Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Une pneumonie nosocomiale..
Mme P 48 ans, cirrhose Child A ATCD crises convulsives 165 cm, 102 Kg Hospitalisée pour hémorragie digestive VO sous cardiale difficile d’accès Intubation et VM pour fibroscopie 250 mg d’erythromycine bolus IV avant la fibro Augmentin 1g X 4 J-1 à J+6 Reste ventilée car agitée et hypoxique (atelectasie basale) J6: T 39°C, aggravation gazométrique, GB Doute sur foyer de la base gauche. Sécrétion trachéale jaunâtre TA 9 NA 1 mg/h Créatinine 102 µm/l, Urée 9,8 mMol/l, Bilirubine 250 UI Diurèse 2200 ml/j
 J6: T 39°C, aggravation gazométrique, GB. Doute sur foyer de la base gauche. Sécrétion trachéale jaunâtre. TA 9 NA 1 mg/h. Créatinine 102 µm/l, Urée 9,8 mMol/l, Bilirubine 250 UI. Diurèse 2200 ml/j.")
2
Fibroscopie Bronchique BA et LBA
BA: quelques leucocytes Petits BGN fins (type pyo) LBA: cellules, 95% PN direct neg Vous décidez de traiter…
 LBA: cellules, 95% PN. direct neg. Vous décidez de traiter…")
3
Germes à évoquer Klebsielles sauvages Enterobactéries de type III
Hemophilus P aeruginosa Acinetobacter baumannii SAMS SAMR S maltophilia

4
VM < 7 jours, antibiotiques
un centre a manoifestement un probleme avec le pyo 2 centre sur 4 ont des soucis avec acinetobacter en regle general, on voit disparaitre pneumocoques et toutes les bactéries très sensibles Rello et al, AJRCCM 1999;160:608

5
Vous proposez une antibiothérapie par?
C3G + gentamicine C3G + ciprofloxacine + Vancomycine Piperacilline + Tazobactam + Tobramycine Penem+ Amikacin+ Vancomycine Penem + vancomycine Autres choix

6
Vous choisissez un Penems lequel?
Ertapenem 1 g X 2 Imipenem 1g en 60min X 3 Meropenem 1g en 60 min X 3 Doripenem 500mg en 4 heures X 3

7
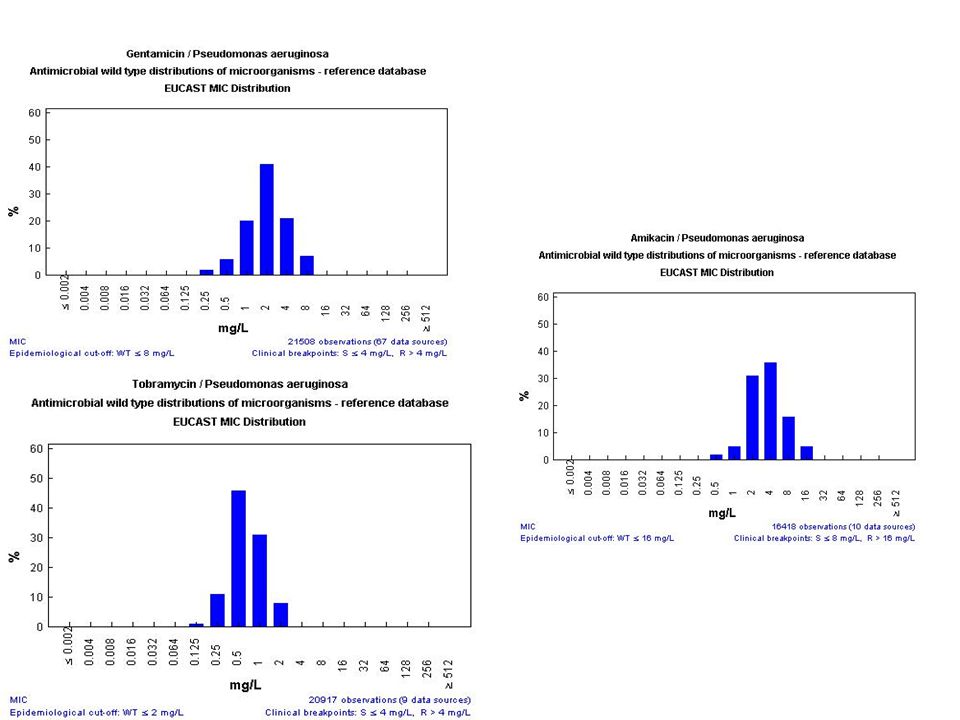
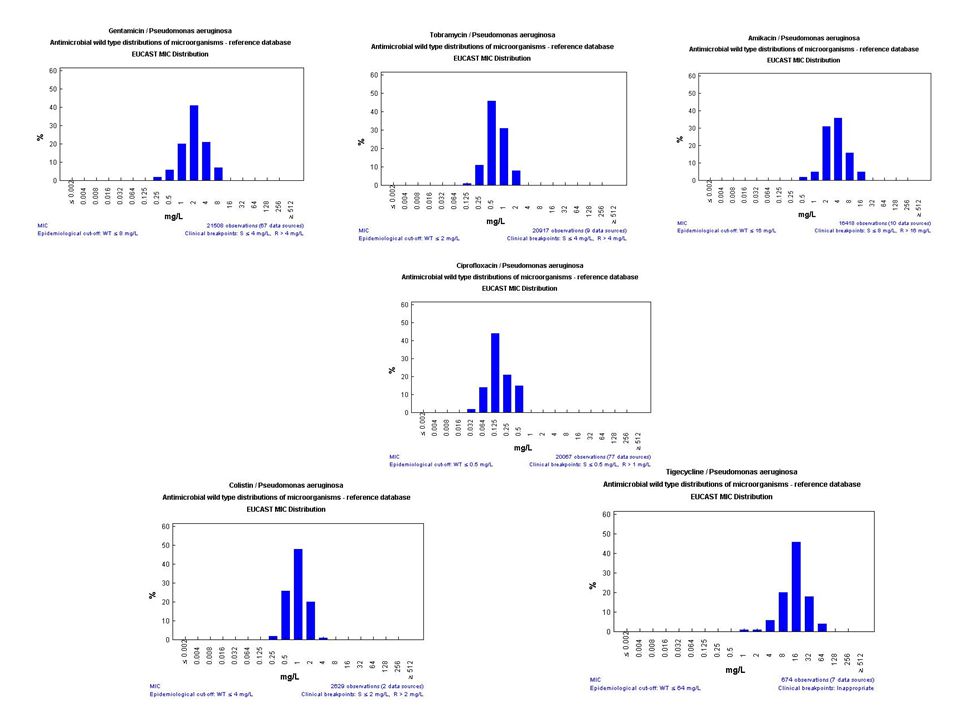
Données de l’EUCAST (Wild type)
")
8
O. Pajot et al. / Réanimation 15 (2006) 188
 188")
9
O Pajot et al. / Réanimation 15 (2006) 188
 188")
10
Imipénème: 500 mg (en 30 min) x 4 ou 1 g (en 60 min) x 3 vs
Doripénème: 500 mg en 4 heures x 3 Mais CMI > 8 mg/L à l’inclusion ou sous traitement Imipénème: 16/25: 64%, doripénème: 5/28: 18%, p< 0,001

11
Vous choisissez d’y adjoindre un autre antibiotique anti-pyo
Parce que la bi –thérapie a prouvé son efficacité dans cette indication? Avec de la tobramycine car rapidement bactéricide et moindre toxicité rénale que les autres aminosides Avec de la levofloxacine car meilleure diffusion et pas de toxicité rénale pour d’autres raisons

12
Comparaison des études avec même béta-lactamine
monothérapie association 1.02 [ ] Mortalité (12, n=1381) 1.09 [0.94 – 1.27] Echecs cliniques (20, n=1870) 1.08 [0.71 – 1.64] Echecs microbiol.(14, n=751) Toxicité rénale (n=5213) 0.36 [0.28 – 0.47] 0,1 0,2 0,5 1 2 5 10 Risque relatif M. Paul & al, BMJ 2004
 1.09 [0.94 – 1.27] Echecs cliniques (20, n=1870) 1.08 [0.71 – 1.64] Echecs microbiol.(14, n=751) Toxicité rénale. (n=5213) 0.36 [0.28 – 0.47] 0,1. 0,2. 0, Risque relatif. M. Paul & al, BMJ")
13
Bactériémies à Klebsiella
Monothérapie Association P Gravité (Pitt) 0 - 3 ≥4 8 / 86 (9%) 16 / 32 (50%) 13 / 90 (14%) 7 / 22 (32%) Choc Normotension Hypotension 11 / 92 (12%) 13 / 26 (50%) 13 / 83 (16%) 7 / 29 (24%) 0.056 Immuno-Dépression Absent Present 16 / 87 (18%) 8 / 31 (26%) 11/ 70 (16%) 9 / 41 (22%) Ensemble pts (n= 230) 24 / 118 (20%) 20 / 112 (18%) NS Prospective Observational Study of Kiebsiella Bacteremia in 230 Patients: Outcome for Antibiotic Combinations versus Monotherapy. Korvick & al, AAC 1992; 36:
 ≥4. 8 / 86 (9%) 16 / 32 (50%) 13 / 90 (14%) 7 / 22 (32%) Choc. Normotension. Hypotension. 11 / 92 (12%) 13 / 26 (50%) 13 / 83 (16%) 7 / 29 (24%) Immuno-Dépression. Absent. Present. 16 / 87 (18%) 8 / 31 (26%) 11/ 70 (16%) 9 / 41 (22%) Ensemble pts. (n= 230) 24 / 118 (20%) 20 / 112 (18%) NS. Prospective Observational Study of Kiebsiella Bacteremia in 230 Patients: Outcome for Antibiotic Combinations versus Monotherapy. Korvick & al, AAC 1992; 36:")
14
Prospective Observational Study of Klebsiella Bacteremia in 230 Patients: Outcome of Antibiotic Combination vs. Monotherapy Pts who experienced hypotension within 72 h, n=55 P=0.03 n=29 n=26 Korvick & al, AAC 1992; 36:

15
Altération PK en réanimation

16
Distribution tissulaire de l’Imipenem chez des patients de réanimation
Tegeder et al Clin. Pharmacol. Ther 2002, 71, Antibiotique temps dépendant A l’exception des septicémies et endocardites, les concentrations tissulaires sont les plus intéressantes Etude 5 volontaires sains versus 6 patients avec au moins une défaillance d’organe Tiénam : 500 mg x 1 chez VS en 20 min 500 mg x 3 ou x 4 chez les malades Microdialyse muscle et tissu sous cutané

17
S= Sujets sains

18
Tissue penetration is correlated to
Clinical scoring system for the prediction of target site penetration of antimicrobials in patients with sepsis. Zeitlinger BS et al Clin Pharmacokinet. 2007;46(1):75-83. Tissue penetration is correlated to SAPS 3 r=-0.33, p=0.006 APACHE III r=-0.27, p=0.03 SOFA r=-0.32, p=0.01 TPP score (lactate/ norepinephrine dose/SpO2) r=-0.52, p<0.0001 Clinical scoring system for the prediction of target site penetration of antimicrobials in patients with sepsis. Zeitlinger BS, Zeitlinger M, Leitner I, Muller M, Joukhadar C. Department of Clinical Pharmacology, Division of Clinical Pharmacokinetics, Medical University of Vienna, Vienna, AustriaDepartment of Otorhinolaryngology, Medical University of Vienna, Vienna, Austria. BACKGROUND AND OBJECTIVES: The present study investigated the usefulness of routinely employed scoring systems in predicting tissue penetration of antimicrobials. In addition, a novel, easy to use scoring system was designed for the estimation of tissue penetration of antimicrobials in patients with sepsis. METHODS: Tissue pharmacokinetics were assessed in skeletal muscle and subcutaneous adipose tissue by use of the microdialysis technique in 34 patients with sepsis. Tissue penetration of antimicrobials was retrospectively determined by the ratios of the area under the concentration-time curves (AUC) in soft tissues (AUC(tissue)) to the AUC in plasma (AUC(plasma)). Mortality and sepsis scores currently used in intensive care were consecutively calculated and correlated with the AUC(tissue) : AUC(plasma) ratio. Single laboratory and clinical parameters showing the highest correlation with tissue penetration were identified and used in the novel Tissue Penetration Prediction Score (TPPS). RESULTS: The currently used scoring systems Simplified Acute Physiology Scores 3 (r = -0.33, p = 0.006), Acute Physiology and Chronic Health Evaluation III (r = -0.27, p = 0.03) and Sepsis-Related (or Sequential) Organ Failure Assessment (r = -0.32, p = 0.01) showed significant overall correlations with tissue penetration. However, their predictive power for the concentrations of antimicrobials in muscle tissue was not satisfying. The parameters oxygen saturation, serum lactate concentration and the dose per time unit of norepinephrine (noradrenaline) administered showed the best correlation with tissue penetration and were used in the TPPS. Its overall correlation (r = -0.52, p = ) as well as correlations for the concentrations of antimicrobials in muscle (r = -0.46, p = 0.006) and adipose tissue (r = -0.59, p = ) were better than the currently used scoring systems. CONCLUSION: The TPPS may prove to be a powerful tool for the estimation of antimicrobial tissue penetration at the bedside in septic patients. This score may allow for adequate individual dose adjustment in septic patients. However, this needs to be verified in subsequent prospective clinical trials.
: Tissue penetration is correlated to. SAPS 3 r=-0.33, p= APACHE III r=-0.27, p=0.03. SOFA r=-0.32, p=0.01. TPP score. (lactate/ norepinephrine dose/SpO2) r=-0.52, p< Clinical scoring system for the prediction of target site penetration of antimicrobials in patients with sepsis. Zeitlinger BS, Zeitlinger M, Leitner I, Muller M, Joukhadar C. Department of Clinical Pharmacology, Division of Clinical Pharmacokinetics, Medical University of Vienna, Vienna, AustriaDepartment of Otorhinolaryngology, Medical University of Vienna, Vienna, Austria. BACKGROUND AND OBJECTIVES: The present study investigated the usefulness of routinely employed scoring systems in predicting tissue penetration of antimicrobials. In addition, a novel, easy to use scoring system was designed for the estimation of tissue penetration of antimicrobials in patients with sepsis. METHODS: Tissue pharmacokinetics were assessed in skeletal muscle and subcutaneous adipose tissue by use of the microdialysis technique in 34 patients with sepsis. Tissue penetration of antimicrobials was retrospectively determined by the ratios of the area under the concentration-time curves (AUC) in soft tissues (AUC(tissue)) to the AUC in plasma (AUC(plasma)). Mortality and sepsis scores currently used in intensive care were consecutively calculated and correlated with the AUC(tissue) : AUC(plasma) ratio. Single laboratory and clinical parameters showing the highest correlation with tissue penetration were identified and used in the novel Tissue Penetration Prediction Score (TPPS). RESULTS: The currently used scoring systems Simplified Acute Physiology Scores 3 (r = -0.33, p = 0.006), Acute Physiology and Chronic Health Evaluation III (r = -0.27, p = 0.03) and Sepsis-Related (or Sequential) Organ Failure Assessment (r = -0.32, p = 0.01) showed significant overall correlations with tissue penetration. However, their predictive power for the concentrations of antimicrobials in muscle tissue was not satisfying. The parameters oxygen saturation, serum lactate concentration and the dose per time unit of norepinephrine (noradrenaline) administered showed the best correlation with tissue penetration and were used in the TPPS. Its overall correlation (r = -0.52, p = ) as well as correlations for the concentrations of antimicrobials in muscle (r = -0.46, p = 0.006) and adipose tissue (r = -0.59, p = ) were better than the currently used scoring systems. CONCLUSION: The TPPS may prove to be a powerful tool for the estimation of antimicrobial tissue penetration at the bedside in septic patients. This score may allow for adequate individual dose adjustment in septic patients. However, this needs to be verified in subsequent prospective clinical trials.")
19
Monothérapies “à risque”
Pathogènes, % [Taux d’éradication] CIP (n=152) IMP (n=155) P. aeruginosa 22 [33%] 17 [41%] H. influenzae 16 [100%] 12 [100%] SAMS 13 [65%] 11 [65%] Enterobacter sp. 6.5 [100%] 13.5 [62%] All, except P. aeruginosa [88%] [73%] Facteurs associés à l’échec thérapeutique: VM (OR 8.5 [2.3-25]; Apache II (OR 1.05); Inf. à P.aeruginosa (OR 2.4 [ ] Fink et al, AAC 1994; 38:
 IMP (n=155) P. aeruginosa. 22 [33%] 17 [41%] H. influenzae. 16 [100%] 12 [100%] SAMS. 13 [65%] 11 [65%] Enterobacter sp. 6.5 [100%] 13.5 [62%] All, except P. aeruginosa. [88%] [73%] Facteurs associés à l’échec thérapeutique: VM (OR 8.5 [2.3-25]; Apache II (OR 1.05); Inf. à P.aeruginosa (OR 2.4 [ ] Fink et al, AAC 1994; 38:")
21
Paramètres pharmacodynamiques
concentrations QI = Cmax/CMI ASC 24h/CMI temps de contact à C>CMI [T (%24h) >CMI] C max ASC CMI Cmin temps T > CMI (h)
 >CMI] C max. ASC. CMI. Cmin. temps. T > CMI (h)")
22
DOSE de charge +++ Concentration (mg/L) Dose de charge
Perfusion continue T>CMI = 100% Cplateau CMP CMI Temps (H)
")
23
1 g X 4 vs 4 g continuous + tobramycin 7mg/kg/d (both groups)
Meropenem by continuous versus intermittent infusion in ventilator-associated pneumonia due to gram-negative bacilli. 1 g X 4 vs 4 g continuous + tobramycin 7mg/kg/d (both groups) Continuous (n=42) Intermittent (n=47) P value Age 57.2 56.5 0.8 APACHE II 15.3 15.2 0.88 Cl Creat 101 102 0.81 SOFA (VAP) 8.64 8.52 MICs 0.54 0.48 Cure rate 90.5% 59.6% <0.0001 Cure rate (P. aeruginosa) 84.6% 40% Cure rate if MIC> 0.5 81% 29.4% <0.001 BACKGROUND: It is known that beta-lactam antibiotics exhibit time-dependent bactericidal activity. Several studies have found continuous infusion of meropenem more effective than intermittent infusion in maintaining constant serum concentrations in excess of the minimum inhibitory concentration. However, limited data exist on the clinical efficacy of meropenem administered by continuous infusion. OBJECTIVE: To evaluate the clinical efficacy of continuous versus intermittent infusion of meropenem for the treatment of ventilator-associated pneumonia (VAP) due to gram-negative bacilli. METHODS: A retrospective cohort study was conducted of patients with VAP caused by gram-negative bacilli who received initial empiric antibiotic therapy with meropenem. We analyzed 2 contemporary cohorts: one group received meropenem by continuous infusion (1 g over 360 min every 6 h), the other by intermittent infusion (1 g over 30 min every 6 h). The administration method was prescribed according to the physician's discretion. Patients received meropenem plus tobramycin for 14 days. RESULTS: There were no significant differences between patient groups with regard to gender, age, APACHE-II at intensive care unit admission, diagnosis, microorganism responsible for VAP, or organ dysfunction severity at the time VAP was suspected. The group receiving medication by continuous infusion showed a greater clinical cure rate than the group treated with intermittent infusion (38 of 42, 90.47%, vs 28 of 47, 59.57%, respectively, with OR 6.44 [95% CI 1.97 to 21.05; p < 0.001]). CONCLUSIONS: Meropenem administered by continuous infusion may have more clinical efficacy than intermittent infusion. But retrospective, treatment too long, mortality not reported, dosage not performed Lorente et al – Ann Pharmacother 2006; 40:219
 Continuous (n=42) Intermittent (n=47) P value. Age APACHE II Cl Creat SOFA (VAP) MICs Cure rate. 90.5% 59.6% < Cure rate (P. aeruginosa) 84.6% 40% Cure rate if MIC> % 29.4% < BACKGROUND: It is known that beta-lactam antibiotics exhibit time-dependent bactericidal activity. Several studies have found continuous infusion of meropenem more effective than intermittent infusion in maintaining constant serum concentrations in excess of the minimum inhibitory concentration. However, limited data exist on the clinical efficacy of meropenem administered by continuous infusion. OBJECTIVE: To evaluate the clinical efficacy of continuous versus intermittent infusion of meropenem for the treatment of ventilator-associated pneumonia (VAP) due to gram-negative bacilli. METHODS: A retrospective cohort study was conducted of patients with VAP caused by gram-negative bacilli who received initial empiric antibiotic therapy with meropenem. We analyzed 2 contemporary cohorts: one group received meropenem by continuous infusion (1 g over 360 min every 6 h), the other by intermittent infusion (1 g over 30 min every 6 h). The administration method was prescribed according to the physician s discretion. Patients received meropenem plus tobramycin for 14 days. RESULTS: There were no significant differences between patient groups with regard to gender, age, APACHE-II at intensive care unit admission, diagnosis, microorganism responsible for VAP, or organ dysfunction severity at the time VAP was suspected. The group receiving medication by continuous infusion showed a greater clinical cure rate than the group treated with intermittent infusion (38 of 42, 90.47%, vs 28 of 47, 59.57%, respectively, with OR 6.44 [95% CI 1.97 to 21.05; p < 0.001]). CONCLUSIONS: Meropenem administered by continuous infusion may have more clinical efficacy than intermittent infusion. But retrospective, treatment too long, mortality not reported, dosage not performed. Lorente et al – Ann Pharmacother 2006; 40:219.")
24
Imipénème: 500 mg (en 30 min) x 4 ou 1 g (en 60 min) x 3 vs
Doripénème: 500 mg en 4 heures x 3 Tps dependance? Mais CMI > 8 mg/L à l’inclusion ou sous traitement Imipénème: 16/25: 64%, doripénème: 5/28: 18%, p< 0,001

25
Conclusion: Pseudomonas
« En cas de suspicion d’infection bactériémique à P. aeruginosa , nous suggérons de débuter l’antibiothérapie par deux molécules anti-pyocyaniques. Si la bactériémie à P. aeruginosa est confirmée, l’antibiothérapie peut néanmoins être rapidement limitée à une monothérapie selon le profil de sensibilité de la souche initialement isolée. Cette approche devrait permettre de limiter le risque d’antibiothérapies initialement inappropriées, tout en réduisant le risque de sélection de souches résistantes, et de toxicité. » Chamot et al, AAC 2003; 47: 2756

26
Vous choisissez d’y adjoindre un autre antibiotique anti-pyo
Parce que la bi –thérapie a prouvé son efficacité dans cette indication? Avec de la tobramycine car rapidement bactéricide et moindre toxicité rénale que les autres aminosides Avec de la levofloxacine car meilleure diffusion et pas de toxicité rénale pour d’autres raisons

27
Neuhauser et al – JAMA 2003

28
Gentamicine 150mg en 45 min X 2 Tobramycine 500 mg en 45 min X 1
Vous n’avez pas vu de SARM depuis plus d’un mois, le dépistage nasal de la patient à l’entrée était négatif – vous choisissez une bi-therapie par Penems + aminosides: lequel? Comment? Gentamicine 150mg en 45 min X 2 Tobramycine 500 mg en 45 min X 1 Amikacine 1,5 ou 2 g en 45 min X 1 Amikacine 1g en 45 min X 1 Amikacine en aérosols

29
quel paramètre de monitoring pharmacologique ?
Relation entre le rapport Pic Max/CMI d’aminosides et le taux de guérison clinique Taux de guérison clinique (%) quel paramètre de monitoring pharmacologique ? Rapport Pic Max/CMI D’après Moore et al, JID, 1987, 155, 93-99
 quel paramètre de monitoring pharmacologique Rapport Pic Max/CMI. D’après Moore et al, JID, 1987, 155,")
30
Optimising aminoglycoside therapy for nosocomial pneumonia
Probability of resolution (%) 100 80 Probability of temperature resolution by Day 7 Probability of white blood cell (WBC) count resolution by Day 7 60 40 First Cmax:MIC 10 gives 90% probability of WBC and temperature resolution 20 5 10 15 20 25 30 First Cmax:MIC Kashuba et al. Antimicrob Agents Chemother 1999;43:623–629 30
 Probability of temperature resolution by Day 7. Probability of white blood cell (WBC) count resolution by Day First Cmax:MIC 10 gives. 90% probability of WBC. and temperature resolution First Cmax:MIC. Kashuba et al. Antimicrob Agents Chemother 1999;43:623–")
31
OPTIMISATION DE LA POSOLOGIE Évolution clinique et 1er pic sérique
91 patients de réanimation; amikacine 15 mg/kg/j n= 7 n= 46 p < 0.05 n= 0 n= 38 Beaucaire et al, Réa Med Urg, 1991,7,352-8

33
Objectif de concentrations sériques * DUJ; fonction rénale normale
DUJ (mg/kg) Pic** Vallée*** Amikacine < 2.5 Gentamicine < 0.5 Netilmicine < 1 * mg/l ** 30 min après la fin d’une perfusion de 30 min *** immédiatement avant l’administration suivante
 Pic** Vallée*** Amikacine < 2.5. Gentamicine < 0.5. Netilmicine < 1. * mg/l. ** 30 min après la fin d’une perfusion de 30 min. *** immédiatement avant l’administration suivante.")
34
Monitoring des concentrations sériques
Si traitement court (3 à 5 jours), contrôle de la valeur du 1er ou 2ème pic de la valeur d’une vallée si fonction rénale altérée ou conditions hémodynamiques instables Si traitement long (illégitime en dehors de l’endocardite), contrôle régulier de la valeur de la vallée
, contrôle. de la valeur du 1er ou 2ème pic. de la valeur d’une vallée si fonction rénale altérée ou conditions hémodynamiques instables. Si traitement long (illégitime en dehors de l’endocardite), contrôle régulier de la valeur de la vallée.")
35
MONITORING DES POSOLOGIES DUJ; INSUFFISANCE RENALE
Insuffisance rénale Cl. créatinine > 30 ml/mn conserver dose unique standard, et espacer les administrations surveiller la vallée; quand < 5 mg/l , nouvelle administration Cl. créatinine < ou = 30 ml/mn réduire dose unique standard de moitié, et idem pour le reste ou une dose unique élevée ou choisir un autre antibiotique Hémodialyse dose unique standard 1 à 2 heures avant le début de la séance++ Hémofiltration continue 1ère dose unique standard si possible avant la séance dosage à 18h; si concentrations sériques < 5mg/l, dose suivante environ 75% de la dose standard

36
AMINOSIDES EN AEROSOL Essentiellement dans la mucoviscidose
Les problèmes Présentation des aminosides (TOBI – TSI) Le nébuliseur Le compresseur La taille des particules La distribution de l’aminoside Extrapolation des données du sujet sain (homme ou animal) au sujet pathologique Intérêt dans la pneumonie Augmentation potentielle sous traitement des CMI de P. aeruginosa (imperméabilité) Sélection de BMR (P. aeruginosa, S. maltophilia)
 Le nébuliseur. Le compresseur. La taille des particules. La distribution de l’aminoside. Extrapolation des données du sujet sain (homme ou animal) au sujet pathologique. Intérêt dans la pneumonie. Augmentation potentielle sous traitement des CMI de P. aeruginosa (imperméabilité) Sélection de BMR (P. aeruginosa, S. maltophilia)")
37
Aérosols: Distribution hétérogène

38
Le LBA > 105 cfu/ml de P aeruginosa. L’amikacine…
Doit être poursuivie pendant toute la durée du traitement avec une dose plus « classique » dès le 3eme jour Doit être suspendue dès J2 et remplacée par la ciprofloxacine Doit être poursuivie 3 à 5 jours pour maximiser son efficacité et diminuer la toxicité Doit être poursuivie au moins une semaine en évitant des vallées toxiques (monitoring)
")
39
Durée de traitement par les Aminosides
- En terme de pharmacodynamie: bactéricidie concentration-dépendante résistance adaptative - Un traitement par AG ne devrait nécessiter que 2 ou 3 doses à posologie élevée, en DUJ.

40
LA RESISTANCE ADAPTATIVE Gilleland (1988-9), Daikos (1990-1), Barclay (1990), Gould (1991)
= effet 1ère dose, 1ère exposition Élévation régulière de la CMI de la population bactérienne sous l’action de l’administration répétée d’AG Phénomène réversible de diminution de perméabilité de la bactérie aux AG Entraîne une diminution de la bactéricidie et de la valeur de l’EPA AG et BGN Décrite in vitro (statique et dynamique), in vivo Phénomène pH et PO2 dépendant (trans-porteurs) Durée: h (liée à l’espèce bactérienne: P. aeruginosa > E. coli)
, in vivo. Phénomène pH et PO2 dépendant (trans-porteurs) Durée: h (liée à l’espèce bactérienne: P. aeruginosa > E. coli)")
41
RESISTANCE ADAPTATIVE CMI; modèle statique in vitro
tobramycine P. aeruginosa D’après Karlowsky et al, JAC, 1994, 33,

42
RESISTANCE ADAPTATIVE Bactéricidie; modèle statique in vitro
tobramycine P. aeruginosa log10 CFU/ml contact = 2h D’après Karlowsky et al, JAC, 1994, 33,

43
RESISTANCE ADAPTATIVE EPA; modèle statique in vitro
tobramycine P. aeruginosa minutes D’après Karlowsky et al, JAC, 1994, 33,

44
RESISTANCE ADAPTATIVE Mucoviscidose
BACTERICIDIE (log10 CFU/ml) P. aeruginosa tobramycine 1 dose = 80 mg D’après Barclay et al, JAC, 1996, 37,
 P. aeruginosa tobramycine. 1 dose = 80 mg. D’après Barclay et al, JAC, 1996, 37,")
45
DUREE DU TRAITEMENT PAR LES AG Toxicité rénale et auditive
- En terme de toxicité rénale et auditive: Bertino et al. JID, 1993, 167, 173-9 Maller et al. JAC, 1993, 31, Prins et al. JAC, 1994, 33, - Un traitement par AG ne devrait pas dépasser une durée de 6 à 7 jours, au grand maximum.

47
CMI

48
Pharmacocinétique/pharmacodynamie

49
β-Lactamines La Bactéricidie dépend du temps à C > CMI
Souris neutropéniques infectées à K. pneumoniae après 24h de Céfotaxime ○ penicillines ▲ céphalosporines Craig, Diagn Microbiol Infect Dis 1996

50
Effet Post-ATB Définition : Maintien de l’inhibition de la croissance bactérienne alors que C<CMI Mécanisme Temps de dissociation ATB-Cible Temps nécessaire à la bactérie pour réparer sa cible ATB : β-lactamines => Cocci Gram + Aminosides, FQ, Ceftazidime, Imipeneme => BGN pH acide, inoculum élevé ⇒ ↓ EPA

51
ATB Temps-dépendant ATB : β-Lactamines, Glycopeptides, macrolides
Caractéristiques de le bactéricidie: Lente Dépend du temps de contact d’une concentration seuil EPA faible La bactéricidie dépend du T> CMI Log10 CFU/mL Craig, Scand Infect Dis 1991

52
ATB Concentration-Dépendant
ATB : Aminosides, Fluoroquinolones Caractéristiques de la bactéricidie Rapide et intense Augmente avec la concentration EPA Bactéricidie dépend Aminosides : Cmax/CMI FQ : ASC/CMI Craig, Scand Infect Dis 1991

53
Relation ASC de ciprofloxacine/CMI
et activité microbiologique et clinique Forrest et al, AAC, 1993

55
Pharmacodynamie des fluoroquinolones: conclusions
Concentration et dose-dépendance Pic/CMI et ASC/CMI Valeurs seuils prédicitives de l’activité in vivo: pour pic/CMI - 100 pour ASC/CMI • efficacité • émergence de la résistance Impact majeur de la CMI sur l’activité

56
Catégorie intermédiaire
Sensibilité aux ATB Définie à partir des concentrations critiques supérieures et inférieures C = Concentration critique supérieure : + grande quantité d’ATB actif dans le serum c = Concentration critique inférieure : Quantité d’ATB actif dans le serum après injection d’une dose normale d’ATB c C Catégorie Sensible Catégorie intermédiaire Catégorie Résistante CMI

57
Sensibilité aux ATB Exemple d’ Enterobacter sp Antibiogramme et CMI :
Bactérie 1 : CMI pour le Céfotaxime 0,01 mg/L => S Bactérie 2 : CMI pour le Céfotaxime 3 mg/L => S En Pratique pour une concentration d’ATB actif = 5μg/mL Bactérie 1 : 500 fois la CMI Bactérie 2 : 1,66 fois la CMI

58
Distribution de la sensibilité d’une population bactérienne
Nb de CFU S I R CMI g/mL

59
Emergence de Résistance
Acquisition de résistances : Par mutation : taux habituel entre 10-8 à 10-7 Extra-chromosomiques : transmission grâce à un plasmide ou transposon Facteurs prédictifs de l’émergence de résistances: ASC/CMI Bactéries à risque : Pseudomonas aeruginosa Bactéries sécrétrices de beta-lactamases ATB à risque : Imipenem et FQ sur Pseudomonas aeruginosa

60
Emergence de Résistance
107 patients ayant une pneumonie nosocomiale 128 bactéries identifiées 4 Essais /5 ATB Thomas ACC 1998

61
Monothérapie vs. association dans les épisodes fébriles des neutropéniques: Méta-analyse
Pip-taz +/- Akn Caz +/- Akn Caz +/- Gen Cpz +/- Akn Mortalité Aucun avantage des associations sur l’efficacité thérapeutique dans les sous-groupes testés, sauf celui “neutropénie sévère” (RR monothérapie 1.5 [ ]) Paul & al, BMJ 2003; 326: 1111
 Paul & al, BMJ 2003; 326:")
62
Les Associations béta-lactamines-aminosides préviennent-elles l’émergence de résistance (Gram -) ?
(Rubinstein, 95) Caz / Cro-Tob (Cometta, 94) Imp / Imp-Net (Croce 93) Cep (Caz) / Cep (Caz)-Gen (GA study, 92) Imp / Ctx-Gen (Gerercht, 89) Mez / Amp-Gen (Mandell, 87) Caz / Cfz (Tic)-Tob (Cone, 85) Caz / Tic-Tob (Gribble, 83) Pip / Tic-Tob N / N 197 / 188 98 / 101 39 / 70 94 / 68 24 / 22 37 / 38 21 / 19 21 / 17 Monothérapie associée à moins de surinfections (OR, 0.62; 95% CI, 0.42–0.93) et moins d’échecs (OR, 0.62; 95% CI, 0.38–1.01). IA. Bliziotis & al, CID 2005; 41:
 Caz / Cro-Tob. (Cometta, 94) Imp / Imp-Net. (Croce 93) Cep (Caz) / Cep (Caz)-Gen. (GA study, 92) Imp / Ctx-Gen. (Gerercht, 89) Mez / Amp-Gen. (Mandell, 87) Caz / Cfz (Tic)-Tob. (Cone, 85) Caz / Tic-Tob. (Gribble, 83) Pip / Tic-Tob. N / N. 197 / / / / / / / / 17. Monothérapie associée à moins de surinfections (OR, 0.62; 95% CI, 0.42–0.93) et moins d’échecs (OR, 0.62; 95% CI, 0.38–1.01). IA. Bliziotis & al, CID 2005; 41:")
63
Beta-lactam monotherapy vs
Beta-lactam monotherapy vs. b-lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and meta-analysis of randomised trials. Risque de mortalité (toutes causes), même béta-lactamine Paul & al, BMJ 2003; 326: 1111
, même béta-lactamine. Paul & al, BMJ 2003; 326:")
64
Beta-lactam monotherapy vs
Beta-lactam monotherapy vs. b-lactam-aminoglycoside combination therapy for sepsis in immunocompetent patients: systematic review and meta-analysis of randomised trials. Risque d’échec clinique Paul & al, BMJ 2003; 326: 1111

65
Relation entre Traitement Empirique et ‘définitif’ et survie dans les bactériémies à P. aeruginosa
Analyse multivariée du risque de décès Antibiothérapie initiale aHR IC P Association adéquate 1 - _ Monothérapie adéquate 3.7 0.05 Inadéquate 5.0 0.02 Antibiothérapie finale aHR IC P Association adéquate 1 - _ Monothérapie adéquate 0.7 0.42 Inadéquate 2.6 0.04 Surgical ICU Non Oui 1.0 3.2 1.2 - 8.9 0.02 Urinary or vascular source No Yes 0.21 0.05 0.94 0.04 Chamot et al, AAC 2003; 47: 2756

66
Intérêt de la bithérapie dans le traitement des PAVM
176 pneumopathies à P. aeruginosa; 54% décès en réa Nb d’ATB empiriques efficaces aOR 0 (15%) 1 (46%) 2 (39%) 1 1.0 ( ) 0.5 ( ) F. Vargas, ... D. Gruson, SRLF 2007
 1 (46%) 2 (39%) ( ) 0.5 ( ) F. Vargas, ... D. Gruson, SRLF")
67
EUCAST: http://217.70.33.99/Eucast2/SearchController/regShowAll.jsp?Title=Pseudomonas%20aeruginosa

69
Objectives: Pseudomonas aeruginosa is a major causative agent of hospital infections. The purpose
of this study was to determine the antibiotic susceptibility of P. aeruginosa in a French multicentre study and to investigate the mechanisms of b-lactam resistance. Methods: Four hundred and fifty non-repetitive strains of P. aeruginosa were collected in 15 French university hospitals in MICs of antibiotics were measured by agar dilution methods. For all the strains with MICs of ticarcillin >16 mg/L, detection and identification of the b-lactamases, quantitative determination of cephalosporinase and overproduction of the MexAB-OprM efflux pump were evaluated. Results: The percentages of susceptible isolates were as follows: ticarcillin, 62%; ticarcillin1clavulanic acid, 61%; piperacillin, 78%; piperacillin1tazobactam, 80% (MICs 16 mg/L); aztreonam, 50%; ceftazidime, 78%; cefepime, 64%; imipenem, 83%; tobramycin, 80% (MICs 4 mg/L); amikacin, 86% (MIC 8 mg/L); ciprofloxacin, 68%; and levofloxacin, 57% (MICs 1 mg/L). Decreased susceptibility to imipenem was linked in two cases to VIM-type carbapenemase production. Overexpression of the AmpC cephalosporinase, production of acquired b-lactamases including SHV2a extended-spectrum b-lactamase and overproduction of the MexAB-OprM efflux pump were present in 16.9%, 6.5% and 22.3% of the strains, respectively. Conclusions: In the last decade, the overall susceptibility of P. aeruginosa hospital isolates to antibiotics has remained quite stable in France. However, the emergence of extended-spectrum b-lactamases and carbapenemases in different locations is a matter of concern.
; aztreonam, 50%; ceftazidime, 78%; cefepime, 64%; imipenem, 83%; tobramycin, 80% (MICs 4 mg/L); amikacin, 86% (MIC 8 mg/L); ciprofloxacin, 68%; and levofloxacin, 57% (MICs 1 mg/L). Decreased susceptibility to. imipenem was linked in two cases to VIM-type carbapenemase production. Overexpression of the. AmpC cephalosporinase, production of acquired b-lactamases including SHV2a extended-spectrum. b-lactamase and overproduction of the MexAB-OprM efflux pump were present in 16.9%, 6.5% and. 22.3% of the strains, respectively. Conclusions: In the last decade, the overall susceptibility of P. aeruginosa hospital isolates to antibiotics. has remained quite stable in France. However, the emergence of extended-spectrum b-lactamases. and carbapenemases in different locations is a matter of concern.")
71
G. Potel et al. / Réanimation 15 (2006) 188 187–192
 –192")
72
VD élevé, mauvaise diffusion tissulaire Augmentation de posologie, dose de charge

73
Elimination perturbée intervalle d’administration

74
Distribution de la pipéracilline au cours d’un choc septique
pipéracilline 4 g en 10 min APACHE [36-66] microdialyse : muscle - tissu adipeux SC Objective: Current guidelines for adjusting antimicrobial therapy regimens commonly are based on drug concentrations measured in plasma. In septic patients, however, the interstitial space of soft tissues in addition to the central compartment represents the target site of infection. We thus hypothesized that one explanation for therapeutic failure during antibiotic treatment might be the inability to achieve effective antimicrobial concentrations in the interstitial space fluid of soft tissues. This is corroborated by the fact that piperacillin, a frequently administered b-lactam antibiotic, often fails to be effective despite documented susceptibility of the causative pathogen in vitro. Design: Prospective comparative study of two groups. Setting: The intensive care unit and research ward of an university hospital. Subjects: Six patients with septic shock and a control group of six gender- and age-matched healthy volunteers. Interventions: To measure piperacillin penetration into the interstitial space fluid of skeletal muscle and subcutaneous adipose tissue, we employed microdialysis after a single intravenous administration of 4.0 g of piperacillin to patients and healthy volunteers. Piperacillin concentrations were assayed by using reversed-phase high-pressure liquid chromatography. Measurements and Main Results: In septic shock patients, interstitial piperacillin concentrations in skeletal muscle and subcutaneous adipose tissue were five- to ten-fold lower than corresponding free plasma concentrations (p < .03). Mean piperacillin concentrations in subcutaneous adipose tissue never exceeded 11 mg/mL, which is below the minimal inhibitory concentration for a range of relevant pathogens in patients with septic shock. Conclusion: The results of the present study demonstrate that in septic shock patients, piperacillin concentrations in the interstitial space may be subinhibitory, even though effective concentrations are attained in plasma. The lack of success of antimicrobial therapy in these patients thus might be attributable to inadequate target site penetration of antibiotics. (Crit Care Med 2001; 29:385–391) Joukhadar et al - Crit Care Med 2001; 29:385–391 74
. Mean piperacillin concentrations. in subcutaneous adipose tissue never exceeded 11 mg/mL, which is below the minimal inhibitory concentration for a range of. relevant pathogens in patients with septic shock. Conclusion: The results of the present study demonstrate that. in septic shock patients, piperacillin concentrations in the interstitial. space may be subinhibitory, even though effective concentrations. are attained in plasma. The lack of success of antimicrobial. therapy in these patients thus might be attributable to. inadequate target site penetration of antibiotics. (Crit Care Med. 2001; 29:385–391) Joukhadar et al - Crit Care Med 2001; 29:385–")
75
Diffusion pulmonaire de la ceftazidime (2g IV puis 4 g PSE)
Diffusion pulmonaire de la ceftazidime (2g IV puis 4 g PSE) Boselli et al – Intens care med 2004; 30:989 CAZ (serum) CAZ (ELF) Breakpoint=8µg/ml
 Boselli et al – Intens care med 2004; 30:989. CAZ (serum) CAZ (ELF) Breakpoint=8µg/ml.")
76
x=observed, y=predicted (based on SC and Fup)
Abstract Objective: Drug dosing during continuous venovenous hemofiltration (CVVH) is based partly upon the CVVH clearance (ClCVVH) of the drug. ClCVVH is the product of the sieving coefficient (SC) and ultrafiltration rate (Quf). Although it has been suggested that the SC can be replaced by the fraction of a drug not bound to protein (Fup), the Fup values as reported in the literature may not reflect the protein binding in critically ill patients with renal failure. We compared the observed ClCVVH (SC × Quf) with the estimated ClCVVH (estimated FUP × Quf) and determined the effect on the maintenance dose multiplication factor (MDMF). Design and setting: Clinical study in a mixed ICU in a university hospital. Patients: 45 oligoanuric patients on CVVH (2 l/h). Interventions: Timed blood and ultrafiltrate samples. Measurements and results: Amoxicillin, ceftazidime, ciprofloxacin, fluconazole, metronidazole, and vancomycin were easily filtered (mean SC > 0.7) but not flucloxacillin (mean SC 0.3). Predicted and observed ClCVVH corresponded only for fluconazole and metronidazole. The difference between observed and predicted MDMF was small for all drugs, with the exception of ceftazidime (mean 0.25, 95% CI –0.96 to 1.48) and vancomycin (0.05, –1.34 to 1.45). However, this difference was clinically relevant only for vancomycin, because of its narrow therapeutic index. Conclusions: Dosing based on predicted CVVH removal provides an as reliable estimate than that based on observed CVVH removal except for those antibiotics that have both a narrow therapeutic index and a predominantly renal clearance (e.g., vancomycin). x=observed, y=predicted (based on SC and Fup)
 is based. partly upon the CVVH clearance. (ClCVVH) of the drug. ClCVVH is the. product of the sieving coefficient. (SC) and ultrafiltration rate (Quf). Although it has been suggested that. the SC can be replaced by the fraction. of a drug not bound to protein (Fup), the Fup values as reported in the. literature may not reflect the protein. binding in critically ill patients. with renal failure. We compared the. observed ClCVVH (SC × Quf) with. the estimated ClCVVH (estimated. FUP × Quf) and determined the effect. on the maintenance dose multiplication. factor (MDMF). Design and. setting: Clinical study in a mixed. ICU in a university hospital. Patients: 45 oligoanuric patients on. CVVH (2 l/h). Interventions: Timed. blood and ultrafiltrate samples. Measurements and results: Amoxicillin, ceftazidime, ciprofloxacin, fluconazole, metronidazole, and vancomycin. were easily filtered (mean. SC > 0.7) but not flucloxacillin. (mean SC 0.3). Predicted and observed. ClCVVH corresponded only. for fluconazole and metronidazole. The difference between observed. and predicted MDMF was small. for all drugs, with the exception of. ceftazidime (mean 0.25, 95% CI. –0.96 to 1.48) and vancomycin (0.05, –1.34 to 1.45). However, this difference. was clinically relevant only for. vancomycin, because of its narrow. therapeutic index. Conclusions: Dosing based on predicted CVVH removal. provides an as reliable estimate. than that based on observed CVVH. removal except for those antibiotics. that have both a narrow therapeutic. index and a predominantly renal. clearance (e.g., vancomycin). x=observed, y=predicted (based on SC and Fup)")
77
Perf continue Antibiotiques temps dépendants ½ vie courte
Effet post-antibiotique faible (CPM basse) Concentration libre tissulaire / CMI faible CMI élevée ou limite Site difficile d’accès
 Concentration libre tissulaire / CMI faible. CMI élevée ou limite. Site difficile d’accès.")
78
Continuous infusion b-lactams for intensive care unit pulmonary infections C. R. Frei and D. S. Burgess - Clin Microbiol Infect 2005; 11: 418–421 This study evaluated the pharmacodynamics of continuous infusion b-lactams against pulmonary isolates of Gram-negative bacteria from patients managed in intensive care units (ICUs) in the USA. Multiple patient Monte Carlo simulations were performed by integrating pharmacokinetic data from healthy individuals with 2408 MICs from the 2002 Intensive Care Unit Surveillance System database. These pharmacodynamic simulations suggested that continuous infusion regimens of cefepime, aztreonam, ceftazidime and piperacillin–tazobactam 13.5 g have the greatest likelihood of achieving pharmacodynamic targets against isolates of Enterobacteriaceae in the ICU. b-Lactams are unlikely to achieve pharmacodynamic targets against Pseudomonas aeruginosa or Acinetobacter baumannii when administered as monotherapy.
 in the. USA. Multiple patient Monte Carlo simulations. were performed by integrating pharmacokinetic. data from healthy individuals with MICs from the 2002 Intensive Care Unit Surveillance. System database. These pharmacodynamic. simulations suggested that continuous infusion. regimens of cefepime, aztreonam, ceftazidime. and piperacillin–tazobactam 13.5 g have the. greatest likelihood of achieving pharmacodynamic. targets against isolates of Enterobacteriaceae in. the ICU. b-Lactams are unlikely to achieve pharmacodynamic. targets against Pseudomonas aeruginosa. or Acinetobacter baumannii when administered. as monotherapy.")
79
Meropenem by continuous versus intermittent infusion in ventilator-associated pneumonia due to gram-negative bacilli. 1 g X 4 vs 4 g continuous + tobramycin 7mg/kg/d (both groups) Continuous (n=42) Intermittent (n=47) P value Age 57.2 56.5 0.8 APACHE II 15.3 15.2 0.88 Cl Creat 101 102 0.81 SOFA (VAP) 8.64 8.52 MICs 0.54 0.48 Cure rate 90.5% 59.6% <0.0001 Cure rate (P. aeruginosa) 84.6% 40% Cure rate if MIC> 0.5 81% 29.4% <0.001 BACKGROUND: It is known that beta-lactam antibiotics exhibit time-dependent bactericidal activity. Several studies have found continuous infusion of meropenem more effective than intermittent infusion in maintaining constant serum concentrations in excess of the minimum inhibitory concentration. However, limited data exist on the clinical efficacy of meropenem administered by continuous infusion. OBJECTIVE: To evaluate the clinical efficacy of continuous versus intermittent infusion of meropenem for the treatment of ventilator-associated pneumonia (VAP) due to gram-negative bacilli. METHODS: A retrospective cohort study was conducted of patients with VAP caused by gram-negative bacilli who received initial empiric antibiotic therapy with meropenem. We analyzed 2 contemporary cohorts: one group received meropenem by continuous infusion (1 g over 360 min every 6 h), the other by intermittent infusion (1 g over 30 min every 6 h). The administration method was prescribed according to the physician's discretion. Patients received meropenem plus tobramycin for 14 days. RESULTS: There were no significant differences between patient groups with regard to gender, age, APACHE-II at intensive care unit admission, diagnosis, microorganism responsible for VAP, or organ dysfunction severity at the time VAP was suspected. The group receiving medication by continuous infusion showed a greater clinical cure rate than the group treated with intermittent infusion (38 of 42, 90.47%, vs 28 of 47, 59.57%, respectively, with OR 6.44 [95% CI 1.97 to 21.05; p < 0.001]). CONCLUSIONS: Meropenem administered by continuous infusion may have more clinical efficacy than intermittent infusion. But retrospective, mortality not reported, dosage not performed Lorente et al – Ann Pharmacother 2006; 40:219
 Continuous (n=42) Intermittent (n=47) P value. Age APACHE II Cl Creat SOFA (VAP) MICs Cure rate. 90.5% 59.6% < Cure rate (P. aeruginosa) 84.6% 40% Cure rate if MIC> % 29.4% < BACKGROUND: It is known that beta-lactam antibiotics exhibit time-dependent bactericidal activity. Several studies have found continuous infusion of meropenem more effective than intermittent infusion in maintaining constant serum concentrations in excess of the minimum inhibitory concentration. However, limited data exist on the clinical efficacy of meropenem administered by continuous infusion. OBJECTIVE: To evaluate the clinical efficacy of continuous versus intermittent infusion of meropenem for the treatment of ventilator-associated pneumonia (VAP) due to gram-negative bacilli. METHODS: A retrospective cohort study was conducted of patients with VAP caused by gram-negative bacilli who received initial empiric antibiotic therapy with meropenem. We analyzed 2 contemporary cohorts: one group received meropenem by continuous infusion (1 g over 360 min every 6 h), the other by intermittent infusion (1 g over 30 min every 6 h). The administration method was prescribed according to the physician s discretion. Patients received meropenem plus tobramycin for 14 days. RESULTS: There were no significant differences between patient groups with regard to gender, age, APACHE-II at intensive care unit admission, diagnosis, microorganism responsible for VAP, or organ dysfunction severity at the time VAP was suspected. The group receiving medication by continuous infusion showed a greater clinical cure rate than the group treated with intermittent infusion (38 of 42, 90.47%, vs 28 of 47, 59.57%, respectively, with OR 6.44 [95% CI 1.97 to 21.05; p < 0.001]). CONCLUSIONS: Meropenem administered by continuous infusion may have more clinical efficacy than intermittent infusion. But retrospective, mortality not reported, dosage not performed. Lorente et al – Ann Pharmacother 2006; 40:219.")
Présentations similaires





>")






 Biomarqueurs IHC (n = 412) Séquençage (n = 418) 200 patients évaluables pour les facteurs pronostiques cliniques et biologiques Comparaison.>")




>")



