Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
NOUVELLES STRATÉGIES THÉRAPEUTIQUES DE LA MALADIE D’ALZHEIMER
Serge Gauthier, MD, FRCPC Centre McGill d’études sur le vieillissement, Montréal, Canada

2
PLAN DE PRESENTATION Histoire naturelle de la MA
Prise en charge actuelle aux divers stades Espoirs de stabilisation/prévention

3
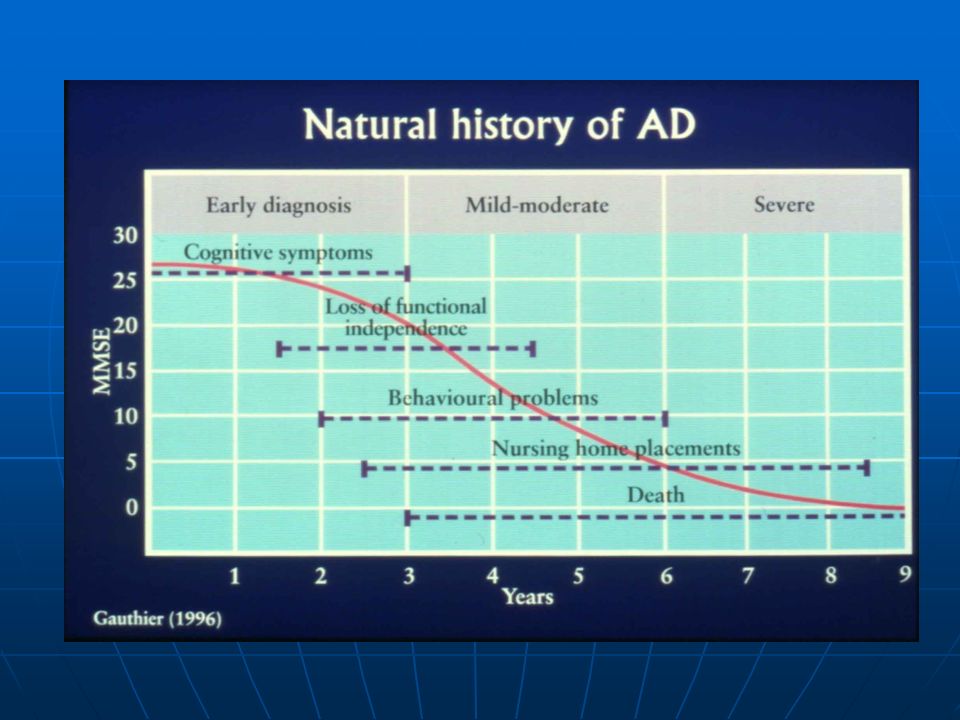
PROGRESSION DES SYMPTÔMES DE LA MALADIE D’ALZHEIMER
Fonction cognitive Autonomie fonctionnelle Motricité Détérioration La progression de la maladie d'Alzheimer, qui s’échelonne sur de nombreuses années, est souvent classée, soit d'intensité légère (stade précoce), modérée (stade intermédiaire) sévère ou avancée (stade tardif). Les symptômes varient selon les personnes et le moment, mais cette diapositive illustre leur mode typique de présentation au cours de la progression de la maladie d'Alzheimer. Les premiers changements transitoires de l'humeur font peu à peu place à un déclin linéaire des capacités cognitives et fonctionnelles. On assiste ensuite à des symptômes neuropsychiatriques dérangeants qui évoluent en dents de scie et sont suivis progressivement de rigidité, d'akinésie et d'instabilité de la démarche. Référence : Lovestone S, Gauthier S. Management of dementia. Martin Dunitz Ltd, Londres, 2001. Humeur Comportement Années Lovestone & Gauthier. Martin Dunitz Ltd, Londres, 2001
, modérée (stade intermédiaire) sévère ou avancée (stade tardif). Les symptômes varient selon les personnes et le moment, mais cette diapositive illustre leur mode typique de présentation au cours de la progression de la maladie d Alzheimer. Les premiers changements transitoires de l humeur font peu à peu place à un déclin linéaire des capacités cognitives et fonctionnelles. On assiste ensuite à des symptômes neuropsychiatriques dérangeants qui évoluent en dents de scie et sont suivis progressivement de rigidité, d akinésie et d instabilité de la démarche. Référence : Lovestone S, Gauthier S. Management of dementia. Martin Dunitz Ltd, Londres, Humeur. Comportement. Années. Lovestone & Gauthier. Martin Dunitz Ltd, Londres,")
5
Histoire naturelle de la maladie d’Alzheimer Gauthier S
Histoire naturelle de la maladie d’Alzheimer Gauthier S. Alzheimer’s & Dementia 2006, 2, Suppl 1, S1-S2 Normal TCL Démence Perte d’autonomie Sévérité Symptômes comportemen-taux Soins prolongés Décès Temps((ans))
)")
6
PLAN DE PRESENTATION Histoire naturelle de la MA
Prise en charge actuelle aux divers stades Espoirs de stabilisation/prévention

7
PRISE EN CHARGE DE LA MA Education sur la maladie
Mandat (“personne de confiance”), procuration générale, testament Sécurité au volant Sécurité à domicile Santé de l’aidant(e) Médications symptomatiques
, procuration générale, testament. Sécurité au volant. Sécurité à domicile. Santé de l’aidant(e) Médications symptomatiques.")
8
MÉDICATIONS SYMPTOMATIQUES
Antidépresseurs (ex. citalopram) Inhibiteurs de la cholinesterase (IC: donepezil, rivastigmine, galantamine) Antagoniste récepteurs NMDA (memantine) Antipsychotiques atypiques (risperidone, olanzapine, quetiapine)
 Inhibiteurs de la cholinesterase (IC: donepezil, rivastigmine, galantamine) Antagoniste récepteurs NMDA (memantine) Antipsychotiques atypiques (risperidone, olanzapine, quetiapine)")
10
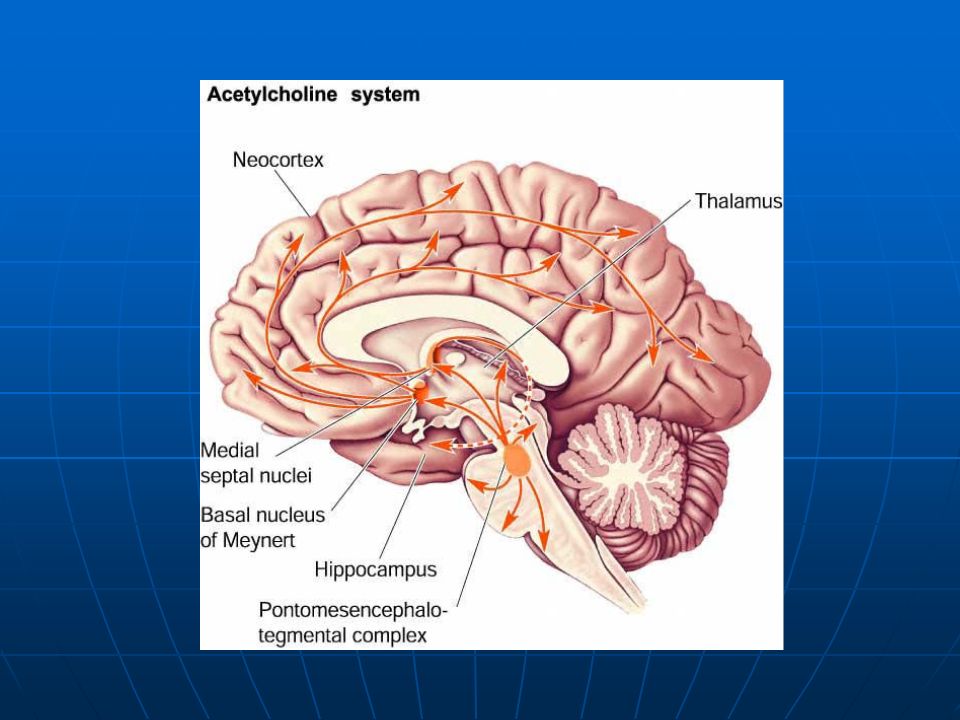
Déficit cholinergique dans la démence vasculaire de type sous-cortical
With permission from Oxford University Press. Selden NR, et al. Brain. 1998;121 : Swartz RH, Black SE. J Neurol Sci. 2002; (C) : 281.
 : 281.")
11
IC Donepezil Rivastig- mine Galanta-mine Demi-vie & posologie
70-80 hrs QD 0.6-2 hrs BID or patch QD 7-8 hrs QD Enzymes inhibés AChE AChE & BuChE Effets Nicotiniques + +++

12
Timbre cutané de rivastigmine

13
EFECTS COGNITIFS DES IC: EXEMPLE DU DONEPEZIL
Winblad et al, Neurology 2001, 57, 52 36 24 12 p=0.053 P<0.001 p=0.019 p=0.001 Amélioration Déclin donepezil n= (135) placebo n= (137) Visite finale -3 -2.5 -2 -1.5 -1 -0.5 0.5 1 1.5 2 2.5 Semaines Comparaison début et fin (±ES) Donepezil Placebo
 placebo n= (137) Visite finale Semaines. Comparaison début et fin (±ES) Donepezil. Placebo.")
14
EFFETS SECONDAIRES DES IC
Nausées, vômissements, diarrhées Bradycardie, syncope Crampes aux membres inférieurs Insomnie; trouble du sommeil paradoxal (REM Behavior Disorder)
")
15
EFFETS COGNITIFS DE LA MEMANTINE EN MONOTHÉRAPIE
Placebo Memantine (20 mg/day) *p=0.002 (OC) **p= (OC) -12 -10 -8 -6 -4 -2 2 4 8 12 16 20 24 28 Semaines Différence au SIB Improvement Worsening * n=126 n=119 n=107 n=117 n=96 n=83 n=106 ** Improvements seen with memantine on function and global impression, as indicated by CIBIC-plus and ADCS-ADLsev scores, were consistent with a favourable effect of memantine on cognition. This slide shows the effect on cognition, as measured by SIB score. The graph shows mean change ( SEM) from baseline in SIB scores during 28 weeks of treatment with either memantine (20 mg/day) or placebo, OC analysis. The memantine group was significantly superior to placebo in cognitive function as measured by SIB. The difference between the groups was already significant at 12 weeks and was maintained throughout the study. After 28 weeks of treatment, the reduction in SIB scores in the memantine group was 4.5 points, compared with 10.2 points in the placebo group (p=0.002, OC analysis). Reisberg et al 2003; H. Lundbeck A/S,
 *p=0.002 (OC) **p= (OC) Semaines. Différence au SIB. Improvement. Worsening. * n=126. n=119. n=107. n=117. n=96. n=83. n=106. ** Improvements seen with memantine on function and global impression, as indicated by CIBIC-plus and ADCS-ADLsev scores, were consistent with a favourable effect of memantine on cognition. This slide shows the effect on cognition, as measured by SIB score. The graph shows mean change ( SEM) from baseline in SIB scores during 28 weeks of treatment with either memantine (20 mg/day) or placebo, OC analysis. The memantine group was significantly superior to placebo in cognitive function as measured by SIB. The difference between the groups was already significant at 12 weeks and was maintained throughout the study. After 28 weeks of treatment, the reduction in SIB scores in the memantine group was 4.5 points, compared with 10.2 points in the placebo group (p=0.002, OC analysis). Reisberg et al 2003; H. Lundbeck A/S,")
16
COMBINAISON DONEPEZIL ET MEMANTINE
Tariot et al., JAMA 2004

17
EFFETS SECONDAIRES DE LA MEMANTINE
Excrété par les reins (attention à la fonction rénales) Confusion, agitation (peut être lié à la dose) Hallucinations visuelles
 Confusion, agitation (peut être lié à la dose) Hallucinations visuelles.")
18
Histoire naturelle de la MA et interventions pour chaque stade
Normal Antidépresseurs IC TCL Sévérité des symptômes IC Memantine Diagnostic de MA Memantine; IC Neuroleptiques atypiques Perte d’autonomie Memantine; IC Neuroleptiques atypiques Troubles du comportement Hébergement Décès Temps (ans) )
 )")
19
A SURVEILLER: Dimebon (“le médicament russe”!)
ADAS-Cog (n=89) (n=94) Doody RS, Gavrilova SI, Sano M, et al. Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer's disease: a randomised, double-blind, placebo-controlled study. Lancet 2008; 372 (9634): 207–215. BACKGROUND: Although treatments for Alzheimer's disease sometimes improve cognition, functional ability, or behaviour compared with baseline levels, such improvements are inconsistent across studies and measures, and effects diminish over time. More effective treatments are needed. We assessed the safety, tolerability, and efficacy of dimebon in the treatment of patients with mild-to-moderate Alzheimer's disease. METHODS: We enrolled 183 patients with mild-to-moderate Alzheimer's disease (mini-mental state examination [MMSE] scores 10-24) at 11 sites in Russia. Patients were randomly assigned by a computer-generated randomisation scheme to receive oral dimebon, 20 mg three times a day (60 mg/day [n=89]), or matched placebo (n=94). Other antidementia drugs were not allowed. The primary outcome measure assessed cognition, the difference in mean change from baseline to week 26, or last completed observation on the cognitive subscale of the Alzheimer's disease assessment scale (ADAS-cog). All patients and study personnel were blinded throughout the study. We compared dimebon with placebo with an intention-to-treat analysis, with last observation carried forward (ITT-LOCF) imputation. Analyses were repeated on the fully evaluable population, defined as all patients in the intention-to-treat population who had an ADAS-cog at week 26 and at least 80% compliance. 134 patients (68 in dimebon group, 66 in placebo group) enrolled in the 6-month blinded extension phase of the study. This trial is registered with Clinicaltrials.gov, number NCT FINDINGS: 155 (85%) patients completed the trial (78 [88%] in dimebon group, 77 [82%] in placebo group). Treatment with dimebon resulted in significant benefits in ADAS-cog compared with placebo (ITT-LOCF) at week 26 (mean drug-placebo difference -4.0 [95% CI to -2.28]; p<0.0001). Results of the ITT-LOCF and the evaluable population analyses were much the same for all measures. Patients given dimebon were significantly improved over baseline for ADAS-cog (mean difference -1.9 [-2.92 to -0.85]; p=0.0005). Dimebon was well tolerated: dry mouth and depressed mood or depression were the most common adverse events associated with dimebon (12 [14%] patients for each symptom by week 26). The percentage of patients who had adverse events in the two groups did not differ. INTERPRETATION: Dimebon was safe, well tolerated, and significantly improved the clinical course of patients with mild-to-moderate Alzheimer's disease. Doody RS, et al. Lancet 2008; 372 (9634): 207–215 19
 (n=94) Doody RS, Gavrilova SI, Sano M, et al. Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer s disease: a randomised, double-blind, placebo-controlled study. Lancet 2008; 372 (9634): 207–215. BACKGROUND: Although treatments for Alzheimer s disease sometimes improve cognition, functional ability, or behaviour compared with baseline levels, such improvements are inconsistent across studies and measures, and effects diminish over time. More effective treatments are needed. We assessed the safety, tolerability, and efficacy of dimebon in the treatment of patients with mild-to-moderate Alzheimer s disease. METHODS: We enrolled 183 patients with mild-to-moderate Alzheimer s disease (mini-mental state examination [MMSE] scores 10-24) at 11 sites in Russia. Patients were randomly assigned by a computer-generated randomisation scheme to receive oral dimebon, 20 mg three times a day (60 mg/day [n=89]), or matched placebo (n=94). Other antidementia drugs were not allowed. The primary outcome measure assessed cognition, the difference in mean change from baseline to week 26, or last completed observation on the cognitive subscale of the Alzheimer s disease assessment scale (ADAS-cog). All patients and study personnel were blinded throughout the study. We compared dimebon with placebo with an intention-to-treat analysis, with last observation carried forward (ITT-LOCF) imputation. Analyses were repeated on the fully evaluable population, defined as all patients in the intention-to-treat population who had an ADAS-cog at week 26 and at least 80% compliance. 134 patients (68 in dimebon group, 66 in placebo group) enrolled in the 6-month blinded extension phase of the study. This trial is registered with Clinicaltrials.gov, number NCT FINDINGS: 155 (85%) patients completed the trial (78 [88%] in dimebon group, 77 [82%] in placebo group). Treatment with dimebon resulted in significant benefits in ADAS-cog compared with placebo (ITT-LOCF) at week 26 (mean drug-placebo difference -4.0 [95% CI to -2.28]; p<0.0001). Results of the ITT-LOCF and the evaluable population analyses were much the same for all measures. Patients given dimebon were significantly improved over baseline for ADAS-cog (mean difference -1.9 [-2.92 to -0.85]; p=0.0005). Dimebon was well tolerated: dry mouth and depressed mood or depression were the most common adverse events associated with dimebon (12 [14%] patients for each symptom by week 26). The percentage of patients who had adverse events in the two groups did not differ. INTERPRETATION: Dimebon was safe, well tolerated, and significantly improved the clinical course of patients with mild-to-moderate Alzheimer s disease. Doody RS, et al. Lancet 2008; 372 (9634): 207–")
20
PLAN DE PRESENTATION Histoire naturelle de la MA
Prise en charge actuelle aux divers stades Espoirs de stabilisation/prévention

21
FACTEURS DE RISQUE POUR LA MA
Age Sexe Faible niveau de scolarité Histoire familiale de MA Génotype ApoE ε4 Hypertension systolique âge 40-60 Diabète

22
FACTEURS DE PROTECTION POUR LA MA
Scolarité plus élevée Loisirs (jardinage) Réseaux sociaux (?mariage) Vin rouge en modération (Bordeaux) Diète méditerranéenne; poisson; ω3 AINS Statines
 Réseaux sociaux ( mariage) Vin rouge en modération (Bordeaux) Diète méditerranéenne; poisson; ω3. AINS. Statines.")
23
Rx ANTI-AMYLOIDE A L’ESSAI POUR LA MA LÉGÈRE
Inhibition de la fibrillogénèse (Tramiprosate ou Alzhemed) –> VIVIMIND en vente libre Inhibition de la gamma-sécrétase & AINS (R-flurbiprofen or Flurizan) -> abandonné Anticorps monoclonaux contre β-amyloide Inhibiteurs γ secretase
 –> VIVIMIND en vente libre. Inhibition de la gamma-sécrétase & AINS. (R-flurbiprofen or Flurizan) -> abandonné. Anticorps monoclonaux contre β-amyloide. Inhibiteurs γ secretase.")
24
DEVIS POUR PROUVER MODIFICATION DE LA PATHOLOGIE AVEC MA
+ médicament sous étude Doses stables D’un IC et/ou memantine Performance clinique + placebo 1) stat sig at t1 2) stat sig between-group difference in performance due to either symptomatic or structural effect, 3)or to a combination of both The goal of the experiment is not to distinguish among the 3 but to determine whether the treatment has been responsible for this benefit, in any part, by altering the coiurse of the dementing process. Structural effect: Group 2 responds but loss relative to group 1, but the effect sustained Symptomatic effect: Group 2 not only response, but “catches up” with group 1 -16 78 Temps (semaines)
 stat sig at t1. 2) stat sig between-group difference in performance due to either symptomatic or structural effect, 3)or to a combination of both. The goal of the experiment is not to distinguish among the 3. but to determine whether the treatment has been responsible for this benefit, in any part, by altering the coiurse of the dementing process. Structural effect: Group 2 responds but loss relative to group 1, but the effect sustained. Symptomatic effect: Group 2 not only response, but catches up with group Temps (semaines)")
25
Cognition - ADAS-cog p=0.860 Preliminary analysis 25

26
VARIABLES BIOLOGIQUES
MA Normal tMTL width = 2.6 mm tMTLwidth = 14.6 mm Speaker notes Comparison of hippocampal size using the thinnest medial temporal lobe (tMTL) width between a 68-year-old woman with Alzheimer’s disease (AD) and a 67-year-old woman normal control. ©Gao FQ and Black SE, Sunnybrook & Women’s College Health Sciences Centre, U of T
 width between a 68-year-old woman with Alzheimer’s disease (AD) and a 67-year-old woman normal control. ©Gao FQ and Black SE, Sunnybrook & Women’s College Health Sciences Centre, U of T.")
27
% personnes n’ayant pas atteint X
DEVIS DE SURVIE 100 Rx nouveau % personnes n’ayant pas atteint X 94 Placebo X Temps

28
Histoire naturelle de la MA et interventions futures
Execices physiques; poisson, vin rouge Entraînement cognitif; Rx anti-amyloide ou statines basé sur âge et genotypes Normal Antidépresseurs IC TCL Sévérité des symptômes IC Memantine Diagnostic de MA Memantine; IC Neuroleptiques atypiques Perte d’autonomie Memantine; IC Neuroleptiques atypiques Troubles du comportement Hébergement Décès Temps (ans) )
 )")
Présentations similaires

 éduquer le patient âgé?>")

















