Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
CAS CLINIQUE I.SIALA, N.JEMAL, F.CHARFI R.JLIDI, R.TOUNSI.
5ème Congres GETOM Hammamet le 02/07/2011

2
OBSERVATION Homme âgé de 65 ans. Douleurs lombosacrées
troubles de la marche évoluant depuis quelques jours.

3
A l ’examen déficit L5 et S1 bilatéral. Réflexes achyléens abolis. réflexes rotuliens vifs marche spastique. VS GB 11200

11
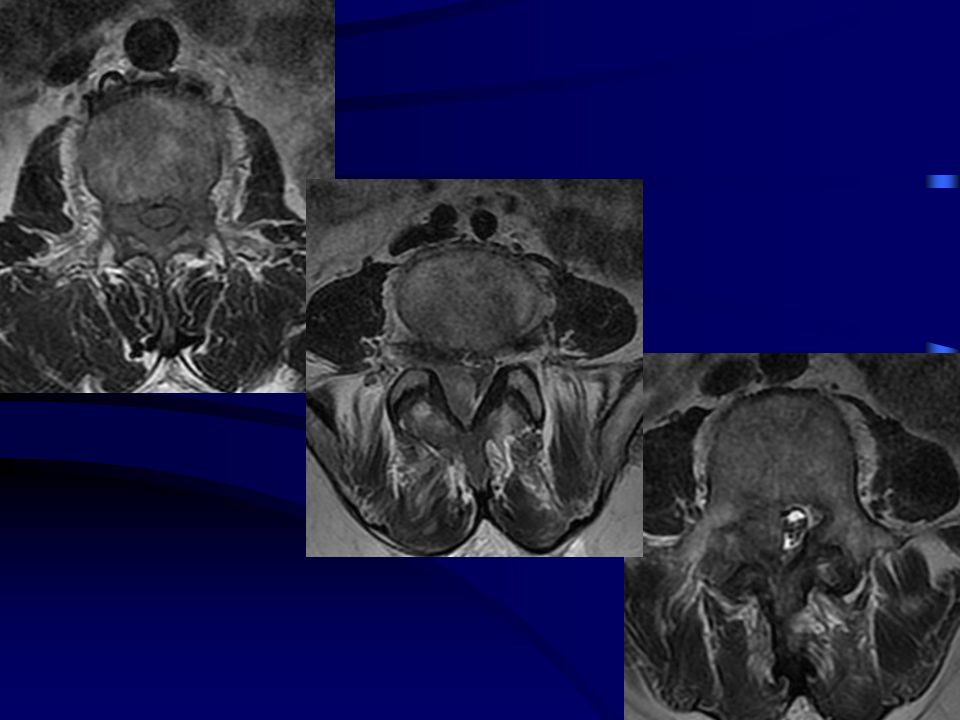
avant injection après injection

14
Quel serait votre diagnostic?

15
TRAITEMENT CHIRURGICAL
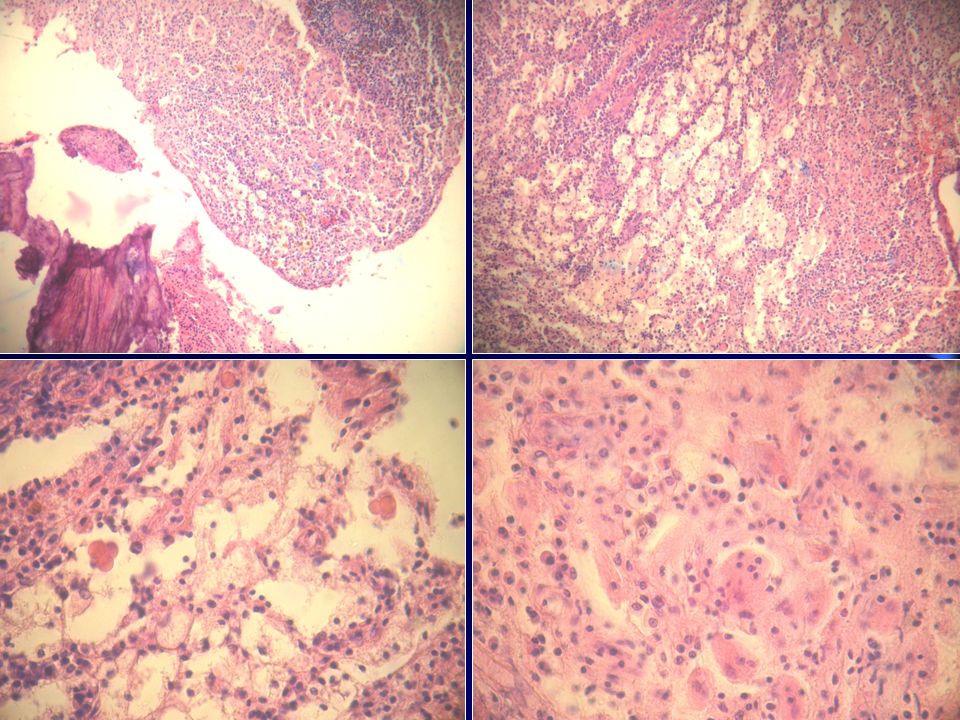
laminectomie L1-L5. Libération du fourreau dural prélèvements: étude bactériologique et anatomopathologique.

18
PS100 + CD1a -

19
PS100 + CD1a -

20
Maladie de Rosaï Dorfman (Destombes Rosaï Dorfman)
CD1a CD CD CD CD CD EMA PS PS100 +

21
Maladie de Rosai Dorfman
Diagnostic Maladie de Rosai Dorfman

22
Maladie de Rosai Dorfman
Histiocytose non langheransienne rare et ubiquitaire. Décrite pour la première fois par Rosai Dorfman en 1969. Age moyen: 20ans sexe masculin.

23
Pathogénie inconnue: virale/ EBV HHV 6 immunologique. Pas de facteurs héréditaires ni de cas familiaux. Cliniquement: 85° des patients: lymphadénopathie cervicale bilatérale massive et indolore. Multifocale: axillaire, inguinale ou médiastinale.

24
Fièvre intermittente et altération de l’ état général.
Bilan biologique: VS accélérée. Hypergammaglobulinémie d ’allure polyclonale. Anémie hypochrome microcytaire modérée. Hyperleucocytose: inconstante.

25
43% des patients: atteinte extra ganglionnaire.
Voies aériennes supérieures, orbite, glandes salivaires, peau. Os, atteinte rénale , pulmonaire. Atteinte osseuse décrite pour la première fois en 1985 par Lewin et all: atteinte du premier métacarpien chez un enfant de 7 ans.

26
L ’atteinte osseuse isolée est rare.
tiers inférieur du radius métacarpe, os temporal., crâne vertèbres, cotes, os de la face. Généralement: lésions lytiques. Lésions ostéocondensantes exceptionnelles Diagnostic anatomopathologique Diagnostic différentiel : tumeurs à cellules géantes, histiocytose X lymphomes, malakoplakie.

27
Am J Surg Pathol 2010; 34: 1324-1333) 8 femmes, 7 hommes
Primary Rosai-Dorfman Disease of Bone A Clinicopathilogic Study of 15 Cases Elizabeth G. Demicco, Andrew E. Rosenberg, Johannes Bjornsson and all Am J Surg Pathol 2010; 34: ) Série de 15 cas 8 femmes, 7 hommes 3 à 56 ans (27 ans) Tibia, fémur, clavicule, voûte, maxillaire, calcanéum, phalanges, métacarpes et sacrum
 Série de 15 cas. 8 femmes, 7 hommes. 3 à 56 ans (27 ans) Tibia, fémur, clavicule, voûte, maxillaire, calcanéum, phalanges, métacarpes et sacrum.")
28
Localisations osseuses rares < 10%
Atteinte osseuse primaire : quelques cas: Métaphyse Lytique Centro-médullaire Bien limitée

29
Radiologiquement : Diagnostic différentiel: métastase, ostéomyélite, granulome éosinophile, TCG, lymphome…. Traitement: curetage ou résection, radiothérapie / chimiothérapie Pronostic bon Chirurgie: meilleur traitement

30
Rosai-Dofman Disease in Neuroradiology : Imaging Findings in a Series of 10 Patients
Osama A. Roslan, Dawid Schellingerhout, Gregory N. Fuller, Leena M. Ketonen AJR 2011; 196: W187-W193

31
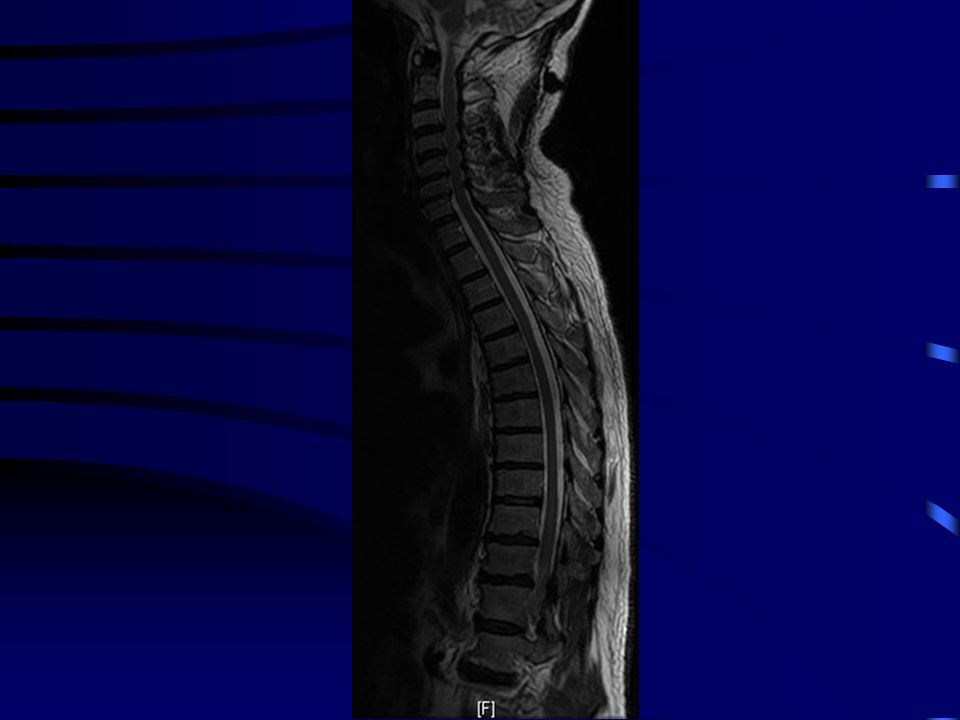
L’attente du SNC est rare < 5%
Seulement 50 cas ont été rapportés Atteinte du crane 2 à 3 fois plus fréquente que celle du rachis Généralement, diagnostiquées comme méningiomes avec présence des masses à large base d’implantation durale rehaussées après injection de PDC Au niveau du rachis : l’atteinte vertébrale est souvent prise pour métastase Diagnostic histologique

32
Conclusion Maladie rare Diagnostic histologique
Atteinte multifocale syndrome ou métachrone

33
2-Rosai-Dorfman disease of the central nervous system
1-Rosai-Dofman Disease in Neuroradiology : Imaging Findings in a Series of 10 Patients Osama A. Roslan, Dawid Schellingerhout, Gregory N. Fuller, Leena M. Ketonen AJR 2011; 196: W187-W193 2-Rosai-Dorfman disease of the central nervous system P Purav, K Ganapathy, VS Mallikarjuna and all Journal of Clinical Neuroscience (2005) 12(6), 3-Rosai-Dorfman disease with extensive extra nodal involvement Dhiraj Baruah, Saurabh Guleria, Tripti Chandra and all European Journal of Radiology Extra 62 (2007) 31-33 4-Extranodal Rosai-Dorfman disease with multiple spinal lesions : a rare presentation Arun Bhandari, Pankaj R. Patel, Mukesh P. Patel Surgical Neurology 65 (2006) Spine 5-Giant intracranial Rosai-Dorfman disease Ugur Ture, Askin Seker, Suheyla Uyar Boskurt and all Journal of Clinical Neuroscience (2004) 11(5), 6-Primary Rosai-Dorfman Disease of Bone A Clinicopathilogic Study of 15 Cases Elizabeth G. Demicco, Andrew E. Rosenberg, Johannes Bjornsson and all Am J Surg Pathol 2010; 34: )
 12(6), Rosai-Dorfman disease with extensive extra nodal involvement. Dhiraj Baruah, Saurabh Guleria, Tripti Chandra and all. European Journal of Radiology Extra 62 (2007) Extranodal Rosai-Dorfman disease with multiple spinal lesions : a rare presentation. Arun Bhandari, Pankaj R. Patel, Mukesh P. Patel. Surgical Neurology 65 (2006) Spine 5-Giant intracranial Rosai-Dorfman disease. Ugur Ture, Askin Seker, Suheyla Uyar Boskurt and all. Journal of Clinical Neuroscience (2004) 11(5), Primary Rosai-Dorfman Disease of Bone A Clinicopathilogic Study of 15 Cases. Elizabeth G. Demicco, Andrew E. Rosenberg, Johannes Bjornsson and all. Am J Surg Pathol 2010; 34: )")
Présentations similaires