Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
INFARCTUS DU VENTRICULE DROIT CAS CLINIQUE
Charles BER DESC Réanimation Médicale Nice – 14 au 18 juin 2004

2
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
Homme 77 ans Troubles du sommeil et insomnies STILNOX®(Médecin traitant) Consultation pneumologique
 Consultation pneumologique.")
3
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
ANTECEDENTS Insuffisance respiratoire chronique - emphysème (Bronchodual®) - suivi pneumologique régulier PNO gauche (traumatisme en 1948) PNO droit spontané en 1951 HTA (Zestorétic®) Hypercholestérolémie (Lanzor®) Tabagisme (30 PA)
 - suivi pneumologique régulier. PNO gauche (traumatisme en 1948) PNO droit spontané en HTA (Zestorétic®) Hypercholestérolémie (Lanzor®) Tabagisme (30 PA)")
4
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
INTERROGATOIRE Majoration dyspnée (marche lente sur terrain plat) depuis deux semaines,stade 3 de la NYHA. Douleurs thoraciques (brûlures) intermittentes avec irradiation dans les deux bras. Pas de modification en inspiration profonde.
 depuis deux semaines,stade 3 de la NYHA. Douleurs thoraciques (brûlures) intermittentes avec irradiation dans les deux bras. Pas de modification en inspiration profonde.")
5
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
EXAMEN CLINIQUE. Fréquence cardiaque: 80 battements/mn, régulier TA = 130/70 Auscultation cardiaque: sans particularité Auscultation pulmonaire: absence de crépitant, rares râles sibilants, diminution du MV dans les apex Pas d’œdème MI, pas de turgescence jugulaire Présence d’une hépatosplénomégalie

6
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
EXAMENS PARACLINIQUES EFR: TVO sévère (VEMS à 840 ml) sans réversibilité Gazométrie artérielle en air ambiant: PO2 = 77 mm Hg PCO2 = 39,6 mm Hg pH = 7,39 RP: distension thoracique, pas de surcharge vasculaire, pas de pneumopathie
 sans réversibilité. Gazométrie artérielle en air ambiant: PO2 = 77 mm Hg. PCO2 = 39,6 mm Hg. pH = 7,39. RP: distension thoracique, pas de surcharge vasculaire, pas de pneumopathie.")
7
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
Pas de décompensation respiratoire Pas d’étiologie pulmonaire évidente à cette dyspnée CONSULTATION CARDIOLOGIQUE

8
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
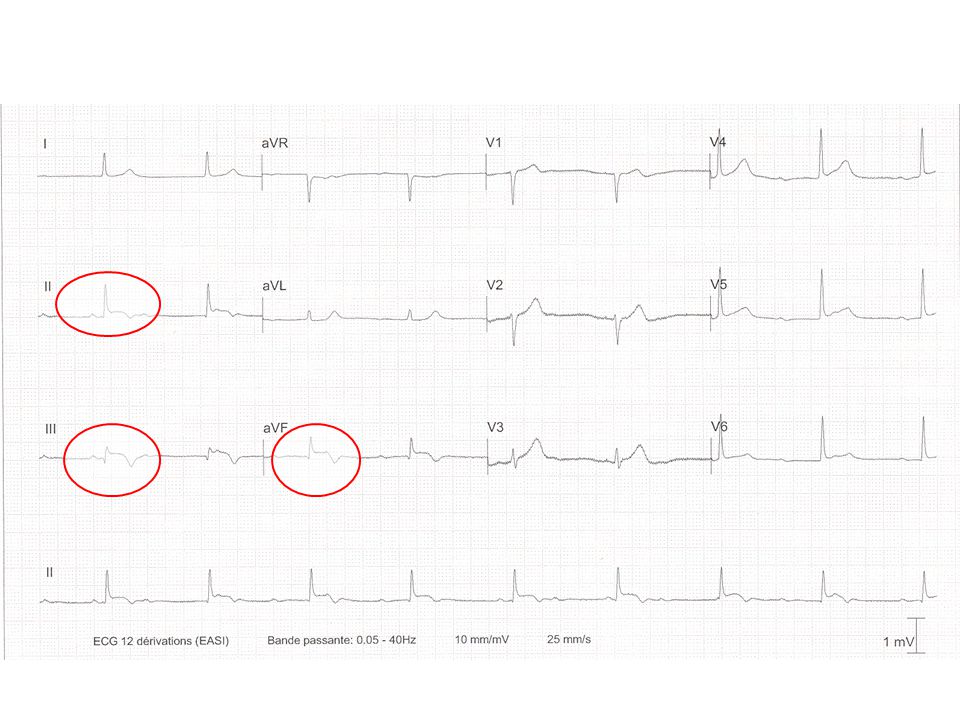
ADMISSION EN CARDIOLOGIE (1) Dégradation clinique notable Hypotension artérielle (80 à 90 mm Hg) Signes de décompensation droite (jugulaires turgescentes, hépatomégalie) Oligurie Signes électriques Bradycardie sinusale Sus-décalage en DII, DIII, VF
 Dégradation clinique notable. Hypotension artérielle (80 à 90 mm Hg) Signes de décompensation droite (jugulaires turgescentes, hépatomégalie) Oligurie. Signes électriques. Bradycardie sinusale. Sus-décalage en DII, DIII, VF.")
11
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
ADMISSION EN CARDIOLOGIE (2) Biologie Troponine = 21,8 CPK = 313 Créatininémie = 243 µmol/L Echocardiographie Akinésie inférieure limitée Akinésie bord libre du VD Dilatation modérée des cavités droites Fonction systolique du VG conservée avec pressions de remplissage basses Pas d’épanchement péricardique
 Biologie. Troponine = 21,8. CPK = 313. Créatininémie = 243 µmol/L. Echocardiographie. Akinésie inférieure limitée. Akinésie bord libre du VD. Dilatation modérée des cavités droites. Fonction systolique du VG conservée avec pressions de remplissage basses. Pas d’épanchement péricardique.")
12
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
ADMISSION EN REANIMATION Persistance du choc avec signes droits (pic des CPK à 414 et de la troponine à 25) Pas de signes échographiques de défaillance gauche Anurie et insuffisance rénale aiguë
 Pas de signes échographiques de défaillance gauche. Anurie et insuffisance rénale aiguë.")
13
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
THERAPEUTIQUE Remplissage vasculaire conséquent Inotropes (Dobutamine puis Adrénaline) Coronarographie suivie d’angioplastie Épuration Extra-Rénale
 Coronarographie suivie d’angioplastie. Épuration Extra-Rénale.")
14
Réseau gauche discrètement athéromateux sans lésion serrée
CORONAIRE GAUCHE Réseau gauche discrètement athéromateux sans lésion serrée

15
CORONAIRE DROITE Occlusion coronaire droite, dominante, à son segment moyen Flux intra-coronaire lent malgré l’implantation de 2 stents couvrant la lésion + REOPRO Résultat non satisfaisant

16
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
EVOLUTION Amélioration très progressive du choc et des signes droits avec sevrage des catécholamines en 8 jours. Épuration extra-rénale poursuivie 5 jours au total. Succession de troubles du rythme BAV Luciani-Wenckebach Flutter

17
Bloc Auriculo-Ventriculaire

18
Périodes de Luciani - Wenckebach

19
Flutter

20
INFARCTUS VENTRICULE DROIT CAS CLINIQUE
EVOLUTION Sortie de réanimation 10 jours après son admission ECG: Q DIII, VF et hémibloc antérieur gauche Echographie confirme infarctus inférieur étendu au VD 6 mois après: TA = 140/90, Nce = 60 /mn, pas de signes d’insuffisance ventriculaire droite, pas de récidive douloureuse thoracique, pas d’ IVG, dyspnée stade 2 NYHA, normalisation de la fonction rénale.

21
INFARCTUS VENTRICULE DROIT DISCUSSION
ASPECTS CLINIQUES Entité clinique individualisée en 1974 par Cohn (1) Infarctus du VD: 30 à 40% des nécroses inférieures, 50% selon Kinch (2) hypotension Triade: absence œdème pulmonaire turgescence veines jugulaires Triade très spécifique des nécroses inférieures mais sensibilité faible 25%. (2, 3) 1 – Cohn JN, Guiha NH. Right ventricular infarction: clinical and hemodynamic features. Am J Cardiol 1974; 33: 2 – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: 3 – The Task Force of the Management of Acute Myocardial Infarction of the European Society of Cardiology. Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. European Heart Journal (2003) 24,
 Infarctus du VD: 30 à 40% des nécroses inférieures, 50% selon Kinch (2) hypotension. Triade: absence œdème pulmonaire. turgescence veines jugulaires. Triade très spécifique des nécroses inférieures mais. sensibilité faible 25%. (2, 3) 1 – Cohn JN, Guiha NH. Right ventricular infarction: clinical and hemodynamic features. Am J Cardiol 1974; 33: – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: – The Task Force of the Management of Acute Myocardial Infarction of the European Society of Cardiology. Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. European Heart Journal (2003) 24,")
22
INFARCTUS VENTRICULE DROIT DISCUSSION
ANATOMIE (2, 4) Artère coronaire droite – 90% Artère circonflexe – 10% 2 – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: 4 – Zimetbaum PJ, Josephson ME. Use of the Electrocardiogram in Acute Myocardial Infarction. N Engl J Med 2003;348:
 Artère coronaire droite – 90% Artère circonflexe – 10% 2 – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: – Zimetbaum PJ, Josephson ME. Use of the Electrocardiogram in Acute Myocardial Infarction. N Engl J Med 2003;348:")
23
INFARCTUS VENTRICULE DROIT DISCUSSION
PHYSIOPATHOLOGIE Occlusion de l’artère coronaire droite en amont de l’artère marginale du bord droit ou Occlusion de l’artère circonflexe lorsque le réseau gauche est dominant

24
INFARCTUS VENTRICULE DROIT DISCUSSION
PHYSIOPATHOLOGIE (2, 5, 6) NECROSE MYOCARDIQUE Altération de la fonction systolique Diminution du flux pulmonaire Diminution de la précharge du VD Diminution du débit cardiaque 2 – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: 5 – Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll Cardiol 2002; 40: 6 – Goldstein JA, Tweddell JS. Importance of left ventricular function and systolic ventricular interaction to right ventricular performance during acute right heart ischemia. J Am Coll Cardiol 1992;19:
 NECROSE MYOCARDIQUE. Altération de la fonction systolique. Diminution du flux pulmonaire. Diminution de la précharge du VD. Diminution du débit cardiaque. 2 – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: – Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll Cardiol 2002; 40: – Goldstein JA, Tweddell JS. Importance of left ventricular function and systolic ventricular interaction to right ventricular performance during acute right heart ischemia. J Am Coll Cardiol 1992;19:")
25
INFARCTUS VENTRICULE DROIT DISCUSSION
PHYSIOPATHOLOGIE INTERACTION MECANIQUE ENTRE LES DEUX VENTRICULES PAR LE BIAIS DU SEPTUM Élévation de la PTDVD Déplacement du septum vers le VG Altération du remplissage et de la compliance du VG 5 – Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll Cardiol 2002; 40:

26
INFARCTUS VENTRICULE DROIT DISCUSSION
PHYSIOPATHOLOGIE EFFETS RESTRICTIFS DU PERICARDE Limitation de la dilatation du VD par le péricarde Adiastolie Travaux expérimentaux de Goldstein sur le chien (1982 – 1983)
")
27
INFARCTUS VENTRICULE DROIT DISCUSSION
PHYSIOPATHOLOGIE SUR LE PLAN ANATOMO-ELECTRIQUE Artère du nœud sinusal naît de la coronaire droite Artère du nœud auriculo-ventriculaire naît également souvent de la coronaire droite.

28
INFARCTUS VENTRICULE DROIT DISCUSSION
SIGNES ELECTROCARDIOGRAPHIQUES Importance des dérivations droites reconnues en 1976 (7) Sus-décalage de ST V3R, V4R, V1(3,4,8,) Aspect QS ou QR en V3R et/ou V4R Sous-décalage de ST très rare mais très spécifique d’atteinte de la paroi libre du VD si associé à une inversion de l’onde T (9) Utilisation des dérivations droites lors d’épreuves d’effort augmente la sensibilité (10) 7 – Erhardt LR, Sjögren A. Single right-sided precordial lead in the diagnosis of right ventricular involvement in inferior myocardial infarction. Am Heart J 1976;91:571-6. 8 – Zehender M, Kasper W. Right ventricular infarction as an independent predictor of prognosis after acute inferior myocardial infarction. N Engl J Med 1993; 328:981-8. 9 – Mittal SR, Tiwari D. Electrocardiographic diagnosis of infarction of the right ventricular anterior wall. J Electrocardiol 1996;29: 10 – Michaelides AP, Psomadaki ZD. Improved detection of coronary artery disease by exercise electrocardiography with the use of right precordial leads. N Engl J Med 1999;340:340-5.
 Sus-décalage de ST V3R, V4R, V1(3,4,8,) Aspect QS ou QR en V3R et/ou V4R. Sous-décalage de ST très rare mais très spécifique d’atteinte de la paroi libre du VD si associé à une inversion de l’onde T (9) Utilisation des dérivations droites lors d’épreuves d’effort augmente la sensibilité (10) 7 – Erhardt LR, Sjögren A. Single right-sided precordial lead in the diagnosis of right ventricular involvement in inferior myocardial infarction. Am Heart J 1976;91: – Zehender M, Kasper W. Right ventricular infarction as an independent predictor of prognosis after acute inferior myocardial infarction. N Engl J Med 1993; 328: – Mittal SR, Tiwari D. Electrocardiographic diagnosis of infarction of the right ventricular anterior wall. J Electrocardiol 1996;29: – Michaelides AP, Psomadaki ZD. Improved detection of coronary artery disease by exercise electrocardiography with the use of right precordial leads. N Engl J Med 1999;340:")
29
11 – Wellens HJJ. The value of the right precordial leads of the electrocardiogram. N Engl J Med 1999;340:381-3.

30
4 – Zimetbaum PJ, Josephson ME
4 – Zimetbaum PJ, Josephson ME. Use of the Electrocardiogram in Acute Myocardial Infarction. N Engl J Med 2003;348:

31
INFARCTUS VENTRICULE DROIT DISCUSSION
SIGNES ELECTROCARDIOGRAPHIQUES Troubles conductifs de tout types (12) 12 – Yusuf S, Tsuyuki RT. Why do patients with right ventricular infarction have a poor prognosis? American heart association. 69th Scientific sessions. New Orleans, November 10-13, 1996.
 12 – Yusuf S, Tsuyuki RT. Why do patients with right ventricular infarction have a poor prognosis American heart association. 69th Scientific sessions. New Orleans, November 10-13,")
32
INFARCTUS VENTRICULE DROIT DISCUSSION
ECHOCARDIOGRAPHIE Diagnostic positif Troubles de la cinétique segmentaire Fraction d’éjection Dilatation OD – VD IT Pressions Diagnostic différentiel Tamponnade Embolie pulmonaire

33
INFARCTUS VENTRICULE DROIT DISCUSSION
HEMODYNAMIQUE (13) Cathétérisme droit par Swan-Ganz Élévation POD Élévation PTDVD>PAPO Série de 60 IDM inférieurs POD > 10 mm Hg ET dépassant la PAPO de 1 à 5 mm Hg Sensibilité = 73% et spécificité = 100% pour le diagnostic d’atteinte du VD 13– Lopez- Sendon J, Coma-Canella I. Sensitivity and specificity of hemodynamic criteria in the diagnosis of acute right ventricular infarction. Circulation 1981;64:
 Cathétérisme droit par Swan-Ganz. Élévation POD. Élévation PTDVD>PAPO. Série de 60 IDM inférieurs. POD > 10 mm Hg ET dépassant la PAPO de 1 à 5 mm Hg. Sensibilité = 73% et spécificité = 100% pour le diagnostic d’atteinte du VD. 13– Lopez- Sendon J, Coma-Canella I. Sensitivity and specificity of hemodynamic criteria in the diagnosis of. acute right ventricular infarction. Circulation 1981;64:")
34
INFARCTUS VENTRICULE DROIT DISCUSSION
THERAPEUTIQUE (3,14,15) Maintien de la précharge ventriculaire Remplissage (salé) Éviction des nitrés, diurétiques, morphiniques Maintien du synchronisme auriculo-ventriculaire Cardioversion rapide si FA Support inotropique Dobutamine 14 – Pochmalicki G, Chatila M. L’infarctus du ventricule droit. Presse Med 1997 ;26 : 15 – Pfisterer M. Right ventricular involvement in myocardial infarction and cardiogenic shock. Lancet. 2003;362(9381):392-4.
 Maintien de la précharge ventriculaire. Remplissage (salé) Éviction des nitrés, diurétiques, morphiniques. Maintien du synchronisme auriculo-ventriculaire. Cardioversion rapide si FA. Support inotropique. Dobutamine. 14 – Pochmalicki G, Chatila M. L’infarctus du ventricule droit. Presse Med 1997 ;26 : – Pfisterer M. Right ventricular involvement in myocardial infarction and cardiogenic shock. Lancet. 2003;362(9381):")
35
INFARCTUS VENTRICULE DROIT DISCUSSION
THERAPEUTIQUE Réduction de la post-charge ventriculaire droite (en présence d’une dysfonction VG) CPBIA Vasodilatateurs prudents si TA conservée Reperfusion précoce Thrombolyse Angioplastie
 CPBIA. Vasodilatateurs prudents si TA conservée. Reperfusion précoce. Thrombolyse. Angioplastie.")
36
INFARCTUS VENTRICULE DROIT DISCUSSION
THERAPEUTIQUE Thrombolyse (16,17) Efficacité altérée en raison d’un bas débit Taux de reperméabilité après thrombolyse plus bas dans les nécroses inférieures étendues au VD que dans les nécroses inférieures isolées. (TIMI 2 ou 3: 31% vs 71%, p<0,005) 16 – Giannitsis E, Potratz J. Impact of right venticular infarction on in-hospital patency after early thrombolysis with an accelerated dose regimen of 100 mg t-PA. American heart association. 69th Scientific sessions. New Orleans, November 10-13, 1996. 17 – Zeymer U, Neuhaus KL. Effects of thrombolytic therapy in acute myocardial infarction with or without right ventricular involvement. HIT-4 Trial Group. Hirudin for Improvement of Thrombolysis. J Am Coll Cardiol 1998; 32:882-4.
 Efficacité altérée en raison d’un bas débit. Taux de reperméabilité après thrombolyse plus bas dans les nécroses inférieures étendues au VD que dans les nécroses inférieures isolées. (TIMI 2 ou 3: 31% vs 71%, p<0,005) 16 – Giannitsis E, Potratz J. Impact of right venticular infarction on in-hospital patency after early thrombolysis. with an accelerated dose regimen of 100 mg t-PA. American heart association. 69th Scientific sessions. New Orleans, November 10-13, – Zeymer U, Neuhaus KL. Effects of thrombolytic therapy in acute myocardial infarction with or without right. ventricular involvement. HIT-4 Trial Group. Hirudin for Improvement of Thrombolysis. J Am Coll Cardiol. 1998; 32:")
37
INFARCTUS VENTRICULE DROIT DISCUSSION
THERAPEUTIQUE Angioplastie (18,19,20,21) 1ère angiolplastie CD en 1988 Etude randomisée 1999 (20) Spectaculaire amélioration des performances du VD (données échographiques) Excellent devenir clinique avec baisse de la mortalité hospitalière (2% en cas de reperfusion correcte vs 58%) Atteinte monotronculaire plus fréquente lors de choc cardiogénique droit que gauche (65% vs 22%) 18 – Moreyra AE, Suh C. Rapid Hemodynamic Improvement in Right Ventricular Infarction After Coronary Angioplasty. Chest 1988;94:197-9. 19 – Kinn JW, Ajluni SC. Rapid Hemodynamic Improvement after Reperfusion During Right Ventricular Infarction. J Am Coll Cardiol 1995 ; 26: 20 – Bowers RT, O’Neill WW, Goldstein JA. Effect of reperfusion on biventricular function and survival after right ventricular infarction. N Engl J Med 1998;338: 21 – Jacobs AK, Leopold JA. Cardiogenic shock caused by right ventricular infarction. A report from the SHOCK registry. J Am Coll Cardiol 2003;41:
 1ère angiolplastie CD en Etude randomisée 1999 (20) Spectaculaire amélioration des performances du VD (données échographiques) Excellent devenir clinique avec baisse de la mortalité hospitalière (2% en cas de reperfusion correcte vs 58%) Atteinte monotronculaire plus fréquente lors de choc cardiogénique droit que gauche (65% vs 22%) 18 – Moreyra AE, Suh C. Rapid Hemodynamic Improvement in Right Ventricular Infarction. After Coronary Angioplasty. Chest 1988;94: – Kinn JW, Ajluni SC. Rapid Hemodynamic Improvement after Reperfusion During Right Ventricular. Infarction. J Am Coll Cardiol 1995 ; 26: – Bowers RT, O’Neill WW, Goldstein JA. Effect of reperfusion on biventricular function and survival after. right ventricular infarction. N Engl J Med 1998;338: – Jacobs AK, Leopold JA. Cardiogenic shock caused by right ventricular infarction. A report from the. SHOCK registry. J Am Coll Cardiol 2003;41:")
38
INFARCTUS VENTRICULE DROIT DISCUSSION
THERAPEUTIQUE Thrombolyse vs angioplastie (22) Tendance (non significative) à une diminution de mortalité quelle que soit la technique pour infarctus du VD sans choc. Lors d’infarctus avec choc, seule l’angioplastie était utilisée: réduction notable de la mortalité hospitalière (89% sans angioplastie vs 58% avec angioplastie) 22 – Lupi-Herrera E, Lasses LA. Acute right ventricular infarction : clinical spectrum, results of reperfusion therapy and short-term prognosis. Coron Artery Dis. 2002; 13(1):57-64.
 Tendance (non significative) à une diminution de mortalité quelle que soit la technique pour infarctus du VD sans choc. Lors d’infarctus avec choc, seule l’angioplastie était utilisée: réduction notable de la mortalité hospitalière (89% sans angioplastie vs 58% avec angioplastie) 22 – Lupi-Herrera E, Lasses LA. Acute right ventricular infarction : clinical spectrum, results of. reperfusion therapy and short-term prognosis. Coron Artery Dis. 2002; 13(1):")
39
INFARCTUS VENTRICULE DROIT DISCUSSION
PRONOSTIC ET EVOLUTION (8) Nécrose inférieure avec extension au VD est hautement prédictif d’une mortalité hospitalière élevée (31% vs 6%) de la survenue de complications majeures (64% vs 28%) par rapport à une nécrose inférieure isolée.
 Nécrose inférieure avec extension au VD est hautement prédictif. d’une mortalité hospitalière élevée (31% vs 6%) de la survenue de complications majeures (64% vs 28%) par rapport à une nécrose inférieure isolée.")
40
INFARCTUS VENTRICULE DROIT DISCUSSION
PRONOSTIC ET EVOLUTION (4,23) Segment ST Sa normalisation est un excellent signe de reperfusion tissulaire Résolution précoce d’un sus-décalage de ST est un signe d’excellent pronostic à court (30 J) et long terme (1 an)* Absence de normalisation du ST 90 mn après thrombolyse doit faire envisager l’angioplastie.* *(étude faite sur des IDM inférieurs et antérieurs) 23 – Schroder K, Wegscheider K. Extent of ST-segment in a single electrocardiogram lead 90 min after thrombolysis as a predictor of medium-term mortality in acute myocardial infarction. Lancet 2001;358:
 Segment ST. Sa normalisation est un excellent signe de reperfusion tissulaire. Résolution précoce d’un sus-décalage de ST est un signe d’excellent pronostic à court (30 J) et long terme (1 an)* Absence de normalisation du ST 90 mn après thrombolyse doit faire envisager l’angioplastie.* *(étude faite sur des IDM inférieurs et antérieurs) 23 – Schroder K, Wegscheider K. Extent of ST-segment in a single electrocardiogram lead 90 min after thrombolysis as a predictor of medium-term mortality in acute myocardial infarction. Lancet 2001;358:")
41
INFARCTUS VENTRICULE DROIT DISCUSSION
PRONOSTIC ET EVOLUTION SUJET AGE Plus de 75 ans (24,25) IDM < avec participation droite: 47% de décès hospitaliers IDM < sans participation droite: 10% de décès hospitaliers Effet non retrouvé statistiquement dans une population plus jeune Avec participation droite: plus grande fréquence de choc(32% vs 5%), de BAV complet(33% vs 9%), de rupture septale (9% vs 0%) 24 – Bueno H, Lopez-Palop R. In-Hospital outcome of elderly patients with acute inferior myocardial infarction and right ventricular involvement. Circulation 1997;96: 25 – Bueno H, Lopez-Palop R. Combined Effect of Age and Right Ventricular Involvement on Acute Inferior Myocardial Infarction Prognosis. Circulation. 1998;98:
 IDM < avec participation droite: 47% de décès hospitaliers. IDM < sans participation droite: 10% de décès hospitaliers. Effet non retrouvé statistiquement dans une population plus jeune. Avec participation droite: plus grande fréquence de choc(32% vs 5%), de BAV complet(33% vs 9%), de rupture septale (9% vs 0%) 24 – Bueno H, Lopez-Palop R. In-Hospital outcome of elderly patients with acute inferior myocardial infarction and right ventricular involvement. Circulation 1997;96: – Bueno H, Lopez-Palop R. Combined Effect of Age and Right Ventricular Involvement on Acute Inferior Myocardial Infarction Prognosis. Circulation. 1998;98:")
42
INFARCTUS VENTRICULE DROIT
1974: entité clinique reconnue 1976: importance des dérivations droites 1988: 1ère angioplastie de coronaire droite 2004: privilégier l’angioplastie surtout si choc associé En pratique: V3R et V4R systématiques Reconnaissance précoce Thérapeutique spécifique

43
INFARCTUS VENTRICULE DROIT BIBLIOGRAPHIE
1 – Cohn JN, Guiha NH. Right ventricular infarction: clinical and hemodynamic features. Am J Cardiol 1974; 33: 2 – Kinch JW, Ryan TJ. Right ventricular infarction. N Engl J Med 1994;330: 3 – The Task Force of the Management of Acute Myocardial Infarction of the European Society of Cardiology. Management of Acute Myocardial Infarction in Patients Presenting with ST-Segment Elevation. European Heart Journal (2003) 24, 4 – Zimetbaum PJ, Josephson ME. Use of the Electrocardiogram in Acute Myocardial Infarction. N Engl J Med 2003;348: 5 – Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll Cardiol 2002; 40:841- 53. 6 – Goldstein JA, Tweddell JS. Importance of left ventricular function and systolic ventricular interaction to right ventricular performance during acute right heart ischemia. J Am Coll Cardiol 1992;19: 7 – Erhardt LR, Sjögren A. Single right-sided precordial lead in the diagnosis of right ventricular involvement in inferior myocardial infarction. Am Heart J 1976;91:571-6. 8 – Zehender M, Kasper W. Right ventricular infarction as an independent predictor of prognosis after acute inferior myocardial infarction. N Engl J Med 1993; 328:981-8. 9 – Mittal SR, Tiwari D. Electrocardiographic diagnosis of infarction of the right ventricular anterior wall. J Electrocardiol 1996;29: 10 – Michaelides AP, Psomadaki ZD. Improved detection of coronary artery disease by exercise electrocardiography with the use of right precordial leads. N Engl J Med 1999;340:340-5. 11 – Wellens HJJ. The value of the right precordial leads of the electrocardiogram. N Engl J Med 1999;340: 12 – Yusuf S, Tsuyuki RT. Why do patients with right ventricular infarction have a poor prognosis? American heart association. 69th Scientific sessions. New Orleans, November 10-13, 1996.
 24, – Zimetbaum PJ, Josephson ME. Use of the Electrocardiogram in Acute Myocardial Infarction. N Engl J Med. 2003;348: – Goldstein JA. Pathophysiology and management of right heart ischemia. J Am Coll Cardiol 2002; 40: – Goldstein JA, Tweddell JS. Importance of left ventricular function and systolic ventricular interaction to right. ventricular performance during acute right heart ischemia. J Am Coll Cardiol 1992;19: – Erhardt LR, Sjögren A. Single right-sided precordial lead in the diagnosis of right ventricular involvement in. inferior myocardial infarction. Am Heart J 1976;91: – Zehender M, Kasper W. Right ventricular infarction as an independent predictor of prognosis after acute. inferior myocardial infarction. N Engl J Med 1993; 328: – Mittal SR, Tiwari D. Electrocardiographic diagnosis of infarction of the right ventricular anterior wall. J. Electrocardiol 1996;29: – Michaelides AP, Psomadaki ZD. Improved detection of coronary artery disease by exercise electrocardiography with the use of right precordial leads. N Engl J Med 1999;340: – Wellens HJJ. The value of the right precordial leads of the electrocardiogram. N Engl J Med 1999;340: – Yusuf S, Tsuyuki RT. Why do patients with right ventricular infarction have a poor prognosis American heart association. 69th Scientific sessions. New Orleans, November 10-13,")
44
INFARCTUS VENTRICULE DROIT BIBLIOGRAPHIE
13 – Lopez- Sendon J, Coma-Canella I. Sensitivity and specificity of hemodynamic criteria in the diagnosis of acute right ventricular infarction. Circulation 1981;64: 14 – Pochmalicki G, Chatila M. L’infarctus du ventricule droit. Presse Med 1997 ;26 : 15 – Pfisterer M. Right ventricular involvement in myocardial infarction and cardiogenic shock. Lancet. 2003;362(9381):392-4. 16 – Giannitsis E, Potratz J. Impact of right venticular infarction on in-hospital patency after early thrombolysis with an accelerated dose regimen of 100 mg t-PA. American heart association. 69th Scientific sessions. New Orleans, November 10-13, 1996. 17 – Zeymer U, Neuhaus KL. Effects of thrombolytic therapy in acute myocardial infarction with or without right ventricular involvement. HIT-4 Trial Group. Hirudin for Improvement of Thrombolysis. J Am Coll Cardiol 1998; 32:882-4. 18 – Moreyra AE, Suh C. Rapid Hemodynamic Improvement in Right Ventricular Infarction After Coronary Angioplasty. Chest 1988;94:197-9. 19 – Kinn JW, Ajluni SC. Rapid Hemodynamic Improvement after Reperfusion During Right Ventricular Infarction. J Am Coll Cardiol 1995 ; 26: 20 – Bowers RT, O’Neill WW, Goldstein JA. Effect of reperfusion on biventricular function and survival after right ventricular infarction. N Engl J Med 1998;338: 21 – Jacobs AK, Leopold JA. Cardiogenic shock caused by right ventricular infarction. A report from the SHOCK registry. J Am Coll Cardiol 2003;41: 22 – Lupi-Herrera E, Lasses LA. Acute right ventricular infarction : clinical spectrum, results of reperfusion therapy and short-term prognosis. Coron Artery Dis. 2002; 13(1):57-64.
: – Giannitsis E, Potratz J. Impact of right venticular infarction on in-hospital patency after early thrombolysis. with an accelerated dose regimen of 100 mg t-PA. American heart association. 69th Scientific sessions. New Orleans, November 10-13, – Zeymer U, Neuhaus KL. Effects of thrombolytic therapy in acute myocardial infarction with or without right. ventricular involvement. HIT-4 Trial Group. Hirudin for Improvement of Thrombolysis. J Am Coll Cardiol. 1998; 32: – Moreyra AE, Suh C. Rapid Hemodynamic Improvement in Right Ventricular Infarction. After Coronary Angioplasty. Chest 1988;94: – Kinn JW, Ajluni SC. Rapid Hemodynamic Improvement after Reperfusion During Right Ventricular. Infarction. J Am Coll Cardiol 1995 ; 26: – Bowers RT, O’Neill WW, Goldstein JA. Effect of reperfusion on biventricular function and survival after. right ventricular infarction. N Engl J Med 1998;338: – Jacobs AK, Leopold JA. Cardiogenic shock caused by right ventricular infarction. A report from the. SHOCK registry. J Am Coll Cardiol 2003;41: – Lupi-Herrera E, Lasses LA. Acute right ventricular infarction : clinical spectrum, results of. reperfusion therapy and short-term prognosis. Coron Artery Dis. 2002; 13(1):")
45
INFARCTUS VENTRICULE DROIT BIBLIOGRAPHIE
23 – Schroder K, Wegscheider K. Extent of ST-segment in a single electrocardiogram lead 90 min after thrombolysis as a predictor of medium-term mortality in acute myocardial infarction. Lancet 2001;358: 24 – Bueno H, Lopez-Palop R. In-Hospital outcome of elderly patients with acute inferior myocardial infarction and right ventricular involvement. Circulation 1997;96: 25 – Bueno H, Lopez-Palop R. Combined Effect of Age and Right Ventricular Involvement on Acute Inferior Myocardial Infarction Prognosis. Circulation. 1998;98:

Présentations similaires


















>")

>")