Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
La vessie qui prend de l’âge
Élie Antébi, MD, FRCSC Février 2013

2
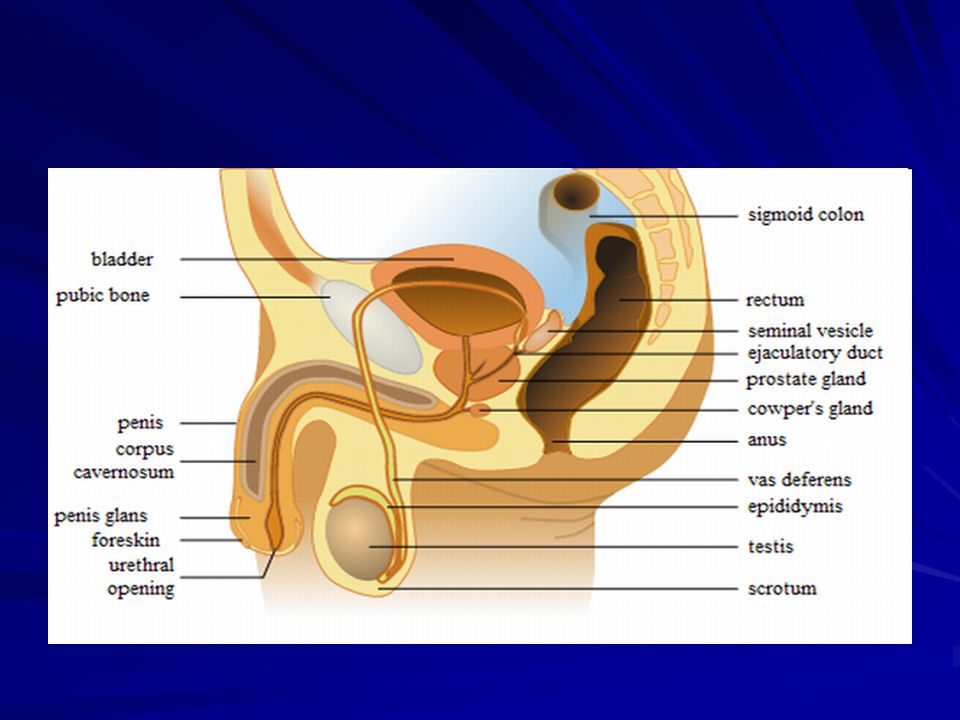
Anatomie

6
Principes de base 2 phases Fonction adéquate si Remplissage / storage
Élimination / miction Fonction adéquate si Remplissage à pression basse Continence Miction à pression basse

7
Remplissage et miction

8
Anatomie Capacité de 500 ml Forme Surfaces Vide : tétrahydrale
Remplie: ovoide Surfaces Paroi antérieure ou supérieure avec un apex à l’ouraque Paroi inféro-latérale bilatérale Paroi postéro-inférieure incluant la base Col de la vessie: point le plus caudal BladderAnatomic RelationshipsWhen filled, the bladder has a capacity of approximately 500 mL and assumes an ovoid shape. The empty bladder is tetrahedral and is described as having a superior surface with an apex at the urachus, two inferolateral surfaces, and a posteroinferior surface or base with the bladder neck at the lowest point (see Fig. 2-23).The urachus anchors the bladder to the anterior abdominal wall (see Fig. 2-8). There is a relative paucity of bladder wall muscle at the point of attachment of the urachus, predisposing to formation of diverticula. The urachus is composed of longitudinal smooth muscle bundles derived from the bladder wall. Near the umbilicus, it becomes more fibrous and usually fuses with one of the obliterated umbilical arteries. Urachal vessels run longitudinally, and the ends of the urachus must be ligated when it is divided. An epithelium-lined lumen usually persists throughout life and uncommonly gives rise to aggressive urachal adenocarcinomas (Begg, 1930). In rare instances, luminal continuity with the bladder serves as a bacterial reservoir or results in an umbilical urinary fistula.The superior surface of the bladder is covered by peritoneum. Anteriorly, the peritoneum sweeps gently onto the anterior abdominal wall (see Fig. 2-13). With distention, the bladder rises out of the true pelvis and separates the peritoneum from the anterior abdominal wall. It is therefore possible to perform a suprapubic cystostomy without risking entry into the peritoneal cavity. Posteriorly, the peritoneum passes to the level of the seminal vesicles and meets the peritoneum on the anterior rectum to form the rectovesical space.Anteroinferiorly and laterally, the bladder is cushioned from the pelvic side wall by retropubic and perivesical fat and loose connective tissue. This potential space (of Retzius) may be entered anteriorly by dividing the transversalis fascia and provides access to the pelvic viscera as far posteriorly as the iliac vessels and ureters (see Fig. 2-11). The bladder base is related to the seminal vesicles, ampullae of the vas deferentia, and terminal ureter. The bladder neck, located at the internal urethral meatus, rests 3 to 4 cm behind the midpoint of the symphysis pubis. It is firmly fixed by the pelvic fasciae (see earlier discussion) and by its continuity with the prostate; its position changes little with varying conditions of the bladder and rectum.In the female, the peritoneum on the superior surface of the bladder is reflected over the uterus to form the vesicouterine pouch and then continues posteriorly over the uterus as the rectouterine pouch (see Fig. 2-13). The vagina and uterus intervene between the bladder and the rectum, so that the base of the bladder and urethra rest on the anterior vaginal wall. Because the anterior vaginal wall is firmly attached laterally to the levator ani, contraction of the pelvic diaphragm (e.g., during increases in intra-abdominal pressure) elevates the bladder neck and draws it anteriorly. In many women with stress incontinence, the bladder neck drops below the pubic symphysis. In infants, the true pelvis is shallow and the bladder neck is level with the upper border of the symphysis. The bladder is a true intra-abdominal organ that can project above the umbilicus when full. By puberty, the bladder has migrated to the confines of the deepened true pelvis.
.The urachus anchors the bladder to the anterior abdominal wall (see Fig. 2-8). There is a relative paucity of bladder wall muscle at the point of attachment of the urachus, predisposing to formation of diverticula. The urachus is composed of longitudinal smooth muscle bundles derived from the bladder wall. Near the umbilicus, it becomes more fibrous and usually fuses with one of the obliterated umbilical arteries. Urachal vessels run longitudinally, and the ends of the urachus must be ligated when it is divided. An epithelium-lined lumen usually persists throughout life and uncommonly gives rise to aggressive urachal adenocarcinomas (Begg, 1930). In rare instances, luminal continuity with the bladder serves as a bacterial reservoir or results in an umbilical urinary fistula.The superior surface of the bladder is covered by peritoneum. Anteriorly, the peritoneum sweeps gently onto the anterior abdominal wall (see Fig. 2-13). With distention, the bladder rises out of the true pelvis and separates the peritoneum from the anterior abdominal wall. It is therefore possible to perform a suprapubic cystostomy without risking entry into the peritoneal cavity. Posteriorly, the peritoneum passes to the level of the seminal vesicles and meets the peritoneum on the anterior rectum to form the rectovesical space.Anteroinferiorly and laterally, the bladder is cushioned from the pelvic side wall by retropubic and perivesical fat and loose connective tissue. This potential space (of Retzius) may be entered anteriorly by dividing the transversalis fascia and provides access to the pelvic viscera as far posteriorly as the iliac vessels and ureters (see Fig. 2-11). The bladder base is related to the seminal vesicles, ampullae of the vas deferentia, and terminal ureter. The bladder neck, located at the internal urethral meatus, rests 3 to 4 cm behind the midpoint of the symphysis pubis. It is firmly fixed by the pelvic fasciae (see earlier discussion) and by its continuity with the prostate; its position changes little with varying conditions of the bladder and rectum.In the female, the peritoneum on the superior surface of the bladder is reflected over the uterus to form the vesicouterine pouch and then continues posteriorly over the uterus as the rectouterine pouch (see Fig. 2-13). The vagina and uterus intervene between the bladder and the rectum, so that the base of the bladder and urethra rest on the anterior vaginal wall. Because the anterior vaginal wall is firmly attached laterally to the levator ani, contraction of the pelvic diaphragm (e.g., during increases in intra-abdominal pressure) elevates the bladder neck and draws it anteriorly. In many women with stress incontinence, the bladder neck drops below the pubic symphysis. In infants, the true pelvis is shallow and the bladder neck is level with the upper border of the symphysis. The bladder is a true intra-abdominal organ that can project above the umbilicus when full. By puberty, the bladder has migrated to the confines of the deepened true pelvis.")
9
Anatomie Jonction urétéro-vésicale
Couche fibromusculaire de Waldeyer : 2-3 cm de la vessie Épaississement musculaire entre les orifices Barre interurétérique de Mercier Trajet intramural de cm Trajet intravésical sous l’urothélium Ureterovesical Junction and the Trigonepage 58 page 59Add to lightbox Figure 2-25 Structure of the male bladder neck and trigone. A, Anterior view reveals that the trigone narrows below the ureteral orifices and then widens at the bladder neck to become continuous with the anterior fibromuscular stroma of the prostate. B, Lateral projection shows that the trigone and anterior fibromuscular stroma are in continuity. The trigone thickens near the bladder neck as it meets the anterior fibromuscular stroma. C, Oblique view shows this structure at the bladder neck, where it forms the internal urethral sphincter. (From Brooks JD, Chao W-M, Kerr J: Male pelvic anatomy reconstructed from the Visible Human data set. J Urol 1998;159: )As the ureter approaches the bladder, its spirally oriented mural smooth muscle fibers become longitudinal. Two to 3 cm from the bladder, a fibromuscular sheath (of Waldeyer) extends longitudinally over the ureter and follows it to the trigone (Tanagho, 1992). The ureter pierces the bladder wall obliquely, travels 1.5 to 2 cm, and terminates at the ureteral orifice (Fig. 2-26). As it passes through a hiatus in the detrusor (intramural ureter), it is compressed and narrows considerably. This is a common site in which ureteral stones become impacted. The intravesical portion of the ureter lies immediately beneath the bladder urothelium and therefore is quite pliant; it is backed by a strong plate of detrusor muscle. With bladder filling, this arrangement is thought to result in passive occlusion of the ureter, like a flap valve. Indeed, reflux does not occur in fresh cadavers when the bladder is filled (Thomson et al, 1994). Vesicoureteral reflux is thought to result from insufficient submucosal ureteral length and poor detrusor backing. Chronic increases in intravesical pressure resulting from bladder outlet obstruction can cause herniation of the bladder mucosa through the weakest point of the hiatus above the ureter and produce a "Hutch diverticulum" and reflux (Hutch et al, 1961).The triangle of smooth urothelium between the two ureteral orifices and the internal urethral meatus is referred to as thetrigone of the bladder (see Fig. 2-26). The fine longitudinal smooth muscle fibers from the vesical side of the ureters pass to either side of their respective orifices to join the lateral and posterior ureteral wall fibers and fan out over the base of the bladder. Fibers from each ureter meet to form a triangular sheet of muscle that extends from the two ureteral orifices to the internal urethral meatus. The edges of this muscular sheet are thickened between the ureteral orifices (the interureteric crest or Mercier's bar) and between the ureters and the internal urethral meatus (Bell's muscle).page 59 page 60Add to lightbox Figure 2-26 Normal ureterovesical junction and trigone. A, Section of the bladder wall perpendicular to the ureteral hiatus shows the oblique passage of the ureter through the detrusor and also shows the submucosal ureter with its detrusor backing. Waldeyer's sheath surrounds the prevesical ureter and extends inward to become the deep trigone. B, Waldeyer's sheath continues in the bladder as the deep trigone, which is fixed at the bladder neck. Smooth muscle of the ureter forms the superficial trigone and is anchored at the verumontanum. (From Tanagho EA, Pugh RC: The anatomy and function of the ureterovesical junction. Br J Urol 1963;35: )The muscle of trigone forms three distinct layers: (1) a superficial layer, derived from the longitudinal muscle of the ureter, which extends down the urethra to insert at the verumontanum; (2) a deep layer, which continues from Waldeyer's sheath and inserts at the bladder neck; and (3) a detrusor layer, formed by the outer longitudinal and middle circular smooth muscle layers of the bladder wall. Through its continuity with the ureter, the superficial trigonal muscle anchors the ureter to the bladder. During ureteral reimplantation, this muscle is tented up and divided to gain access to the space between Waldeyer's sheath and the ureter. In this space, only loose fibrous and muscular connections are found. This anatomic arrangement helps prevent reflux during bladder filling by fixing and applying tension to the ureteral orifice. As the bladder fills, its lateral wall telescopes outward on the ureter, thereby increasing intravesical ureteral length (Hutch et al, 1961).The urothelium overlying the muscular trigone is usually only three cells thick and adheres strongly to the underlying muscle by a dense lamina propria. During filling and emptying of the bladder, this mucosal surface remains smooth.
As the ureter approaches the bladder, its spirally oriented mural smooth muscle fibers become longitudinal. Two to 3 cm from the bladder, a fibromuscular sheath (of Waldeyer) extends longitudinally over the ureter and follows it to the trigone (Tanagho, 1992). The ureter pierces the bladder wall obliquely, travels 1.5 to 2 cm, and terminates at the ureteral orifice (Fig. 2-26). As it passes through a hiatus in the detrusor (intramural ureter), it is compressed and narrows considerably. This is a common site in which ureteral stones become impacted. The intravesical portion of the ureter lies immediately beneath the bladder urothelium and therefore is quite pliant; it is backed by a strong plate of detrusor muscle. With bladder filling, this arrangement is thought to result in passive occlusion of the ureter, like a flap valve. Indeed, reflux does not occur in fresh cadavers when the bladder is filled (Thomson et al, 1994). Vesicoureteral reflux is thought to result from insufficient submucosal ureteral length and poor detrusor backing. Chronic increases in intravesical pressure resulting from bladder outlet obstruction can cause herniation of the bladder mucosa through the weakest point of the hiatus above the ureter and produce a Hutch diverticulum and reflux (Hutch et al, 1961).The triangle of smooth urothelium between the two ureteral orifices and the internal urethral meatus is referred to as thetrigone of the bladder (see Fig. 2-26). The fine longitudinal smooth muscle fibers from the vesical side of the ureters pass to either side of their respective orifices to join the lateral and posterior ureteral wall fibers and fan out over the base of the bladder. Fibers from each ureter meet to form a triangular sheet of muscle that extends from the two ureteral orifices to the internal urethral meatus. The edges of this muscular sheet are thickened between the ureteral orifices (the interureteric crest or Mercier s bar) and between the ureters and the internal urethral meatus (Bell s muscle).page 59 page 60Add to lightbox Figure 2-26 Normal ureterovesical junction and trigone. A, Section of the bladder wall perpendicular to the ureteral hiatus shows the oblique passage of the ureter through the detrusor and also shows the submucosal ureter with its detrusor backing. Waldeyer s sheath surrounds the prevesical ureter and extends inward to become the deep trigone. B, Waldeyer s sheath continues in the bladder as the deep trigone, which is fixed at the bladder neck. Smooth muscle of the ureter forms the superficial trigone and is anchored at the verumontanum. (From Tanagho EA, Pugh RC: The anatomy and function of the ureterovesical junction. Br J Urol 1963;35: )The muscle of trigone forms three distinct layers: (1) a superficial layer, derived from the longitudinal muscle of the ureter, which extends down the urethra to insert at the verumontanum; (2) a deep layer, which continues from Waldeyer s sheath and inserts at the bladder neck; and (3) a detrusor layer, formed by the outer longitudinal and middle circular smooth muscle layers of the bladder wall. Through its continuity with the ureter, the superficial trigonal muscle anchors the ureter to the bladder. During ureteral reimplantation, this muscle is tented up and divided to gain access to the space between Waldeyer s sheath and the ureter. In this space, only loose fibrous and muscular connections are found. This anatomic arrangement helps prevent reflux during bladder filling by fixing and applying tension to the ureteral orifice. As the bladder fills, its lateral wall telescopes outward on the ureter, thereby increasing intravesical ureteral length (Hutch et al, 1961).The urothelium overlying the muscular trigone is usually only three cells thick and adheres strongly to the underlying muscle by a dense lamina propria. During filling and emptying of the bladder, this mucosal surface remains smooth.")
10
Anatomie Col de la vessie Hommes Femmes
Couche longitudinale interne continue avec l’urètre Couche circulaire au milieu Sphincter circulaire pré-prostatique Couche longitudinale externe Épaisse en postérieur Insertion dans le trigone médian (apex du trigone) Mélange avec muscle lisse prostatique Passage latéral et antérieur pour faire un loop autour du col Innervation sympathiqe importante Femmes Couche circulaire au milieu ? Loop antérieur de la couche longitudinale externe Peu ou pas d’innervation sympathique
 Mélange avec muscle lisse prostatique. Passage latéral et antérieur pour faire un loop autour du col. Innervation sympathiqe importante. Femmes. Couche circulaire au milieu Loop antérieur de la couche longitudinale externe. Peu ou pas d’innervation sympathique.")
11
Urètre Muscle lisse - couches évidentes Rhabdosphincter: fer à cheval
Longitudinale interne et circulaire externe Rhabdosphincter: fer à cheval Homme: base de la vessie Aspect antérieur de la prostate Urètre membraneux Innervation sympatique et α-adrénergique Femme: compressor urethrae + sphincter uretrovaginal Muscle strié qui s’étend de proximal en distal Mécanismes de continence Contrôle neurologique actif (contraction avant toux) Transmission de pression abdominale a/n de l’urètre proximal Hammock hypothesis Ligaments pubourétraux et muscle pubourétralis (lvator ani) - complexe mid-urétral Compression de l’urètre contre le pubis lors de continence Sphincter uretral externe: plancher pelvien Innervation volontaire THE URETHRAThe urethra is composed of striated and smooth muscles. Contraction of the longitudinal smooth muscle could play a role in stabilizing the urethra and allowing force generated by the circular muscle elements to occlude the lumen or in aiding in the opening of the bladder neck during micturition. There is controversy about the relative roles of the urethral smooth and striated circular muscles and the lamina propria in generating the urethral pressure profile, but it seems likely that both contribute (Thind, 1995). Blocking striated sphincter activity with nicotinic neuromuscular blocking agents has variable effects and may reduce urethral tone, but rarely by more than 40%, suggesting that the smooth muscles are important. Blocking sympathetic tone with α-adrenoceptor blockers may also reduce urethral pressure by about a third (Torrens, 1987). There is little evidence for the involvement of the cholinergic innervation in generating urethral pressure.Urethral MuscleThe smooth muscle cells in the urethra are gathered into small bundles and linked to each other by many adherens-type junctions but no gap junctions. The smooth muscle bundles in the urethral wall are thinner than in the detrusor and arranged in obvious layers. In humans and larger mammals, there is a relatively thick inner layer that is predominantly longitudinally arranged, and outside this, there is a thinner circular muscle layer. In the lamina propria of the urethra, scattered small bundles of only a few cells are often found.Striated muscle occurs in the walls of the male and female urethra, where it forms a rhabdosphincter that is separate from the periurethral skeletal muscle of the pelvic floor. In the male, the striated muscle extends from the base of the bladder and the anterior aspect of the prostate to the full length of the membranous urethra. In the female, the striated muscle extends from the proximal urethra distally. The striated sphincter is horseshoe shaped, and the muscle cells are smaller than ordinary skeletal muscle, being 15 to 20 μm in diameter.MorphologyThe urethral stroma has been less extensively studied than the bladder stroma, but it is known to contain primarily longitudinally arranged collagen fibers and elastin fibers (Hickey et al, 1982; Huisman, 1983). The vascular filling of the urethral lamina propria is known to be of importance for urinary continence, although the magnitude of its contribution to continence is still not understood (Rud et al, 1980). Estrogen is known to increase the urethral blood flow, resulting in an increased distention of the lamina propria blood vessels (Brading, 1997).Impaired arterial blood supply to the urethra decreases the intraluminal pressure (Rud et al, 1980), but at present, it is not known whether it is the decrease in vascular filling or the urethral hypoxia that mediates the decrease in urethral pressure. It has been suggested that both these mechanisms may be involved because it was shown that the initial drop in urethral pressure was mediated through decreased vascular filling, whereas the later phase was due to a hypoxic effect on the urethral smooth muscle (Greenland and Brading, 1996).Sphincter ConfigurationAn issue of continuing confusion for urologists is what composes the external sphincter and what the distinction is between the rhabdosphincter and the external striated sphincter proper. In the membranous urethra, a thin smooth muscle layer extends along the entire urethra in the female and throughout the prostate and its capsule in the male (Tanagho, 1982; Dixon and Gosling, 1987). On the anterior surface of the male urethra, an outer layer of circularly oriented striated muscle forms a horseshoe configuration in the adult near the prostatic apex. This striated muscle develops as a complete ring in the fetus and neonate and forms the external urethral sphincter or rhabdosphincter. The periurethral striated muscles of the pelvic floor lie external to the rhabdosphincter (see Fig. 56-2).Despite the horseshoe configuration, urethral pressure recording at the external sphincter during bladder filling increases uniformly along the entire circumference like an iris (Morita and Tsuchida, 1989). Norepinephrine or hypogastric nerve stimulation augments this pressure, suggesting a role for adrenergic receptors and sympathetic nerves in the function of the external urethral sphincter (Kakizaki et al, 1991).page 1935 page 1936The arrangement of muscle forming the distal sphincter of the female differs from that in the male. The female has an attenuated striated sphincter mechanism as well as additional muscle structures termed the compressor urethrae and urethrovaginal sphincter (DeLancey, 1989). The posterior wall remains rigid if there is adequate pelvic support from muscle and connective tissues. As in the male, the striated components are deficient posteriorly. This relative deficiency of periurethral striated musculature contributes to the difficulty in obtaining reliable external sphincter electromyography results during urodynamic studies in women. This attenuation of distal sphincteric muscles may contribute to urinary incontinence in females after resection of the bladder neck.In women, urinary continence is maintained during elevations in intra-abdominal pressure by three processes. First, there is passive transmission of abdominal pressure to the proximal urethra. A guarding reflex involving an active contraction of striated muscle of the external urethral sphincter can transiently help continence (Enhorning, 1961; Tanagho, 1982). However, mere transmission of abdominal pressure to proximal urethra does not account for the entire increase in urethral pressure (Constantinou and Govan, 1982). Urethral pressure rises before cough transmission (Fig ). These findings implicate an active urethral continence (neural) mechanism in women (Constantinou and Govan, 1982). DeLancey proposes the "hammock hypothesis" that abdominal pressure transmitted through the proximal urethra presses the anterior wall against the posterior wall. The posterior wall remains rigid if there is adequate pelvic support from muscle and connective tissues. More distally, based on morphologic data, DeLancey and colleagues (DeLancey, 1989, 1997; Sampselle and DeLancey, 1998) have postulated that the urethral attachments to the pubis (pubourethral) and vaginal connections to pelvic muscles and fascia actively change the position of the bladder neck and proximal urethra with voiding. This arrangement compresses the urethra against the pubis during bladder filling and straining. These attachments contain both fascia and smooth muscle (Oerlich, 1983; DeLancey, 1988, 1989). Thus, urinary continence results from the combination of active muscle tone and passive anatomic coaptation.
 Transmission de pression abdominale a/n de l’urètre proximal. Hammock hypothesis. Ligaments pubourétraux et muscle pubourétralis (lvator ani) - complexe mid-urétral. Compression de l’urètre contre le pubis lors de continence. Sphincter uretral externe: plancher pelvien. Innervation volontaire. THE URETHRAThe urethra is composed of striated and smooth muscles. Contraction of the longitudinal smooth muscle could play a role in stabilizing the urethra and allowing force generated by the circular muscle elements to occlude the lumen or in aiding in the opening of the bladder neck during micturition. There is controversy about the relative roles of the urethral smooth and striated circular muscles and the lamina propria in generating the urethral pressure profile, but it seems likely that both contribute (Thind, 1995). Blocking striated sphincter activity with nicotinic neuromuscular blocking agents has variable effects and may reduce urethral tone, but rarely by more than 40%, suggesting that the smooth muscles are important. Blocking sympathetic tone with α-adrenoceptor blockers may also reduce urethral pressure by about a third (Torrens, 1987). There is little evidence for the involvement of the cholinergic innervation in generating urethral pressure.Urethral MuscleThe smooth muscle cells in the urethra are gathered into small bundles and linked to each other by many adherens-type junctions but no gap junctions. The smooth muscle bundles in the urethral wall are thinner than in the detrusor and arranged in obvious layers. In humans and larger mammals, there is a relatively thick inner layer that is predominantly longitudinally arranged, and outside this, there is a thinner circular muscle layer. In the lamina propria of the urethra, scattered small bundles of only a few cells are often found.Striated muscle occurs in the walls of the male and female urethra, where it forms a rhabdosphincter that is separate from the periurethral skeletal muscle of the pelvic floor. In the male, the striated muscle extends from the base of the bladder and the anterior aspect of the prostate to the full length of the membranous urethra. In the female, the striated muscle extends from the proximal urethra distally. The striated sphincter is horseshoe shaped, and the muscle cells are smaller than ordinary skeletal muscle, being 15 to 20 μm in diameter.MorphologyThe urethral stroma has been less extensively studied than the bladder stroma, but it is known to contain primarily longitudinally arranged collagen fibers and elastin fibers (Hickey et al, 1982; Huisman, 1983). The vascular filling of the urethral lamina propria is known to be of importance for urinary continence, although the magnitude of its contribution to continence is still not understood (Rud et al, 1980). Estrogen is known to increase the urethral blood flow, resulting in an increased distention of the lamina propria blood vessels (Brading, 1997).Impaired arterial blood supply to the urethra decreases the intraluminal pressure (Rud et al, 1980), but at present, it is not known whether it is the decrease in vascular filling or the urethral hypoxia that mediates the decrease in urethral pressure. It has been suggested that both these mechanisms may be involved because it was shown that the initial drop in urethral pressure was mediated through decreased vascular filling, whereas the later phase was due to a hypoxic effect on the urethral smooth muscle (Greenland and Brading, 1996).Sphincter ConfigurationAn issue of continuing confusion for urologists is what composes the external sphincter and what the distinction is between the rhabdosphincter and the external striated sphincter proper. In the membranous urethra, a thin smooth muscle layer extends along the entire urethra in the female and throughout the prostate and its capsule in the male (Tanagho, 1982; Dixon and Gosling, 1987). On the anterior surface of the male urethra, an outer layer of circularly oriented striated muscle forms a horseshoe configuration in the adult near the prostatic apex. This striated muscle develops as a complete ring in the fetus and neonate and forms the external urethral sphincter or rhabdosphincter. The periurethral striated muscles of the pelvic floor lie external to the rhabdosphincter (see Fig. 56-2).Despite the horseshoe configuration, urethral pressure recording at the external sphincter during bladder filling increases uniformly along the entire circumference like an iris (Morita and Tsuchida, 1989). Norepinephrine or hypogastric nerve stimulation augments this pressure, suggesting a role for adrenergic receptors and sympathetic nerves in the function of the external urethral sphincter (Kakizaki et al, 1991).page 1935 page 1936The arrangement of muscle forming the distal sphincter of the female differs from that in the male. The female has an attenuated striated sphincter mechanism as well as additional muscle structures termed the compressor urethrae and urethrovaginal sphincter (DeLancey, 1989). The posterior wall remains rigid if there is adequate pelvic support from muscle and connective tissues. As in the male, the striated components are deficient posteriorly. This relative deficiency of periurethral striated musculature contributes to the difficulty in obtaining reliable external sphincter electromyography results during urodynamic studies in women. This attenuation of distal sphincteric muscles may contribute to urinary incontinence in females after resection of the bladder neck.In women, urinary continence is maintained during elevations in intra-abdominal pressure by three processes. First, there is passive transmission of abdominal pressure to the proximal urethra. A guarding reflex involving an active contraction of striated muscle of the external urethral sphincter can transiently help continence (Enhorning, 1961; Tanagho, 1982). However, mere transmission of abdominal pressure to proximal urethra does not account for the entire increase in urethral pressure (Constantinou and Govan, 1982). Urethral pressure rises before cough transmission (Fig ). These findings implicate an active urethral continence (neural) mechanism in women (Constantinou and Govan, 1982). DeLancey proposes the hammock hypothesis that abdominal pressure transmitted through the proximal urethra presses the anterior wall against the posterior wall. The posterior wall remains rigid if there is adequate pelvic support from muscle and connective tissues. More distally, based on morphologic data, DeLancey and colleagues (DeLancey, 1989, 1997; Sampselle and DeLancey, 1998) have postulated that the urethral attachments to the pubis (pubourethral) and vaginal connections to pelvic muscles and fascia actively change the position of the bladder neck and proximal urethra with voiding. This arrangement compresses the urethra against the pubis during bladder filling and straining. These attachments contain both fascia and smooth muscle (Oerlich, 1983; DeLancey, 1988, 1989). Thus, urinary continence results from the combination of active muscle tone and passive anatomic coaptation.")
12
Croissance – évolution
Miction réflexe naissance Fréquence 1X/heure à 1 mois de vie 8-10 fois/jour à 2-3 ans Éléments de dyssynergie (pression détrusor plus élevée et miction saccadée) Contrôle volontaire vers 2-3 ans ↑ capacité vésicale Maturation du contrôle volontaire du muscle strié Maturation du contrôle volontaire sur l’unité vessie-sphincter Test eau glacée intravésicale Instillation rapide de 100 ml de NS à 40C Adulte Normal Sensation froide et contrôle maintenu Enfant moins de 4 ans ou neuropathie Contraction détrusor involontaire Developmental Changes of Bladder ReflexesThe neonatal bladder is a conduit of urine more than a storage organ. Without cerebral control, the bladder will reflexively empty into a diaper when it reaches functional capacity. Therefore, by definition, a normal toddler has detrusor overactivity. Neonatal animal bladder strips have repetitive spontaneous contraction, perhaps initiated by pacemaker cells within the bladder and propagated by gap junctions between cells (see Fig. 56-1) (Pezzone et al, 1999; Szell et al, 2003).Add to lightbox Figure The voiding reflex involves afferent neurons from the bladder that project on spinal tract neurons that ascend to the brain. Descending pathways connect to parasympathetic efferent nerves to contract the bladder (bladder-bladder reflex). A spinal bladder-urethra reflex is activated by a similar bladder afferent innervation. In cases of supraspinal dysfunction, overactive micturition reflexes occur. The sacral nerve stimulation (SNS) inhibits urinary urgency, frequency, and urge incontinence by inhibiting the bladder-bladder and bladder-urethra reflexes.The bladder overactivity neonatal pathways do not disappear with growth and development; rather, increasing cerebral maturation actively inhibits them. Inhibition rather than resolution of neonatal reflexes may be difficult to grasp initially, but this concept holds true across most concepts of neuroscience. With disease processes such as neurologic diseasesand aging, the neonatal reflexes are released and involuntary detrusor contractions recur (de Groat et al, 1975).One of the most interesting clinical demonstrations of the reemergence of the primitive neonatal micturition reflex is the bladder ice-water test. The bladder ice-water cooling test is performed by quickly instilling up to 100 mL of 4°C sterile saline solution. The normal adult will sense cold but maintain a stable bladder. However, infants and neuropathic patients will develop involuntary detrusor contractions with this test (Chancellor and de Groat, 1999).The bladder cooling response is triggered by activation of cold receptors within the bladder wall. The receptors are supplied by unmyelinated C-fiber afferent neurons (Chancellor and de Groat, 1999). The cooling response represents a neonatal reflex that may be unmasked by central neuropathologic processes, analogous to the appearance of the Babinski reflex in pyramidal tract lesions. The cooling response is present (development of involuntary detrusor contraction) in neurologically normal infants and children until about the age of 4 years. The reflex becomes absent with further maturation of the nervous system, but the response may be unmasked by pathologic processes that disturb the descending neuronal control of normal voiding (Geirsson et al, 1999). It has also been suggested that men with prostatic bladder outlet obstruction also have an ice-water test response. Chai and colleagues (1998) reported an ice-water test response in 12 of 17 patients (71%) with bladder outlet obstruction, but their method of ice-water infusion has been criticized (Geirsson et al, 1999). More recently, Hirayama and colleagues (2003) have also reported that an ice-water test response was found in 35 (27%) of 127 patients with benign prostatic hyperplasia and that the patients with the ice-water test response had detrusor overactivity and higher bladder outlet obstruction index than the nonresponders on the pressure flow study.
 Contrôle volontaire vers 2-3 ans. ↑ capacité vésicale. Maturation du contrôle volontaire du muscle strié. Maturation du contrôle volontaire sur l’unité vessie-sphincter. Test eau glacée intravésicale. Instillation rapide de 100 ml de NS à 40C. Adulte Normal. Sensation froide et contrôle maintenu. Enfant moins de 4 ans ou neuropathie. Contraction détrusor involontaire. Developmental Changes of Bladder ReflexesThe neonatal bladder is a conduit of urine more than a storage organ. Without cerebral control, the bladder will reflexively empty into a diaper when it reaches functional capacity. Therefore, by definition, a normal toddler has detrusor overactivity. Neonatal animal bladder strips have repetitive spontaneous contraction, perhaps initiated by pacemaker cells within the bladder and propagated by gap junctions between cells (see Fig. 56-1) (Pezzone et al, 1999; Szell et al, 2003).Add to lightbox Figure The voiding reflex involves afferent neurons from the bladder that project on spinal tract neurons that ascend to the brain. Descending pathways connect to parasympathetic efferent nerves to contract the bladder (bladder-bladder reflex). A spinal bladder-urethra reflex is activated by a similar bladder afferent innervation. In cases of supraspinal dysfunction, overactive micturition reflexes occur. The sacral nerve stimulation (SNS) inhibits urinary urgency, frequency, and urge incontinence by inhibiting the bladder-bladder and bladder-urethra reflexes.The bladder overactivity neonatal pathways do not disappear with growth and development; rather, increasing cerebral maturation actively inhibits them. Inhibition rather than resolution of neonatal reflexes may be difficult to grasp initially, but this concept holds true across most concepts of neuroscience. With disease processes such as neurologic diseasesand aging, the neonatal reflexes are released and involuntary detrusor contractions recur (de Groat et al, 1975).One of the most interesting clinical demonstrations of the reemergence of the primitive neonatal micturition reflex is the bladder ice-water test. The bladder ice-water cooling test is performed by quickly instilling up to 100 mL of 4°C sterile saline solution. The normal adult will sense cold but maintain a stable bladder. However, infants and neuropathic patients will develop involuntary detrusor contractions with this test (Chancellor and de Groat, 1999).The bladder cooling response is triggered by activation of cold receptors within the bladder wall. The receptors are supplied by unmyelinated C-fiber afferent neurons (Chancellor and de Groat, 1999). The cooling response represents a neonatal reflex that may be unmasked by central neuropathologic processes, analogous to the appearance of the Babinski reflex in pyramidal tract lesions. The cooling response is present (development of involuntary detrusor contraction) in neurologically normal infants and children until about the age of 4 years. The reflex becomes absent with further maturation of the nervous system, but the response may be unmasked by pathologic processes that disturb the descending neuronal control of normal voiding (Geirsson et al, 1999). It has also been suggested that men with prostatic bladder outlet obstruction also have an ice-water test response. Chai and colleagues (1998) reported an ice-water test response in 12 of 17 patients (71%) with bladder outlet obstruction, but their method of ice-water infusion has been criticized (Geirsson et al, 1999). More recently, Hirayama and colleagues (2003) have also reported that an ice-water test response was found in 35 (27%) of 127 patients with benign prostatic hyperplasia and that the patients with the ice-water test response had detrusor overactivity and higher bladder outlet obstruction index than the nonresponders on the pressure flow study.")
13
Contrôle neurologique
NEURAL CONTROL OF THE LOWER URINARY TRACTPeripheral Nervous SystemAdd to lightboxpage 1937 page 1938 Figure Diagram showing the sympathetic, parasympathetic, and somatic innervation of the urogenital tract of the male cat. Sympathetic preganglionic pathways emerge from the lumbar spinal cord and pass to the sympathetic chain ganglia (SCG) and then through the inferior splanchnic nerves (ISN) to the inferior mesenteric ganglia (IMG). Preganglionic and postganglionic sympathetic axons then travel in the hypogastric nerve (HGN) to the pelvic plexus and the urogenital organs. Parasympathetic preganglionic axons that originate in the sacral spinal cord pass in the pelvic nerve to ganglion cells in the pelvic plexus and to distal ganglia in the organs. Sacral somatic pathways are contained in the pudendal nerve, which provides an innervation to the penis and the ischiocavernosus (IC), bulbocavernosus (BC), and external urethral sphincter (EUS) muscles. The pudendal and pelvic nerves also receive postganglionic axons from the caudal sympathetic chain ganglia. These three sets of nerves contain afferent axons from the lumbosacral dorsal root ganglia. PG, prostate gland; U, ureter; VD, vas deferens.The lower urinary tract is innervated by three sets of peripheral nerves involving the parasympathetic, sympathetic, and somatic nervous systems (Fig ). Pelvicparasympathetic nerves arise at the sacral level of the spinal cord, excite the bladder, and relax the urethra. Lumbar sympathetic nerves inhibit the bladder body and excite the bladder base and urethra. Pudendal nerves excite the external urethral sphincter. These nerves contain afferent (sensory) as well as efferent axons (Wein, 1992; de Groat et al, 1993; Sugaya et al, 1997b; Yoshimura and de Groat, 1997a).Parasympathetic PathwaysParasympathetic preganglionic neurons innervating the lower urinary tract are located in the lateral part of the sacral intermediate gray matter in a region termed the sacral parasympathetic nucleus (Nadelhaft et al, 1980; Morgan et al, 1981, 1993; de Groat et al, 1993, 1996). Parasympathetic preganglionic neurons send axons through the ventral roots to peripheral ganglia, where they release the excitatory transmitter acetylcholine (de Groat and Booth, 1993). Parasympathetic postganglionic neurons in humans are located in the detrusor wall layer as well as in the pelvic plexus. This is an important fact to remember because patients with cauda equina or pelvic plexus injury are neurologically decentralized but may not be completely denervated. Cauda equina injury allows possible afferent and efferent neuron interconnection at the level of the intramural ganglia (de Groat et al, 1993, 1996).Sympathetic PathwaysSympathetic outflow from the rostral lumbar spinal cord provides a noradrenergic excitatory and inhibitory input to the bladder and urethra (Andersson, 1993). Activation of sympathetic nerves induces relaxation of the bladder body and contraction of the bladder outlet and urethra, which contribute to urine storage in the bladder. The peripheral sympathetic pathways follow a complex route that passes through the sympathetic chain ganglia to the inferior mesenteric ganglia and then through the hypogastric nerves to the pelvic ganglia (Kihara and de Groat, 1997).Somatic PathwaysThe external urethral sphincter motoneurons are located along the lateral border of the ventral horn, commonly referred to as Onuf's nucleus (Fig ) (Thor et al, 1989). Sphincter motoneurons also exhibit transversely oriented dendritic bundles that project laterally into the lateral funiculus, dorsally into the intermediate gray matter, and dorsomedially toward the central canal. Figure Diagram showing the sympathetic, parasympathetic, and somatic innervation of the urogenital tract of the male cat. Sympathetic preganglionic pathways emerge from the lumbar spinal cord and pass to the sympathetic chain ganglia (SCG) and then through the inferior splanchnic nerves (ISN) to the inferior mesenteric ganglia (IMG). Preganglionic and postganglionic sympathetic axons then travel in the hypogastric nerve (HGN) to the pelvic plexus and the urogenital organs. Parasympathetic preganglionic axons that originate in the sacral spinal cord pass in the pelvic nerve to ganglion cells in the pelvic plexus and to distal ganglia in the organs. Sacral somatic pathways are contained in the pudendal nerve, which provides an innervation to the penis and the ischiocavernosus (IC), bulbocavernosus (BC), and external urethral sphincter (EUS) muscles. The pudendal and pelvic nerves also receive postganglionic axons from the caudal sympathetic chain ganglia. These three sets of nerves contain afferent axons from the lumbosacral dorsal root ganglia. PG, prostate gland; U, ureter; VD, vas deferens
 and then through the inferior splanchnic nerves (ISN) to the inferior mesenteric ganglia (IMG). Preganglionic and postganglionic sympathetic axons then travel in the hypogastric nerve (HGN) to the pelvic plexus and the urogenital organs. Parasympathetic preganglionic axons that originate in the sacral spinal cord pass in the pelvic nerve to ganglion cells in the pelvic plexus and to distal ganglia in the organs. Sacral somatic pathways are contained in the pudendal nerve, which provides an innervation to the penis and the ischiocavernosus (IC), bulbocavernosus (BC), and external urethral sphincter (EUS) muscles. The pudendal and pelvic nerves also receive postganglionic axons from the caudal sympathetic chain ganglia. These three sets of nerves contain afferent axons from the lumbosacral dorsal root ganglia. PG, prostate gland; U, ureter; VD, vas deferens.The lower urinary tract is innervated by three sets of peripheral nerves involving the parasympathetic, sympathetic, and somatic nervous systems (Fig ). Pelvicparasympathetic nerves arise at the sacral level of the spinal cord, excite the bladder, and relax the urethra. Lumbar sympathetic nerves inhibit the bladder body and excite the bladder base and urethra. Pudendal nerves excite the external urethral sphincter. These nerves contain afferent (sensory) as well as efferent axons (Wein, 1992; de Groat et al, 1993; Sugaya et al, 1997b; Yoshimura and de Groat, 1997a).Parasympathetic PathwaysParasympathetic preganglionic neurons innervating the lower urinary tract are located in the lateral part of the sacral intermediate gray matter in a region termed the sacral parasympathetic nucleus (Nadelhaft et al, 1980; Morgan et al, 1981, 1993; de Groat et al, 1993, 1996). Parasympathetic preganglionic neurons send axons through the ventral roots to peripheral ganglia, where they release the excitatory transmitter acetylcholine (de Groat and Booth, 1993). Parasympathetic postganglionic neurons in humans are located in the detrusor wall layer as well as in the pelvic plexus. This is an important fact to remember because patients with cauda equina or pelvic plexus injury are neurologically decentralized but may not be completely denervated. Cauda equina injury allows possible afferent and efferent neuron interconnection at the level of the intramural ganglia (de Groat et al, 1993, 1996).Sympathetic PathwaysSympathetic outflow from the rostral lumbar spinal cord provides a noradrenergic excitatory and inhibitory input to the bladder and urethra (Andersson, 1993). Activation of sympathetic nerves induces relaxation of the bladder body and contraction of the bladder outlet and urethra, which contribute to urine storage in the bladder. The peripheral sympathetic pathways follow a complex route that passes through the sympathetic chain ganglia to the inferior mesenteric ganglia and then through the hypogastric nerves to the pelvic ganglia (Kihara and de Groat, 1997).Somatic PathwaysThe external urethral sphincter motoneurons are located along the lateral border of the ventral horn, commonly referred to as Onuf s nucleus (Fig ) (Thor et al, 1989). Sphincter motoneurons also exhibit transversely oriented dendritic bundles that project laterally into the lateral funiculus, dorsally into the intermediate gray matter, and dorsomedially toward the central canal. Figure Diagram showing the sympathetic, parasympathetic, and somatic innervation of the urogenital tract of the male cat. Sympathetic preganglionic pathways emerge from the lumbar spinal cord and pass to the sympathetic chain ganglia (SCG) and then through the inferior splanchnic nerves (ISN) to the inferior mesenteric ganglia (IMG). Preganglionic and postganglionic sympathetic axons then travel in the hypogastric nerve (HGN) to the pelvic plexus and the urogenital organs. Parasympathetic preganglionic axons that originate in the sacral spinal cord pass in the pelvic nerve to ganglion cells in the pelvic plexus and to distal ganglia in the organs. Sacral somatic pathways are contained in the pudendal nerve, which provides an innervation to the penis and the ischiocavernosus (IC), bulbocavernosus (BC), and external urethral sphincter (EUS) muscles. The pudendal and pelvic nerves also receive postganglionic axons from the caudal sympathetic chain ganglia. These three sets of nerves contain afferent axons from the lumbosacral dorsal root ganglia. PG, prostate gland; U, ureter; VD, vas deferens.")
14
Principes de base 2 phases Fonction adéquate si Remplissage / storage
Élimination / miction Fonction adéquate si Remplissage à basse pression Continence Miction à basse pression

15
Remplissage et miction

16
Miction volontaire Distension vésicale et ↑ pression intravésicale
Afférence via nerfs pelviens parasympathiques Coordination aux centres supérieurs Protubérance et cortex cérébral Efférence dans l’ordre Relâchement du sphincter lisse et strié - sympathique et NO Funneling de l’urètre qui diminue la résistance Contraction du détrusor - parasympathique

17
Failure to store Vessie Outlet Hyperactivité vésicale
CNI ou ↓ compliance Causes: Maladies neuro, inflammation, obstruction, veillissement, idiopathique Hypersensibilité vésicale Cystite interstitielle Outlet ↓ résistance du sphincter Incontinence de stress primaire (hypermobilité urétrale) Faiblesse du plancher pelvien Déficience intrinsèque du sphincter Causes: maladies neuro, trauma ou chirurgie
 Faiblesse du plancher pelvien. Déficience intrinsèque du sphincter. Causes: maladies neuro, trauma ou chirurgie.")
18
Failure to store Vessie Outlet Hyperactivité vésicale
CNI ou ↓ compliance Causes: Maladies neuro, inflammation, obstruction, veillissement, idiopathique Hypersensibilité vésicale Cystite interstitielle Outlet ↓ résistance du sphincter Incontinence de stress primaire (hypermobilité urétrale) Faiblesse du plancher pelvien Déficience intrinsèque du sphincter Causes: maladies neuro, trauma ou chirurgie
 Faiblesse du plancher pelvien. Déficience intrinsèque du sphincter. Causes: maladies neuro, trauma ou chirurgie.")
19
Failure to empty Vessie Outlet ↓ contraction vésicale Hyperactivité
Neurologique Surdistension, médicaments, fibrose, infection sévère Outlet Hyperactivité Dyssynergie vésico-sphinctérienne Obstruction

20
Vessie Changements avec l’age Relié au gendre
Contraction musculaire vésicale et sphinctérienne Capacité Se retenir Pression urétrale Relié au gendre Hommes Femmes bladder contractility, capacity, and the ability to postpone voiding decline in both sexes, whereas urethral length and maximum closure pressure—as well as striated muscle cells in the rhabdosphincter—probably decline with age in women prostate enlarges in most men and appears to cause urodynamic obstruction in half involuntary detrusor contractions increases whereas the postvoid residual (PVR) probably increases to no more than 50 to 100 ml elderly often excrete most of their fluid intake at night
 probably increases to no more than 50 to 100 ml. elderly often excrete most of their fluid intake at night.")
21
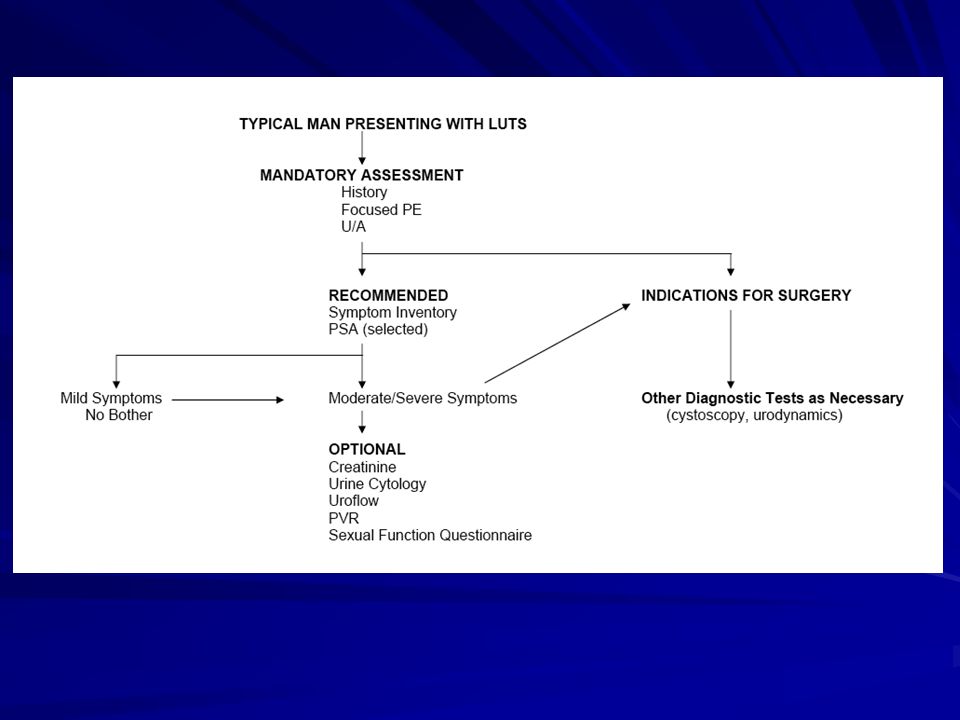
BPH - symptoms Pathological diagnosis
Refered to as LUTS in clinical practice Lower urinary tract symptoms Symptomes du bas appareilurinaire Irritatifs Obstructifs Symptom inventory

23
Nocturia Causes of polyuria High fluid intake
Untreated diabetes (Type 1 and Type 2) Diabetes insipidus, gestational diabetes (occurs during pregnancy) Causes of nocturnal polyuria Congestive heart failure Edema of lower extremities (swelling of the legs) Sleeping disorders such as obstructive sleep apnea Certain drugs, including diuretics (water pills), cardiac glycosides, demeclocycline, lithium, methoxyflurane, phenytoin, propoxyphene, and excessive vitamin D Drinking too much fluid before bedtime, especially coffee, caffeinated beverages, or alcohol
 Diabetes insipidus, gestational diabetes (occurs during pregnancy) Causes of nocturnal polyuria. Congestive heart failure. Edema of lower extremities (swelling of the legs) Sleeping disorders such as obstructive sleep apnea. Certain drugs, including diuretics (water pills), cardiac glycosides, demeclocycline, lithium, methoxyflurane, phenytoin, propoxyphene, and excessive vitamin D. Drinking too much fluid before bedtime, especially coffee, caffeinated beverages, or alcohol.")
24
Nocturia Causes of low nocturnal bladder capacity
Bladder obstruction Bladder overactivity Bladder infection or recurrent urinary tract infection Bladder inflammation (swelling) Interstitial cystitis (pain in the bladder) Bladder malignancy Benign prostatic hyperplasia Possible causes of mixed nocturia Any of the possible causes listed under nocturnal polyuria and low nocturnal bladder capacity
 Interstitial cystitis (pain in the bladder) Bladder malignancy. Benign prostatic hyperplasia. Possible causes of mixed nocturia. Any of the possible causes listed under nocturnal polyuria and low nocturnal bladder capacity.")
26
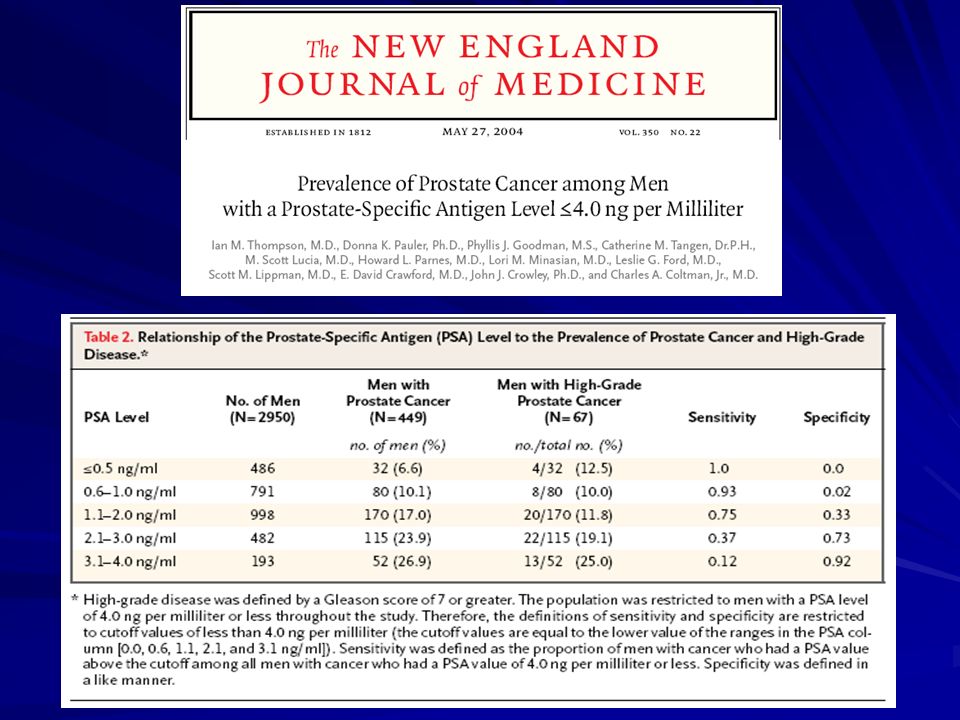
Interpreting PSA results in prostate cancer screening
Elie Antebi MD FRCSC General Urology and Urologic Oncology Urologie de la Rive-Sud de Montréal

27
PSA hK3 (APS) Serine protease Ectopicsecretion
Breast tissue (bénign or malignant) Breastmilk Renal and adrenalCarcinoma Produced by prostate epithelialcells
 Breastmilk. Renal and adrenalCarcinoma. Produced by prostate epithelialcells.")
28
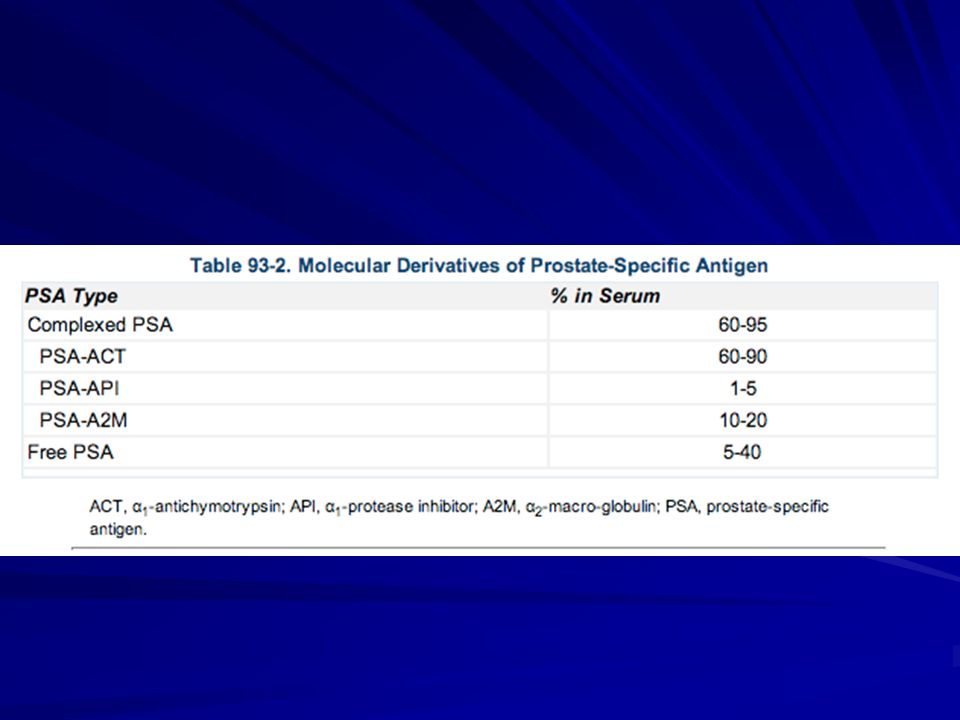
PSA Function=liquefysemen Protein-bound in the serum
Anti-protéases ACT, and macroglobulin (MG) Free PSA Detectable in lab tests
 Free PSA. Detectable in lab tests.")
31
PSA Variations according to Prostate diseases Prostatic manipulations
Massage/ Biopsy / TUR Age Race Prostate volume Intercourse

32
PSA Prostate diseases BPH Prostatitis Prostate cancer

33
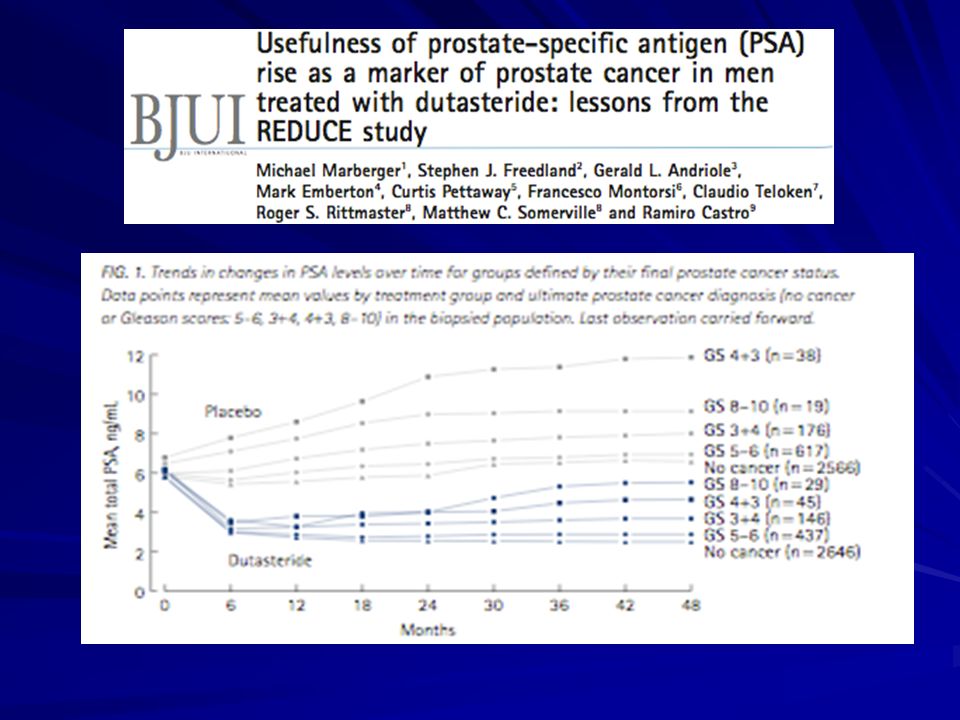
Variations of PSA Without BPH With BPH 5-alpha reductase inhibitor
Variation de 0.04 ng/ml par année With BPH Variation de 0.07 – 0.27 ng/ml par année 5-alpha reductase inhibitor ↓ PSA of 50% in 6 months Finasteride 1 ou 5 mg die Dutasteride 0.5 mg die

34
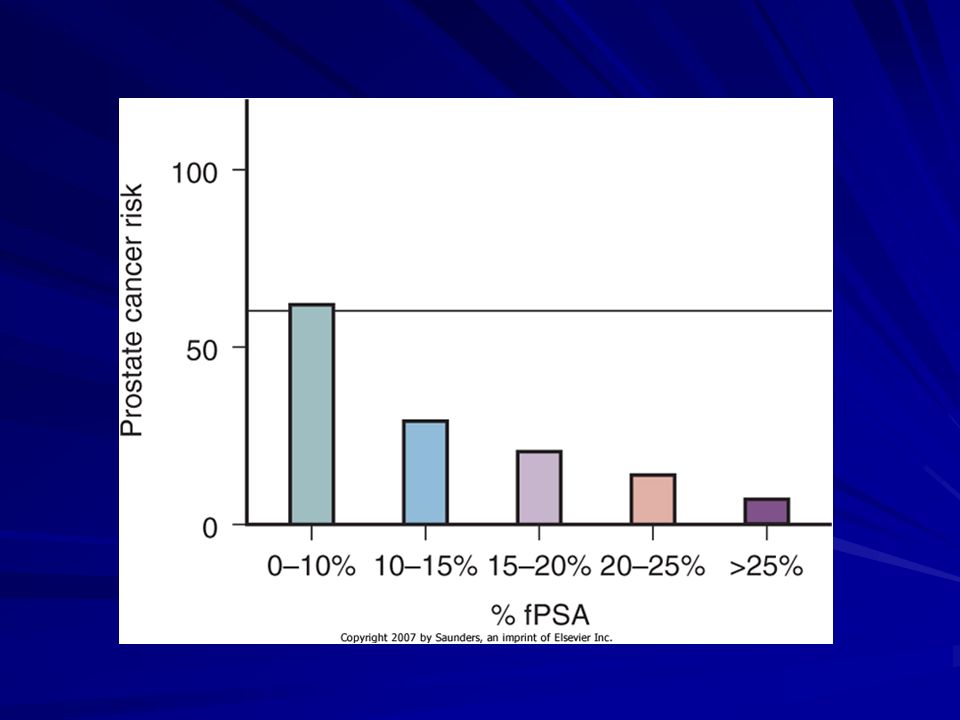
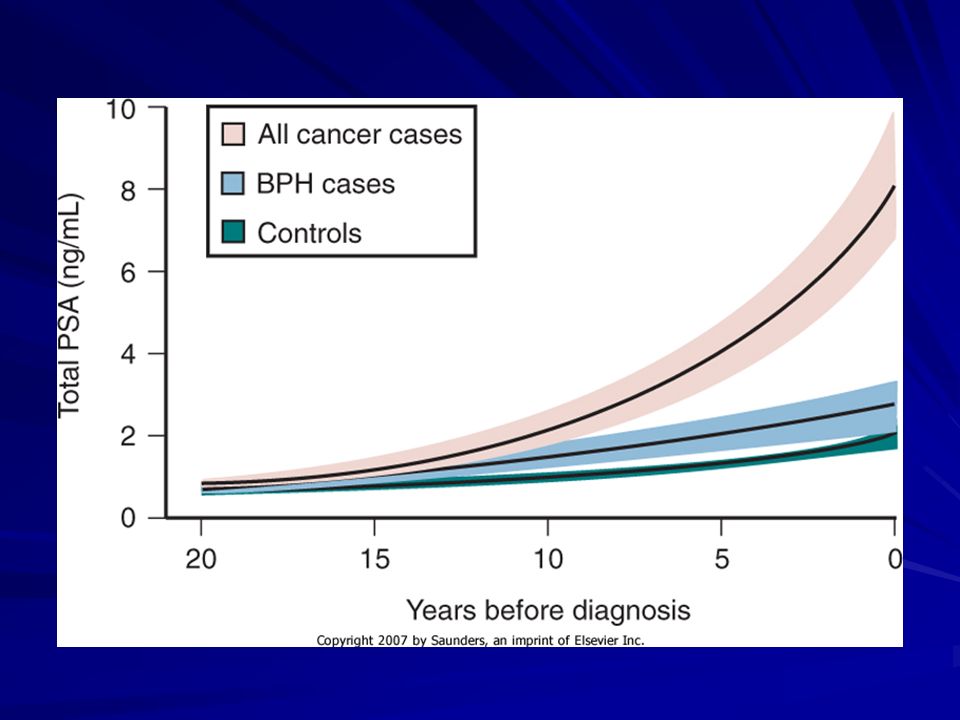
Variations of PSA Prostatitis Prostate cancer Rapid increase in PSA
Prostate cancer cells do not produce PSA Destabilization of the prostate histologic architecture and prostate cancer progression / inflammation

35
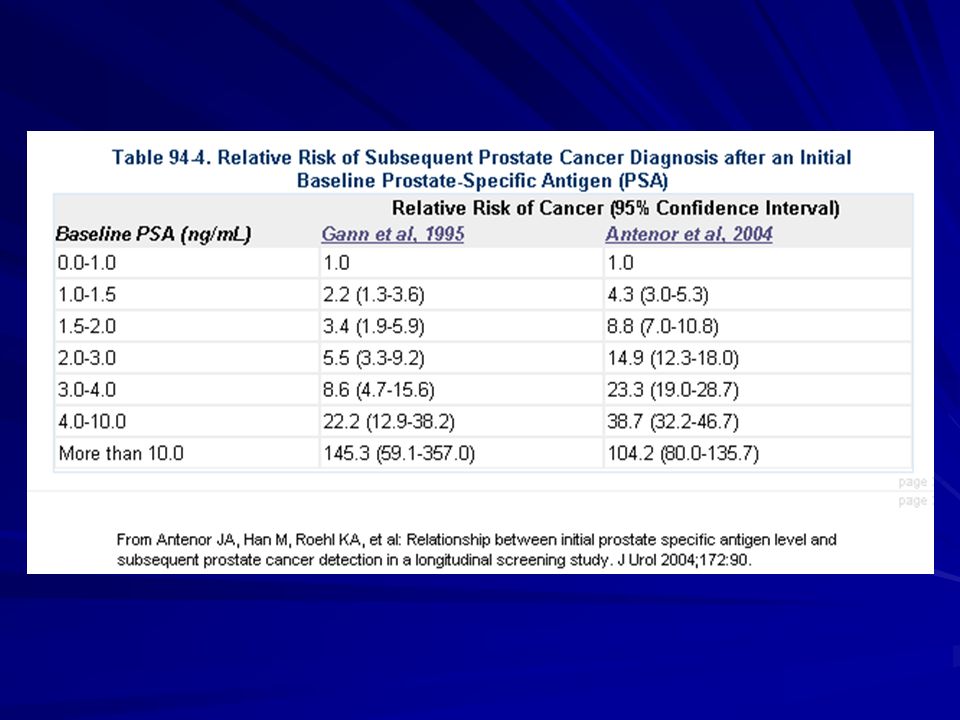
Why do we need PSA Useful for
Prostate cancer screening Widespread use after 1987 Follow-up after therapy Diagnostic value of PSA alone without rectal exam

Présentations similaires





 and associated factors in HIV-infected patients,>")




>")













