Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Chimiothérapie adjuvante
Dr Anne-Claire HARDY-BESSARD Clinique Armoricaine, Saint-Brieuc SFCP, Metz 19 Sept 2008

2
Quoi de neuf ? Décembre 2007 : SABCS Mai 2008 : ASCO
Septembre 2008 : ASCO BREAST 18 Aout 2008 : RBU Inca Cancer du sein

3
RBU Inca Cancer du sein ADJUVANT 1 2 3 Epirubicine
Epirubicine + Herceptin X Herceptin 1 an Taxol N+ ( 4 AC + 4 TXL / 3 sem) N+ hebdo Taxotère N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)
 N+ hebdo. Taxotère. N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)")
4
Epirubicine Tous les droits mais pas avec l’Herceptin

5
Herceptin 1 an Association avec taxanes non évoquée TCH ???

6
Essais d’Herceptin® adjuvant
T 3 sem. x 4 NSABP B31 AC x 4 T 3 sem. x 4 + H hebdo. 12 mois T hebdo. x 12 NCCTG N9831 AC x 4 T hebdo. x 12 H hebdo. 12 mois T hebdo. x 12 + H hebdo. 12 mois Observation H 3 sem. x 12 mois H 3 sem. x 24 mois HERA Toute chimio. adj. ou néoadj. AC x 4 Tx 3 sem. x 4 BCIRG 006 AC x 4 Tx 3 sem. x 4 + H 12 mois Carboplatine + Tx 3 sem. x 6 + H 12 mois Observation H = trastuzumab AC = adriamycine-cyclophosphamide ET = épirubicine-docétaxel T = paclitaxel. Tx = docétaxel FEC x 6 PACS 04 ET x 6 H 3 sem. x 12 mois D’après Saint-Gall 2003

7
Schéma des deux études initiales
Analyse combinée NSABP B31/NCCTG N9831 Schéma des deux études initiales NSABP B patientes, N+, HER2 IHC 3+ ou FISH+ Objectif : survie globale NCCTG N patientes, N+ et N-, HER2 IHC 3+ ou FISH+ Objectif : survie sans récidive Bras 1 Bras 2 AC P H Bras A (contrôle) Bras B (séquentiel) Bras C (concomitant) AC (adriamycine/cyclophosphamide 60/600 mg/m2 toutes les 3 sem. x 4 paclitaxel 175 mg/m2 toutes les 3 sem. x 4 paclitaxel 80 mg/m2 hebdomadaires x 12 trastuzumab dose de charge 4 mg/kg puis 2 mg/kg hebdomadaires x 51 (1 an) E.H. Romond et al., ASCO 2005
 Bras B (séquentiel) Bras C (concomitant) AC (adriamycine/cyclophosphamide 60/600 mg/m2 toutes les 3 sem. x 4. paclitaxel 175 mg/m2 toutes les 3 sem. x 4. paclitaxel 80 mg/m2 hebdomadaires x 12. trastuzumab dose de charge 4 mg/kg puis 2 mg/kg hebdomadaires x 51 (1 an) E.H. Romond et al., ASCO")
8
Analyse combinée NSABP B31/NCCTG N9831 Survie sans maladie
AC TH 87 % 85 % AC T % 75 % 67 % n Événements AC T AC TH HR = 0,48 ; 2 p = 3 x 10-12 Années depuis la randomisation

9
Analyse NSABP B31/NCCTG N9831 Survie sans maladie de chaque étude
1 2 3 4 5 50 60 70 80 90 100 B31 N9831 AC TH AC TH 87 % 87 % 85 % 86 % AC T AC T 78 % 74 % % % 66 % 68 % n Événements n Événements AC T AC T AC TH AC TH HR = 0,55 ; 2 p = 0,0005 HR = 0,45 ; 2 p = 1 x 10-9 Années depuis la randomisation

10
Analyse combinée NSABP B31/NCCTG N9831 Survie globale
94 % AC TH 91 % AC T 92 % 87 % n Décès AC T AC TH HR = 0,67 ; 2 p = 0,015 B31/N9831 Années depuis la randomisation

11
Analyse NCCTG N9831 Quand commencer Herceptin? B vs C
100 90 80 70 60 50 40 30 20 10 AC --> T + H --> H Events=53 AC --> T --> H Events=84 % Hazard ratio=0.64 Stratified logrank 2P=0.0114 Years Number of patients followed B C

12
Etude HERA Stratification Randomisation n = 1 694 n = 1 694 n = 1 693
16 Cancer du sein invasif HER2+ IHC3+ ou FISH+ avec confirmation centralisée Chirurgie + chimiothérapie (néo)adjuvante (CT) radiothérapie 5 090 patientes incluses 5 081 patientes analysables à 1 an Stratification Statut ganglionnaire, type de CT adjuvante, RH, hormonothérapie, âge, région Randomisation M. Piccart-Gebhart, du Centre Jules-Bordet de Bruxelles, a présenté, au nom des multiples co-investigateurs, les résultats de l’essai HERA. Cette étude comporte 3 bras : un bras contrôle sans trastuzumab (Herceptin®), un bras avec trastuzumab toutes les 3 semaines pendant une durée totale d’un an, et un bras avec trastuzumab toutes les 3 semaines pendant 2 ans. L’analyse intermédiaire présentée à l’ASCO étant très précoce, avec un an de recul médian, seule la comparaison entre le bras contrôle et le bras trastuzumab un an a été réalisée et communiquée. Les résultats portent donc sur patientes, au lieu des incluses au total dans cet essai. Pour les données d’efficacité antitumorale, l’analyse a été faite en intention de traiter. Pour les données de toxicité, les patientes randomisées dans les bras avec trastuzumab mais qui ne l’ont pas reçu ont été affectées au bras contrôle (n =1 736 pour le contrôle, et donc pour le bras traité). Les patientes étaient incluses après la fin de leur chimiothérapie adjuvante. Elles pouvaient également avoir reçu une chimiothérapie préopératoire. Les investigateurs n’avaient pas défini de schéma de chimiothérapie de référence en raison de la très grande diversité des pays participant à cette étude et de l’absence de consensus sur la chimiothérapie de référence en situation adjuvante. Trastuzumab 8 mg/kg 6 mg/kg 3 sem. x 2 ans Trastuzumab 8 mg/kg 6 mg/kg 3 sem. x 1 an Observation n = 1 694 n = 1 694 n = 1 693 ASCO 2005 n = 3 387 M.J. Piccart-Gehbart et al. ASCO 2005
adjuvante (CT) radiothérapie patientes incluses patientes analysables à 1 an. Stratification. Statut ganglionnaire, type de CT adjuvante, RH, hormonothérapie, âge, région. Randomisation. M. Piccart-Gebhart, du Centre Jules-Bordet de Bruxelles, a présenté, au nom des multiples co-investigateurs, les résultats de l’essai HERA. Cette étude comporte 3 bras : un bras contrôle sans trastuzumab (Herceptin®), un bras avec trastuzumab toutes les 3 semaines pendant une durée totale d’un an, et un bras avec trastuzumab toutes les 3 semaines pendant 2 ans. L’analyse intermédiaire présentée à l’ASCO étant très précoce, avec un an de recul médian, seule la comparaison entre le bras contrôle et le bras trastuzumab un an a été réalisée et communiquée. Les résultats portent donc sur patientes, au lieu des incluses au total dans cet essai. Pour les données d’efficacité antitumorale, l’analyse a été faite en intention de traiter. Pour les données de toxicité, les patientes randomisées dans les bras avec trastuzumab mais qui ne l’ont pas reçu ont été affectées au bras contrôle (n =1 736 pour le contrôle, et donc pour le bras traité). Les patientes étaient incluses après la fin de leur chimiothérapie adjuvante. Elles pouvaient également avoir reçu une chimiothérapie préopératoire. Les investigateurs n’avaient pas défini de schéma de chimiothérapie de référence en raison de la très grande diversité des pays participant à cette étude et de l’absence de consensus sur la chimiothérapie de référence en situation adjuvante. Trastuzumab. 8 mg/kg 6 mg/kg. 3 sem. x 2 ans. Trastuzumab. 8 mg/kg 6 mg/kg. 3 sem. x 1 an. Observation. n = n = n = ASCO 2005 n = M.J. Piccart-Gehbart et al. ASCO")
13
Caractéristiques des patientes
Etude HERA Caractéristiques des patientes Relecture centralisée du statut HER2 50 % RH % N- 6 % chimiothérapie adjuvante sans anthracyclines Résultats 0,26 0,47-1,23 0,76 96 % 95 % Survie globale < 0,0001 0,40-0,66 0,51 89,7 % 81,8 % Survie sans métastase 0,40-0,63 0,50 87,2 % 78,6 % Survie sans récidive p IC95 RR Bras trastuzumab (Herceptin®) Bras contrôle La répartition des patientes entre les deux bras était bien équilibrée. Seules 6 % d’entre elles n’avaient pas reçu d’anthracyclines dans leur chimiothérapie adjuvante, qui devait comporter un minimum de 4 cycles. Trente-deux pour cent n’avaient pas d’envahissement ganglionnaire. Malgré le recul médian de seulement un an, la différence de survie sans maladie était déjà très nettement significative en faveur du traitement avec trastuzumab. La différence était également nette en termes de survie sans métastase. L’analyse était trop précoce pour avoir des éléments précis sur la survie globale. M.J. Piccart-Gehbart et al. ASCO 2005
 Bras contrôle. La répartition des patientes entre les deux bras était bien équilibrée. Seules 6 % d’entre elles n’avaient pas reçu d’anthracyclines dans leur chimiothérapie adjuvante, qui devait comporter un minimum de 4 cycles. Trente-deux pour cent n’avaient pas d’envahissement ganglionnaire. Malgré le recul médian de seulement un an, la différence de survie sans maladie était déjà très nettement significative en faveur du traitement avec trastuzumab. La différence était également nette en termes de survie sans métastase. L’analyse était trop précoce pour avoir des éléments précis sur la survie globale. M.J. Piccart-Gehbart et al. ASCO")
14
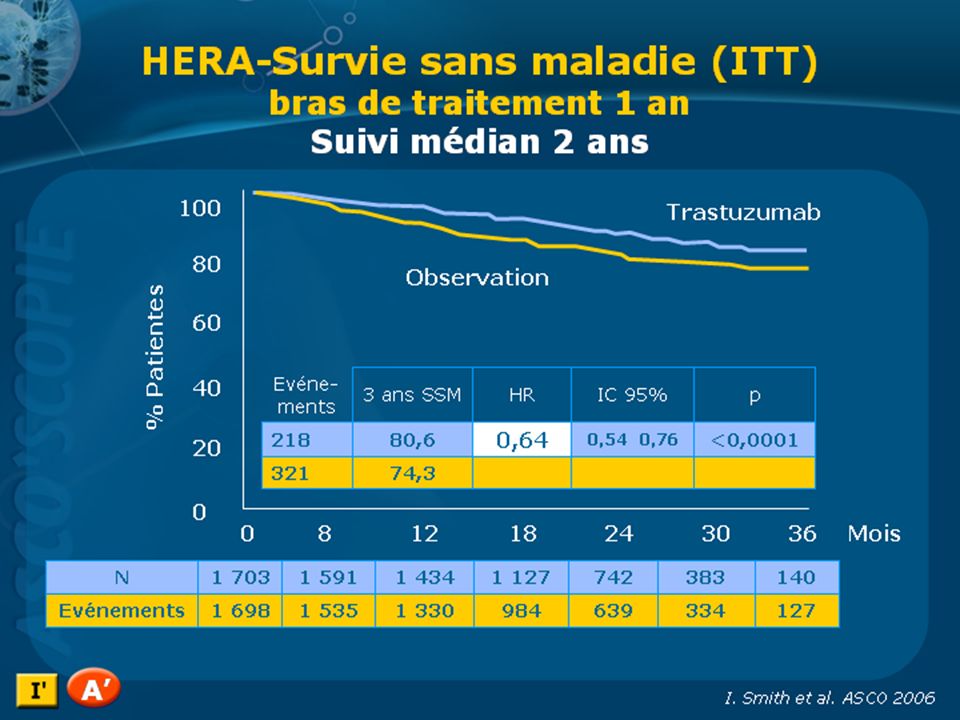
Etude HERA : Survie sans maladie
1 an d ’Herceptin® 100 80 Observation 60 Vie sans maladie (%) 2 - ans 40 SSM % HR IC95 Événements p 20 127 85,8 0,54 0,43-0,67 < 0,0001 Malgré le recul médian de seulement un an, la différence de survie sans maladie était déjà très nettement significative en faveur du traitement avec trastuzumab (Herceptin®). L’analyse en sous-groupes montrait un bénéfice dans tous les groupes, la différence n’étant pas toujours significative en raison de faibles effectifs. 220 77,4 5 10 15 20 25 Mois depuis la randomisation n à risque 1 694 1 472 1 067 629 303 102 1 693 1 428 994 580 280 87 M.J. Piccart-Gehbart et al. ASCO 2005
 2 - ans. 40. SSM. % HR. IC95. Événements. p ,8. 0,54. 0,43-0,67. < 0,0001. Malgré le recul médian de seulement un an, la différence de survie sans maladie était déjà très nettement significative en faveur du traitement avec trastuzumab (Herceptin®). L’analyse en sous-groupes montrait un bénéfice dans tous les groupes, la différence n’étant pas toujours significative en raison de faibles effectifs , Mois depuis la randomisation. n à risque M.J. Piccart-Gehbart et al. ASCO")
16
BCIRG 006 ACT Her2+ N+ or high risk N- ACTH TCH 4 x AC 60/600 mg/m2
4 x Docetaxel 100 mg/m2 ACT Her2+ (Central FISH) N+ or high risk N- 4 x AC 60/600 mg/m2 4 x Docetaxel 100 mg/m2 ACTH 1 Year Trastuzumab 6 x Docetaxel and Carboplatin 75 mg/m2 AUC 6 N=3,222 TCH Stratified by Nodes and Hormonal Receptor Status 1 Year Trastuzumab Slamon D., SABCS 2005
 N+ or high. risk N- 4 x AC 60/600 mg/m2. 4 x Docetaxel. 100 mg/m2. ACTH. 1 Year Trastuzumab. 6 x Docetaxel and Carboplatin. 75 mg/m2 AUC 6. N=3,222. TCH. Stratified by Nodes and Hormonal Receptor Status. 1 Year Trastuzumab. Slamon D., SABCS")
17
Endpoints Primary Secondary Disease-free Survival Overall Survival
Toxicity Pathologic & Molecular Markers

18
Tumor Characteristics
Randomized (n=3,222) AC-T n=1,073 AC-TH n=1,074 TCH n=1,075 Number of nodes + % 29 1 – 3 39 38 4 – 10 22 24 23 > 10 11 9 10 Tumor Size (cm) 2 41 40 > 2 and 5 53 55 54 > 5 6 7 ER and/or PR +
 AC-T n=1,073. AC-TH n=1,074. TCH n=1,075. Number of nodes + % – – > Tumor Size (cm) > 2 and > ER and/or PR +")
19
First Interim Efficacy Analysis
1.0 93% 0.9 91% 86% 84% 86% 80% 80% 0.8 77% % Disease Free 73% Disease Free Survival 0.7 Patients Events 0.6 1073 147 AC->T 1074 77 AC->TH HR (AC->TH vs AC->T) = [0.37;0.65] P<0.0001 1075 98 TCH HR (TCH vs AC->T) = 0.61 [0.47;0.79] P=0.0002 0.5 1 2 3 4 5 Year from randomization
 = 0.49 [0.37;0.65] P< TCH. HR (TCH vs AC->T) = 0.61 [0.47;0.79] P= Year from randomization.")
20
SSR 2ème analyse intermédiaire
% de patientes en vie sans rechute 10 93 92 87 0,9 83 87 86 0,8 82 81 77 0,7 AC TH AC T TCH HR 0.61 [0.48;0.76] p<0,0001 Bénéfice absolu 6% 0,6 HR [0.54;0.83] p= Bénéfice absolu 7% Années 0,5 1 2 3 4 5 D. Slamon et al., SABCS 2007, abst. 13

21
RBU Inca Cancer du sein ADJUVANT 1 2 3 Epirubicine
Epirubicine + Herceptin X Herceptin 1 an Taxol N+ ( 4 AC + 4 TXL / 3 sem) N+ hebdo Taxotère N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)
 N+ hebdo. Taxotère. N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)")
22
Paclitaxel QW and Q3W vs Docetaxel QW and Q3W
Week 24, completion of therapy if HR negative Week 12, randomization P3: Paclitaxel 175 Q3W x 4 HR positive Tamoxifen OR Aromatase inhibitor Switch x 5 years Patients with N+ and N- ≥ 2 cm (N = 4988) Doxo 60 mg/m2 Cyclo 600 mg/m2 Q3W x 4 cycles P1: Paclitaxel 80 QW x 12 For more information about this study, please see the Capsule Summary at: Primary endpoint Survival without relapse or new cancer All 4 taxane treatment arms compared P3 treatment group compared to other 3 individually P3 group considered standard reference arm Current analysis reflects 4th interim results 856 protocol-defined disease/death occurrences including 483 deaths Median follow-up, 47 months D3: Docetaxel 100 Q3W x 4 D1: Docetaxel 35 QW x 12 Sparano JA, et al. SABCS Abstract 48.
 Doxo 60 mg/m2 Cyclo 600 mg/m2 Q3W x 4 cycles. P1: Paclitaxel 80. QW x 12. For more information about this study, please see the Capsule Summary at: Track=Metastatic%20Therapy. Primary endpoint. Survival without relapse or new cancer. All 4 taxane treatment arms compared. P3 treatment group compared to other 3 individually. P3 group considered standard reference arm. Current analysis reflects 4th interim results. 856 protocol-defined disease/death occurrences. including 483 deaths. Median follow-up, 47 months. D3: Docetaxel 100. Q3W x 4. D1: Docetaxel 35. QW x 12. Sparano JA, et al. SABCS Abstract 48.")
23
Paclitaxel QW and Q3W vs Docetaxel QW and Q3W
Outcome Pacli 3 n=1261 Pacli1 n=1239 Docé3 n=1243 Docé1 n=1245 P Protocol-defined negative outcome All events, n 230 195 206 225 Relapse ± death, n 199 172 171 192 Death, other, n 21 18 24 Contralateral BC, n 10 5 11 9 Survival without relapse/new tumor, HR compared with P3 1.20 1.13 1.03 .06 4-year disease-freeS, % 81 84 83 4-year overall survival, % 89 92 For more information about this study, please see the Capsule Summary at: *Disease-free survival advantage of P1 over P3, P = .06; D3 and D1 regimens not significantly different from P3, P = .20 and .78, respectively. Sparano JA, et al. SABCS Abstract 48.

24
RBU Inca Cancer du sein ADJUVANT 1 2 3 Epirubicine
Epirubicine + Herceptin X Herceptin 1 an Taxol N+ ( 4 AC + 4 TXL / 3 sem) N+ hebdo Taxotère N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)
 N+ hebdo. Taxotère. N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)")
25
R TAC vs FAC F 5-FU 500 mg/m2 Doxorubicine 50 mg/m2
Cyclophosphamide 500 mg/m2 R Toutes les 3 semaines x 6 cycles Stratification Ganglions Centre T A C Docetaxel 75 mg/m2 Doxorubicine 50 mg/m2 Cyclophosphamide 500 mg/m2

26
Caractéristiques de la tumeur
TAC n=745 % FAC n=746 Taille de la tumeur, cm 2 40 43 >2 and 5 53 51 > 5 8 6 Statut ganglionnaire 1-3 62 4 + 38 RE+ et/ou RP+ 76 HER2+ (FISH) 21 22
")
27
Survie sans rechute (ITT)
1.0 TAC 0.8 75% FAC 68% 0.6 Probabilité cumulative 0.4 N Evènements HR P Log Rank stratifié TAC FAC 0.2 0.0 6 12 18 24 30 36 42 48 54 60 66 Temps (mois)
")
28
Probabilité cumulative
Survie globale (ITT) 1.0 87% TAC 0.8 FAC 81% 0.6 Probabilité cumulative 0.4 N Evènements HR P Log-Rank stratifié TAC FAC 0.2 0.0 6 12 18 24 30 36 42 48 54 60 66 Temps (mois)
 % TAC FAC. 81% 0.6. Probabilité cumulative N Evènements HR P Log-Rank stratifié. TAC FAC Temps (mois)")
29
SSR par statut ganglionnaire
100 100 1-3 ganglions >4 ganglions 90 90 TAC 80 80 % en vie sans rechute FAC 70 70 TAC HR = 0.61 P = HR = 0.83 P = 0.17 60 60 FAC 50 50 6 12 18 24 30 36 42 48 54 60 66 6 12 18 24 30 36 42 48 54 60 66 Temps jusqu’au 1er évènement Temps jusqu’au 1er évènement Rapport des HRs 1.34 p=

30
PACS 01 6FEC100 C Fluorouracile 500 mg/m² J1 H
Stratification par: Centre Age: > or < 50 N: 1-3; > 4 6FEC100 Fluorouracile 500 mg/m² J1 Epirubicine mg/m² J1 Cyclophosphamide 500 mg/m² J1 6 cycles tous les 21 jours C H I R U G E R 3FEC100-3D 3 FEC 100 tous les 21 jours suivis de 3 Docetaxel 100 mg/m² tous les 21 jours Suivi médian: 59,7 mois Tamoxifene 20 mg/jour pendant 5 ans prescrit chez les patientes RH+ après chimiothérapie Prophylaxie primaire avec G-CSF et antibiotiques non-autorisée

31
Caractéristiques 6FEC100 N=996 3FEC100-3D N=1003 ² test
Age, médiane (intervalle) 49,8 (26,2-66,9) 50,0 (25,2-65,0) 0,38 < 50 ans, % 50,7 49,8 0,70 Tumorectomie, % 51,2 52,9 0,59 pT 2 cm, % 65,5 60,9 0,08 N 1-3, % 61,3 62,4 0,77 SBR 2-3, % 84,7 82,7 0,51 RE positive, % 71,1 76,3 0,016 RE et RP negative, % 22,3 19,1 0,023 Tamoxifene, % 68,4
 49,8 (26,2-66,9) 50,0 (25,2-65,0) 0,38. < 50 ans, % 50,7. 49,8. 0,70. Tumorectomie, % 51,2. 52,9. 0,59. pT 2 cm, % 65,5. 60,9. 0,08. N 1-3, % 61,3. 62,4. 0,77. SBR 2-3, % 84,7. 82,7. 0,51. RE positive, % 71,1. 76,3. 0,016. RE et RP negative, % 22,3. 19,1. 0,023. Tamoxifene, % 68,4.")
32
SSR à 5 ans, ITT 3FEC100-3Docetaxel: 78,3% 6FEC100: 73,2% RR: 17%
1,00 3FEC100-3Docetaxel: 78,3% Rechutes = 482 218 (21,7%) 264 (26,5%) 0,75 6FEC100: 73,2% 0,50 Probabilité Log-rank non ajusté P= 0,012 RR: 17% Log-rank ajusté P = 0,014 0,25 HR (Cox model) = 0,83 [0,69-0,99], P = 0,041 0,00 1 2 3 4 5 6 7 8 Temps (ans)
 264 (26,5%) 0,75. 6FEC100: 73,2% 0,50. Probabilité. Log-rank non ajusté P= 0,012. RR: 17% Log-rank ajusté P = 0,014. 0,25. HR (Cox model) = 0,83 [0,69-0,99], P = 0,041. 0, Temps (ans)")
33
SSR par N, ITT N > 4 N 1-3 Log-rank P = 0,042
HR (Cox model) = 0,76 [0,58-1,00] Kaplan-Meier Estimé 0,00 0,25 0,50 0,75 1,00 Survie (ans) 1 2 3 4 5 6 7 8 6FEC100 3FEC100-3Docetaxel N 1-3 Log-rank P = 0,120 HR (Cox model) = 0,87 [0,68-1,11]
 = 0,76 [0,58-1,00] Kaplan-Meier Estimé. 0,00. 0,25. 0,50. 0,75. 1,00. Survie (ans) FEC100. 3FEC100-3Docetaxel. N 1-3. Log-rank P = 0,120. HR (Cox model) = 0,87 [0,68-1,11]")
34
Survie Globale, ITT RR :23% Décés = 235 100 (10,0%) 135 (13,5%)
1,00 Décés = 235 100 (10,0%) 135 (13,5%) 0,75 3FEC100-3Docetaxel: SG à 5 ans = 90,7% 6FEC100: SG à 5 ans = 86,7% 0,50 Probabilité Log-rank non ajusté P = 0,013 Log-rank ajusté P = 0,017 HR (Cox model) = 0,77 [0,59-1,00], P = 0,050 RR :23% 0,25 0,00 1 2 3 4 5 6 7 8 Temps (ans)
 135 (13,5%) 0,75. 3FEC100-3Docetaxel: SG à 5 ans = 90,7% 6FEC100: SG à 5 ans = 86,7% 0,50. Probabilité. Log-rank non ajusté P = 0,013. Log-rank ajusté P = 0,017. HR (Cox model) = 0,77 [0,59-1,00], P = 0,050. RR :23% 0,25. 0, Temps (ans)")
35
RBU Inca Cancer du sein ADJUVANT 1 2 3 Epirubicine
Epirubicine + Herceptin X Herceptin 1 an Taxol N+ ( 4 AC + 4 TXL / 3 sem) N+ hebdo Taxotère N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)
 N+ hebdo. Taxotère. N+ ( TAC) N+ ( 3 FEC TXT) N- ( TAC ou TC)")
36
Phase III Trial Comparing Doxorubicin Plus Cyclophosphamide With Docetaxel Plus Cyclophosphamide As Adjuvant Therapy for Operable Breast Cancer J Clin Oncol. 2006;24: Jones & al. SABCS 2007

37
US Oncology 9735: Study Design
AC x 4 q3w Doxorubicin (60 mg/m2) Cyclophosphamide (600 mg/m2) n=510 R TC x 4 q3w Taxotere (75 mg/m2) Cyclophosphamide (600 mg/m2) N=1016 71% ER+ 48% N– USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. n=506 Chemotherapy doses based on actual BSA (no cap) Chemotherapy given prior to radiation Tamoxifen for all ER+ patients after chemotherapy +/- radiation Eligibility: Stage I, II, or III disease Jones et al. J Clin Oncol. 2006;24:
 Cyclophosphamide (600 mg/m2) n=510. R. TC x 4 q3w. Taxotere (75 mg/m2) Cyclophosphamide (600 mg/m2) N= % ER+ 48% N– USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. n=506. Chemotherapy doses based on actual BSA (no cap) Chemotherapy given prior to radiation. Tamoxifen for all ER+ patients after chemotherapy +/- radiation. Eligibility: Stage I, II, or III disease. Jones et al. J Clin Oncol. 2006;24:")
38
Disease-free Survival by Treatment
With a median follow-up of 7 years, disease-free survival remains significantly increased with TC. The reduction in risk of recurrence approximated 27%. The rates of DFS at 7 years were 81% in the TC arm and 75% in the AC arm. Jones et al. SABCS Abstract 12.

39
Disease-free Survival by Treatment and Age Group
The benefit of TC over AC in DFS remained in both age subgroups (<65 and ≥ 65 years of age). Jones et al. SABCS Abstract 12.
. Jones et al. SABCS Abstract 12.")
40
DFS for HER2-positive Patients
Within the HER2-positive subset, the HR for DFS with TC relative to AC was also 0.73, suggesting that the results are similar in this population despite the lack of anthracycline in the TC arm. Jones et al. SABCS Abstract 12.

41
DFS for HER2-negative Patients
The HR for DFS decreased further to 0.56 with TC in the HER2-negative subset. Jones et al. SABCS Abstract 12.

42
Overall Survival by Treatment
With respect to overall survival in the total study population, the improvement in survival with TC became statistically significant with 7 years of follow-up. The relative risk reduction was approximately 30% with TC relative to AC. The 7-year survival rates were 87% with TC and 82% with AC for an absolute survival benefit of 5%. Jones et al. SABCS Abstract 12.

43
Overall Survival by Treatment
With respect to overall survival in the total study population, the improvement in survival with TC became statistically significant with 7 years of follow-up. The relative risk reduction was approximately 30% with TC relative to AC. The 7-year survival rates were 87% with TC and 82% with AC for an absolute survival benefit of 5%. Jones et al. SABCS Abstract 12.

44
Survie Globale, ITT PACSO1, 1999 ptes, toutes N+, 40% > 3N+ RR :23%
1,00 Décés = 235 100 (10,0%) 135 (13,5%) 0,75 3FEC100-3Docetaxel: SG à 5 ans = 90,7% 6FEC100: SG à 5 ans = 86,7% 0,50 Probabilité Log-rank non ajusté P = 0,013 Log-rank ajusté P = 0,017 HR (Cox model) = 0,77 [0,59-1,00], P = 0,050 RR :23% 0,25 0,00 1 2 3 4 5 6 7 8 Temps (ans)
 135 (13,5%) 0,75. 3FEC100-3Docetaxel: SG à 5 ans = 90,7% 6FEC100: SG à 5 ans = 86,7% 0,50. Probabilité. Log-rank non ajusté P = 0,013. Log-rank ajusté P = 0,017. HR (Cox model) = 0,77 [0,59-1,00], P = 0,050. RR :23% 0,25. 0, Temps (ans)")
45
Etude TANGO R EC 90x 4 q3w puis 4 TXL 175 / 3 sem + GEM 1250 J1 J8
41% ER- 77% N+ 65% III 61% > 2cm 55% <50 ans 26% HER2 3+ USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. n=1576 Pool et al. J Clin Oncol. 2008

46
Etude TANGO Pas de différence en DFS ni en SG Suivi 35 mois 339 décès
548 évènements Pas de différence en DFS ni en SG USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. Pool et al. J Clin Oncol. 2008

47
CALGB/CTSU 49907 > 65 ans R 6 CMF ou 4 AC
DFS 91% TAC 86% FAC HR 0,66 ( 0,46-0,94) p = 0,202 6 CMF ou 4 AC R Capécitabine 2000 mg/m² J114 / 3 sem X6 N = 633 66% HR+ 69% N+ 54% > 2cm 61% > 70 ans USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. Muss et al. J Clin Oncol. 2008
 p = 0, CMF ou 4 AC. R. Capécitabine 2000 mg/m² J114. / 3 sem X6. N = % HR+ 69% N+ 54% > 2cm. 61% > 70 ans. USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. Muss et al. J Clin Oncol")
48
CALGB/CTSU 49907 > 65 ans 2 DC toxiques dans le bras Capé
2,4 fois plus d’évènements dans le bras Capé p = 0,0003 2,1 fois plus de décès dans le bras Capé p = 0,02 2 DC toxiques dans le bras Capé USO 9735 was a phase III study designed to evaluate the efficacy and safety of the Taxotere–cyclophosphamide combination. 71% of the population was ER+ and 48% were node-negative. The study was conducted prior to trastuzumab and HER2 status is not available for these patients. The goal was to compare a non-anthracycline-containing regimen with a standard anthracycline combination for the treatment of patients with operable breast cancer. Muss et al. J Clin Oncol. 2008

49
R TAC vs FAC F 5-FU 500 mg/m2 Doxorubicine 50 mg/m2
Cyclophosphamide 500 mg/m2 R Toutes les 3 semaines x 6 cycles T A C Docetaxel 75 mg/m2 Doxorubicine 50 mg/m2 Cyclophosphamide 500 mg/m2 T1-T3 N0 II ou III 2cm < 35 ans HR- 1059 patientes Suivi 6 ans Martin & al ASCO 2008

50
TAC vs FAC DFS 91% TAC 86% FAC HR 0,66 ( 0,46-0,94) p = 0,202
OS 97% TAC 95% FAC 45DC 19 TAC 26 FAC Martin & al ASCO 2008

Présentations similaires





>")
 RIBBON-1 (Tax/Anthra) (n = 722)(n = 488)(n = 1 237) Non-BEVBEVNon-BEVBEV*Non-BEVBEVNon-BEVBEV SSR en.>")
>")




>")



 Biomarqueurs IHC (n = 412) Séquençage (n = 418) 200 patients évaluables pour les facteurs pronostiques cliniques et biologiques Comparaison.>")
 : schéma>")

