Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Jacques Turgeon, B.Pharm., Ph.D. Professeur titulaire, Faculté de pharmacie, Université de Montréal Directeur de la recherche, CRCHUM Centre Hospitalier de l’Université de Montréal Interactions médicamenteuses et polymorphismes génétiques: Leur rôle dans la variabilité inter-individuelle dans la réponse aux médicaments

2
Pharmacologie Clinique PharmacocinétiquePharmacodynamique DoseConcentrationEffet

3
Healthy volunteers, 15-35 years of age, male Intersubject variability in drug response

4
Not all patients look alike, indeed! Intersubject variability in drug response

5
Pharmacologie Clinique PharmacocinétiquePharmacodynamique DoseConcentrationEffet Facteurs Physiologique Race Facteurs Génétiques SexeÂgePathologiesTempératureMédicamentsChronopharmacologieEnvironnement Variabilité Inter-individuelle

6
And some patients appear to be very different. Intersubject variability in drug response

7
Génétique et Pharmacogénétique Génétique + Environnement Concentration Protéine Effet Variabilité inter- individuelle dans la réponse aux médicamens Pathologie PD Dose PK

8
Génétique et Pharmacogénétique Pharmacogénétique Génétique + Environnement Médicament Protéine Effet Facteurs physiologiques Race Facteurs génétiques SexeÂgePathologiesTempératureMédicamentsChronopharmacologieEnvironnement Variabilité inter- individuelle dans la réponse aux médicamens Pathologie PD Dose PK

9
PharmacocinétiquePharmacodynamique DoseConcentrationEffet Facteurs Physiologique Race Facteurs Génétiques SexeÂgePathologiesTempératureMédicamentsChronopharmacologieEnvironnement Variabilité Inter-individuelle CYP450

10
Le système des cytochromes P450 SHSOH NADPH/H + O2O2O2O2 H2OH2OH2OH2O NADP + Transformer des substrats lipophiliques en produits hydro- phyliques

11
Intersubject variability in drug response CYP3 CYP1 CYP2

12
Variabilité Inter-individuelle dans les effets du nébivolol

13
Résultats 15 Métabolisateurs lents DM/DEX:0.002-0.182 203 Métabolisateurs rapides DM/DEX:0.333-6.667 14 Sujets étudiés 5 CYP2D6 *4/*4 3 CYP2D6 *4/*3 3 CYP2D6 *4/*5 2 CYP2D6 *5/*5 1 CYP2D6 *4/*6 218 patients phénotypés pour le CYP2D6 23 Contrôles appariés 13 CYP2D6 *1/*4 9 CYP2D6 *1/*1 1 CYP2D6 *1/*5 1180

14
Variabilité Inter-individuelle dans les effets du nebivolol Rapides Lents

15
Variabilité Inter-individuelle dans les effets du nebivolol

16
Génétique et Pharmacogénétique Génétique Médicament Protéine Effet Variabilité inter- individuelle dans la réponse aux médicamens Pathologie PD Dose PK

17
Génétique et Pharmacogénétique Génétique Protéine Variabilité inter- individuelle dans la réponse aux médicamens Pathologie

18
Renin Angiotensin System Angiotensinogen Angiotensin I Renin Angiotensin II ACE Classic understanding of RAS

19
Renin Angiotensin System D Allele I Allele Alu repeat Intron 16 190 pb 490 pb 26 exons, 25 introns 21 000 nucleotides ACE gene locus 5 ’ 3 ’ (-93 CT and -240 AC) (-93 C T and -240 A C)
 (-93 C T and -240 A C)")
20
Renin Angiotensin System ACE concentration ( g/L) IIIDDD II 299±49 g/L ID 393±67 g/L DD 494±88 g/L
 IIIDDD II 299±49 g/L ID 393±67 g/L DD 494±88 g/L")
21
Renin Angiotensin System 30 Controls MI Patients Allele frequency 35 40 45 50 55 16 82 208 336380416

22
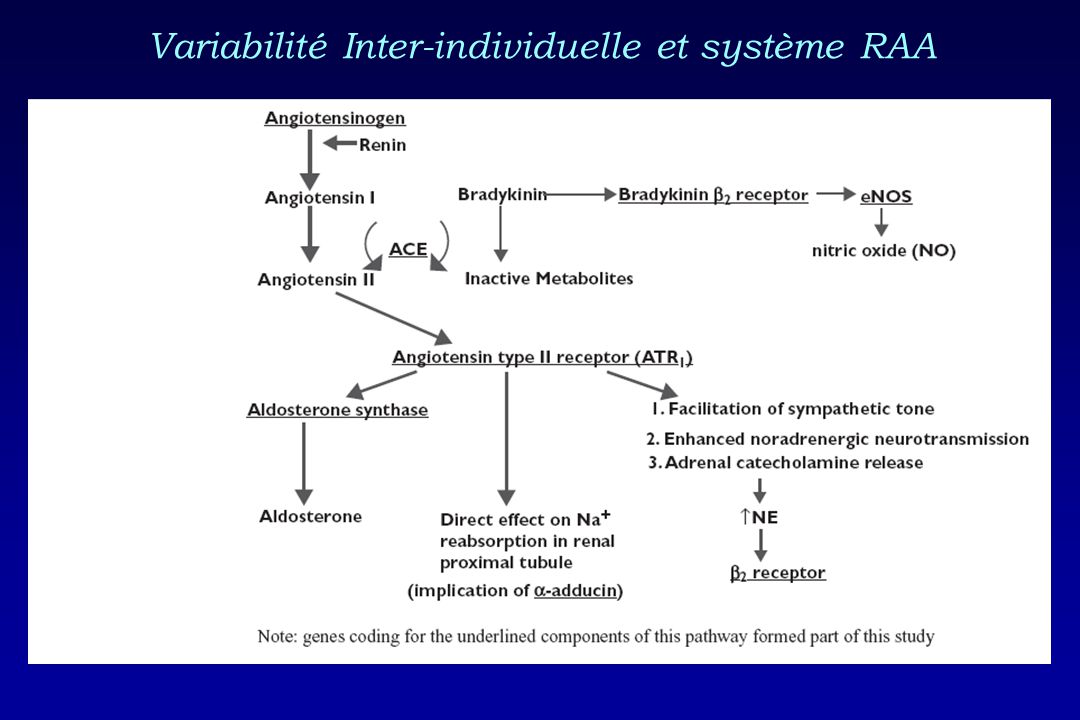
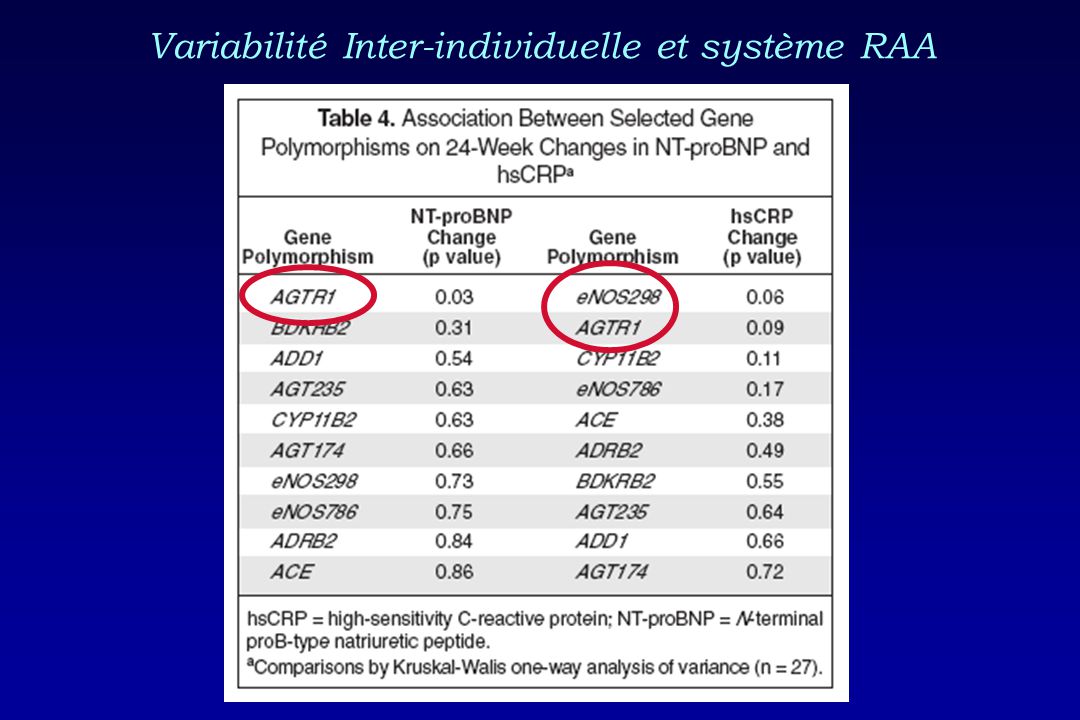
Variabilité Inter-individuelle et système RAA

26
PharmacocinétiquePharmacodynamique DoseConcentrationEffet Facteurs Physiologique Race Facteurs Génétiques SexeÂgePathologiesTempératureMédicamentsChronopharmacologieEnvironnement Variabilité Inter-individuelle

27
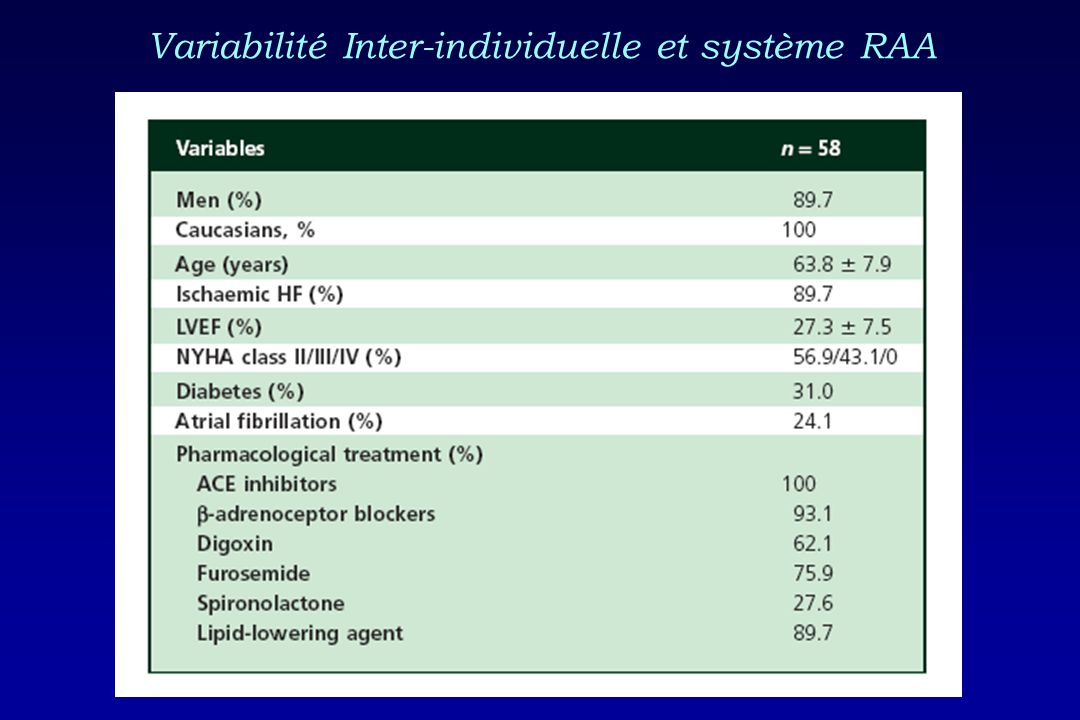
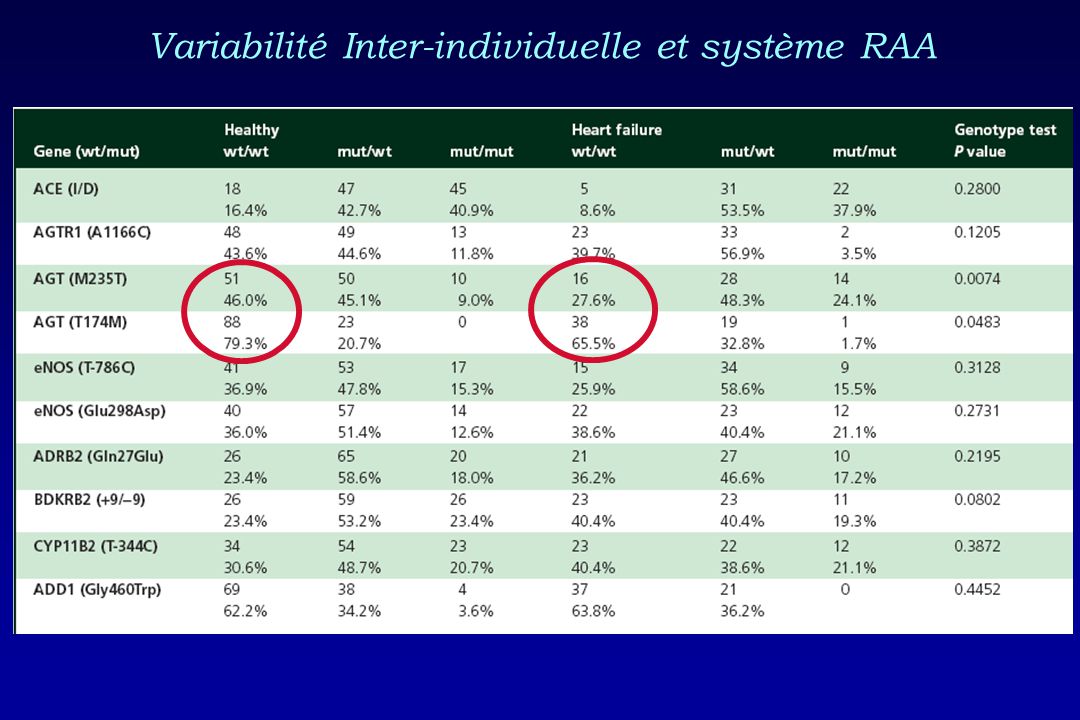
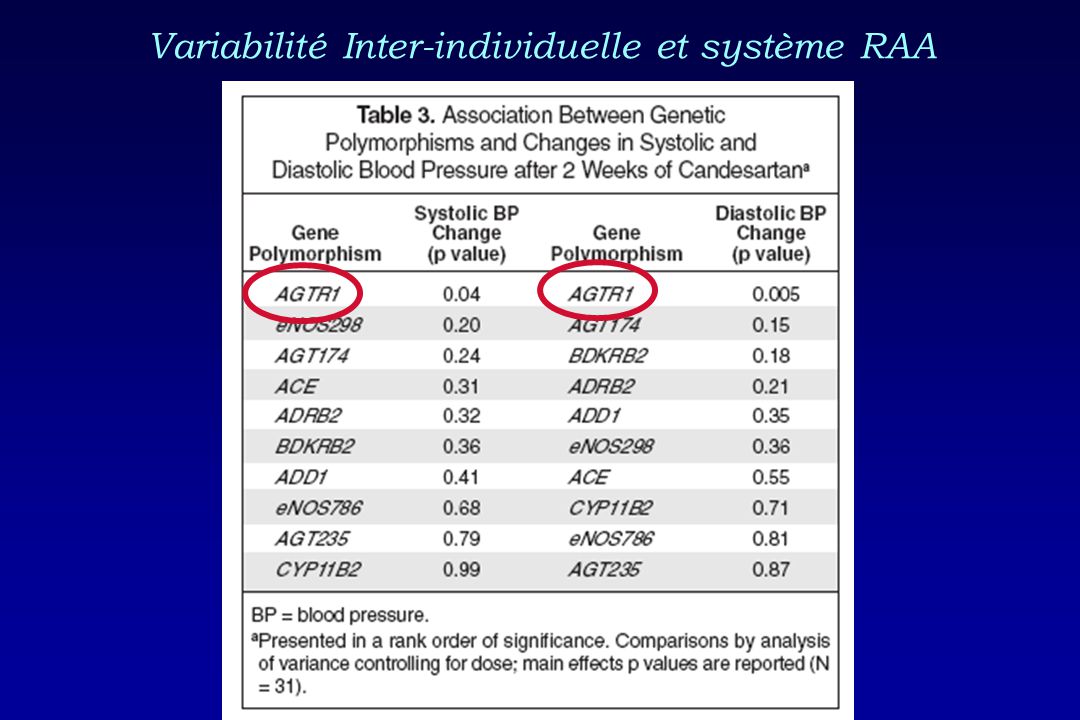
Variabilité Inter-individuelle et système RAA

30
Influence de polymorphismes génétiques du système rénine-angiotensine-aldostérone sur la réponse aux antagonistes des récepteurs AT 1 à l’angiotensine chez des patients présentant de l’hypertension artérielle. Jean Lefebvre, Luc Poirier, Jacques Turgeon, Yves Lacourcière

31
Résultats 85 (17%) HTA blouse blanche TAAMJ < 135/85 mmHg 428 HTA confirmée par MATA traités avec Losartan 523 patients hypertendus en clinique: génotypés 579 patients évalués période de wash-out 66 exclus TA clin <140/90 mmHg (41) Consentement retiré (9) Lab anormal (7) MATA non-valide (6) Autres (3)
 HTA blouse blanche TAAMJ < 135/85 mmHg 428 HTA confirmée par MATA traités avec Losartan 523 patients hypertendus en clinique: génotypés 579 patients évalués période de wash-out 66 exclus TA clin <140/90 mmHg (41) Consentement retiré (9) Lab anormal (7) MATA non-valide (6) Autres (3)")
32
Effets des polymorphismes étudiés sur la T.A. ambulatoire de base N II89 12.8149.0 12.6130,5 ID209 12.8149.2 13.3130,4 DD130 16.8150.3 17.0132,3 Thr/Thr 80 16.4152.6 16.3135 Thr/Met 204 14.0150.1 14.2130,7 Met/Met 144 12.7146.9 13.0129,8 CC 43 13.9148.7 14.0131,4 AC 183 13.5150.4 13.9131,8 AA 201 14.8148.9 14.9130,2 0.5520.5620.615 143.516,6 145.114,6 AT1R A1166C 143.716,0 0.019*0.010*0.039* 141.913,6 144.615,7 AGT Met 235 Thr 147.316,1 0.6300.7460.526 145.218,1 143.813,9 ABPM-Confirmed Hypertension (n=428) ACE-I/D 143.715,9 Systolic ABP 24-hourDaytimeNight-time
 ACE-I/D ,9 Systolic ABP 24-hourDaytimeNight-time.")
33
Polymorphisme AGT M 235 T et profile de tension artérielle ambulatoire des 24-h 7911131517192123135 70 80 90 100 Thr/Thr Thr/Met Met/Met 120 130 140 150 160 SBP P = 0.02* DBP P = 0.25 Hour of the day Blood pressure (mmHg)
")
34
Angiotensinogène Angiotensine I Angiotensine II Mécanisme probable de la toux aux IECA ECA Bradykinine Fragments inactifs Israili & Hall. Arch Intern Med 1992 Prostaglandines Leukotriènes PG E 2 récepteurs à adaption rapide Toux Acide Arachidonique BK B 2 R IECA ARA

35
Enalapril 20 mg Losartan 50 mg Patients présentant de la toux (%) HCTZ 12.5 mg 70 60 50 40 30 20 10 0 p<0.001 Losartan 50 Enalapril 20 HCTZ 12.5 Enalapril 20Placebo 8 semaines6 semaines4 semaines “Losartan Cough Study“ Rechallenge de la toux sous Losartan Lacourcière Y et al. J Hypertens 1994;12:1387-93

36
Sujets d’étude 75 cas: histoire de toux sèche aux inhibiteurs de l’ECA, confirmée par épreuve de challenge-déchallenge-rechallenge 150 contrôles: aucune toux sèche durant au moins 6 mois de traitement avec un inhibiteur de l’ECA; Appariement selon le sexe, l’âge et le poids dans un rapport 2:1 225 patients avec hypertension artérielle essentielle non compliquée:

37
Interaction des polymorphismes B 2 BKR(+9/-9) et ACE (I/D)
 et ACE (I/D)")
38
PharmacocinétiquePharmacodynamique DoseConcentrationEffet Facteurs Physiologique Race Facteurs Génétiques SexeÂgePathologiesTempératureMédicamentsChronopharmacologieEnvironnement Variabilité Inter-individuelle

39
FDA News: August 16 2007 New genetic information may help providers improve initial dosing estimates of the anticoagulant for individual patients.

40
Initiation of warfarin therapy represents a challenge: Narrow therapeutic index drug. Narrow therapeutic index drug. Effective daily doses vary widely from one patient to another (0.5 to 30 mg/day). Effective daily doses vary widely from one patient to another (0.5 to 30 mg/day). 6-8 weeks are required to achieve a therapeutic INR (2-3). 6-8 weeks are required to achieve a therapeutic INR (2-3). Pharmacogenetic trial with warfarin IntroductionHypothesisMethodsResultsDiscussionConclusions
. Effective daily doses vary widely from one patient to another (0.5 to 30 mg/day). 6-8 weeks are required to achieve a therapeutic INR (2-3). 6-8 weeks are required to achieve a therapeutic INR (2-3). Pharmacogenetic trial with warfarin IntroductionHypothesisMethodsResultsDiscussionConclusions.")
41
S-Warfarin R-Warfarin Effective daily doses widely vary from one patient to another (0.5 to 30 mg/day). Warfarin metabolism CYP2C9*1, CYP2C9*2 and CYP2C9*3

42
Dose of Warfarin *3/*3 *2/*3 *2/*2 *1/*3 *1/*2*1/*1 CYP2C9 Genotype *adapted from Scordo 2002 Correlation between CYP2C9 genotypes and warfarin dose In patients, CYP2C9 genotype explains a limited fraction of intersubject variability in warfarin dose requirements.

43
Mechanism of warfarin action Warfarin exerts its pharmacodynamic effects through inhibition of the vitamin K epoxide reductase (VKOR). VKOR affects the synthesis of various coagulation factors ( Wallin and Hutson, 2004 ).
..")
44
Rieder: VKORC1 Haplotypes SNPs in VKORC1 gene may modulate warfarin action.

45
Comparative studiesStudiesCovariates R 2 % AgeWeight, Height or BSA 2C9VKORRx Sconce et al. (Blood 2005) H367354 Wadelius et al. (Pharmacogenom J 2005) W56 Herman et al. a (Pharmacogenom J 2005) W-37 Herman et al. b (Thromb Heamost 2006) BSA9041,648460 Takahashi et al. (Pharmacogen Genom 2006 W57 Schalekamp et al. (CPT 2006) -648439 Aquilante et al.* (CPT 2006) -367351 No Limited Limited No Limited No Limited Enrolled patients are ambulatory patients with no or limited drug regimens
 H Wadelius et al. (Pharmacogenom J 2005) W56 Herman et al. a (Pharmacogenom J 2005) W-37 Herman et al. b (Thromb Heamost 2006) BSA9041, Takahashi et al. (Pharmacogen Genom 2006 W57 Schalekamp et al. (CPT 2006) - Aquilante et al.* (CPT 2006) - No Limited Limited No Limited No Limited Enrolled patients are ambulatory patients with no or limited drug regimens.")
46
Pharmacogenetic trial with warfarin Clinical Pharmacology & Therapeutics 2008; 83:740-748.

47
Hypothesis & Objectives Objectives To determine the relative contribution of CYP2C9 and VKORC1 polymorphisms in a hospitalized, heavily medicated population of patients requiring initiation of warfarin treatment. To test an innovative approach by combining genotype (CYP2C9 and VKORC1) and phenotype assessments. Hypothesis CYP2C9 phenotype would be a major predictor of warfarin doses in addition to CYP2C9 and VKORC1 genotypes in a doses in addition to CYP2C9 and VKORC1 genotypes in a polymedicated population. polymedicated population. IntroductionHypothesisMethodsResultsDiscussionConclusions
 and phenotype assessments. Hypothesis CYP2C9 phenotype would be a major predictor of warfarin doses in addition to CYP2C9 and VKORC1 genotypes in a doses in addition to CYP2C9 and VKORC1 genotypes in a polymedicated population. polymedicated population. IntroductionHypothesisMethodsResultsDiscussionConclusions.")
48
Study protocol Patients beginning a warfarin treatment were recruited at the Montreal Heart Institute, Quebec Heart Institute, Maisonneuve-Rosemont Hospital and Haut-Richelieu Hospital. INR at day 1, day 4 and day 14 were recorded. Mean warfarin dose corresponding to INR at day 14 was estimated by calculating the average of doses at day 12, 11 and 10. Analyses of concomitant drug administration, diet, alcohol consumption were performed at day 1 and 14. IntroductionHypothesisMethodsResultsDiscussionConclusions

49
Patients characteristics IntroductionHypothesisMethodsResultsDiscussionConclusions 11.1 ±4.2* Concomitant drugs per day 674436436 Indication for warfarin therapy Atrial fibrillation Mechanical heart valve Deep venous thrombosis Stroke/ Transient ischemic attack Heart failure/Cardiomyopathy Pulmonary embolism Other 131:0:1 Ethnicity (Caucasian:Black:Other) 1.66 ±0.09* Height (m) 78.2 ±20.1* Weight (kg) 61.8 ±13.0* Age (years) 75:57 Gender (male:female) Cohort n=132Demographic data
 1.66 ±0.09* Height (m) 78.2 ±20.1* Weight (kg) 61.8 ±13.0* Age (years) 75:57 Gender (male:female) Cohort n=132Demographic data")
50
Association between genetic polymorphisms of VKORC1 and warfarin doses IntroductionHypothesisMethodsResultsDiscussionConclusions 4.7 ±1.8 mg * 3.9 ±0.9 mg3.4 ±1.8 mg * 9041 (G>A) 5.8 mg3.8 ±2.0 mg8773 (C>T) 2.3 ±1.1 mg3.7 ±1.1 mg*4.5 ±2.2 mg † 7566 (C>T) 2.3 ±1.1 mg3.8 ±1.1 mg *4.4 ±2.3 mg † 6853(C>G) 2.3 ±1.0 mg3.7 ±1.1 mg*4.5 ±2.3 mg † 6484 (C>T) 3.3 ±1.4 mg4.3 ±1.2 mg3.6 ±1.7 mg6009 (C>T) 2.0 ±0.9 mg3.9 ±1.0 mg *4.0 ±2.2 mg*5808 (T>G) 2.3 ±1.1 mg3.7 ±1.0 mg *4.5 ±2.3 mg † 3673 (G>A) 3.8 ±2.4 mg4.1 ±1.6 mg3.6 ±1.9 mg861 (C>A) 2 variant alleles 1 variant allele 2 wild-type alleles VKORC1 SNPs
 5.8 mg3.8 ±2.0 mg8773 (C>T) 2.3 ±1.1 mg3.7 ±1.1 mg*4.5 ±2.2 mg † 7566 (C>T) 2.3 ±1.1 mg3.8 ±1.1 mg *4.4 ±2.3 mg † 6853(C>G) 2.3 ±1.0 mg3.7 ±1.1 mg*4.5 ±2.3 mg † 6484 (C>T) 3.3 ±1.4 mg4.3 ±1.2 mg3.6 ±1.7 mg6009 (C>T) 2.0 ±0.9 mg3.9 ±1.0 mg *4.0 ±2.2 mg*5808 (T>G) 2.3 ±1.1 mg3.7 ±1.0 mg *4.5 ±2.3 mg † 3673 (G>A) 3.8 ±2.4 mg4.1 ±1.6 mg3.6 ±1.9 mg861 (C>A) 2 variant alleles 1 variant allele 2 wild-type alleles VKORC1 SNPs")
51
Linear regression model Name of variables Estimates RSQInterceptAgeBSACYP2C9*1*MCYP2C9*M*M VKORC1 9041 (GA) VKORC1 9041 (AA) VKORC1 3673 (G) S:R-warfarin (14h) INR 51%3.394-0.0462.473-0.256-1.5750.5231.889-0.237-3.1740.196 * * * * * p 0.05 IntroductionHypothesisMethodsResultsDiscussionConclusions
 VKORC (AA) VKORC (G) S:R-warfarin (14h) INR 51% * * * * * p 0.05 IntroductionHypothesisMethodsResultsDiscussionConclusions")
52
Correlation between predicted & observed dose S:R warfarin ratio as a phenotypic measure r 2 =0.51 Hospitalized patients with multiple drug regimens (on average 11±4 drugs)
")
53
Linear regression model Name of variables Estimates RSQInterceptAgeBSACYP2C9*1*MCYP2C9*M*M VKORC1 9041 (GA) VKORC1 9041 (AA) VKORC1 3673 (G) INR DAY4/Dose INR 52%4.438-0.0461.4-0.599-1.4430.2821.284-0.107-3.2230.279 * * * * * p 0.05 IntroductionHypothesisMethodsResultsDiscussionConclusions
 VKORC (AA) VKORC (G) INR DAY4/Dose INR 52% * * * * * p 0.05 IntroductionHypothesisMethodsResultsDiscussionConclusions")
54
Correlation between predicted & observed dose INR DAY4 as a phenotypic measure Hospitalized patients with multiple drug regimens (on average 11±4 drugs)
")
55
Our herein described models explain more than 51% of variability in warfarin dose in hospitalized patients with multiple drug regimens. According to our models, it is suggested that VKORC1, age, BSA, S:R-warfarin ratio or INR at DAY4 are major factors of the variance in warfarin dose. IntroductionHypothesisMethodsResultsDiscussionConclusions

56
Hypothesis & Objectives Objectives To determine the relative contribution of phenotyping and genotyping measures in ambulatory care patients at initiation and at steady-state of warfarin therapy over a 8-week period. To test an innovative approach by combining genotype (CYP2C9 and VKORC1) and phenotype assessments. Hypothesis Phenotyping measures will be better predictors of warfarin dose requirements. IntroductionHypothesisMethodsResultsDiscussionConclusions
 and phenotype assessments. Hypothesis Phenotyping measures will be better predictors of warfarin dose requirements. IntroductionHypothesisMethodsResultsDiscussionConclusions.")
57
Study protocol Patients (n=75) beginning a warfarin treatment at the anticoagulation clinic of City de la santé, Laval, Quebec, Canada were recruited. Warfarin doses were adjusted by pharmacists according to standard of care. Covariables recorded over 8 weeks (weeks 1-2, 3-4, 5-6, and 7-8) and included: - Warfarin dose, INR, plasma levels for R and S warfarin, intake of drugs (amiodarone, acetaminophen, CYP2C9 substrates, CYP3A substrates, antibiotics, etc…), green vegetables, smoking,age, gender. IntroductionHypothesisMethodsResultsDiscussionConclusions
 and included: - Warfarin dose, INR, plasma levels for R and S warfarin, intake of drugs (amiodarone, acetaminophen, CYP2C9 substrates, CYP3A substrates, antibiotics, etc…), green vegetables, smoking,age, gender. IntroductionHypothesisMethodsResultsDiscussionConclusions.")
58
Michaud et al., in preparation

59
Pharmacologie Clinique PharmacocinétiquePharmacodynamique DoseConcentrationPlasmatiqueEffet Effet ConcentrationIntracellulaire CYP450

60
Expression relative d’ARNm de CYP450 mesurée dans 79 coeurs humains provenant d’échantillon de ventricule gauche. Les niveaux d’expression ont été déterminés en utilisant la méthode 2 -∆CT.

61
Les niveaux d’expression ont été déterminés en utilisant la méthode 2 -∆∆CT avec un calibrateur.

62
Vérapamil Métabolites

63
Vérapamil: Ventricule gauche vs droit

64
Dompéridone: Ventricule gauche

65
Pharmacologie Clinique PharmacocinétiquePharmacodynamique DoseConcentrationPlasmatiqueEffet Effet ConcentrationIntracellulaire LiaisonintracellulaireIKr

66
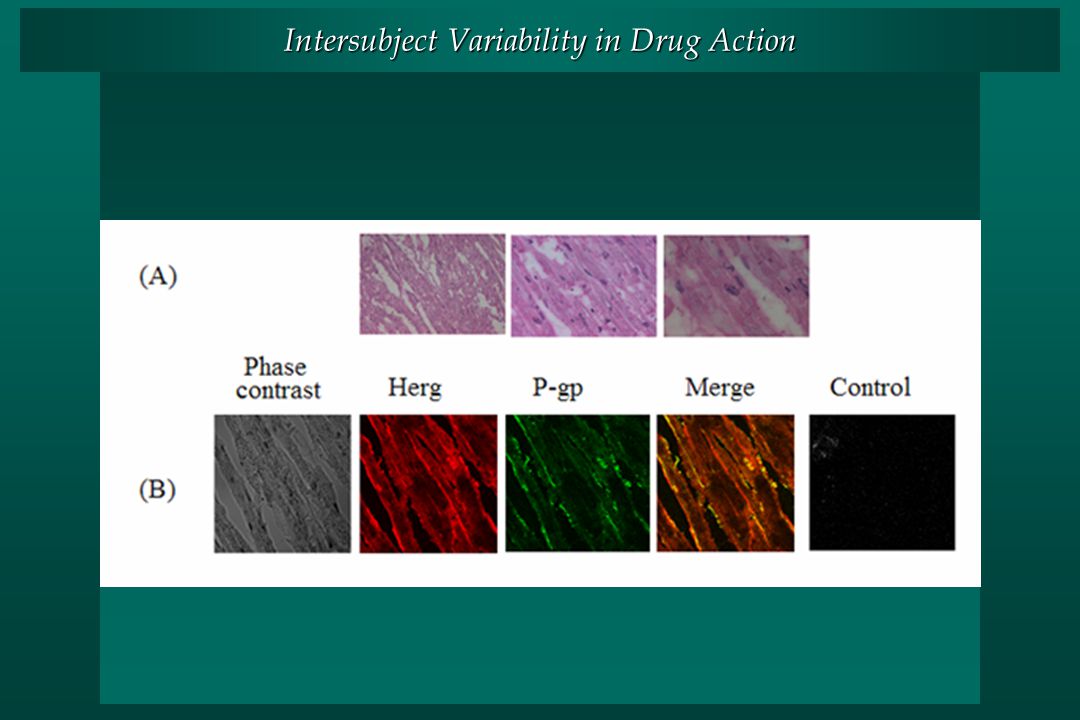
Les transporteurs membranaires. P-glycoproteine (mdr1) Les transporteurs membranaires travaillent en synergie avec les CYP450s pour protéger l’organisme.
 Les transporteurs membranaires travaillent en synergie avec les CYP450s pour protéger l’organisme..")
67
Intersubject Variability in Drug Action Autoradioluminograms of distribution of 3H-domperidone- related radioactivity in myocardium of male wild-type (A) and mdr1a/1b (-/-) (B) mice following an intravenous administration of 3H-domperidone..
 and mdr1a/1b (-/-) (B) mice following an intravenous administration of 3H-domperidone..")
68
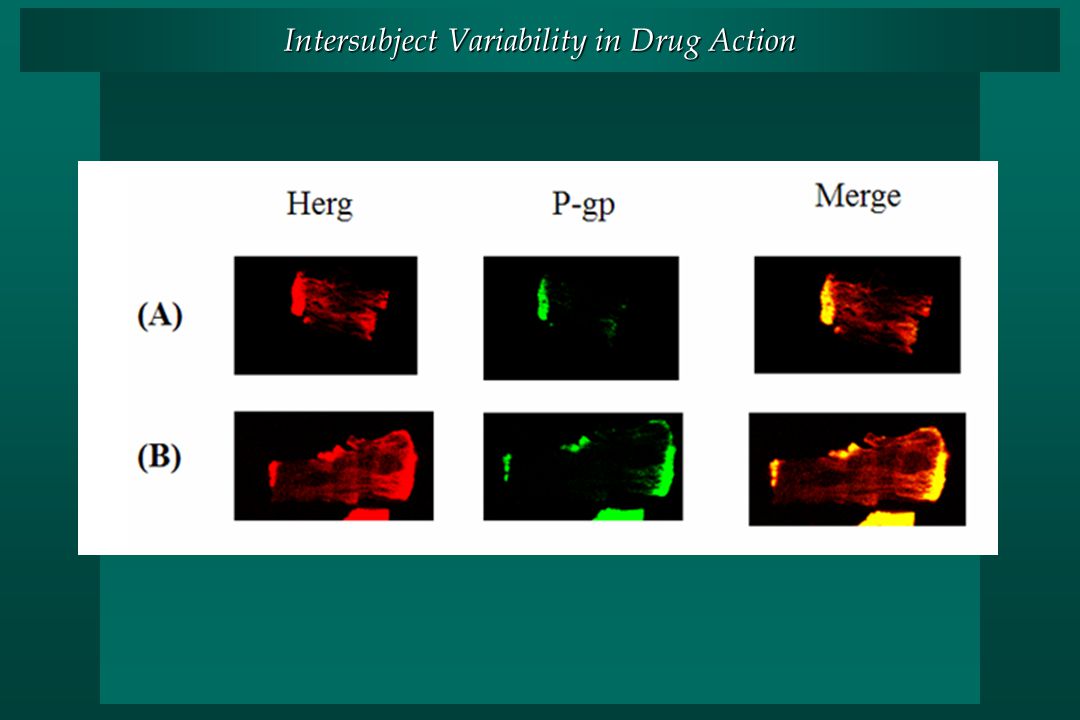
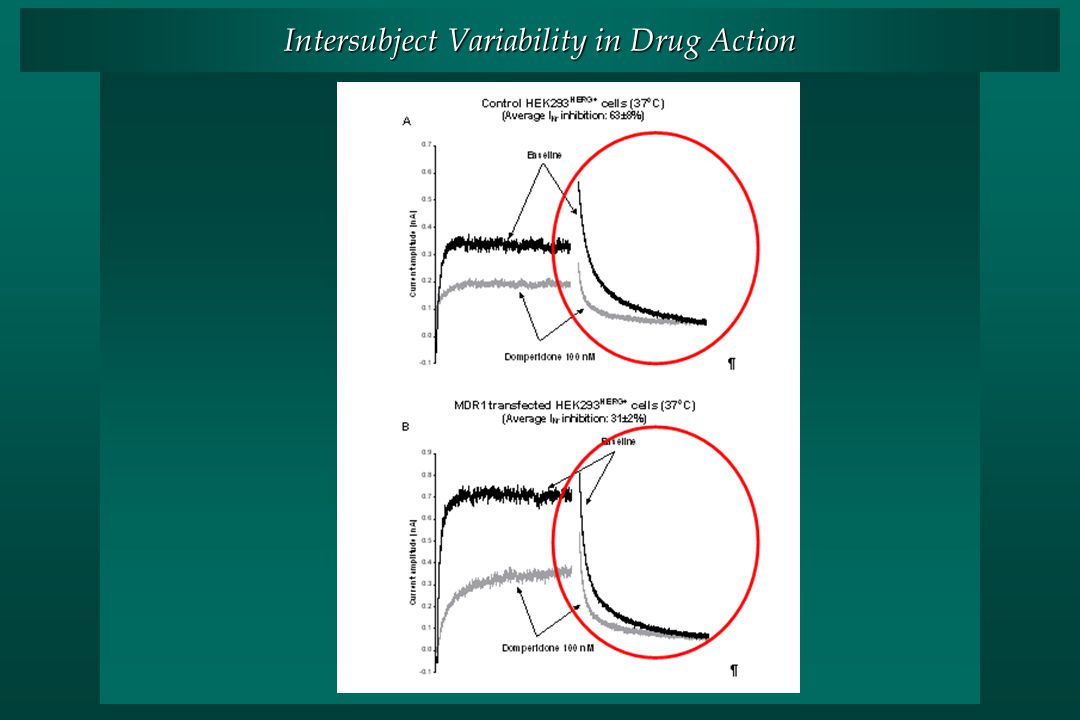
Intersubject Variability in Drug Action

72
Role of CYP3A and P-gp in renal toxicity of tacrolimus.

73
Background Post-transplant renal dysfunction is associated with increased morbidity and mortality in heart-transplant patients. The calcineurin inhibitors, cyclosporin and tacrolimus, have a narrow therapeutic index. Calcineurin inhibitors are substrates of CYP3As and the P-glycoprotein (ABCB1). Genetic polymorphisms in both CYP3A5 and ABCB1 could influence the pharmacokinetics of cyclosporin and tacrolimus. 160 heart transplant patients with a mean follow- up of 4.2 years.
. Genetic polymorphisms in both CYP3A5 and ABCB1 could influence the pharmacokinetics of cyclosporin and tacrolimus. 160 heart transplant patients with a mean follow- up of 4.2 years..")
74
Methods Retrospective cohort study of heart transplant recipients (160) who were discharged alive after transplant and who received calcineurin inhibitors during follow-up. The primary endpoint of the study was to evaluate the impact of common variants of CYP3A5*3 and ABCB1 G2677A and C3435T on changes in estimated glomerular filtration rate (eGFR). Data on renal function were collected at hospital discharge following cardiac transplantation and subsequently at 3, 6, 12, 18, 24 months and every year for up to 9 years. 160 heart transplant patients with a mean follow- up of 4.2 years.
. Data on renal function were collected at hospital discharge following cardiac transplantation and subsequently at 3, 6, 12, 18, 24 months and every year for up to 9 years. 160 heart transplant patients with a mean follow- up of 4.2 years..")
75
Role of CYP3A and P-gp in renal toxicity of tacrolimus.

76
Concentration/dose/kg Mois Role of CYP3A and P-gp in renal toxicity of tacrolimus. 160 heart transplant patients with a mean follow- up of 4.2 years.

77
Role of CYP3A and P-gp in renal toxicity of tacrolimus. 160 heart transplant patients with a mean follow- up of 4.2 years.

78
Concentration/dose/kg Mois Role of CYP3A and P-gp in renal toxicity of tacrolimus. 160 heart transplant patients with a mean follow- up of 4.2 years.

79
Remerciements au laboratoire François Bélanger Sylvie Larabie-Poirier Isabelle Plante, Ph.D. Pierre Morissette, Ph.D. Lucie Couture, Ph.D. Raymond Hreiche, Ph.D. Jean Lefebvre, Ph.D. Véronique Michaud, Ph.D. Yahi Hakima, Ph.D. Heidi Ligeret, Ph.D. Marcin Zakrzewski Simon DeDenus Tatiana Stepanova Julie Grenier Philippe Colucci Marie Lordkipanidzé Frédérique Fenneteau Andréa Sirhan-Daneau Jade Huguet Hubert Zakrzweski, Jean-Philippe Dion, Marie-Christine Dumas, Benoît Pronovost, Louis-Philippe David, Martin Frappier, Joëlle Desjardins, Sophie Zezmi, Maude St-Onges

80
Acknowledgements Canadian Institutes of Health Research Fondation des maladies du coeur du Québec Fonds de la recherche en santé du Québec Génome Canada / Génome Québec

Présentations similaires










cinétique/pharmaco (toxico)dynamie>")



 Nombres (1-100).>")




