75,000/mL Etiology Ribavirin: hemolysis Interferon: bone marrow suppression Monitor Monitor labs closely first weeks Assess severity of symptoms Monitor platelet counts closely during the first weeks Assess for gum bleeding, bruising, nose bleeds Dose Adjust Adjust ribavirin dose per PI Adjust interferon dose per PI Consider Pharmacologic Intervention* Epoetin alfa 40,000 units SC weekly or darbepoetin alfa 300 µg SC every other week Granulocyte colony-stimulating factor 300 µg SC TIW Should not be given as primary therapy to prevent peginterferon alfa dose reductions Administration of oprelvekin is associated with edema in the lower extremities and cannot be recommended Phase I studies of eltrombopag show promise but optimal dose not yet determined Anemia is another common adverse effect of HCV treatment, resulting from a combination of ribavirin-induced hemolysis and interferon-related bone marrow suppression. Anemia is defined as a hemoglobin < 12g/dL or a > 3-g/dL decrease in hemoglobin from baseline. Ribavirin-induced hemolytic anemia typically occurs during the first month of treatment with an average 2.5- to 3.0-g/dL drop in hemoglobin. Patients should be monitored closely for anemia with frequent laboratory testing during the initial treatment period including at baseline, treatment Weeks 2 and 4, and monthly thereafter. In addition to monitoring laboratory results, assess for symptoms of anemia at each clinic visit. Some patients may have a minimal change in hemoglobin but may develop symptoms that impact quality of life and could affect medication adherence. To date, management of hematologic abnormalities in large, phase III clinical trials has relied on dose reduction of peginterferon and ribavirin. Medication adherence affects sustained virologic response, which has led many treating providers to use erythropoietin and granulocyte colony stimulating factor (G-CSF) as adjunctive therapies to minimize the need for dose reduction, although none of these agents are currently indicated for this therapeutic strategy. The use of epoetin alfa or darbepoetin alfa to treat anemia has been successful in avoiding ribavirin dose reduction. It is important to maintain full-dose ribavirin particularly during the first 12 weeks of therapy to optimize the potential for an early virologic response. Thrombocytopenia is another commonly associated hematologic consequence of HCV therapy and is defined as < 75,000 platelets/mL. Platelet count should be monitored at every visit and intensively for the first weeks of therapy. Oprelvekin has been used as a pharmacologic intervention for HCV treatment–related thrombocytopenia but is associated with edema in the lower extremities and cannot be recommended in this population. The investigational agent eltrombopag has shown promise in restoring HCV patients’ platelet counts both as treatment before and after initiation of HCV therapy, but it has not been tested in the injection drug user population. *Off-label use, no known interactions with methadone. PEG-Intron [package insert]. Kenilworth, NJ: Schering Corp; July Pegasys [package insert]. Nutley, NJ: Roche Pharmaceuticals; May Soza A, et al. Hepatology. 2002;36: Afdhal NH, et al. DDW Abstract 505.
 < 750 cells/mL. Platelets < 75,000/mL. Etiology. Ribavirin: hemolysis. Interferon: bone marrow suppression. Monitor. Monitor labs closely first weeks. Assess severity of symptoms. Monitor platelet counts closely during the first weeks. Assess for gum bleeding, bruising, nose bleeds. Dose Adjust. Adjust ribavirin dose per PI. Adjust interferon dose per PI. Consider Pharmacologic Intervention* Epoetin alfa 40,000 units SC weekly or darbepoetin alfa 300 µg SC every other week. Granulocyte colony-stimulating factor 300 µg SC TIW. Should not be given as primary therapy to prevent peginterferon alfa dose reductions. Administration of oprelvekin is associated with edema in the lower extremities and cannot be recommended. Phase I studies of eltrombopag show promise but optimal dose not yet determined. Anemia is another common adverse effect of HCV treatment, resulting from a combination of ribavirin-induced hemolysis and interferon-related bone marrow suppression. Anemia is defined as a hemoglobin < 12g/dL or a > 3-g/dL decrease in hemoglobin from baseline. Ribavirin-induced hemolytic anemia typically occurs during the first month of treatment with an average 2.5- to 3.0-g/dL drop in hemoglobin. Patients should be monitored closely for anemia with frequent laboratory testing during the initial treatment period including at baseline, treatment Weeks 2 and 4, and monthly thereafter. In addition to monitoring laboratory results, assess for symptoms of anemia at each clinic visit. Some patients may have a minimal change in hemoglobin but may develop symptoms that impact quality of life and could affect medication adherence. To date, management of hematologic abnormalities in large, phase III clinical trials has relied on dose reduction of peginterferon and ribavirin. Medication adherence affects sustained virologic response, which has led many treating providers to use erythropoietin and granulocyte colony stimulating factor (G-CSF) as adjunctive therapies to minimize the need for dose reduction, although none of these agents are currently indicated for this therapeutic strategy. The use of epoetin alfa or darbepoetin alfa to treat anemia has been successful in avoiding ribavirin dose reduction. It is important to maintain full-dose ribavirin particularly during the first 12 weeks of therapy to optimize the potential for an early virologic response. Thrombocytopenia is another commonly associated hematologic consequence of HCV therapy and is defined as < 75,000 platelets/mL. Platelet count should be monitored at every visit and intensively for the first weeks of therapy. Oprelvekin has been used as a pharmacologic intervention for HCV treatment–related thrombocytopenia but is associated with edema in the lower extremities and cannot be recommended in this population. The investigational agent eltrombopag has shown promise in restoring HCV patients’ platelet counts both as treatment before and after initiation of HCV therapy, but it has not been tested in the injection drug user population. *Off-label use, no known interactions with methadone. PEG-Intron [package insert]. Kenilworth, NJ: Schering Corp; July Pegasys [package insert]. Nutley, NJ: Roche Pharmaceuticals; May Soza A, et al. Hepatology. 2002;36: Afdhal NH, et al. DDW Abstract 505.")
29
Hépatite B chronique

30
Virus de l’hépatite B - Virus à ADN - 2 types :
- Virus sauvage (AgHBe+) : 35% - Virus mutant pré-C (AgHBe -) : 65%
 : 35% - Virus mutant pré-C (AgHBe -) : 65%")
31
F A C Ba E B 400 millions de porteurs chroniques Bj
décès par an (dont 10% hépatite aiguë et 90 % cirrhose + Carcinome hépatocellulaire) A D B C F Ba Bj E Fung et Lok. Hepatology 2004 8 Génotypes 360 millions de personnes dans le monde atteints d ’hépatite B chronique décès/an ( hépatite aiguë et cirrhose ou CHC) Prévalence < 1% Europe, Amérique du Nord et Australie 1-8% régions Méditerranéennes et Europe de l’Est > 8% Afrique et Asie 3 zones géographiques correspondant à niveaux d ’endémie différent : - zone de faible endémie : contamination sexuelle ou par toxicomanie, entre 15 et 25 ans. Ag Hbe + - zone de moyenne endémie : contamination intra-familiale, périnatale ou sexuelle. Ag Hbe -. - zone de haute endémie : infection précoce (materno-infantile ou intrafamiliale précoce). AgHBe +. Prévalence de l’AgHBs ≥ 8% - Forte 2-7% - Moyenne < 2% - Faible 3
 A. D. B. C. F. Ba. Bj. E. Fung et Lok. Hepatology Génotypes. 360 millions de personnes dans le monde atteints d ’hépatite B chronique décès/an. ( hépatite aiguë et cirrhose ou CHC) Prévalence. < 1% Europe, Amérique du Nord et Australie. 1-8% régions Méditerranéennes et Europe de l’Est. > 8% Afrique et Asie. 3 zones géographiques correspondant à niveaux d ’endémie différent : - zone de faible endémie : contamination sexuelle ou par toxicomanie, entre 15 et 25 ans. Ag Hbe + - zone de moyenne endémie : contamination intra-familiale, périnatale ou sexuelle. Ag Hbe -. - zone de haute endémie : infection précoce (materno-infantile ou intrafamiliale précoce). AgHBe +. Prévalence de l’AgHBs. ≥ 8% - Forte. 2-7% - Moyenne. < 2% - Faible. 3.")
32
L’hépatite B chronique: une maladie silencieuse
70% asymptomatic 30% symptomatic 1% fulminant => hepatic transplantation Contamination Acute hepatitis 90-95% 5-10% HBsAg+ HBsAg - Anti-HBs+ & HBc+ Cure Chronic infection 70% 30% Chronic hepatitis 20% HCC Cirrhosis Inactive carrier 20% (3-5%/year)
")
33
Natural history of chronic HBV infection
anti HBs HBsAg Inactive phase Cure Tolerance phase Active phase DNA ALT HBe Ag anti HBe 33

34
Progression des variants HBe-
HBeAg Anti HBe ALT HBV DNA Wild PreC mutant

35
Influence de la réplication virale B sur l’histoire naturelle
Survie 1.0 0.8 0.6 0.4 0.2 AgHBe - AgHBe + 84 24 36 48 60 72 12 Décompensation P=0.018* Niederau et al. N Eng J Med 1996 Chen et al. JAMA; 2006, 295: 65-73 Carcinome Hépatocellulaire

36
Influence de la charge virale sur l’incidence de la cirrhose: REVEAL
Cumulative Incidence of Liver Cirrhosis All Subjects (n=3,582) 40 Baseline HBV DNA level, copies/mL 36.2% ≥106 (n=602) 105–<106 (n=333) 104–<105 (n=628) 300–<104 (n=1,150) <300 (n=869) 30 23.5% Cumulative incidence of liver cirrhosis (% subjects) 20 The cumulative incidence of liver cirrhosis over time increased with increasing baseline HBV DNA levels: high viral load is associated with increased incidence of cirrhosis. The figure on this slide shows the cumulative incidence of cirrhosis in the R.E.V.E.A.L.-HBV study. The cumulative incidence rates were calculated for different categories of serum HBV DNA level using the Nelson–Aalen method, a nonparametric method for estimating the cumulative hazard. The cumulative incidence of liver cirrhosis was 4.5%, 5.9%, 9.8%, 23.5% and 36.2% for patients with baseline serum HBV DNA serum levels of <300, 300–9.9 x 103, 104–9.9 x 104, 105–9.9 x 105 and ≥106 copies/mL, respectively. The greatest cumulative incidence of cirrhosis (36.2%) was observed in patients with serum HBV DNA levels of ≥106 copies/mL. However, it is interesting to note that the 1,563 patients (44%) with HBV DNA levels of 104 copies/mL or more accounted for 274 (75%) of the cirrhosis cases. Log rank test of trend p<0.001 10 9.8% 5.9% 4.5% 1 2 3 4 5 6 7 8 9 10 11 12 13 Year of follow-up Iloeje UH, et al. Gastroenterology. 2006;130; 36
 40. Baseline HBV DNA level, copies/mL. 36.2% ≥106 (n=602) 105–<106 (n=333) 104–<105 (n=628) 300–<104 (n=1,150) <300 (n=869) % Cumulative incidence of liver cirrhosis (% subjects) 20. The cumulative incidence of liver cirrhosis over time increased with increasing baseline HBV DNA levels: high viral load is associated with increased incidence of cirrhosis. The figure on this slide shows the cumulative incidence of cirrhosis in the R.E.V.E.A.L.-HBV study. The cumulative incidence rates were calculated for different categories of serum HBV DNA level using the Nelson–Aalen method, a nonparametric method for estimating the cumulative hazard. The cumulative incidence of liver cirrhosis was 4.5%, 5.9%, 9.8%, 23.5% and 36.2% for patients with baseline serum HBV DNA serum levels of <300, 300–9.9 x 103, 104–9.9 x 104, 105–9.9 x 105 and ≥106 copies/mL, respectively. The greatest cumulative incidence of cirrhosis (36.2%) was observed in patients with serum HBV DNA levels of ≥106 copies/mL. However, it is interesting to note that the 1,563 patients (44%) with HBV DNA levels of 104 copies/mL or more accounted for 274 (75%) of the cirrhosis cases. Log rank test of trend. p< % 5.9% 4.5% Year of follow-up. Iloeje UH, et al. Gastroenterology. 2006;130;")
37
Pourquoi dépister ? Maladie fréquente : Risque d’évolution vers :
Cirrhose Cancer primitif du foie Traitements : Diminuer la multiplication virale Contrôler la progression de la fibrose

38
Qui dépister ? Obligatoire : Recommandé :
Donneurs de sang, d’organes, de tissus ou cellules Femmes enceintes Recommandé : Sujets contacts d’un malade ayant une hépatite B Sujets ayant une augmentation des transaminases Sujets ayant des facteurs de risque d’infection : Transfusion sanguine Toxicomanie Exposition nosocomiale Prisonnier Migrant, zone d’endémie Partenaires sexuels multiples

39
Comment dépister ? Un test : antigène HBS

40
Comment interpréter une sérologie VHB ?
Hépatite Vaccin Guérison Ag HBs + - Ac anti-HBs Ac anti-HBc + * *IgM anti-HBC négatif si chronique

41
Diagnostic d’une hépatite chronique B
Ag HBe Ac anti-HBe ADN du VHB Interprétation Transaminases* + - > 5 log Hépatite chronique B (Virus sauvage) - + > 5 log Hépatite chronique B (Virus mutant) (fluctuantes *) - + < 4 log * Portage inactif N (constantes *) *plusieurs dosages nécessaires
 - + > 5 log. Hépatite chronique B. (Virus mutant) (fluctuantes *) - + < 4 log * Portage inactif. N. (constantes *) *plusieurs dosages nécessaires.")
42
ADN du VHB Hépatite chronique AgHBe+ Portage inactif Fluctuant 103-108
<104 copies/ml >106 copies/ml copies/ml Hépatite chronique AgHBe- L’ADN VHB ne permet pas de bien discriminer les porteurs inactifs des malades atteints d ’hépatite chronique AgHBe négatif. Seul le suivi régulier permet d ’affirmer le diagnostic de porteur inactif

43
Evaluation de la fibrose
Examen de référence : biopsie hépatique Examens non invasifs : évaluation en cours Marqueurs sériques Fibroscan

44
Obstacle au diagnostic de la fibrose: la PBH
Examen invasif, mal toléré par les patients Morbidité (0,3 à 0,6%) Mortalité (0 à 0,05%) Méthode contestée Coûteux (500 €)- Hospitalisation ≥ 6-18H Développement de marqueurs non invasifs : Biochimiques : Fibrotest, Fibromètre, Shasta, Zeng, Apri, Hepascore, AST/ALT, Acide hyaluronique, Forns, Fib-4 Mesure de l’elastométrie : Fibroscan Etiologie hépatopathie influence les performances diagnostiques et les seuils des tests non invasifs
 Mortalité (0 à 0,05%) Méthode contestée. Coûteux (500 €)- Hospitalisation ≥ 6-18H. Développement de marqueurs non invasifs : Biochimiques : Fibrotest, Fibromètre, Shasta, Zeng, Apri, Hepascore, AST/ALT, Acide hyaluronique, Forns, Fib-4. Mesure de l’elastométrie : Fibroscan. Etiologie hépatopathie influence les. performances diagnostiques et les. seuils des tests non invasifs.")
45
Objectifs du traitement
Atteindre une suppresion durable de la réplication de l’ADN-VHB 1 Diminution d’au moins > 1 log à 12 semaines Indetectabilité à 24 semaines Contrôler l’évolution de la maladie hépatique 1 normalisation des ALAT régression de l’nflammation Prevention de la cirrhose et du CHC séroconversion HBeAg et HBsAg à long terme ? AASLD guidelines, Hepatology,2007: 45: 439

46
Quels patients doivent être traités?
Plusieurs paramètres doivent être pris en compte : Charge virale VHB Répéter les dosages de l’AND-VHB est nécessaire ALAT Répéter les dosages est nécessaire Lésions histologiques Biopsiehépatique ou tests non invasifs Prendre en compte l’histoire médicale du patient (transmission verticale, comorbiditées..)
")
47
Quand traiter les patients HBeAg + ?
HBV-DNA ALT STRATEGY > UI/mLa > 2 Nb Follow-up at 3 months (spontaneous Hbe seroconversion) TREATMENT Biopsy Treatment if inflammatoray lesions or fibrosis < 2 N a : UI/mL = 105 cop/mL b : ALT N = 30 UI for male, 19 IU/l for female
 TREATMENT. Biopsy. Treatment if inflammatoray lesions or fibrosis. < 2 N. a : UI/mL = 105 cop/mL. b : ALT N = 30 UI for male, 19 IU/l for female.")
48
Quand traiter les patients Hbe- Ag ?
Evolution plus défavorable de la maladie HBV-DNA ALT Strategy > UI/mLa > 2N TREATMENT > 2000 UI/mLb 1 – 2 N < 2000 UI/mLb < 1 N Follow-up Biopsy Treatment if inflammatoray lesions or fibrosis a : UI/mL = 105 cop/mL ; b : 2000 IU/mL = 104 cop/mL

49
Quand traiter les patients cirrhotiques ?
ADN-VHB Cirrhosis Strategy Detectable > 2000 UI/mla Compensated Treatment Decompensated Transplantation Indetectable Follow-up a : 2000 IU/mL = 104 cop/mL

50
Développement des traitements antiVHB
IFN 1983 Adefovir 2003 Entecavir 2006 Tenofovir 2008 Lamivudine 1999 Peg IFN 2005 Telbivudine 2007

51
Efficacité 6 mois après l’arrêt du traitement
IFN PEG alpha 2a dans l’HC AgHBe+ Efficacité 6 mois après l’arrêt du traitement 80 Malades (%) 60 41% 40 32% 32% 20 14% 3% ALAT N Seroconv HBe ADN VHB < ADN VHB- PCR AgHBs- Lau et al. NEJM 2005
 % % 32% % 3% ALAT N. Seroconv. HBe. ADN VHB. < ADN VHB- PCR. AgHBs- Lau et al. NEJM")
52
Efficacité 6 mois après l’arrêt du traitement
IFN PEG alpha 2a dans l’HC AgHBe- Efficacité 6 mois après l’arrêt du traitement 80 Malades (%) 59% 60 42% 40 17% 20 4% ALAT N ADN VHB < ADN VHB- PCR AgHBs- Marcellin et al. NEJM 2004
 59% % % 20. 4% ALAT N. ADN VHB. < ADN VHB- PCR. AgHBs- Marcellin et al. NEJM")
53
Interferon Pegylé Avantages Traitement limité dans le temps : 12 mois
Absence de résistance Traitement conduisant au plus haut taux de séroconversion (8-10% après 1 an de traitement) Limites Efficacité globale faible : HBV-DNA indetectable dans 30% des cas tolérance mauvaise Injections Contre-indiqué en cas de cirrhose décompensée ALAT élevée (> 5N) Genotype A et B HBV DNA bas
 Limites. Efficacité globale faible : HBV-DNA indetectable dans 30% des cas. tolérance mauvaise. Injections. Contre-indiqué en cas de cirrhose décompensée. ALAT élevée (> 5N) Genotype A et B. HBV DNA bas.")
54
Facteurs pronostics d’efficacité de l’interféron Peg chez les patients HBeAg+
Age < 40 ans ALAT > 5N Genotype A ou B HBV DNA bas (< copies/mL)
")
55
Éviter la monotherapie
Lamivudine Analogue nucléosidique Dosage: 100 mg/d Avantages Effet antiviral rapide excellent profile de tolérance Coût modeste du traitement Limites incidence élevée de résistance Réactivation virale Rate of genotypic resistance in naive HBeAg + patients Éviter la monotherapie Pas de 1ère intention

56
Lamivudine dans l’HC AgHBe+
Séroconversion HBe 60 48% 50 40% 40 29% Séroconversion AgHBe (%) 30 22% 20 10 ans
 % ans.")
57
Adefovir dipivoxil Analogue Nucleotide Dosage: 10 mg/d Avantages
Absence de résistance croisée avec la lamivudine Limites Modeste décroissance de l’ HBV DNA Emergence de résistance

58
Adefovir dans l’HC AgHBe+ Efficacité virologique et biochimique
Adefovir dans l’HC AgHBe+ Efficacité virologique et biochimique* à 3 ans 1 an 2 ans 3 ans 90% 80% 80% 70% 46% 70% 63% 60% 48% 33% Malades (%) 50% 38% 40% 29% 30% 14% 20% 10% 0% ADN VHB<1000 cp/ml Normalisation ALAT Séroconversion e *Estimation Kaplan Meier Marcellin et al. EASL 2004
 50% 38% 40% 29% 30% 14% 20% 10% 0% ADN VHB<1000 cp/ml. Normalisation ALAT. Séroconversion e. *Estimation Kaplan Meier. Marcellin et al. EASL")
59
Adefovir dans l’HC AgHBe- Efficacité virologique et biochimique à 5 ans
90 80 70% 69% 67% 65% 70 60 Malades (%) 50 40 30 20 10 ADN <1000 copies/mL Normalisation des ALAT Hadziyannis et al. AASLD 2005
 ADN <1000 copies/mL. Normalisation des ALAT. Hadziyannis et al. AASLD")
60
Résistance génotypique à l’adéfovir
40 29% 30 Malades (%) 18% 20 11% 10 3% 0% ans Hadziyannis et al. AASLD 2005
 18% % 10. 3% 0% ans. Hadziyannis et al. AASLD")
61
Médicaments récemment commercialisés ou en cours d’évaluation
Entecavir Tenofovir (AMM pour VIH) Emtricitabine (AMM pour VIH) Telbivudine Combinaisons : Interféron pegylé + analogue Deux analogues
 Emtricitabine (AMM pour VIH) Telbivudine. Combinaisons : Interféron pegylé + analogue. Deux analogues.")
62
Entecavir Analogue nucléosidique
0,5 mg/d chez patients naifs - 1 mg/d patients LAMr Avantages Activité antivirale importante à un 1 an : 67% d’ HBV DNA indétectable pour les patients HBeAg + 90% d’HBV DNA indétectable pour les patients HBeAg - Très faible taux de resistance (<1% à 4 ans) Excellente tolérance Limites Barrière génétique basse chez les patients avec LAM resistance Eviter d’utiliser en cas de HIV infection if patient non traité par HAART
 Excellente tolérance. Limites. Barrière génétique basse chez les patients avec LAM resistance. Eviter d’utiliser en cas de HIV infection if patient non traité par HAART.")
63
Telbivudine Globe study : % of patients with indectectable
Analogue Nucleosidique Dosage: 10 mg/d Avantages Efficacité supérieure à celle de la lamivudine Limites Moins efficace que entecavir et tenofovir Résistance croisée avec lamivudine Emergence rapide de resistance tolérance ? Globe study : % of patients with indectectable HBV DNA at 2 years 63

64
Ténofovir Analogue nucléotidique Commercialisation en 2002 pour le VIH
Essais thérapeutiques chez le patient mono-infecté VHB présenté en 2007 Probablement le plus puissant des traitements anti-VHB Besoin d’evaluer à long terme la tolérance rénale et osseuse.

65
patients HBeAg + : efficacité des traitements à un an
% of patients with indectectable HBV DNA : < 300 cop/ml*/ < 400 cop/ml**

66
patients HBeAg - : efficacité des traitements à un an
% of patients with indectectable HBV DNA: < 300 cop/ml*/ < 400 cop/ml** 66

67
Patients HBe+ Ag : seroconversion Hbe après deux ans de traitement

68
DEUX STRATEGIES THERAPEUTIQUES
INTERFERON ANALOGUES Durée limitée Durée indéfinie Tolérance médiocre Tolérance bonne Négativation AgHBs Plus rare Pas de résistance Résistance RÉPONSE PROLONGÉE RÉPONSE MAINTENUE

69
INTERFERON Réplication Activité Réponse prolongée IFN (ADN VHB) (ALAT
histologie) Réponse prolongée
 Réponse. prolongée.")
70
Analogue nucléos(t)idique
ANALOGUES Analogue nucléos(t)idique Réplication (ADN VHB) Échappement Résistance Activité (ALAT histologie) Réponse maintenue
idique. Réplication. (ADN VHB) Échappement. Résistance. Activité. (ALAT. histologie) Réponse. maintenue.")
71
QUI TRAITER ? - ADN VHB > 100 000 copies/mL (20 000 UI/ml)
Fibrose hépatique significative (F ≥ 2) ALAT augmentées: faible efficacité si < 2N - Et selon l’age, la probabilité de réponse, les risques... EASL Consensus Statement. J Hepatol 2003; Sup 1
 ALAT augmentées: faible efficacité si < 2N. - Et selon l’age, la probabilité de réponse, les risques... EASL Consensus Statement. J Hepatol 2003; Sup 1.")
72
COMMENT TRAITER ? (INF PEG)
En première intention (traitement court et possibilité de réponse prolongée): Interferon - En cas de non réponse à l ’interféron ou de contre-indication: analogues (INF PEG) EASL Consensus Statement. J Hepatol 2003; Sup 1
: Interferon. - En cas de non réponse à l ’interféron ou de contre-indication: analogues. (INF PEG) EASL Consensus Statement. J Hepatol 2003; Sup 1.")
73
Résumé AgHBs + ADN VHB> 100 000 et transaminases élevées
Ponction Biopsie < A1 et F > A2 ou F2 Surveillance Traitement Interferon Analogue EASL Consensus Statement. J Hepatol 2003; Sup 1

74
Comment commencer le traitement ?
Monotherapie puis addition ! Combinaison seulement !

75
Follow-up every 3 months
Strategie « add-on » : monotherapie initiale puis addition si nécessaire HBV-DNA A + B Follow-up every 3 months 300 cop/ml Month3 Month6 time

76
Strategie de combinaison
% de résistance à lamivudine Pas d’avantage en terme de décroissance virale Décroissance de résistance Sung, J Hepatol, 2003

77
% patients with disease progression
L’effet antiviral sur la progression de la maladie est réduit si émergence de mutations Kaplein-Meier estimates of time to disease progression in Asians with CHB 25 Placebo (n=215) 21% Lamivudine treatment wild-type HBV (n=221) 20 Lamivudine treatment lamivudine-resistant HBV (n=209, 49%) 15 % patients with disease progression 13% 10 5% 5 6 12 18 24 30 36 Time after randomisation (months) Liaw Y-F, et al. Semin Liver Dis. 2005;25(Suppl 1):40-7. 77
 21% Lamivudine treatment wild-type HBV (n=221) 20. Lamivudine treatment. lamivudine-resistant HBV (n=209, 49%) 15. % patients with disease progression. 13% 10. 5% Time after randomisation (months) Liaw Y-F, et al. Semin Liver Dis. 2005;25(Suppl 1):")
78
Meilleurs choix initiaux
Si monotherapie : Entecavir 0.5 mg/d Tenofovir 300 mg/d Combinaison en cas de maladie sévère Entecavir + Tenofovir Lamivudine 100 mg/d + Adefovir 10 mg/d Chez les patients HBeAg+, si bons facteurs de réponse : Pegylated IFN pour 12 mois

79
Particularités des co-infections VIH - hépatites chroniques
Pourquoi traiter tôt ? Outils de diagnostic et de suivi Avancées thérapeutiques Nouveaux challenges

80
Pourquoi traiter tôt ?

81
Pourquoi traiter tôt ? (1)
VIH et morbi-mortalité hépatique mortalité hépatique2,3 Ère post cART Incidence / Mortalité Evts SIDA1 MTF / CHC5,6 VHB: patients vivant en Europe 36% excès de risque décès / VHB (OR=1.36 [1.12 – 1.64]4 Risque accru d’hépatotoxocité / co-infections à l’instauration des ARVs7 1Palella FJ, JAIDS Konopnicki D, AIDS Lewden C, JAIDS Nikolopoulos G, CID Thio CL, Lancet Salmon-Ceron D, J Hepatol Sulkowski MS, et al. JAMA 2000.

82
Pourquoi traiter tôt ? (2)
Co-infections multiples Modes de contamination communs VIH, VHB, VHC et VHD 29.9% VIH-VHB-VHC dans Eurosida1 7.8% of VIH-VHB-VHD et VIH-VHB-VHC-VHD dans Cohorte VIH-VHB Paris-Lyon2 réplications VHC et VHD sans effet des traitements sur le VHD3 progression de la fibrose et risque majeur de MTF4,5 1Konopnicki D, AIDS Lacombe K, AIDS Boyd A, J Viral Hepat lacombe K, AIDS Sheng WH, CID 2007.

83
Démarche diagnostique et de suivi

84
Diagnostic et suivi (1) Fréquence du screening périodique
Au moment du diagnostic VIH puis tous les ans / 3 ans (+ si IST)1 Tester pour VHD (si VHB) et VHA (voire VHE ?!) Si sérologie VHA et VHB négatives, vacciner +++ Si anticorps antiHBc isolés Rechercher l’hépatite B occulte, voire la co-infection VHC3,4 Quantifier la charge virale VHB, voire VHC 1Rapport Yéni Piroth L, JHepatol Perez-Rodriguez MK, World J Gastroenterol 2009
1. Tester pour VHD (si VHB) et VHA (voire VHE !) Si sérologie VHA et VHB négatives, vacciner +++ Si anticorps antiHBc isolés. Rechercher l’hépatite B occulte, voire la co-infection VHC3,4. Quantifier la charge virale VHB, voire VHC. 1Rapport Yéni Piroth L, JHepatol Perez-Rodriguez MK, World J Gastroenterol")
85
Diagnostic et suivi (2) Évaluation initiale
Clinique: examen clinique et recherche de comorbidités (syndrome métabolique, alcool, drogues, hépatites virales multiples) Biologique: tests bio standards, autres causes d’hépatites chroniques : sérologies des hépatites virales (VHC, VHB, VHD, VHA, VHE?) Virologique: quantification virale appropriée Évaluation de la fibrose hépatique: Biopsie hépatique: encore important1 Tests biochimiques: intéressants Elastométrie: oui mais pas seule dans la co-infection VIH-VHC, pas évaluée dans la co-infection VIH-VHB. Attention aux conditions de lecture. 1Don CR, Hepatol 2009.
 Biologique: tests bio standards, autres causes d’hépatites chroniques : sérologies des hépatites virales (VHC, VHB, VHD, VHA, VHE ) Virologique: quantification virale appropriée. Évaluation de la fibrose hépatique: Biopsie hépatique: encore important1. Tests biochimiques: intéressants. Elastométrie: oui mais pas seule dans la co-infection VIH-VHC, pas évaluée dans la co-infection VIH-VHB. Attention aux conditions de lecture. 1Don CR, Hepatol")
86
Diagnostic et suivi (3) Suivi et prévention des maladies terminales du foie1: Examen + doppler US + FP Cirrhose: tous les 3 mois Pré-cirrhotique: tous les 6 mois Autres: tous les ans Si suspicion de nodules hépatiques Doppler US / Sonoview / TDM / IRM2 1AASLD guidelines ZechCJ, Dig Dis 2009.

87
Avancées thérapeutiques: co-infection VIH-VHB

88
IFN 1983 Adéfovir 2003 Entecavir 2006 Ténofovir 2002 Lamivudine 1999 Peg IFN 2005 Telbivudine 2007

89
« Take home message » #1: IFN et PegIFN
Co-infection VIH-VHB (1) « Take home message » #1: IFN et PegIFN Peg-IFN + ADV2: 17 patients traités ADV + PegIFN2a pour 48s (pilote) pas de séroconversion HBe or HBs 100% rechute réplication à la fin du traitement effet sur ALAT/ASAT pendant le traitement seulement PegIFN + TDF3 : 10 patients traités par TDF seul ou PegIFN2a seul pendant 24s, puis ajout TDF (essai randomisé) Pas de différence dans les taux de séroconversion ou niveau HBV-DNA à S48 1 HIV-/IFN+ HIV+/IFN- HIV+/IFN+ HIV-/IFN- A-B, A-C, A-D: p<0,05 B-C, B-D, C-D: NS Y a-t-il encore une place pour le PegIFN dans le contexte VIH-VHB? 1Di Martino V, Gastroenterol Ingiliz M, Antivir Ther Johnson M, HIV Clin Trials 2007.
 « Take home message » #1: IFN et PegIFN. Peg-IFN + ADV2: 17 patients traités ADV + PegIFN2a pour 48s (pilote) pas de séroconversion HBe or HBs 100% rechute réplication à la fin du traitement. effet sur ALAT/ASAT pendant le traitement seulement. PegIFN + TDF3 : 10 patients traités par TDF seul ou PegIFN2a seul pendant 24s, puis ajout TDF (essai randomisé) Pas de différence dans les taux de séroconversion ou niveau HBV-DNA à S HIV-/IFN+ HIV+/IFN- HIV+/IFN+ HIV-/IFN- A-B, A-C, A-D: p<0,05. B-C, B-D, C-D: NS. Y a-t-il encore une place pour le PegIFN. dans le contexte VIH-VHB 1Di Martino V, Gastroenterol Ingiliz M, Antivir Ther Johnson M, HIV Clin Trials")
90
« Take home message » #2: Lamivudine
Co-infection VIH-VHB (2) « Take home message » #2: Lamivudine > 90% des patients VIH-VHB traités par Lamivudine = échappement virologique à 4 ans CEPENDANT : 3TC efficace en prévention des réactivations VHB si Ac antiHBc isolés en cas de traitement immunosupresseur + PTME-VHB en situation précaire 1Benhamou Y, Hepatol 1999.
 « Take home message » #2: Lamivudine. > 90% des patients VIH-VHB traités par Lamivudine = échappement virologique à 4 ans. CEPENDANT : 3TC efficace en prévention des réactivations VHB si Ac antiHBc isolés en cas de traitement immunosupresseur + PTME-VHB en situation précaire. 1Benhamou Y, Hepatol")
91
«Take home message» #3: Adéfovir
Co-infection VIH-VHB (3) «Take home message» #3: Adéfovir 1 TDF, n=56 ADV, n=29 Sélection de souches ADV-R4 HBV DNA (< 2.6 log10 copies/ml) 8/35 HBeAg negative 3/33* HBe seroconversion 2/33* 1Benhamou Y, J Hepatol Peters M, Hepatol Lacombe K,et al. Antivir Ther Lacombe K, et al. AIDS 2006
 «Take home message» #3: Adéfovir. 1. TDF, n=56. ADV, n=29. Sélection de souches ADV-R4. HBV DNA (< 2.6 log10 copies/ml) 8/35. HBeAg negative 3/33* HBe seroconversion 2/33* 1Benhamou Y, J Hepatol Peters M, Hepatol Lacombe K,et al. Antivir Ther Lacombe K, et al. AIDS")
92
«Take home message» #4: Entécavir
Co-infection VIH-VHB (4) «Take home message» #4: Entécavir Selection of M184V following ETV tx1,2 70 % with M184V ART naïve 3/5 60 ART experienced 6/12 50 Total Univariate analysis for selection of M184V 3/7 40 Risk factor p value Total duration on ETV 0.05 Magnitude of HBV-DNA reduction on ETV 0.04 HIV-RNA pre-ETV therapy 0.87 HBV-DNA pre-ETV therapy 0.69 Nadir CD4+ count 0.20 30 20 10 Median time to M184V days 98 days 1Sasdeusz J, AIDS McMahon MA, NEJM 2007
 «Take home message» #4: Entécavir. Selection of M184V following ETV tx1, % with M184V. ART naïve. 3/ ART experienced. 6/ Total. Univariate analysis for selection of M184V. 3/ Risk factor. p value. Total duration on ETV Magnitude of HBV-DNA reduction on ETV HIV-RNA pre-ETV therapy HBV-DNA pre-ETV therapy Nadir CD4+ count Median time to M184V 148 days 98 days. 1Sasdeusz J, AIDS McMahon MA, NEJM")
93
«Take home message» #5: Telbivudine
Co-infection VIH-VHB (5) «Take home message» #5: Telbivudine Baisse modérée de la réplication du VIH sous LdT sans acquisition de résistance VIH chez ce patient 1Low E, AIDS 2009
 «Take home message» #5: Telbivudine. Baisse modérée de la réplication du VIH sous LdT sans acquisition de résistance VIH chez ce patient. 1Low E, AIDS")
94
«Take home message » #6: Ténofovir
Co-infection VIH-VHB (6) «Take home message » #6: Ténofovir Essai clinique (21 patients) Cohorte VIH-VHB Paris / Lyon1: 165 patients sous TDF (±3TC/FTC, 80% LAM-R) BL 24 weeks -1 -2 -3 -4 -5 P=0.045 TDF/TDF+3TC vs. 3TC -6 TDF 3TC TDF/3TC N = - TDF/3TC > 3TC seul mais pas au TDF seul chez patients naïfs - pas de bénéfice à continuer le 3TC chez les patients virémiques - pas de différence entre ajouter ou switcher vers le TDF 98% <2000 UI/ml 0 non répondeur, 2 rechuteurs, 4 blippers Resistance ? 1Lacombe K, CROI Lewin R, Hepatol 2009
 «Take home message » #6: Ténofovir. Essai clinique (21 patients) Cohorte VIH-VHB Paris / Lyon1: 165 patients sous TDF (±3TC/FTC, 80% LAM-R) BL. 24 weeks P= TDF/TDF+3TC vs. 3TC. -6. TDF. 3TC. TDF/3TC. N = TDF/3TC > 3TC seul mais pas au TDF seul chez patients naïfs. - pas de bénéfice à continuer le 3TC chez les patients virémiques. - pas de différence entre ajouter ou switcher vers le TDF. 98% <2000 UI/ml. 0 non répondeur, 2 rechuteurs, 4 blippers. Resistance 1Lacombe K, CROI Lewin R, Hepatol")
95
VIH-VHB: Recommandations de traitement (1)
Indication à un traitement VIH EACS guidelines 2008 HBV-DNA ≥ 2000IU/mL HBV-DNA < 2000IU/mL cirrhosis cART incluant 3TC / FTC et TDF et insérer dans le circuit TH si décompensation Patient without HBV Associated 3TC resistance Patient with HBV Associated 3TC resistance cART incluant 3TC / FTC et TDF Substituer les NUCs by TDF or ajouter TDF ou ETC cART au choix (incluant TDF + 3TC/FTC ?)
")
96
VIH-VHB: Recommandations de traitement (2)
Pas d’indication à un traitement VIH EACS guidelines 2008

97
Avancées thérapeutiques: co-infection VIH-VHC

98
Comment améliorer la réponse au traitement (1) ?
En agissant sur VIH et immunité 33 16 62 36 29 47 41 34 73 27 69 10 20 30 40 50 60 70 80 90 100 All patients (n=242) HCV genotype 1 (n=150) HCV genotypes 2-3 (n=78) Min – Q1 Q1 – Med Med – Q3 Q3 – Max taux CD4 inclusion = taux de RVS (essai clinique APRICOT) Opravil et al. J Acquir Immuno Defic Syndr 2008;47:36–49
 HCV genotype 1. (n=150) HCV genotypes 2-3. (n=78) Min – Q1. Q1 – Med. Med – Q3. Q3 – Max. taux CD4 inclusion = taux de RVS (essai clinique APRICOT) Opravil et al. J Acquir Immuno Defic Syndr 2008;47:36–49.")
99
Reduction HCV RNA (% patients)
Comment améliorer la réponse au traitement (2) ? En agissant sur dose RBV et durée traitement Reduction HCV RNA (% patients) APRICOT = 800mg (n=176) >2 log >1 log 34 63 84 50 75 81 10 20 30 40 60 70 80 90 PRESCO, Analyse per protocole, S12 100 10 20 30 40 50 60 70 80 90 48 S. 72 S. 24 S 48 S 31 53 67 82 59/192 HCV GT 1/4 (n=237) HCV GT 2/3 (n=152) RVS (% patients) 24/45 64/96 46/56 indétectable (<50 IU/mL) Nunez et al. AIDS Res Hum Retroviruses 2007;23:972–82 PRESCO = mg (n=94)
 En agissant sur dose RBV et durée traitement. Reduction HCV RNA (% patients) APRICOT = 800mg (n=176) >2 log. >1 log PRESCO, Analyse per protocole, S S. 72 S. 24 S. 48 S /192. HCV GT 1/4 (n=237) HCV GT 2/3 (n=152) RVS (% patients) 24/45. 64/96. 46/56. indétectable (<50 IU/mL) Nunez et al. AIDS Res Hum Retroviruses 2007;23:972–82. PRESCO = mg (n=94)")
100
Comment améliorer la réponse au traitement (3) ?
En agissant sur le régime ARV associé Interaction RBV-DDI avec risque d’acidose lactique Interaction RBV-ABC avec baisse des concentrations intracellulaires de RBV et moins bonne réponse Sans ABC ABC 10 20 30 40 50 60 70 80 S4 S12 S24 S36 S48 S60 S72 Patients non répondeurs (%) Laufer et al. Antiviral Ther 2008;13:953–957 Non réponse selon ABC (RBV > &3,2mg/kg/j) p=0.08 n= Rechutes (% patients) 20 40 60 80 100 RBV >2.2 µg/mL p=0.44 RBV <2.2 µg/mL avec ABC sans ABC Barreiro P et al. AASLD Abstract 342 Rechute selon ABC et [RBV]
 Laufer et al. Antiviral Ther 2008;13:953–957. Non réponse selon ABC (RBV > &3,2mg/kg/j) p=0.08. n= Rechutes (% patients) RBV >2.2 µg/mL. p=0.44. RBV <2.2 µg/mL. avec ABC. sans ABC. Barreiro P et al. AASLD Abstract 342. Rechute selon ABC et [RBV]")
101
VIH-VHC: Recommandations de traitement
G2/3 24 semaines de traitement* HCV-RNA négatif G1/4 48 semaines de traitement G2/3 HCV-RNA négatif Baisse >2 log HCV-RNA 72 semaines de traitement G1/4 HCV-RNA positif HCV-RNA positif Stop Baisse <2 log HCV-RNA Stop *chez les patients avec charge virale initiale faible et fibrose peu évoluée EACS guidelines 2008

102
Catégories Interventions recommandées
Traitements antérieurs sub-optimaux: Interferon (monothérapie ou + ribavirine) Doses faibles de ribavirine Durée de traitement courte Re-traiter avec Peg-IFN et ribavirine à dose adaptée au poids Toxicité et mauvaise observance Retraiter en maximisant le support (psychiatrique, observance, facteurs de croissance) Échec virologique Essai d’intensification (ETOC ?) Attendre les nouvelles molécules
 Doses faibles de ribavirine. Durée de traitement courte. Re-traiter avec Peg-IFN et ribavirine à dose adaptée au poids. Toxicité et mauvaise observance. Retraiter en maximisant le support (psychiatrique, observance, facteurs de croissance) Échec virologique. Essai d’intensification (ETOC ) Attendre les nouvelles molécules.")
103
Nouveaux challenges

104
Co-infection VIH-VHB: 1- Variabilité génétique
Lee WM.N Engl J Med. 1997 4 gènes (C, S, Pol, X) avec superposition des cadres de lecture Mutations sur le gène Pol sélectionnées par l’exposition aux nucléos(t)ides (3TC, FTC, ADV, ETV, LdT) Mutations sur le gène S peuvent être sélectionnées en même temps, et donc associées aux mutations du gène Pol Or, mutations du gène S baisse de l’antigénicité HBs1 et échappement vaccinal2 Impact de santé publique de l’émergence de ces mutants chez les patients traités à long terme comme les patients infectés par le VIH ? 1Torresi J, J clinc virol Kamili S, Hepatol 2009
 avec superposition des cadres de lecture. Mutations sur le gène Pol sélectionnées par l’exposition aux nucléos(t)ides (3TC, FTC, ADV, ETV, LdT) Mutations sur le gène S peuvent être sélectionnées en même temps, et donc associées aux mutations du gène Pol. Or, mutations du gène S baisse de l’antigénicité HBs1 et échappement vaccinal2. Impact de santé publique de l’émergence de ces mutants chez les patients traités à long terme comme les patients infectés par le VIH 1Torresi J, J clinc virol Kamili S, Hepatol")
105
S Gene Mutations (1) S120, S145 S gene mutations P120T/S, G145R/K/A described as conferring vaccine failure1,2 Associated with Pol mutations in position 128, 153, 181, 191 Figure. Incidence of S Gene Mutations over Follow-up % We also analysed S gene mutations. Mutations at position 120 and 145 have been previously associated with HBV vaccine failure. These mutations can be induced by Pol mutations on position 128, 153, 181 and 191. The prevalence of 120 and 145 mutations at inclusion was under 6% but steadily increased during the 3-year follow-up to almost 12% at a 2.1% person year rate, mostly driven by the emergence of P120S and G145R. Just as a reminder, these mutations are associated with Pol mutations at position 128 and 153. M12 M36 n = 186 Incidence S gene mutations (positions 120, 145) = 2.1% p∙y 1Carman, et al. Lancet Tian J, et al. J clin Microbiol 2007.
 = 2.1% p∙y. 1Carman, et al. Lancet Tian J, et al. J clin Microbiol")
106
S Gene Mutations (2) S164, S195, S196 E164D + I195M (associated with triple Pol mutations): recently described as responsible for infection in vaccinated chimpanzees1 Prevalence at baseline: 18.8% Incidence: 1.8 p∙y Mutations at position 164, 195, 196 conferring a decrease in HBsAg antigenicity2 Prevalence at baseline: W196L = 7.1%, E164D = 19.3%, I195M = 56.9% Incidence: W196L = 1.5% p∙y, E164D = 1.9% p∙y, I195M = 7.5% p∙y Among S gene mutations, E164D + I195M has recently been associated with HBV infection in vaccinated chimpanzees, and our colleague Dr. Saleem Kamili will hopefully tell us more about that tomorrow. The prevalence of this association in our cohort is as high as 18.8% with a yearly incidence of 1.8/100 patient-years. Other mutations at position 164, 195 and 196 have also been described as conferring a decrease in HBsAg antigenicity. The prevalence of I195M at inclusion is rather high and continues to increase during follow-up. All these mutations are associated with Pol mutations at position 173 or 204, emerging after exposure to lamivudine. 1Kamili, et al. Hepatol Torresi, et al. 2002
: recently described as responsible for infection in vaccinated chimpanzees1. Prevalence at baseline: 18.8% Incidence: 1.8 p∙y. Mutations at position 164, 195, 196 conferring a decrease in HBsAg antigenicity2. Prevalence at baseline: W196L = 7.1%, E164D = 19.3%, I195M = 56.9% Incidence: W196L = 1.5% p∙y, E164D = 1.9% p∙y, I195M = 7.5% p∙y. Among S gene mutations, E164D + I195M has recently been associated with HBV infection in vaccinated chimpanzees, and our colleague Dr. Saleem Kamili will hopefully tell us more about that tomorrow. The prevalence of this association in our cohort is as high as 18.8% with a yearly incidence of 1.8/100 patient-years. Other mutations at position 164, 195 and 196 have also been described as conferring a decrease in HBsAg antigenicity. The prevalence of I195M at inclusion is rather high and continues to increase during follow-up. All these mutations are associated with Pol mutations at position 173 or 204, emerging after exposure to lamivudine. 1Kamili, et al. Hepatol Torresi, et al")
107
Co-infection VIH-VHB: 2- Nouveaux marqueurs d’efficacité
Rare séroconversion HBe ou HBs sous nucléos(t)ides malgré HBV-DNA<12UI/mL autres marqueurs prédictifs de séroconversion? cccDNA: très corrélé à la clearance HBs clearance sous ADV (mono-VHB), mais mesuré dans le foie…1 quantification HBsAg : bon marqueur de la clearance HBs sous PegIFN (mono-VHB)2,3 Quantification HBe: encore débattue Un travail rétrospectif sur 36 patients sous TDF5 Décroissance HBs lente et inconstante (3 baisses rapides perte HBs) Besoin d’évaluation dans le contexte VIH 1Werle-Lapostolle B, et al. Gastroenterol 2004; 2Brunetto MR, et al. Hepatol 2009; 3Moucari R, et al. Hepatol ; 5Thibault V. et al, CROI 2009
ides malgré HBV-DNA<12UI/mL autres marqueurs prédictifs de séroconversion cccDNA: très corrélé à la clearance HBs clearance sous ADV (mono-VHB), mais mesuré dans le foie…1. quantification HBsAg : bon marqueur de la clearance HBs sous PegIFN (mono-VHB)2,3. Quantification HBe: encore débattue. Un travail rétrospectif sur 36 patients sous TDF5. Décroissance HBs lente et inconstante (3 baisses rapides perte HBs) Besoin d’évaluation dans le contexte VIH. 1Werle-Lapostolle B, et al. Gastroenterol 2004; 2Brunetto MR, et al. Hepatol 2009; 3Moucari R, et al. Hepatol ; 5Thibault V. et al, CROI")
108
Co-infection VIH-VHC: 3- Hépatite C aigue (1): épidémiologie ?
Europe: 951 cas – UK3,4 552 – Allemagne5 157 – France6,7 117 – Pays Bas8 81 – Suisse9 23 – Italie10 21 USA:1,2 54 cas Australie:11 28 cas

109
Co-infection VIH-VHC: 3- Hépatite C aigue (2): traitement ?
Ribavirine nécessaire? Mieux si S48? RVR RVS 100 90 p=0.067* p=0.042* 80 p=0.499* 70 G1 ou 4 (n=27) G ou 3 (n=7) G 1 ou 4 (n=27) G 2 ou 3 (n=7) PegIFN + RBV (n=21) PegIFN seul (n=15) PegIFN + RBV (n=21) PegIFN seul (n=15) 60 Patients avec RVR/RVS (%) 50 24 semaines (n=27) 48 semaines (n=9) 24 semaines (n=27) 48 semaines (n=9) 40 30 20 10 16 Génotype Ribavirine Durée de traitement Vogel et al. Antivir Ther 2006;11:1097–1101
 G ou 3 (n=7) G 1 ou 4 (n=27) G 2 ou 3 (n=7) PegIFN + RBV (n=21) PegIFN seul (n=15) PegIFN + RBV (n=21) PegIFN seul (n=15) 60. Patients avec RVR/RVS (%) semaines (n=27) 48 semaines (n=9) 24 semaines (n=27) 48 semaines (n=9) Génotype. Ribavirine. Durée de traitement. Vogel et al. Antivir Ther 2006;11:1097–1101.")
110
Co-infection VIH-VHC: 4- Nouvelles molécules
Télaprévir ? Bocéprévir ?

111
Co-infection VIH-hépatites: 5- Accès à la transplantation / thérapeutiques innovantes
CHC = “a harbinger of an emerging problem for persons living with hepatic co-infection in regions with access to potent ARV regimen” dixit M. Sulkowski (J Hepatol 2009) Très bon pronostic si VHB : 100% de survie à 3 ans1 Besoin +++ d’évaluer les traitements innovants (sorafénib – interactions ARV ?, probablement non, sauf NFV - RAL) quand TH impossible2 1Tatteo M, AIDS Deeken JF, Curr Opin Oncol 2009
 Très bon pronostic si VHB : 100% de survie à 3 ans1. Besoin +++ d’évaluer les traitements innovants (sorafénib – interactions ARV , probablement non, sauf NFV - RAL) quand TH impossible2. 1Tatteo M, AIDS Deeken JF, Curr Opin Oncol")
112
Co-infection VIH-hépatites: 5- Challenges pour les pays à ressources limitées
Accès au screening VHB-VHC fait partie des recommandations OMS, mais en pratique peu fait (coût ?) Accès à la vaccination (VHB) coût du vaccin et efficacité faible car immunodépression souvent profonde Accès aux traitements VHB TDF recommandé (OMS 2008) mais pas accessible en 1ère ligne dans de nombreux pays VHC illusoire hors essais… Accès à la PTME-hépatites VHB Ig anti VHB trop chère, évaluation TDF + 3TC ++ (3TC efficace) Accès au traitement maladies terminales du foie impossible = prévention +++
 Accès à la vaccination (VHB) coût du vaccin et efficacité faible car immunodépression souvent profonde. Accès aux traitements. VHB TDF recommandé (OMS 2008) mais pas accessible en 1ère ligne dans de nombreux pays. VHC illusoire hors essais… Accès à la PTME-hépatites. VHB Ig anti VHB trop chère, évaluation TDF + 3TC ++ (3TC efficace) Accès au traitement maladies terminales du foie impossible = prévention +++")
Présentations similaires