Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Insuffisance rénale aiguë
01/04/2017 Insuffisance rénale aiguë Traitement médical Epuration extra-rénale D. Journois, HEGP

2
Diurétiques Expérimental -> l’atteinte rénale résulte de :
vasoconstriction ; réduction de perméabilité capillaire ; obstruction tubulaire ; rétrodiffusion de l’ultrafiltrat ; ischémie. Etudes cliniques Pas d’efficacité (Hager, 1996) Diurèse seulement (Kleinknecht, 1976 ; Brown, 1981)
 Diurèse seulement (Kleinknecht, 1976 ; Brown, 1981)")
3
Diurétiques Produisent une diurèse (rassurante) ; Déshydratent ;
Réduisent la volémie ; Ne sont efficaces qu’associés à une inflation hydrique ; Doivent être réservés : hypervolémie ; hyperchlorémie (diurétiques de l’anse) ; indications spécifiques (hyperkaliémie, OAP).
 ; indications spécifiques (hyperkaliémie, OAP).")
4
Dopamine Natriurétique/Diurétique (alpha, beta, DA1, DA2…)
Notion de dose « dopaminergique » 30 études cliniques : 3 positives (niveaux III-V) ; 27 négatives (700 pts, niveau II-V). Arguments contre : Ischémie mésentérique (Segal, J Appl Physiol, 1992) Gangrènes de extrémités (NEJM 1976)
 ; 27 négatives (700 pts, niveau II-V). Arguments contre : Ischémie mésentérique (Segal, J Appl Physiol, 1992) Gangrènes de extrémités (NEJM 1976)")
5
Swygert, Anesthesiology 1988 (Transplantation hépatique)
dopamine placebo Créat. 180 160 140 120 100 80 60 40 20 day 0 day 1 day 3 day 5 day 7

6
Produits de contraste Dopamine : détériore la fonction rénale (Hall) ;
Diurétiques : délétères (Weinstein, Solomon) ; Mannitol : moins efficace que l’hydratation ; Inhibiteurs calciques : efficaces hors situations cliniques ; Hyperhydratation N-acétylcystéine ; Théophylline.
 ; Mannitol : moins efficace que l’hydratation ; Inhibiteurs calciques : efficaces hors situations cliniques ; Hyperhydratation. N-acétylcystéine ; Théophylline.")
7
Indications de l’EER Situations « classiques » : Indications réelles :
hyperkaliémie ; inflation hydrique ou volémique ; acidose (à TA élevé sans lactate) ; urémie Indications réelles : Objectifs Survie ? Physiologie ? Supra-physiologiques ?
 ; urémie. Indications réelles : Objectifs. Survie Physiologie Supra-physiologiques")
8
Hémodialyse Sortie dialysat Entrée dialysat Entrée sang Sortie sang
01/04/2017 Hémodialyse Sortie dialysat Entrée dialysat Entrée sang Sortie sang effluent (du patient) (vers patient) CONC. ELEVEE FAIBLE CONC
 (vers patient) CONC. ELEVEE. FAIBLE CONC.")
9
Ultrafiltration Entrée Sang Réduction Volume plasmatique Sortie sang
01/04/2017 Ultrafiltration Entrée Sang Sortie sang Effluent (du patient) (vers patient) PRESSION ELEVEE FAIBLE PRESS Réduction Volume plasmatique Restitution
 (vers patient) PRESSION ELEVEE. FAIBLE PRESS. Réduction Volume. plasmatique. Restitution.")
10
Différences HF / HD: Modalités d’équilibration
Poids moléculaire des substances éliminées

11
Equilibre électrolytique en CVVH
substitution 450ml/h Na+ 150 mEq/l Cl- 114 mEq/l K HCO mEq/l Mg mEq/l Ca mEq/l Ultrafiltrat 600ml/h Na+ 140 mEq/l Cl- 100 mEq/l K mEq/l PO mEq/l Creat mg/dl urée mg/dl balance liquide ml/h Na+ -16 mEq/h Cl mEq/h K mEq/h Creat mg/h urée mg/h

12
Composition de solutions
Citrate HEGP Hemosol K0 K2 K4 RL EL00 Physio Plasmion Bic14 Na K ,4 0/2 5 Cl Ca Mg Glucose Citrate 8 Lactate Bicarbonate

13
01/04/2017 Clairances usuelles

14
} Poids Moléculaires • Albumin (55,000 - 60,000)
01/04/2017 Poids Moléculaires • Albumin (55, ,000) • Beta 2 Microglobulin (11,800) • Inulin (5,200) • Vitamin B12 (1,355) • Aluminum/Desferoxamine Complex (700) • Glucose (180) • Uric Acid (168) • Creatinine (113) • Phosphate (80) • Urea (60) • Phosphorus (31) • Sodium (23) • Potassium (35) 100,000 50,000 10,000 5,000 1,000 500 100 50 10 5 Poids molecul. daltons } “petites” “moyennes” “Grosses”
 • Beta 2 Microglobulin (11,800) • Inulin (5,200) • Vitamin B12 (1,355) • Aluminum/Desferoxamine Complex (700) • Glucose (180) • Uric Acid (168) • Creatinine (113) • Phosphate (80) • Urea (60) • Phosphorus (31) • Sodium (23) • Potassium (35) 100, , ,000. 5,000. 1, Poids. molecul. daltons. } petites moyennes Grosses")
15
CAVH Heparin Blood circuit Hemofilter Ultrafiltrate

16
Pressions Usuelles Durant le Traitement
01/04/2017 Pressions Usuelles Durant le Traitement Pression Accès Negative -50 to -150 mmHg Pression Filtre Positive +100 to +250 mmHg Pression Effluente Négative ou Positive > +50 mmhg to -150 mmHg Pression Retour Positive +50 to +150 mmHg

17
Description d’un hémofiltre
01/04/2017 Description d’un hémofiltre Entrée sang Coupe Sortie dialysat Membrane capillaire Extérieur des Fibres (effluent) Intérieur des Fibres (Sang) Entrée dialysat Sortie sang
 Intérieur des Fibres (Sang) Entrée. dialysat. Sortie sang.")
18
Membrane d’hémofiltre
01/04/2017 Membrane d’hémofiltre

19
Pression osmotique Volume Volémie Extravasculaire
01/04/2017 Pression osmotique Volémie Extravasculaire Hémofiltration Pression hydrostatique Pression oncotique Volume

20
Hypovolémie Pression osmotique Volume Volémie Extravasculaire CRRT
01/04/2017 Pression osmotique Hypovolémie Volémie Extravasculaire CRRT Pression hydrostatique Pression Oncotique Volume

21
Précharge cardiaque - Loi de Franck Starling
01/04/2017 Précharge cardiaque - Loi de Franck Starling Volume d’éjection ventriculaire Précharge Ventriculaire

22
Volume vasculaire et fonction ventriculaire
01/04/2017 Volume vasculaire et fonction ventriculaire Pression oncotique Volume d’éjection ventriculaire 2 3 1 Volume Précharge

23
Evaluation volémique en CVVH
01/04/2017 Evaluation volémique en CVVH Volume d’éjection ventriculaire TEE TTE ITBV DPP PCWP CVP 3 Précharge MAP

24
Points «délicats» Température ; Elimination de nutriements ;
Cathéters ; Solutions de substitution.

25
Matamis D et al. Int Care Med 1994 : 20, 431
p<0.01

26
Equilibre thermique à 6 l/h d’ultrafiltration

28
Cathéters d’hémofiltration
IP

29
Comparaison de cathéters d ’hémofiltration

30
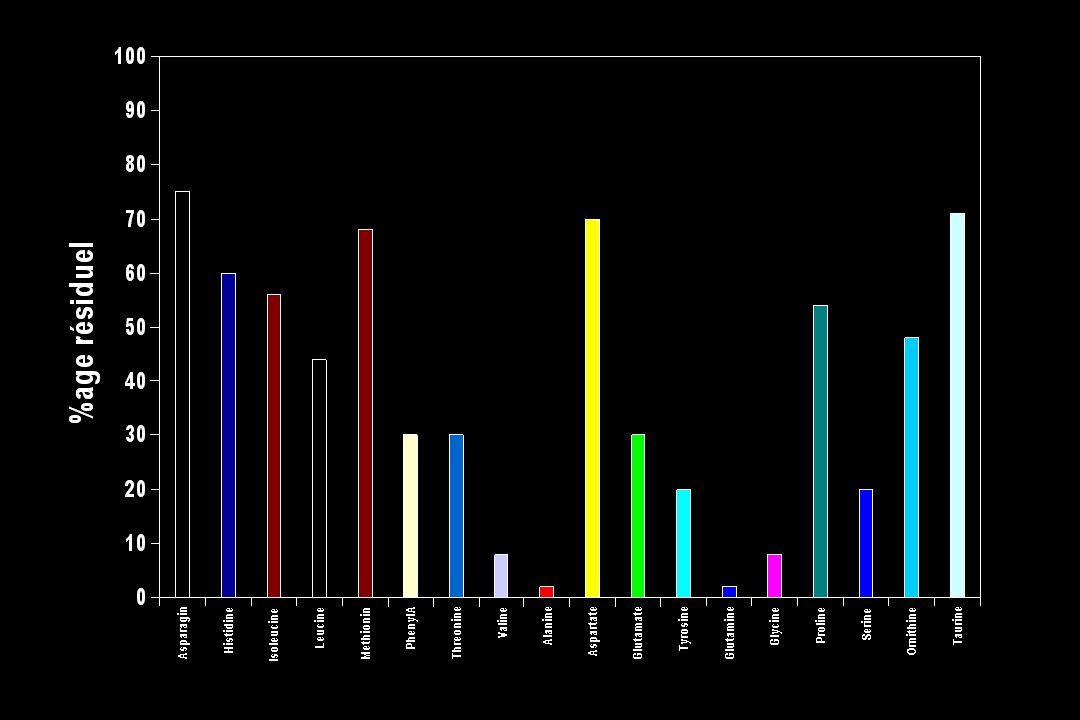
Cations

31
Indications spécifiques de l’HF
Etats septiques sévères Etats inflammatoires sévères

32
Gomez et al. Anesthesiology, Oct 1990

33
Filter Pore Size in Experimental Staphylococcal Bacteremia
01/04/2017 Filter Pore Size in Experimental Staphylococcal Bacteremia p < 0.03 No Animals Alive Lee et al. CCM 1998

34
TNF TNF IL-1 IL-8 IL-10 Trimère PM = 3 x 17000 instable
01/04/2017 TNF TNF IL-1 IL-8 IL-10 Trimère PM = 3 x 17000 instable Mesures bio & ag

35
IL-10 Cytokine « protectrice » PM = 14000

36
Removal of mediators Authors+ ref. Study Diagnosis Design CRRT UFR Mediators Clinical Delay to Patient UFV/hour subject and Technique ml/hour removal effects initiate body indexed to number severity mb + S therapy weight body size (1)Tonnesen 9 Sepsis P, Unc CAVH, TNF-, NA NA NA=75 kg 10 ml/kg/h E et al PS/S : NA IL-1 (E) (2) Gueugniaud 6 Burns, Rs, Unc CVVH, NA IL-6 MAP NA NA NA PY et al ARF PAN/S : NA (3) Wakabayashi 6 SIRS P, Unc CVVH NA IL-6,IL-8 MAP NA NA= 75 kg Na et al Mb&S:NA SVR = E (4) Hoffman 16 Sepsis P, Unc LV-CVVH C3a, C5a MAP NA NA= 75 kg 26 et al PA/S:NA SVR = E ml/kg/h(E) (5)Heering P 33 Sepsis, P, C LV-CVVH TNF-, MAP NA NA=75kg 13 et al ANF PS/S:1.35m2 IL-6,IL-8 CO = E ml/kg/h (E) (6) Sander A 26 SIRS R LV-CVVH IL-6 MAP NA NA = 75 kg 13 et al :CVVH CO = E ml.kg/h(E) 13:IHD PAN/S:0.6m2 (7)Kellum J 13 SIRS + R, Cros LV-CVVH TNF- NA NA NA= 75 kg 26 et al ARF CVHHD = E ml/kg/h(E) PAN/S:0.6m2 (8) De Vriese A 15 Sepsis P, Unc MV-CVVH TNF-, IL-6, in SVR NA NA = 75 kg 20 et al ARF PAN/S:1m IL-10,IL-1Ra, = E ml/kg/h (E) sTNFR-I, sTNFR-II ml/kg/h (E) (5) Heering P et al. Intensive Care Med 23; ,1997. (6) Sander et al. Intensive Care Med 23; ,1997. (7) Kellum J et al. Crit Care Med 26, ,1998. (8) De Vriese A et al. J Am Soc Nephrol 10;846-53:1999 P =Prospective, Unc = Uncontrolled, C = controlled, R = randomized, Cross = Cross over study, ARF = Acute Renal Failure, NA = Not Available, E = Estimated, RS = Retrospective (1) Tonnesen E et al. Anaesth Intens Care 21; , 1993. (2) Gueugniaud PY et al. Crit Care Med 22 ;717, 1994. (3) Wakabayashi et al. Br J Surg 83 ; ,1996 (4) Hoffman et al. Intensive Care Med 22; :1996.
Tonnesen 9 Sepsis P, Unc CAVH, 750 TNF-, NA NA NA=75 kg 10 ml/kg/h. E et al 1993 PS/S : NA IL-1 (E) (2) Gueugniaud 6 Burns, Rs, Unc CVVH, NA IL-6 MAP NA NA NA. PY et al 1994 ARF PAN/S : NA. (3) Wakabayashi 6 SIRS P, Unc CVVH NA IL-6,IL-8 MAP NA NA= 75 kg Na. et al 1996 Mb&S:NA SVR = E. (4) Hoffman 16 Sepsis P, Unc LV-CVVH 2000 C3a, C5a MAP NA NA= 75 kg 26. et al 1996 PA/S:NA SVR = E ml/kg/h(E) (5)Heering P 33 Sepsis, P, C LV-CVVH 1000 TNF-, MAP NA NA=75kg 13. et al 1997 ANF PS/S:1.35m2 IL-6,IL-8 CO = E ml/kg/h (E) (6) Sander A 26 SIRS R LV-CVVH 1000 IL-6 MAP NA NA = 75 kg 13. et al :CVVH CO = E ml.kg/h(E) 13:IHD. PAN/S:0.6m2. (7)Kellum J 13 SIRS + R, Cros LV-CVVH TNF- NA NA NA= 75 kg 26. et al 1998 ARF CVHHD = E ml/kg/h(E) PAN/S:0.6m2. (8) De Vriese A 15 Sepsis P, Unc MV-CVVH 1500 TNF-, IL-6, in SVR NA NA = 75 kg 20. et al ARF PAN/S:1m IL-10,IL-1Ra, = E ml/kg/h (E) sTNFR-I, 36. sTNFR-II ml/kg/h (E) (5) Heering P et al. Intensive Care Med 23; ,1997. (6) Sander et al. Intensive Care Med 23; ,1997. (7) Kellum J et al. Crit Care Med 26, ,1998. (8) De Vriese A et al. J Am Soc Nephrol 10;846-53:1999. P =Prospective, Unc = Uncontrolled, C = controlled, R = randomized, Cross = Cross over study, ARF = Acute Renal Failure, NA = Not Available, E = Estimated, RS = Retrospective. (1) Tonnesen E et al. Anaesth Intens Care 21; , (2) Gueugniaud PY et al. Crit Care Med 22 ;717, (3) Wakabayashi et al. Br J Surg 83 ; ,1996. (4) Hoffman et al. Intensive Care Med 22; :1996.")
37
IL-1 plasma reduction is not due to its removal
20 children, neonatal cardiac surgery randomisation : 180 ml/kg.h zero balanced UF vs 0 Clinical benefit : Lower PA-aO2, Reduced extubation delay Decreased temperature production Journois et al. Anesthesiology, Nov. 1996

38
+ n=21 n=19 n= 12 animal n= 16 humain n=7 n= 0 humain
01/04/2017 Elimination de médiateurs Bénéfice clinique lié à la convection Production de médiateurs n=19 n=21 n= 12 animal n= 16 humain Bénéfice clinique lié à la convection Elimination de médiateurs + n=7 Bénéfice clinique lié à la convection Elimination de médiateurs n= 0 humain

39
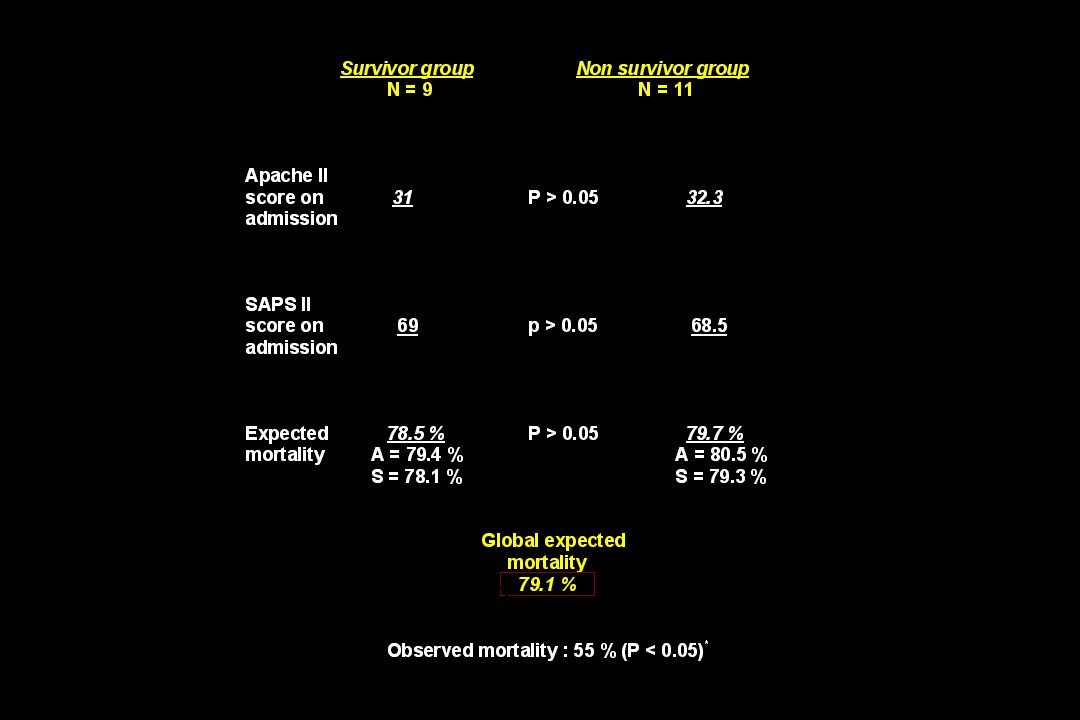
Intractable circulatory failure complicating severe septic shock
Clinical status before the start of the procedure 1° Hemodynamic status - MAP - Inotropic support : after failure of maximal dosages of dopamine and dobutamine-norepinephrine - Cardiac index - Wedge pressure 2° Acid-base balance - Arterial pH - Serum lactate 3° Septic status - SIRS criteria (ACCP/SCCM criteria) - Objective source of sepsis 4° Respiratory support - Mechanical ventilation - paO2/FIO2 ratio 5° Renal status - < 55 mmHg - Epinephrine not for more than 2 hours - < 2 l/min/m2 - > < 18 mmHg - < 7.15 - > 5 mmol/l - 3 out of 4 - Always present - All the patients - < 100 No incidence on the inclusion criteria Dopamine : up to 20 mg/Kg/min Norepinephrine : up to 2 mg/Kg/min Dobutamine : up to 14 mg/Kg/min Epinephrine : up to 0.5 mg/Kg/min
 - Objective source of sepsis. 4° Respiratory support. - Mechanical ventilation. - paO2/FIO2 ratio. 5° Renal status. - < 55 mmHg. - Epinephrine. not for more than 2 hours. - < 2 l/min/m2. - > 14 < 18 mmHg. - < > 5 mmol/l. - 3 out of 4. - Always present. - All the patients. - < 100. No incidence on the inclusion criteria. Dopamine : up to 20 mg/Kg/min Norepinephrine : up to 2 mg/Kg/min. Dobutamine : up to 14 mg/Kg/min Epinephrine : up to 0.5 mg/Kg/min.")
41
Effect of different doses of CVVH on survival
Ronco C. et al. Lancet 2000, 356:26-30 Group 3 = 45 ml/h.kg Group 2 = 35 ml/h.kg Group 1 = 20 ml/h.kg

42
Evidence levels

43
Grades de recommandation

Présentations similaires


![[number 1-100].](/1/172887/big_thumb.jpg "[number 1-100].>")





 Par Juli Powers>")










