Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Les défis de la prise en charge intra-hospitalière
Pr. Gilles Capellier Pôle Urgences-SAMU- Réanimation Médicale CHRU Besançon,EA 3920 Université de Franche-Comté

3
Réanimation Néonatale Chirurgie pédiatrique Arrêt Cardiaque ?
Traumatismes graves Brûlés Syndrome coronarien AVC Maternités Réanimation Néonatale Chirurgie pédiatrique Arrêt Cardiaque ? For starters, an immediately available specialized critical care team including a physician team leader, akin to the lead trauma surgeon, should be immediately summoned to the emergency department to begin to care for the patient upon his or her arrival in the emergency department. Decisions must be made regarding immediate cooling, immediate cardiac catheterization, immediate thrombolytic therapy, and the like. Use of the optimal pressor agents, antiarrhythmic agents, respiratory care management, nutrition, and ways to stabilize a metabolically unstable medical condition need to be made rapidly in order to optimize the patient’s chance for survival. The optimal balance between diagnostic studies and timing of intervention is critical in these patients, much like with the hemorrhagic shock patient.

4
Langhelle et al. Resuscitation 2005
In conclusion, I hope that I reached my goal that was to convince you that the last part of the chain of survival should not be neglected. We can speculate that additional effort should be performed in order to provide the best quality of care to these patients. Thank you very much for your attention. Langhelle et al. Resuscitation 2005

6
Enjeux du traitement de l’arrêt cardiaque: Coordination des moyens
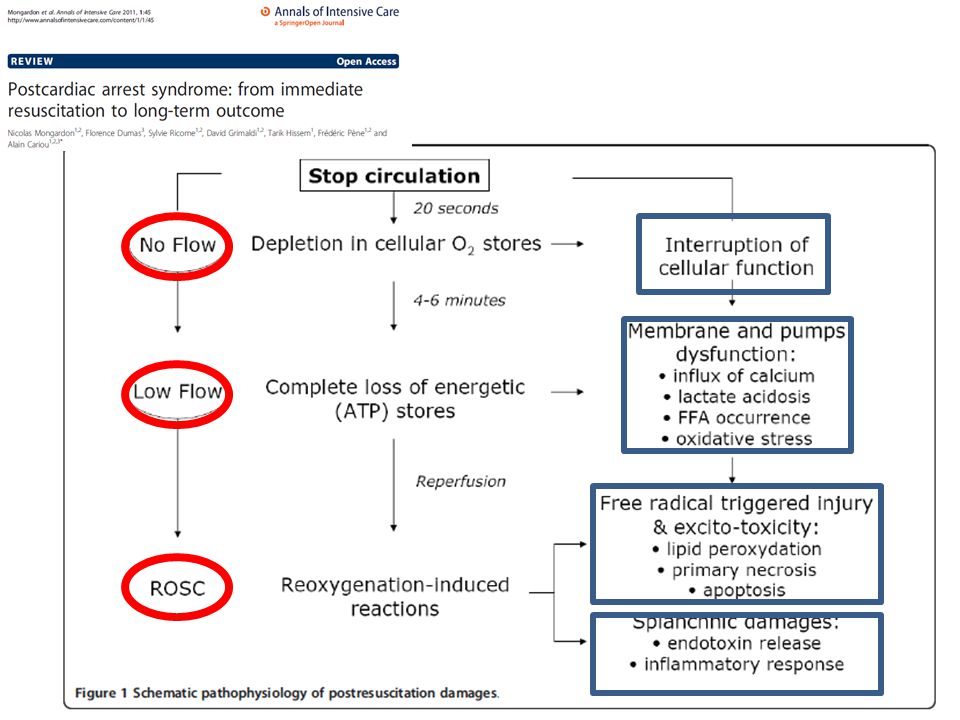
Hémodynamique Neuroprotection Prevention de l’infection Pronostic Décision de LATA - PMO Séquelles et devenir

7
Prehospital hypothermia
ECPR ECPR In conclusion, I hope that I reached my goal that was to convince you that the last part of the chain of survival should not be neglected. We can speculate that additional effort should be performed in order to provide the best quality of care to these patients. Thank you very much for your attention. Prehospital hypothermia Langhelle et al. Resuscitation 2005

8
Enjeux du traitement de l’arrêt cardiaque: Coordination des moyens
Hémodynamique: Arrêt cardiaque réfractaire Etat de choc: drogues Coronarographie Assistance circulatoire Attention: Pneumothorax, hémorragie, atélectasies, désordres métaboliques Neuroprotection Prevention de l’infection Pronostic Décision de LATA Séquelles et devenir

9
Une discussion transdisciplinaire
Médecin régulateur Chirurgiens Thoraciques Cardiologues 15 Réanimateurs Anesthésistes ACR Médecins Urgentistes SMUR Pompiers Réfractaire

10
Incertitude AC réfractaire
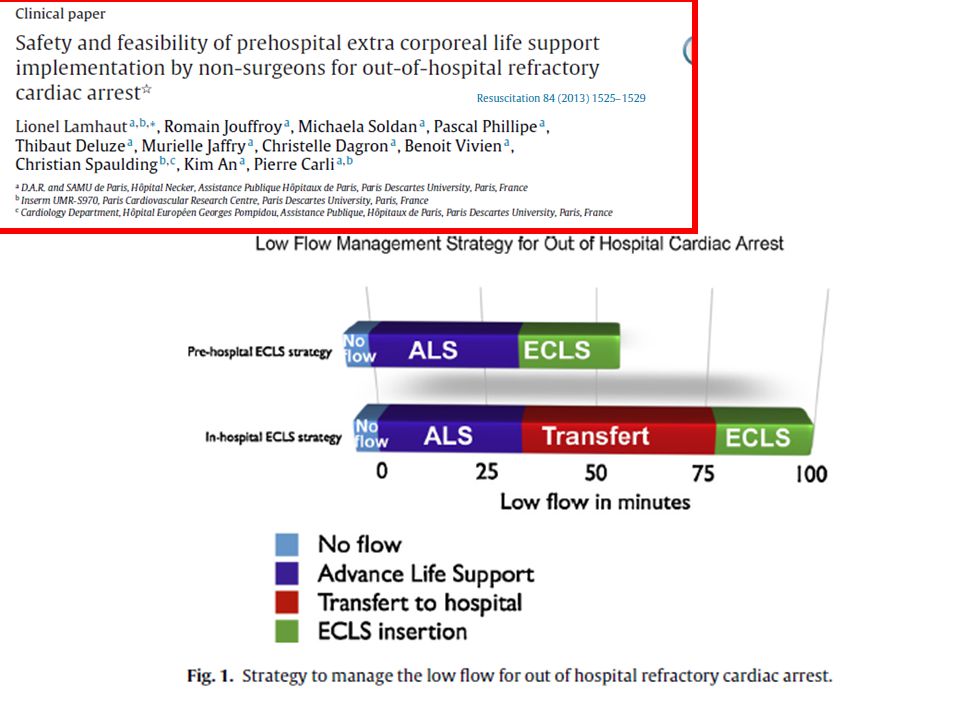
Algorithme décisionnel: Assistance circulatoire devant un AC réfractaire Indication possible Incertitude AC réfractaire Pas d’indication Intoxication Hypothermie Comorbidités Signes de vie Durée de No-Flow? >5 min 0-5 min Rythme cardiaque? TV, TP, FV Asystolie ETCO2>10mmHg Low-Flow<100min Durée de Low-Flow? ETCO2<10mmHg Low-Flow>100min

13
IHCA OHCA Initial rhythm: PEA VF or asystole CPR duration: pH: 7, ,85 Lactate: mg/dl Survival rate %:

14
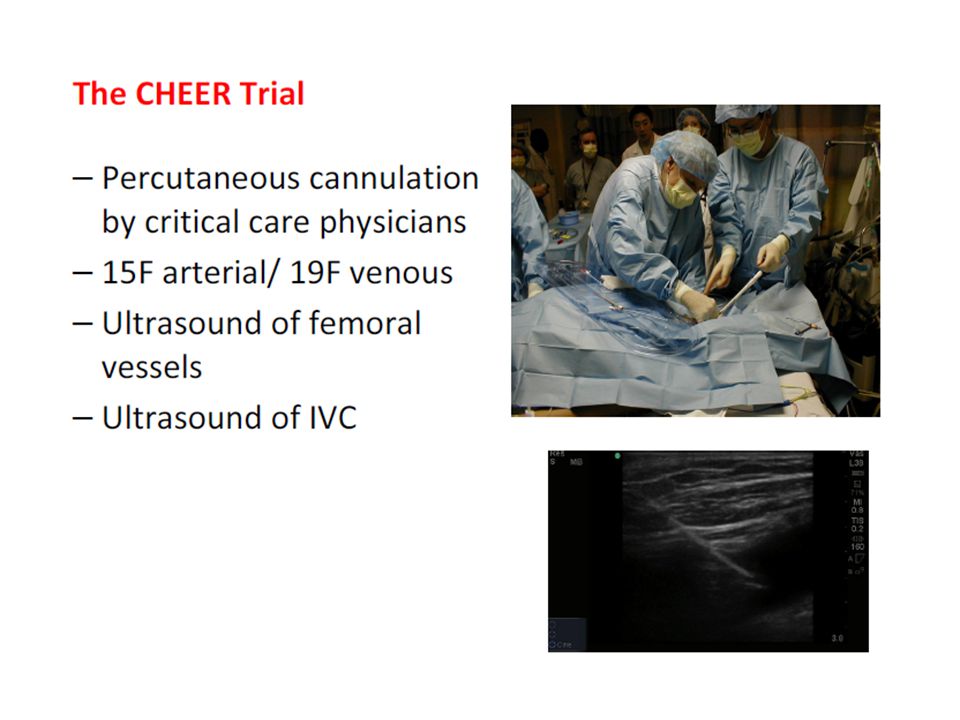
ECMO implantation during CPR was associated with a marked increase in the risk of death [OR (1.09– 392.03)] in the trial by Cheng et al. [12] and 4.12 (2.17–7.83) in the trial by Beurtheret et al. [11&]. ECMO implantations shortly after CPR and during CPR carry different risk of death and should thus be considered separately. ECMO implantation shortly after CPR sounds reasonable, with reported survival rates between 22% [11&] and 50% [9&& Chen et al. [21] reported a cumulative 30-day survival rate of 34%. They also demonstrated that compared to conventional CPR, ECPR increased the rate of successful defibrillation and extended the duration of resuscitation associated with good neurological outcome. The probability to survive to discharge was 50% when ECMO flow was initiated within 30 min of IHCA, 30% between 30 and 60 min, and 18% after 60 min. Of note in the conventional group, these percentages were 20, 9, and 0%, respectively [21] When can cardiac arrest be considered as refractory to standard CPR? In a large database of patients with IHCA, half of the patients achieving ROSC did it within 10 min of the onset of cardiac arrest, one-fourth during the subsequent 10 min, and very few patients experienced ROSC after more than 30min of CPR [2&&]. In OHCA, ROSC occurred within 16.1 min of CPR in 89.7% of the patients with good functional outcome [3&&]. After 15 min, the probability of good functional recovery among all attempted CPR fell to less than 2%. Hence, cardiac arrest can be considered refractory to standard CPR after 15 min. At Erasme University Hospital, we evaluate the patient with cardiac arrest as a potential candidate for ECPR at 10min of CPR, which results in initiation of ECMO within 30 and 60 min, depending on the location of cardiac arrest When deciding the time of death after cardiac death under ECMO: non beating organ donation :Up to one-third of nonsurvivors after ECPR die from postanoxic brain damage, but only a minority will present brain death. In centers with a program of nonheart beating organ donation, these patients may be selected for organ donation [35&]. Regarding this, a major ethical concern of this strategy was the determination of death after cardiac death. In many patients, absence of recovery of cardiac activity and poor neurologic state were used to define death after cardiac death and suitability for organ donation OHCA: witnessed cardiac arrest, with a no-flow period less than 5 min, whenever possible bystander CPR or a very rapid response team, a prehospital care policy prompt to alert a specialized hospital with an ECMO team, and rapid transport after initiation of CPR (scoop and run strategy). “At Erasme University Hospital, we evaluate the patient with cardiac arrest as a potential candidate for ECPR at 10min of CPR, which results in initiation of ECMO within 30 and 60 min, depending on the location of cardiac arrest”
] in the trial by Cheng et al. [12] and (2.17–7.83) in the trial by Beurtheret et al. [11&]. ECMO implantations shortly after CPR and during. CPR carry different risk of death and should thus be. considered separately. ECMO implantation shortly. after CPR sounds reasonable, with reported survival. rates between 22% [11&] and 50% [9&& Chen. et al. [21] reported a cumulative 30-day survival. rate of 34%. They also demonstrated that compared. to conventional CPR, ECPR increased the rate of. successful defibrillation and extended the duration. of resuscitation associated with good neurological. outcome. The probability to survive to discharge. was 50% when ECMO flow was initiated within. 30 min of IHCA, 30% between 30 and 60 min, and. 18% after 60 min. Of note in the conventional. group, these percentages were 20, 9, and 0%, respectively [21] When can cardiac arrest be considered as refractory. to standard CPR In a large database of patients with IHCA, half of the patients achieving. ROSC did it within 10 min of the onset of cardiac. arrest, one-fourth during the subsequent 10 min, and very few patients experienced ROSC after more. than 30min of CPR [2&&]. In OHCA, ROSC occurred. within 16.1 min of CPR in 89.7% of the patients. with good functional outcome [3&&]. After 15 min, the probability of good functional recovery among. all attempted CPR fell to less than 2%. Hence, cardiac. arrest can be considered refractory to standard. CPR after 15 min. At Erasme University Hospital, we. evaluate the patient with cardiac arrest as a potential. candidate for ECPR at 10min of CPR, which results. in initiation of ECMO within 30 and 60 min, depending on the location of cardiac arrest. When deciding the time of death after cardiac death under ECMO: non beating organ donation :Up to one-third of nonsurvivors after ECPR die from. postanoxic brain damage, but only a minority will. present brain death. In centers with a program of. nonheart beating organ donation, these patients. may be selected for organ donation [35&]. Regarding. this, a major ethical concern of this strategy was the. determination of death after cardiac death. In many. patients, absence of recovery of cardiac activity and. poor neurologic state were used to define death after. cardiac death and suitability for organ donation. OHCA: witnessed cardiac arrest, with a no-flow. period less than 5 min, whenever possible bystander. CPR or a very rapid response team, a prehospital care. policy prompt to alert a specialized hospital with. an ECMO team, and rapid transport after initiation. of CPR (scoop and run strategy). At Erasme University Hospital, we evaluate the patient with cardiac arrest as a potential candidate for ECPR at 10min of CPR, which results in initiation of ECMO within 30 and 60 min, depending on the location of cardiac arrest")
15
Outcome of ECLS according to CPR duration
Discharge

17
17

18
Extracorporeal CPR CIRCONSTANCES DE L'ACR 2010 (n=10) 2011 (n=14)
2010 (n=10) 2011 (n=14) 2012 (n=15) Site extra-hospitalier 6 (60%) 6 (42,8%) 7 (46,7%) Site intra-hospitalier 4 (40%) 8 (57,2%) 8 (53,3%) Durée de No Flow 1'20''+/-3'20'' 1'27''+/-2'55'' 1'31''+/-2'58'' Durée de Low Flow 61'45''+/-34'04 58'01''+/-34'58'' 64'5''+/-38'11'' Nombre de bolus d'adrénaline de 1mg 16+/-11,8 11,8+/-8,2 6,7+/-3,5 Nombre de chocs délivrés 3,9+/-5,9 4,5+/-3,1 3,6+/-2,4 EtCO2 à l'arrivée aux urgences 15+/-7,1 N 21,2+/-14,3
 2011 (n=14) 2012 (n=15) Site extra-hospitalier. 6 (60%) 6 (42,8%) 7 (46,7%) Site intra-hospitalier. 4 (40%) 8 (57,2%) 8 (53,3%) Durée de No Flow / / /-2 58 Durée de Low Flow / / / Nombre de bolus d adrénaline de 1mg. 16+/-11,8. 11,8+/-8,2. 6,7+/-3,5. Nombre de chocs délivrés. 3,9+/-5,9. 4,5+/-3,1. 3,6+/-2,4. EtCO2 à l arrivée aux urgences. 15+/-7,1. N. 21,2+/-14,3.")
19
Current Opinion in Critical Care June, 2014
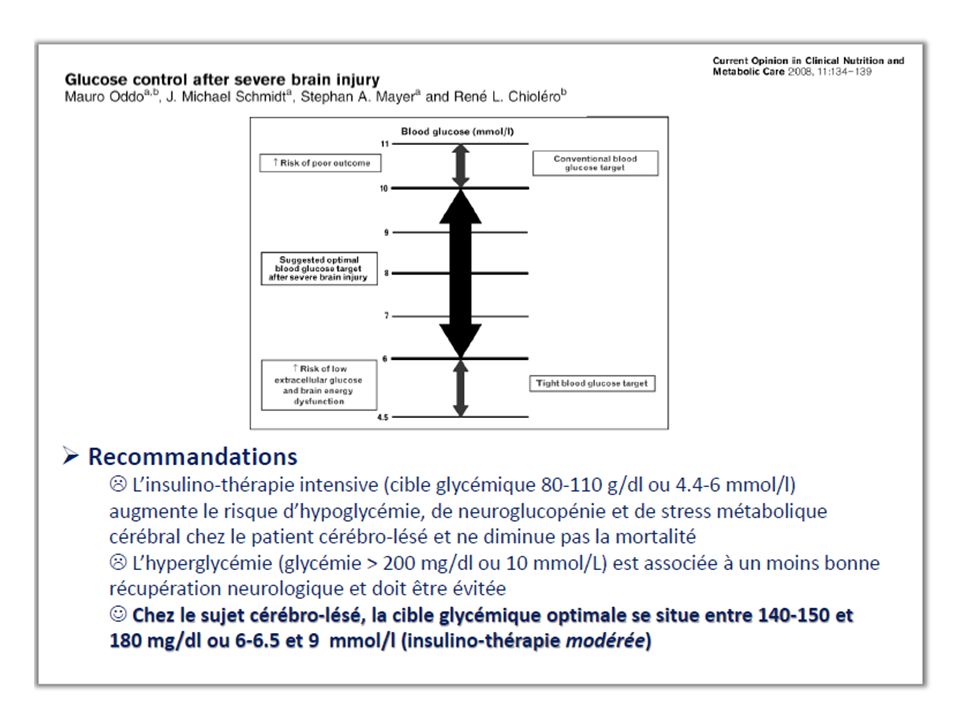
ST+ et Enzymes ont des sensibilités insuffisantes pour décider de la réalisation d’une coronarographie Initial rhythm analysis may be informative in this condition. Indeed, a recent coronary occlusion is more frequently observed in patients with ventricular fibrillation compared with those with unshockable rhythm [Recently, the additional value of high sensitivity troponin has been evaluated in OHCA patients but was disappointing for diagnosing ACS [20] (Table 1). To investigate the best time frame, Strote et al. [26] compared in a retrospective study the ICU survival of OHCA patients according to the delay of coronary angiography realization. Adjusting for cofounders with a propensity score, they found that immediate (defined in the study as less than 6 hours) coronary angiography was associated with a better survival, regardless of the ST-segment finding [26]. When doing a coronaro angio is the best time in OHCA without ST+. Debatable question In light of these results, it seems realistic to perform coronary angiography as soon as possible afterOHCA, even in patientswithout STEMI. In our own institution, all patients are directly admitted to the cardiac catheterization laboratory, regardless of clinical and ECG findings, providing that there is no evidence for a noncardiac cause (sepsis, trauma, metabolic disorder, hemorrhage, or any other obvious noncardiac cause). An immediate coronary angiogram is then performed using standard techniques, and a PCI is attempted if there is an acute coronary artery occlusion or an unstable lesion considered responsible for OHCA. the safety of the early invasive strategy needs to be further confirmed. As an example, the risk of acute kidney injury (AKI) might be argued to avoid performing coronary angiography in OHCA patients, as these patients are highly exposed to renal failure. Indeed, AKI, which occurs in nearly 20% of patients regardless of an eventual underlying chronic kidney disease, might be worsened by contrast iodine injection used during coronary angiography. Mainly due to ischemia-reperfusion phenomenon, AKI is more frequently observed in patients requiring mechanical ventilation or inotropes [28]. According to this hypothesis, a multiple PCI of all significant lesions could be associated with an improvement in outcome. In the same manner, Mylotte et al. [31] reported the superiority of a multiple vessel PCI in patients with cardiogenic shock or after cardiac arrest in an observational prospective study of 266 patients. Further clinical evaluation should also be performed for antiplatelet treatment since the rate of acute stent thrombosis appears to be high in this situation [33].
. To investigate the best time. frame, Strote et al. [26] compared in a retrospective. study the ICU survival of OHCA patients according. to the delay of coronary angiography realization. Adjusting for cofounders with a propensity score, they found that immediate (defined in the study. as less than 6 hours) coronary angiography was. associated with a better survival, regardless of the. ST-segment finding [26]. When doing a coronaro angio is the best time in OHCA without ST+. Debatable question In light of these results, it. seems realistic to perform coronary angiography as. soon as possible afterOHCA, even in patientswithout. STEMI. In our own institution, all patients are directly. admitted to the cardiac catheterization laboratory, regardless of clinical and ECG findings, providing. that there is no evidence for a noncardiac cause. (sepsis, trauma, metabolic disorder, hemorrhage, or any other obvious noncardiac cause). An immediate. coronary angiogram is then performed using. standard techniques, and a PCI is attempted if. there is an acute coronary artery occlusion or an. unstable lesion considered responsible for OHCA. the safety of the early invasive. strategy needs to be further confirmed. As an. example, the risk of acute kidney injury (AKI) might. be argued to avoid performing coronary angiography. in OHCA patients, as these patients are. highly exposed to renal failure. Indeed, AKI, which. occurs in nearly 20% of patients regardless of. an eventual underlying chronic kidney disease, might be worsened by contrast iodine injection. used during coronary angiography. Mainly due to. ischemia-reperfusion phenomenon, AKI is more. frequently observed in patients requiring mechanical. ventilation or inotropes [28]. According to this. hypothesis, a multiple PCI of all significant lesions. could be associated with an improvement in. outcome. In the same manner, Mylotte et al. [31] reported the superiority of a multiple vessel PCI in. patients with cardiogenic shock or after cardiac. arrest in an observational prospective study of 266. patients. Further clinical evaluation should. also be performed for antiplatelet treatment since. the rate of acute stent thrombosis appears to be high. in this situation [33].")
21
Possibilité de réaliser une angiographie / PCI sous assistance ?
Arrêt cardiaque réanimé, sans reprise d’activité cardiaque spontanée, ni reprise de conscience Possibilité de réaliser une angiographie / PCI sous assistance ? Utilisation d’un système de massage cardiaque externe (LUCAS). 13 cas d’angiographie , bonne visualisation des coronaires. Larsen Resuscitation 2007;75:454
. 13 cas d’angiographie , bonne visualisation des coronaires. Larsen Resuscitation 2007;75:454.")
22
Dysfunction Myocardique ou “Stunned myocardium”
Relation avec la durée de la réanimation et le retour à rythme propre Evaluation: Echographie cardiaque Méthodes invasives Sidération myocardique ou “Stone Heart”: Ischémie globale du VG Epaississement de la paroi ventriculaire Rigidité de la paroi VG (diminution de la compliance) Diminution du volume VG Situation de “Myocardial rigor mortis”
 Diminution du volume VG. Situation de Myocardial rigor mortis")
23
De nombreuses inconnues et peu de données dans la littérature
Optimisation de l’hémodynamique aprés AC Mecanism in the post anoxic brain injury BBB brain blood barrier, ROS: reactive oxygen species De nombreuses inconnues et peu de données dans la littérature

25
Enjeux du traitement de l’arrêt cardiaque
Etat de choc: Dépression CV: DBX, Adrénaline, NA + DBX, autres Vasoplégie: Hémofiltration à haut débit Objectif TA : PAS>120 mmHg ?! Exploration: échographie, autres? Revascularisation coronaire: Assistance circulatoire

26
Enjeux du traitement de l’arrêt cardiaque: Coordination des moyens
Hémodynamique Neuroprotection Hypothermie Oxygène Gaz carbonique Glycémie Autres traitements: EPO, Cyclosporine Prevention de l’infection Pronostic Décision de LATA Séquelles et devenir

27
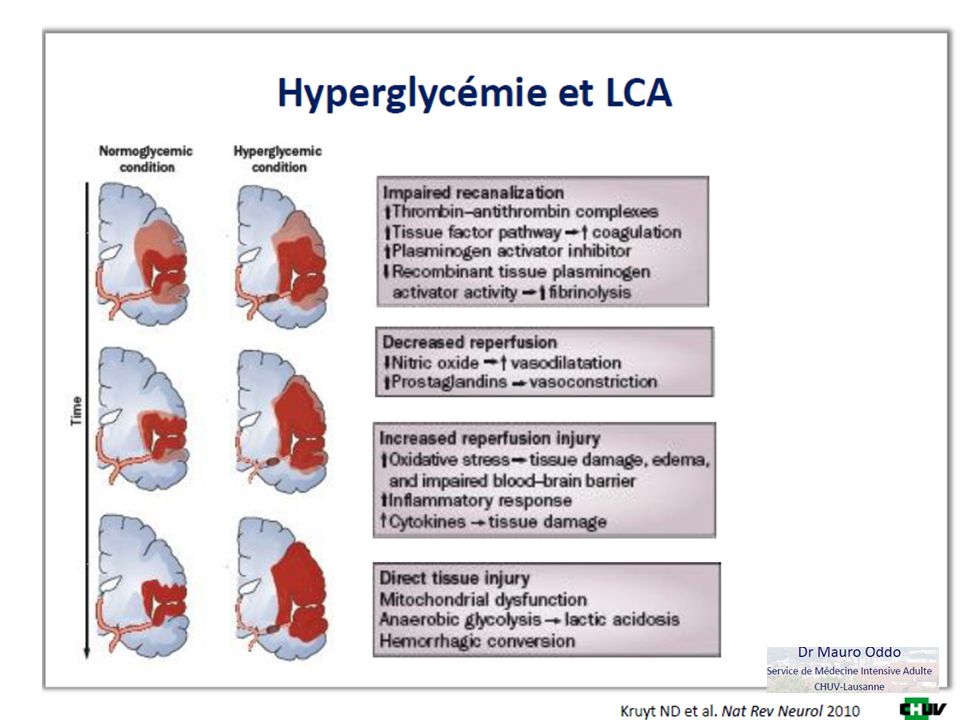
Mecanism in the post anoxic brain injury
BBB brain blood barrier, ROS: reactive oxygen species Therapeutic hypothermia provides effective neuroprotection by increasing tissue tolerance to ischemia, on one hand, and by hampering the development of inflammatory cascade and radical oxygen species (ROS) production after reperfusion, on the other (Fig. 2) [12,13]. Experimental studies yielded that therapeutic hypothermia was even more effective when it was initiated immediately after the ischemic event most of them suggested the administration of 30 ml/kg of crystalloids over 30 min to achieve around 1.58C temperature reduction before hospital admission [18,19,24]. Also, Skulec et al. [25] suggested that a lower liquid amount (15–20 ml/kg) could be effective as well. prehospital cooling was more effective in reducing core temperature [mean overall difference 0.958C (95% CI, confidence interval, 1.15 to 0.75)] than standard hypothermia but showed no significant benefit on survival and good neurological outcome [risk ratio for favorable outcome 1.01 (95% CI 0.82–1.25)]. Even when patients were considered separately according to their initial rhythm, even more controversial after some recent retrospective studies showed that those patients who achieved more rapidly the target temperature after cardiac arrest had no major differences in overall neurological outcome when compared with the others [27] or presented an even higher risk of increased mortality [28,29&]. in contrast with the results published by Wolff et al. [30], who showed that a delay in reaching target temperature was independently associated with a worse outcome [OR (odds ratio) for every hour 0.69 (95% CI 0.51–0.98)] in a prospective cohort of 49 comatose cardiac arrest patients hypothermia induced by a closed loop suystem the effectiveness and usefulness of prehospital therapeutic hypothermia in comatose survivors from cardiac arrest. Over a 5-year period, the authors randomized 1359OHCA (583 with ventricular fibrillation and 776 without ventricular fibrillation) to receive either early post- ROSC cooling with 2 l of intravenous saline or standard treatment. A significant reduction in mean core temperature by 1.208C (95% CI 1.33 to 1.078C) in patients with ventricular fibrillation and by 1.308C (95% CI 1.40 to 1.208C) in patients without ventricular fibrillation was observed. However, survival was similar between the two groups, both for patients with ventricular fibrillation (62.7 versus 64.3%, P¼0.69) and those without ventricular fibrillation (19.2 versus 16.3%, P¼0.30) Kim F, Nichol G, Maynard C, et al. Effect of prehospital induction of mild hypothermia on survival and neurological status among adults with cardiac arrest: a randomized clinical trial. JAMA 2013; 311:45–52. This article showed evidence that prehospital therapeutic hypothermia obtained by cold fluids bolus did not provide any further neuroprotective advantages when compared to standard in-hospital cooling.: questions 1/3 pas hypothermia achieved inhospital, delay 4 to 5 hours to reach hypothermia, fluid (chloride) might have induced acidosis, overload, pulmonary oedema in the pivotal articles that introduced therapeutic hypothermia after cardiac arrest in clinical practice, time to hypothermia has also been quite variable among studies, ranging from 2 [7] to 8h [8]. However, the ‘therapeutic window’ for initiating therapeutic hypothermia (i.e., the time after arrest during which therapeutic hypothermia ismost effective) is narrow,
 production after reperfusion, on the other (Fig. 2) [12,13]. Experimental studies. yielded that therapeutic hypothermia was even. more effective when it was initiated immediately. after the ischemic event most of them suggested the administration. of 30 ml/kg of crystalloids over 30 min to. achieve around 1.58C temperature reduction before. hospital admission [18,19,24]. Also, Skulec et al. [25] suggested that a lower liquid amount (15–20 ml/kg) could be effective as well. prehospital cooling was more. effective in reducing core temperature [mean overall. difference 0.958C (95% CI, confidence interval, 1.15 to 0.75)] than standard hypothermia but. showed no significant benefit on survival and good. neurological outcome [risk ratio for favorable outcome (95% CI 0.82–1.25)]. Even when patients. were considered separately according to their initial. rhythm, even more controversial after. some recent retrospective studies showed that those. patients who achieved more rapidly the target. temperature after cardiac arrest had no major differences. in overall neurological outcome when compared. with the others [27] or presented an even. higher risk of increased mortality [28,29&]. in contrast with the results published by Wolff. et al. [30], who showed that a delay in reaching target. temperature was independently associated with a. worse outcome [OR (odds ratio) for every hour (95% CI 0.51–0.98)] in a prospective cohort of 49. comatose cardiac arrest patients hypothermia induced by a closed loop suystem the effectiveness. and usefulness of prehospital therapeutic hypothermia. in comatose survivors from cardiac arrest. Over. a 5-year period, the authors randomized 1359OHCA. (583 with ventricular fibrillation and 776 without. ventricular fibrillation) to receive either early post- ROSC cooling with 2 l of intravenous saline or. standard treatment. A significant reduction in mean. core temperature by 1.208C (95% CI 1.33 to C) in patients with ventricular fibrillation. and by 1.308C (95% CI 1.40 to 1.208C) in. patients without ventricular fibrillation was. observed. However, survival was similar between. the two groups, both for patients with ventricular. fibrillation (62.7 versus 64.3%, P¼0.69) and those. without ventricular fibrillation (19.2 versus 16.3%, P¼0.30) Kim F, Nichol G, Maynard C, et al. Effect of prehospital induction of mild. hypothermia on survival and neurological status among adults with cardiac. arrest: a randomized clinical trial. JAMA 2013; 311:45–52. This article showed evidence that prehospital therapeutic hypothermia obtained by. cold fluids bolus did not provide any further neuroprotective advantages when. compared to standard in-hospital cooling.: questions 1/3 pas hypothermia achieved inhospital, delay 4 to 5 hours to reach hypothermia, fluid (chloride) might have induced acidosis, overload, pulmonary oedema. in the pivotal articles that introduced. therapeutic hypothermia after cardiac arrest. in clinical practice, time to hypothermia has also. been quite variable among studies, ranging from 2. [7] to 8h [8]. However, the ‘therapeutic window’ for. initiating therapeutic hypothermia (i.e., the time. after arrest during which therapeutic hypothermia. ismost effective) is narrow,")
28
Quelle méthode de refroidissement?

29
Effets secondaires de l’hypothermie et ACR
Susceptibilité aux infections : pneumopathies d’inhalation, pneumopathies AV Troubles de la coagulation Anomalies métaboliques: kalièmie, Magnésium, phosphore Modification des volumes circulants Récidive de troubles du ryhtme ventriculaire Diminution du métabolisme des médicaments, diminution possible de la tolérance (PRIS), augmentation des effets secondaires
, augmentation des effets secondaires.")
30
December 2013 Over a decade ago, two pivotal trials altered the standard of care for unconscious patients after cardiac arrest. Many of these patients suffer severe neurologic injury and death; researchers sought a treatment that could reduce global brain ischemia and prevent neurologic damage even when initiated after cardiopulmonary resuscitation and the restoration of circulation. The trial results, published in 2002, suggested that induced hypothermia, also known as “targeted temperature management,” could serve as such a treatment. Patients treated with hypothermia (temperatures of 32°C to 34°C) were found to have improved survival and neurological function as compared to patients receiving routine care. Since then, international resuscitation guidelines have incorporated therapeutic hypothermia into their recommendations, and the practice has become widely adopted. More than a decade later, however, criticism of this guideline persists. In the original trials, many patients in the routine treatment arm developed fever, which is known to be associated with poor outcomes. Did the patients in the intervention arm do better because they were treated with hypothermia, or simply because they were kept from developing hyperthermia? In this week’s NEJM, Nielsen et al report findings from a large randomized controlled trial that addresses this question. The trial, conducted in intensive care units across Europe and Australia, randomly assigned 950 unconscious adults who had suffered out-of-hospital cardiac arrest to targeted temperature management at either 33°C (“induced hypothermia”) or 36°C (“near-normal temperature”) for 36 hours. In contrast to the previous studies, which only included patients with ventricular fibrillation, this study enrolled patients with both shockable and nonshockable rhythms. Importantly, fever prevention measures were used to keep all patients below 37.5°C until 72 hours after cardiac arrest. The primary outcome was all-cause mortality, and the main secondary outcome was a composite of neurologic function and death at 180 days. Unlike the previous studies, this trial established a clear protocol for when life-sustaining therapy should be withdrawn. A physician blinded to the intervention assignments performed neurological evaluations 72 hours after the intervention period ended and recommended either continuing or withdrawing life-sustaining therapy, according to pre-specified criteria. During the first seven days, life-sustaining therapy was withdrawn in 132 patients in the 33°C group and 115 in the 36°C group, for reasons including brain death and multi-organ failure. By the end of the trial, overall mortality did not differ significantly between the two study arms: 50% of the patients in the 33°C group had died, as compared to 48% of those in the 36°C group (HR 1.06, p=0.51). There was also no difference between the two groups in neurological function (measured either by the Cerebral Performance Category: HR 1.02, p=0.78; or by the modified Rankin scale: HR 1.01, p=0.87) or death at 180 days (HR 1.01, p=0.92). Is therapeutic hypothermia actually therapeutic, then? In this study, neither benefit nor harm was evident at 33°C as compared to 36°C. Several factors may have contributed to the departure of results from those of older studies. This trial had fewer exclusion criteria, resulting in a broader, more heterogeneous patient population; 20% of participants, for example, had nonshockable rhythms. In addition, improvements in pre-hospital and critical care management over the last decade may have made it harder to isolate the incremental benefits of a single intervention. Finally, as some have argued all along, it is possible that the real value of targeted temperature management lies not in the induction of hypothermia but rather in the prevention of hyperthermia. In an accompanying editorial, Drs. Jon Rittenberger and Clifton Callaway of the University of Pittsburgh write, “The exceptional rates of good outcomes in both the 33°C and 36°C groups in the present trial may reflect the active prevention of hyperthermia. Whatever the mechanisms, it seems clear that we should not regress to a pre-2002 style of care that does not manage temperature at all.” They conclude, “Perhaps the most important message to take from this trial is that modern, aggressive care that includes attention to temperature works, making survival more likely than death when a patient is hospitalized after CPR.” NEJM Deputy Editor Dr. John Jarcho states, “This trial illustrates the importance of carefully testing and evaluating each individual component of patient management in critical care, to be certain that our practice is not only evidence-based, but based on evidence that is derived from adequate testing of appropriate options.” Further investigation is needed to clarify whether, and to what extent, induced hypothermia can be therapeutic. If benefits can be demonstrated in future studies, additional research will also be needed to identify an optimal target temperature. It is encouraging that outcomes for patients who suffer cardiac arrest have improved considerably over the last decade. It is equally encouraging that even widely accepted treatment guidelines can be challenged by new evidence so that outcomes may continue to improve in the decades to come. What is your current approach to temperature management for unconscious patients brought into the hospital after cardiac arrest? Is there a specific temperature you target? How will the findings of this study affect your approach? patients 18 years of age or older who were unconscious (a score of <8 on the Glasgow Coma Scale [on which scores range from 3 to 15, with lower scores indicating reduced levels of consciousness]) on admission to the hospital after out-of-hospital cardiac arrest of presumed cardiac cause, irrespective of the initial rhythm. Eligible patients had more than 20 consecutive minutes of spontaneous circulation after resuscitation.14 The main exclusion criteria were an interval from the return of spontaneous circulation to screening of more than 240 minutes, unwitnessed arrest with asystole as the initial rhythm, suspected or known acute intracranial hemorrhage or stroke, and a body temperature of less than 30°C.
 were found to have improved survival and neurological function as compared to patients receiving routine care. Since then, international resuscitation guidelines have incorporated therapeutic hypothermia into their recommendations, and the practice has become widely adopted. More than a decade later, however, criticism of this guideline persists. In the original trials, many patients in the routine treatment arm developed fever, which is known to be associated with poor outcomes. Did the patients in the intervention arm do better because they were treated with hypothermia, or simply because they were kept from developing hyperthermia In this week’s NEJM, Nielsen et al report findings from a large randomized controlled trial that addresses this question. The trial, conducted in intensive care units across Europe and Australia, randomly assigned 950 unconscious adults who had suffered out-of-hospital cardiac arrest to targeted temperature management at either 33°C ( induced hypothermia ) or 36°C ( near-normal temperature ) for 36 hours. In contrast to the previous studies, which only included patients with ventricular fibrillation, this study enrolled patients with both shockable and nonshockable rhythms. Importantly, fever prevention measures were used to keep all patients below 37.5°C until 72 hours after cardiac arrest. The primary outcome was all-cause mortality, and the main secondary outcome was a composite of neurologic function and death at 180 days. Unlike the previous studies, this trial established a clear protocol for when life-sustaining therapy should be withdrawn. A physician blinded to the intervention assignments performed neurological evaluations 72 hours after the intervention period ended and recommended either continuing or withdrawing life-sustaining therapy, according to pre-specified criteria. During the first seven days, life-sustaining therapy was withdrawn in 132 patients in the 33°C group and 115 in the 36°C group, for reasons including brain death and multi-organ failure. By the end of the trial, overall mortality did not differ significantly between the two study arms: 50% of the patients in the 33°C group had died, as compared to 48% of those in the 36°C group (HR 1.06, p=0.51). There was also no difference between the two groups in neurological function (measured either by the Cerebral Performance Category: HR 1.02, p=0.78; or by the modified Rankin scale: HR 1.01, p=0.87) or death at 180 days (HR 1.01, p=0.92). Is therapeutic hypothermia actually therapeutic, then In this study, neither benefit nor harm was evident at 33°C as compared to 36°C. Several factors may have contributed to the departure of results from those of older studies. This trial had fewer exclusion criteria, resulting in a broader, more heterogeneous patient population; 20% of participants, for example, had nonshockable rhythms. In addition, improvements in pre-hospital and critical care management over the last decade may have made it harder to isolate the incremental benefits of a single intervention. Finally, as some have argued all along, it is possible that the real value of targeted temperature management lies not in the induction of hypothermia but rather in the prevention of hyperthermia. In an accompanying editorial, Drs. Jon Rittenberger and Clifton Callaway of the University of Pittsburgh write, The exceptional rates of good outcomes in both the 33°C and 36°C groups in the present trial may reflect the active prevention of hyperthermia. Whatever the mechanisms, it seems clear that we should not regress to a pre-2002 style of care that does not manage temperature at all. They conclude, Perhaps the most important message to take from this trial is that modern, aggressive care that includes attention to temperature works, making survival more likely than death when a patient is hospitalized after CPR. NEJM Deputy Editor Dr. John Jarcho states, This trial illustrates the importance of carefully testing and evaluating each individual component of patient management in critical care, to be certain that our practice is not only evidence-based, but based on evidence that is derived from adequate testing of appropriate options. Further investigation is needed to clarify whether, and to what extent, induced hypothermia can be therapeutic. If benefits can be demonstrated in future studies, additional research will also be needed to identify an optimal target temperature. It is encouraging that outcomes for patients who suffer cardiac arrest have improved considerably over the last decade. It is equally encouraging that even widely accepted treatment guidelines can be challenged by new evidence so that outcomes may continue to improve in the decades to come. What is your current approach to temperature management for unconscious patients brought into the hospital after cardiac arrest Is there a specific temperature you target How will the findings of this study affect your approach patients 18 years of age. or older who were unconscious (a score of <8 on. the Glasgow Coma Scale [on which scores range. from 3 to 15, with lower scores indicating reduced. levels of consciousness]) on admission to. the hospital after out-of-hospital cardiac arrest of. presumed cardiac cause, irrespective of the initial. rhythm. Eligible patients had more than 20 consecutive. minutes of spontaneous circulation after. resuscitation.14 The main exclusion criteria were. an interval from the return of spontaneous circulation. to screening of more than 240 minutes, unwitnessed arrest with asystole as the initial. rhythm, suspected or known acute intracranial. hemorrhage or stroke, and a body temperature of. less than 30°C.")
32
CO2 can be good for you! Hypocapnie: Hypercapnie: Lésions neuronales
Modèles animaux et après TBI Hypercapnie: Action de neuroprotection Hypercapnie modérée augmente la perfusion cérébrale Propriétès anticonvulsivantes, anti oxydantes et antiinflammatoires Améliore le pronostic neurologique et limite la lésion cérébrale dans modèle ischémie reperfusion et AVC Amélioration du métabolisme oxydatif et inhibition de la production de glutamate Attention: HIC, HTAP, CPA et altération fonction VD On the other hand, we found that hypercapnia was independently associated with a greater chance of discharge home. This is consistent with previous findings that elevated PaCO2 is associated with less brain damage and better neurological outcome in animal models of hypoxia–ischemia14 and stroke.37 These findings appear mediated by improved oxidative metabolism and inhibition of glutamate secretion.18,38,39 Moreover, CO2 can increase cerebral blood flow and tissue oxygen tension via cerebrovascular vasodilatation.40,41 Indeed, there is evidence that cerebral blood flow could be decreased in the post-resuscitation phase15,42 due to an imbalance between local vasodilators and vasoconstrictors. Therefore, CO2 mediated vasodilatation might reverse these abnormalities. This was demonstrated in a recent physiologic study,43 where the upper normal range PaCO2 (45 mmHg) was associated with increased cerebral perfusion and decreased cerebral lactate as compared with lower normal range PaCO2 (30 mmHg). This hypothesis remains plausible even in the context of therapeutic hypothermia as such therapy does not seem to affect cerebrovascular reactivity to PaCO2.44 Despite these findings, there are concerns that hypercapnia after cardiac arrest could be associated with pulmonary vasoconstriction, impaired right ventricular function, respiratory acidosis and increased intracranial pressure, all of which could lead to poor patient outcomes.46 Indeed, severe hypercapnia has been shown to be deleterious.47,48 In a rat model of cerebral ischemiareperfusion injury49 moderate hypercapnia (60–100 mmHg) was found to be neuro-protective while severe (>100 mmHg) hypercapnia increased brain injury. Hence, the International Liaison Committee on Resuscitation (ILCOR) currently recommends a normal PaCO2 as target for mechanically ventilated cardiac arrest survivors.50 Our findings, however, suggest that mild to moderate hypercapnia may not be harmful
 was associated. with increased cerebral perfusion and decreased cerebral lactate. as compared with lower normal range PaCO2 (30 mmHg). This. hypothesis remains plausible even in the context of therapeutic. hypothermia as such therapy does not seem to affect cerebrovascular. reactivity to PaCO2.44. Despite these findings, there are concerns that hypercapnia. after cardiac arrest could be associated with pulmonary vasoconstriction, impaired right ventricular function, respiratory acidosis. and increased intracranial pressure, all of which could lead to. poor patient outcomes.46 Indeed, severe hypercapnia has been. shown to be deleterious.47,48 In a rat model of cerebral ischemiareperfusion. injury49 moderate hypercapnia (60–100 mmHg) was. found to be neuro-protective while severe (>100 mmHg) hypercapnia. increased brain injury. Hence, the International Liaison. Committee on Resuscitation (ILCOR) currently recommends a normal. PaCO2 as target for mechanically ventilated cardiac arrest. survivors.50 Our findings, however, suggest that mild to moderate. hypercapnia may not be harmful.")
33
Eviter l’hypocapnie et peut être tolérerer une certaine hypercapnie
Sortie à domicile pour survivants Eviter l’hypocapnie et peut être tolérerer une certaine hypercapnie Normocapnie Hypercapnie Odd Ratio 3.6. APD-PaCO2 timing and relationship with peak PaCO2 Within the Full-ABG cohort, the APD-PaCO2 corresponded with a value measured within the first 2 h of admission in 90.7% and in the first 4 h in 94% of cases. Similarly, within the Austin cohort, 83% of such values were obtained within the first 2 h and 96% within the first 4 h. 3.7. Classification into CO2 groups As presented in Table 4, within patients in the Full-ABG cohort classified as hypocapnic using the APD-PaCO2, 85.6% of all CO2 values taken in the first 24 h were within the hypocapnic or normocapnic range. Similarly, for those patients classified as hypercapnic, 90% of all CO2 values were in the normocapnic or hypercapnic range. Normocapnie Hypocapnie

34
Oxygen: when Too much is not good!

35
You hacve all seen this phenomenon
You hacve all seen this phenomenon. Cut a nice apple and in a short period of time you will find this browny lawer, this crust on top of your fruit. Doesn’t look so good now! In fact, Apple contains enzymes (polyphenol oxidase) that react with oxygen and this form this sort of rust on the surface of the fruit. When the fruit is cut or damage, oxygen will react with the cells. Let think abot lung Cells , injured or bruised and exposed to high FiO2. Does it apply in the same way.
 that react with oxygen and this form this sort of rust on the surface of the fruit. When the fruit is cut or damage, oxygen will react with the cells. Let think abot lung Cells , injured or bruised and exposed to high FiO2. Does it apply in the same way.")
36
Hospital death with hyperoxia and normoxia on first ABG on ICU admission post ROSC.
Kilgannon et al 2010 IMPACT/ 131 ICU in USA Retrospective data base CPR in the 24 hours 6326 patients Mortality rate /PaO2 >300: 63% <60: 57% 60< >300: 45% Hyperoxia lowered likelihood of independent functional status (n=1171) (n=1156) Early 1976, 200 patients with myoacardial infarction, 6l versus air for the first 24 hours, randomizd control trial, no significant difference in mortality, arythmia anbalgesics used In dogs resuscitated with ox or air , worse neurologic defict after 12 and 24 hours A llarger clinical trial collected data from project impactr (131 ICU in USA°, cardiac arrest, non trauma, ; patients classified as hypoxic, normoxic or hyperoxicet al. reported results of a multi-center trial comparing outcomes in patients after non-traumatic cardiac arrest based on PaO2. They showed that hyperoxemia (PaO2 300 mmHg) was associated with increased mortality compared to both the normoxemic and the hypoxemic group (PaO2 60 mmHg). Reperfusion after an ischemic insult is associated with a surge of reactive oxygen species, which may overwhelm host natural antioxidant defenses The oxidative stress from the reactive oxygen species formed after reperfusion may lead to increased cellular death by diminishing mitochondrial oxidative metabolism, disrupting normal enzymatic activities, and damaging membrane lipids through peroxidation Since both hypoxia and hyperoxia exposures were associated with lower survival, it appears that supplemental oxygen may be a drug with a narrow therapeutic window in postresuscitation care. .
 (n=1156) Early 1976, 200 patients with myoacardial infarction, 6l versus air for the first 24 hours, randomizd control trial, no significant difference in mortality, arythmia anbalgesics used. In dogs resuscitated with ox or air , worse neurologic defict after 12 and 24 hours. A llarger clinical trial collected data from project impactr (131 ICU in USA°, cardiac arrest, non trauma, ; patients classified as hypoxic, normoxic or hyperoxicet al. reported results of a multi-center trial comparing outcomes in patients after non-traumatic cardiac arrest based on PaO2. They showed that hyperoxemia (PaO2 300 mmHg) was associated with increased mortality compared to both the normoxemic and the hypoxemic group (PaO2 60 mmHg). Reperfusion after an ischemic insult is associated with a surge of reactive oxygen species, which may overwhelm host natural antioxidant defenses The oxidative stress from the reactive oxygen species formed after reperfusion may lead to increased cellular death by diminishing mitochondrial oxidative metabolism, disrupting normal enzymatic activities, and damaging membrane lipids through peroxidation. Since both hypoxia and hyperoxia exposures were associated with lower survival, it appears that supplemental oxygen may be a drug with a narrow therapeutic window in postresuscitation care. .")
37
Avoid Hyperoxaemia after ROSC; titrate oxygen to SaO2 94-98% !

40
Enjeux du traitement de l’arrêt cardiaque
Neuroprotection: Limiter les conséquences de l’arrêt cardiaque Hypothermie thérapeutique Echanges gazeux: PaO2, SaO2, PaCO2 Métabolique: Variation de la glycémie, hyper, hypoglycémie Traitements: cyclosporine, érythropoiétine ?

41
Enjeux du traitement de l’arrêt cardiaque
Prevention de l’infection: Coma et inhalation: Pneumopathies précoces fréquentes Contrôle des VAS Hypothermie Voies d’abord MCE, VM, inhalation : PAVM

42
Pronostic de l’arrêt cardiaque: évaluation
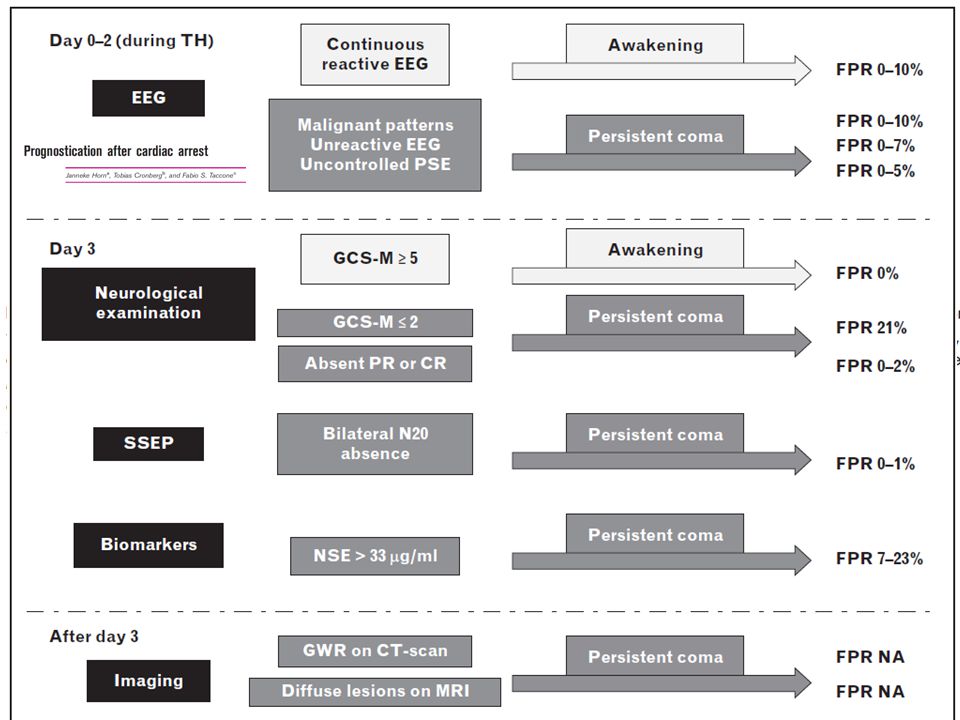
After cardiac arrest, neurologic examen and score GOS or CPC, neurological outcomewillimprove within1–2 weeks after brain injury. Although it is generally considered that almost all patients who survive after cardiac arrest have a good outcome (GOS 5 or CPC 1), it is also known that substantial cognitive disturbances can be detected in as much as 50%of this population Early prediction of a poor prognosis based solely on neurological examination could lead to withdrawal of lifesustaining therapy in almost 20% of patients, who would otherwise have a complete neurological Preservation of the N20 response does not imply a favorable outcome, almost half the patients with a present N20 will have a poor outcome. Other evoked potentials have been investigated in patients with PAC but only in small studies, leaving too much uncertainty at the moment to advocate their use in daily clinical care. Potentially, cognitiveevoked potentials, such as the P300 and ‘mismatch negativity’, may be useful to predict a good outcome The most extensively studied biomarkers of brain injury in cardiac arrest patients are neuron-specific enolase (NSE) and S-100b a CT scan on admission is helpful to rule out the cerebral causes of coma or cardiac arrest [53,54]. For prognostication in PAC, MRI seems to be a more promising tool. Especially, apparent diffusion coefficient techniques can reveal the details of hypoxic–ischemic brain injury and may provide useful additional information to predict outcome in patients with PAC [55–57]. The optimal timing to perform MRI would be 2–5 days after cardiac arrest After initial neurological examination, continuous or repeated standard EEG monitoring should be started to identify early seizures or ‘malignant’ EEG patterns. A reactive EEG or continuous background activity indicates a high probability of good outcome and these patients usually wake up quickly after discontinuation of sedation. In contrast, malignant EEG patterns are associated with a poor outcome. Aggressive therapy should be considered for PSE, especially if it occurs in the re-warming phase and in the absence of other signs of extensive brain injury. Importantly, no EEG finding alone should be used to predict poor outcome. A prolonged observation period (1–2 weeks) should be considered to allow for delayed neurological recovery recovery [16]. Thus, when therapeutic hypothermia is used, only the loss of all brain-stem functions can be regarded as poor prognostic factors in the very early phase. These are usually signs of total brain infarction and herniation, which happens in only a small minority of patients after cardiac arrest If the patient remains unresponsive to pain or with extension to painful stimuli (GCS-M 2) on day 3, a poor prognosis is likely in 80% of patients. Pupillary and corneal reflexes confer additional prognostic information, as a bilateral absence On the opposite, generalized myoclonus (including face, trunk and limbs) and continuing for more than 30 min can be regarded as a status myoclonus. This is associated with a very high rate of poor neurological outcome, especially if this occurs in the first day after arrest [23]. Statusmyoclonus is often associated with burst suppression on EEG, further supporting extensive brain damage survivors with good neurological recovery have been reported, a status myoclonus should no longer motivate a decision to withdraw intensive care [25 Somatosensory-evoked potentials The SSEP is a small electrical signal that can be recorded noninvasively from the skull after administering a set of electrical stimuli to one of the peripheral nerves. For prognosis of a poor outcome after cardiac arrest, only the short cortical latencies (N20, expected to appear 20ms after median nerve stimulation) are used [34]. In order to have ‘absent SSEPs’, predictive of a poor outcome, cortical responses have to be absent bilaterally in a technically well performed test [35]. In patients with PAC, SSEPs have been shown to reliably predict poor outcome, with a FPR of (95% CI 0.001–0.047) [6&&]. Cortical N20 responses are not influenced by moderate sedation or metabolic disturbances [36]. False positives were identified when SSEP was performed too early (within 24 h) after cardiac arrest [37]
, it is. also known that substantial cognitive disturbances. can be detected in as much as 50%of this population Early prediction. of a poor prognosis based solely on neurological. examination could lead to withdrawal of lifesustaining. therapy in almost 20% of patients, who. would otherwise have a complete neurological Preservation of the. N20 response does not imply a favorable outcome, almost half the patients with a present N20 will have. a poor outcome. Other evoked potentials have been investigated in. patients with PAC but only in small studies, leaving. too much uncertainty at the moment to advocate. their use in daily clinical care. Potentially, cognitiveevoked. potentials, such as the P300 and ‘mismatch. negativity’, may be useful to predict a good outcome The most extensively. studied biomarkers of brain injury in cardiac arrest. patients are neuron-specific enolase (NSE) and. S-100b a CT scan on admission is helpful to rule out the. cerebral causes of coma or cardiac arrest [53,54]. For prognostication in PAC, MRI seems to be a. more promising tool. Especially, apparent diffusion. coefficient techniques can reveal the details of. hypoxic–ischemic brain injury and may provide. useful additional information to predict outcome. in patients with PAC [55–57]. The optimal timing to. perform MRI would be 2–5 days after cardiac arrest After initial neurological. examination, continuous or repeated standard. EEG monitoring should be started to identify early. seizures or ‘malignant’ EEG patterns. A reactive EEG. or continuous background activity indicates a high. probability of good outcome and these patients. usually wake up quickly after discontinuation of. sedation. In contrast, malignant EEG patterns are. associated with a poor outcome. Aggressive therapy. should be considered for PSE, especially if it occurs. in the re-warming phase and in the absence of. other signs of extensive brain injury. Importantly, no EEG finding alone should be used to predict. poor outcome. A prolonged. observation period (1–2 weeks) should be considered. to allow for delayed neurological recovery. recovery [16]. Thus, when therapeutic hypothermia. is used, only the loss of all brain-stem functions can. be regarded as poor prognostic factors in the very. early phase. These are usually signs of total brain. infarction and herniation, which happens in only a. small minority of patients after cardiac arrest If the patient remains unresponsive to pain or. with extension to painful stimuli (GCS-M 2) on. day 3, a poor prognosis is likely in 80% of patients. Pupillary and corneal reflexes confer additional. prognostic information, as a bilateral absence On the opposite, generalized myoclonus (including face, trunk. and limbs) and continuing for more than 30 min. can be regarded as a status myoclonus. This is. associated with a very high rate of poor neurological. outcome, especially if this occurs in the first day. after arrest [23]. Statusmyoclonus is often associated. with burst suppression on EEG, further supporting. extensive brain damage survivors with good neurological recovery have. been reported, a status myoclonus should no longer. motivate a decision to withdraw intensive care [25 Somatosensory-evoked potentials. The SSEP is a small electrical signal that can be. recorded noninvasively from the skull after administering. a set of electrical stimuli to one of the. peripheral nerves. For prognosis of a poor outcome. after cardiac arrest, only the short cortical latencies. (N20, expected to appear 20ms after median nerve. stimulation) are used [34]. In order to have ‘absent. SSEPs’, predictive of a poor outcome, cortical. responses have to be absent bilaterally in a technically. well performed test [35]. In patients with. PAC, SSEPs have been shown to reliably predict poor. outcome, with a FPR of (95% CI 0.001–0.047) [6&&]. Cortical N20 responses are not influenced by. moderate sedation or metabolic disturbances [36]. False positives were identified when SSEP was performed. too early (within 24 h) after cardiac arrest. [37]")
44
DTI: diffusion tensor imaging can characterize the architecture of the white matter by exploring the diffusion of water molecules in the brain FA: Fractional anisotropy on of the three Eigenvalues of the diffusion tensor ADC: apparent diffusion coefficient Clinical score combined withh reaction too pain (no, extension or abnormal flexion), reflexe pupillaire et cornéen, GCS,
, reflexe pupillaire et cornéen, GCS,")
46
Pronostic après Arrêt Cardiaque
Limitations thérapeutiques: réflexion éthique, LATA , PMO impact famille et soignants Pronostic cardiaque Pronostic neurologique: fonctions motrices, supérieures, cognitives Pronostic psychologique: Anxiété: % Dépression: 8-45% PTSD: % Devenir social et familial: qualité de vie, symptomes “familiaux” Coûts familial, social et sociétal

47
Devenir des arrêts cardiaques réanimés
SMR; standardized mortality rate (mortalité observée d’une population standardisée de 11% soit une SMR de 2,3 (1,9-2,9) The SMR for death due to cardiac disease, in OHCA of cardiac origin, was higher than the overall SMR with a value of 42 in males and 140 in females Origine des décés surtout cardiaque après la sortie..brain injury à l’hopital Nb d’années de vie gagnées : 22,8 ans Survie à 1 an: 90% CI 95%: 85,4-93,6 Survie à 5 ans: 76% CI 95%: 69-82,4 Mortalité observée : 25% SMR : 2,3 (1,9-2,9)
 The SMR for death due to cardiac disease, in OHCA of cardiac origin, was higher than the overall SMR with a value of 42 in males and 140 in females. Origine des décés surtout cardiaque après la sortie..brain injury à l’hopital. Nb d’années de vie gagnées : 22,8 ans. Survie à 1 an: 90% CI 95%: 85,4-93,6. Survie à 5 ans: 76% CI 95%: 69-82,4. Mortalité observée : 25% SMR : 2,3 (1,9-2,9)")
48
Relation Activité et Pronostic
En fait Pour chaque augmentation de 5 malades traités, augmentation de: - Survie OR:1,06; 95%CI 1,04-1,08 - Bon pronostic neurologique: OR 1,06; 95%CI 1,04-1,08

49
Indications de développer des centres spécialisés de prise en charge
Message: Relation nombre d’arrêts cardiaques pris en charge et pronostic de l’ACR Indications de développer des centres spécialisés de prise en charge 87 ICU admissions 5857 ACR Mortalité: 56% Cardiopulmonary resuscitation of good quality, with uninterrupted chest compressions as well as early defibrillation - depending on initial electrocardiogram rhythm - improves the outcome after cardiac arrest significantly [5-7]. The etiology of cardiac arrest is also known to influence the prognosis. Of note is the fact, that the outcome of patients resuscitated from cardiac arrest treated in different hospitals and intensive care units (ICU) has shown a significant variability [8-10]. Hospital factors during the postresuscitation period and their implications for patient survival have long been underappreciated and have not been well defined. Geographic factors as well as the level of care of the centers involved influence outcome after cardiac arrest and cost effectiveness [9,11,12]. The first standardized algorithms for the postresuscitation care period have just recently been implemented in the European guidelines for resuscitation [13]. Several hospital-related factors, such as hospital size and teaching status have been identified to be of importance for the outcome after cardiac arrest and regional differences have been described [10,14,15]. With regard to the role models of acute coronary care units, stroke-, trauma- and burn injury centers, specialized cardiac arrest care centers as well as predefined treatment bundles for the postresuscitation period have become a subject of discussion recently [16-24]. the frequency of post cardiac arrest intensive care was associated with risk-adjusted mortality. The ICU stratum with the highest number of resuscitations showed the lowest riskadjusted mortality. The SAPS II adjusted, observed to expected mortality ratios (O/E-Ratios) in the three strata (less than <18; 18 to 26; more than 26 resuscitations per ICU per year) were 0.869 (95-%-confidence interval: – 894), ( ) and ( 0.833). A comparison of postresuscitation care in Göteborg found a significant difference in survival to discharge rate of two hospitals (33% vs. 44%). This was caused by baseline differences, socioeconomic status and in hospital factors (technical capabilities and staff resources) [9]. Carr et al. investigated correlations between hospital related factors and outcome after cardiac arrest in different hospitals in the US. They found different mortality rates rather comparing A significant difference in intensive care measures provided was found. Especially the reduced use of mechanical ventilation, renal support and multiple vasoactive substances probably reflects a different treatment approach in higher volume centers. In contrast to Callaway et al. we did not find an association between the hospital’s capability to perform coronary angiography and mortality [12]. hospital status than treatment frequency. The highest survival was found in large teaching hospitals in urban areas [14]. The same authors found an association between the volume of cardiac arrest cases treated per year and favourable outcome [10]. In contrast Callaway et al. found no independent associations between survival or length of stay and hospital characteristics [12]. Our analysis identified a subgroup of cardiac arrest patients with low to intermediate SAPS II scores, whose post cardiac arrest intensive care in a specialized high frequency center was associated with lower mortality (Figure 1). This might be caused by the fact that most patients above a specific SAPS II score are so severely injured that none of the expertise in those high frequency centers could change their grim outcome. Nombre d’Arrêt Cardiaque
 has shown a significant variability [8-10]. Hospital factors during the postresuscitation period and their implications for patient survival. have long been underappreciated and have not been well defined. Geographic factors as well. as the level of care of the centers involved influence outcome after cardiac arrest and cost. effectiveness [9,11,12]. The first standardized algorithms for the postresuscitation care period. have just recently been implemented in the European guidelines for resuscitation [13]. Several hospital-related factors, such as hospital size and teaching status have been identified. to be of importance for the outcome after cardiac arrest and regional differences have been. described [10,14,15]. With regard to the role models of acute coronary care units, stroke-, trauma- and burn injury centers, specialized cardiac arrest care centers as well as predefined. treatment bundles for the postresuscitation period have become a subject of discussion. recently [16-24]. the frequency of post cardiac arrest intensive care was associated with risk-adjusted. mortality. The ICU stratum with the highest number of resuscitations showed the lowest riskadjusted. mortality. The SAPS II adjusted, observed to expected mortality ratios (O/E-Ratios) in the three strata (less than <18; 18 to 26; more than 26 resuscitations per ICU per year) were (95-%-confidence interval: – 894), ( ) and ( ). A comparison of postresuscitation care in Göteborg found a significant difference in survival. to discharge rate of two hospitals (33% vs. 44%). This was caused by baseline differences, socioeconomic status and in hospital factors (technical capabilities and staff resources) [9]. Carr et al. investigated correlations between hospital related factors and outcome after cardiac. arrest in different hospitals in the US. They found different mortality rates rather comparing A significant difference in intensive. care measures provided was found. Especially the reduced use of mechanical ventilation, renal support and multiple vasoactive substances probably reflects a different treatment. approach in higher volume centers. In contrast to Callaway et al. we did not find an. association between the hospital’s capability to perform coronary angiography and mortality. [12]. hospital status than treatment frequency. The highest survival was found in large teaching. hospitals in urban areas [14]. The same authors found an association between the volume of. cardiac arrest cases treated per year and favourable outcome [10]. In contrast Callaway et al. found no independent associations between survival or length of. stay and hospital characteristics [12]. Our. analysis identified a subgroup of cardiac arrest patients with low to intermediate SAPS II. scores, whose post cardiac arrest intensive care in a specialized high frequency center was. associated with lower mortality (Figure 1). This might be caused by the fact that most. patients above a specific SAPS II score are so severely injured that none of the expertise in. those high frequency centers could change their grim outcome. Nombre d’Arrêt Cardiaque.")
50
Transport des patients vers un Centre Spécialisé
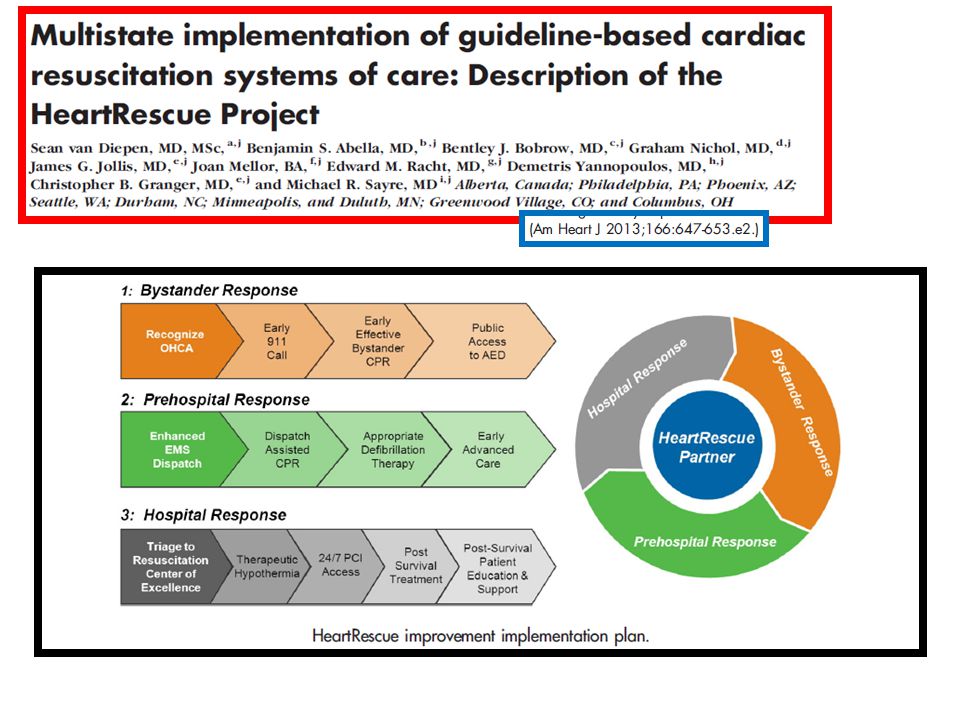
Hospitals with this designation were original called Cardiac Arrest Centers, but as noted above, these same centers were often the ones equipped to care for patients with STEMIs. Thus, in Arizona, the designation of these hospitals was changed to Cardiac Receiving Centers (CRCs). One criticism of this concept was the safety of a delay of therapy by increasing the transit time by bypassing the nearest hospital to reach a CRC-designated hospital. Spaite and colleagues did an observational study looking at the feasibility and safety of transporting patients to the CRC, bypassing the nearest hospital en route. Results showed that a modest increase in transport time (about 15 minutes) did not influence survival. Spaite DW, Bobrow BJ, Vadeboncoeur TF, et al. The impact of prehospital transport interval on survival in out-of-hospital cardiac arrest: Implications for regionalization of post-resuscitation care. Resuscitation. 2008;79:61–66. Spaite DW, Stiell IG, Bobrow BJ, et al. Effect of transport interval on out-of-hospital cardiac arrest survival in the OPALS study: implications for triaging patients to specialized cardiac arrest centers. Ann Emerg Med. 2009;54:248–255. Temps de transport modéré ne modifiait pas le pronostic et n’influençait pas la survie
. One criticism of this concept was the safety of a delay of therapy by increasing the transit time by bypassing the nearest hospital to reach a CRC-designated hospital. Spaite and colleagues did an observational study looking at the feasibility and safety of transporting patients to the CRC, bypassing the nearest hospital en route. Results showed that a modest increase in transport time (about 15 minutes) did not influence survival. Spaite DW, Bobrow BJ, Vadeboncoeur TF, et al. The impact of prehospital transport interval on survival in out-of-hospital cardiac arrest: Implications for regionalization of post-resuscitation care. Resuscitation. 2008;79:61–66. Spaite DW, Stiell IG, Bobrow BJ, et al. Effect of transport interval on out-of-hospital cardiac arrest survival in the OPALS study: implications for triaging patients to specialized cardiac arrest centers. Ann Emerg Med. 2009;54:248–255. Temps de transport modéré ne modifiait pas le pronostic et n’influençait pas la survie.")
52
RESULTATS: ACR - ECLS en 2012 Admises en Réanimation (>4H)
Veino-Artérielle Admises en Réanimation (>4H) n=27 ECLS pour "Chocs cardiogéniques réfractaires" n=12 Décès précoce (<4H) n=10 ECLS ACR réfractaires n=15 ECLS ACR réfractaires Extra-Hospitaliers n=7 Survie=57.2% ECLS ACR réfractaires Intra-Hospitaliers n=8 Survie=0% Survie totale 16% sur 25 ACR canulés
 n=27. ECLS pour. Chocs cardiogéniques réfractaires n=12. Décès précoce (<4H) n=10. ECLS. ACR réfractaires. n=15. ECLS. ACR réfractaires. Extra-Hospitaliers. n=7. Survie=57.2% ECLS. ACR réfractaires. Intra-Hospitaliers. n=8. Survie=0% Survie totale. 16% sur 25 ACR canulés.")
53
Quels sont les Défis ? Coordination des soins: médical, technique, organisationnel Appliquer des interventions pour améliorer le pronostic Délais de prise en charge: ACR réfractaire Hypothermie thérapeutique Angioplastie coronaire Assistance circulatoire Antibiothérapie précoce Sédation, curarisation Evaluation neurologique, Evaluation neurophysiologique Volume de prise en charge, Centre hospitalier spécialisé de prise en charge secondaire

Présentations similaires