Télécharger la présentation
1
Dr Serge Lepage cardiologue CHUS
Recommandation consensuelle du traitement du patient avec dysfonction ventriculaire gauche asymptomatique. Dr Serge Lepage cardiologue CHUS

2
Pré-angioplastie primaire
Post-angioplastie primaire

3
L ’insuffisance cardiaque (2)
Classification Étapes de la maladie et (périodes critiques d ’organisation des services3) Classes NYHA2 (New York Heart Association) A : Avant B : Émergence de l ’insuffisance cardiaque I : Aucun symptôme II : Symptômes pendant des activités ordinaires III : Symptômes pendant des activités moins qu’ordinaires IV : Symptômes au repos C : Relative autonomie D: Perte sévère d ’autonomie E: Fin de vie
 Classes NYHA2. (New York Heart Association) A : Avant. B : Émergence de l ’insuffisance cardiaque. I : Aucun symptôme. II : Symptômes pendant des activités ordinaires. III : Symptômes pendant des activités moins qu’ordinaires. IV : Symptômes au repos. C : Relative autonomie. D: Perte sévère d ’autonomie. E: Fin de vie.")
4
Période après inclusion (années)
Pronostic de l’IC 1,0 0,8 0,6 0,4 0,2 Survie Pas d’IC (n = 1728) Classe I NYHA (n = 36) Classe II NYHA (n = 79) Classe III NYHA (n = 62) Classe IV NYHA (n = 59) Période après inclusion (années) NYHA = New York Heart Association Smith WM. Am J Cardiol 1985;55:3A-8A.
 Classe I NYHA (n = 36) Classe II NYHA (n = 79) Classe III NYHA (n = 62) Classe IV NYHA (n = 59) Période après inclusion (années) NYHA = New York Heart Association. Smith WM. Am J Cardiol 1985;55:3A-8A.")
5
Continuum d’événements conduisant à la mortalité cardiovasculaire :
Les BRAs dans le traitement de l’insuffisance cardiaque congestive L’insuffisance cardiaque congestive (ICC) est une complication cardiovasculaire importante associée à l’hypertension non-maîtrisée. Le taux de mortalité suite à une ICC demeure élevé, malgré les progrès considérables en thérapie pharmacologique. Un nombre alarmant, 50 % des patients avec ICC meurent de cette condition en l’espace de 5 ans après le diagnostic. Cela souligne l’importance de traiter l’hypertension de façon plus aggressive, et à un stade précoce de la maladie, pour réduire l’incidence d’événements cardiovasculaires potentiellement mortels, incluant l’insuffisance cardiaque. Il a été démontré que la thérapie avec les inhibiteurs de l’ECA améliore la survie des patients atteints d’ICC. Des études incluant un très grand nombre de patients sont en cours avec les BRAs, en vue d’évaluer leurs potentiels bienfaits sur les événements cliniques affectant les patients avec ICC. Dzau V, Braunwald E, et al. Resolved and unresolved issues in the prevention and treatment of coronary artery disease: A workshop consensus statement. Am Heart J 1991;121: Kannel WB, Belanger AJ. Epidemiology of heart failure. Am Heart J 1991;121: Cohn JN. The management of chronic heart failure. N Engl J Med 1996;335:
 est une complication cardiovasculaire importante associée à l’hypertension non-maîtrisée. Le taux de mortalité suite à une ICC demeure élevé, malgré les progrès considérables en thérapie pharmacologique. Un nombre alarmant, 50 % des patients avec ICC meurent de cette condition en l’espace de 5 ans après le diagnostic. Cela souligne l’importance de traiter l’hypertension de façon plus aggressive, et à un stade précoce de la maladie, pour réduire l’incidence d’événements cardiovasculaires potentiellement mortels, incluant l’insuffisance cardiaque. Il a été démontré que la thérapie avec les inhibiteurs de l’ECA améliore la survie des patients atteints d’ICC. Des études incluant un très grand nombre de patients sont en cours avec les BRAs, en vue d’évaluer leurs potentiels bienfaits sur les événements cliniques affectant les patients avec ICC. Dzau V, Braunwald E, et al. Resolved and unresolved issues in the prevention and treatment of coronary artery disease: A workshop consensus statement. Am Heart J 1991;121: Kannel WB, Belanger AJ. Epidemiology of heart failure. Am Heart J 1991;121: Cohn JN. The management of chronic heart failure. N Engl J Med 1996;335:")
6
Diagnostic clinique Critères de Framingham1
2 symptômes majeurs OU 1 majeur + 2 mineurs = diagnostic Majeur DNP ou orthopnée DVC Râles Cardiomégalie Œdème pulmonaire aigu Bruits de galop PVC > 16 cm H2O Temps de circulation 25 sec. Reflux hépatojugulaire Mineur Œdème bilatéral des chevilles Toux nocturne Dyspnée à l’effort ordinaire Hépatomégalie Épanchement pleural Baisse de la capacité vitale du ⅓ p/r aux valeurs maximales notées Tachycardie (≥ 120 battements/min.) Majeur ou mineur Perte pondérale ≥ 4,5 kg en 5 jours en réponse au traitement PVC = pression veineuse centrale PVJ = pression veineuse jugulaire DVC = distention des veines du cou DNP = dyspnée nocture paroxystique 1. McKee PA, et al. N Engl J Med 1971;285:
 Majeur ou mineur. Perte pondérale ≥ 4,5 kg en 5 jours en réponse au traitement. PVC = pression veineuse centrale. PVJ = pression veineuse jugulaire. DVC = distention des veines du cou. DNP = dyspnée nocture paroxystique. 1. McKee PA, et al. N Engl J Med 1971;285:")
7
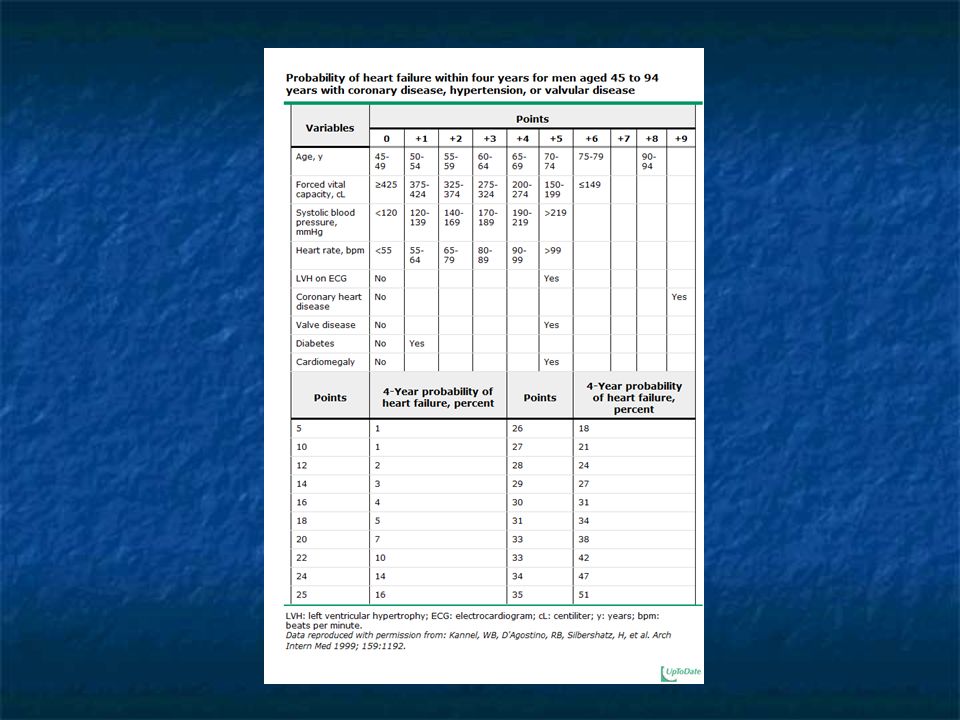
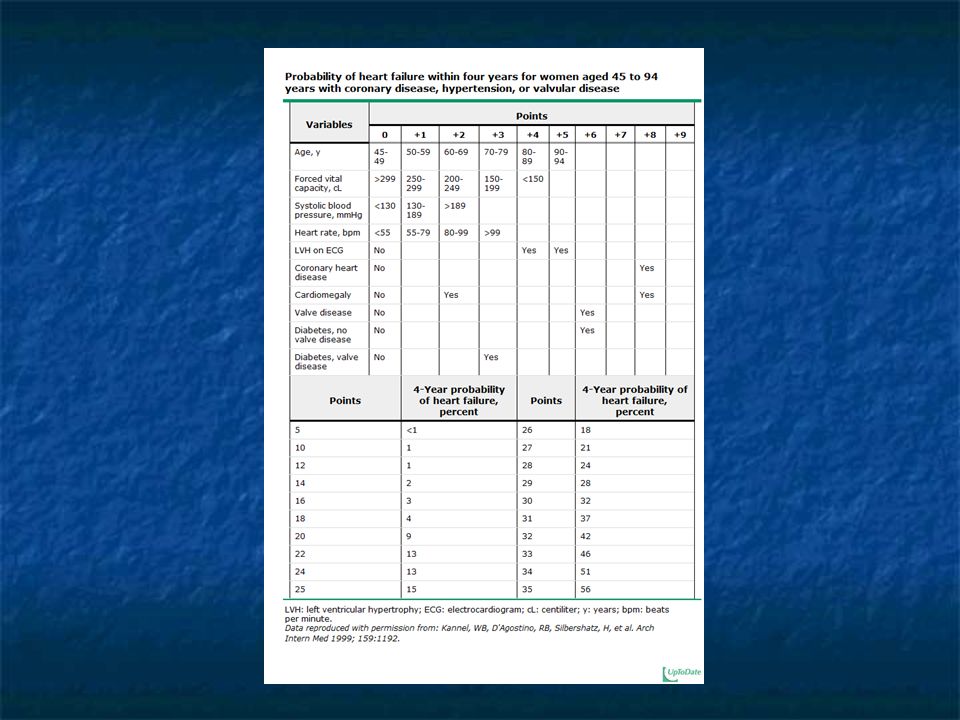
Screening studies using LVEF
The prevalence in echocardiographic screening studies varies in part with the LVEF used to define LV systolic dysfunction and with age. The normal reference limit for LVEF by echocardiography is ≥55 percent [8]. The following observations illustrate the reported prevalence of asymptomatic LV systolic dysfunction in relation to LVEF; the mean age in these studies was 50 to 70 years [9]: LVEF ≤54 percent — 12.5 percent [10] LVEF ≤50 percent — 3.3 to 4.7 percent [11,12] LVEF ≤40 percent — 0.9 to 2.1 percent [10-13] LVEF ≤30 percent — 1.4 percent; almost all of these patients with severe LV dysfunction had evidence of coronary heart disease and/or hypertension [14 ]

8
First National Health and Nutrition Examination Survey (NHANES I)
13,643 men and women who were followed for 19 years found that the risk factors for HF and their population attributable risk (PAR) were as follows Coronary heart disease — relative risk 8.1; overall PAR 62 percent, 68 percent in men and 56 percent in women Cigarette smoking — relative risk 1.6, PAR 17 percent Hypertension — relative risk 1.4, PAR 10 percent Overweight — relative risk 1.3, PAR 8 percentDiabetes — relative risk 1.9, PAR 3 percent Valvular heart disease — relative risk 1.5, PAR 2 percent; however, valve disease is an increasingly common cause of HF at older ages, with calcific aortic stenosis being the most common disorder requiring surgery
 were as follows. Coronary heart disease — relative risk 8.1; overall PAR 62 percent, 68 percent in men and 56 percent in women. Cigarette smoking — relative risk 1.6, PAR 17 percent. Hypertension — relative risk 1.4, PAR 10 percent. Overweight — relative risk 1.3, PAR 8 percentDiabetes — relative risk 1.9, PAR 3 percent. Valvular heart disease — relative risk 1.5, PAR 2 percent; however, valve disease is an increasingly common cause of HF at older ages, with calcific aortic stenosis being the most common disorder requiring surgery.")
11
Symptomatic and asymptomatic left-ventricular systolic dysfunction in an urban population.
McDonagh TA, Morrison CE, Lawrence A, Ford I, Tunstall-Pedoe H, McMurray JJ, Dargie HJ BACKGROUND: In most previous epidemiological studies on the prevalence of chronic heart failure (CHF) the disorder has been defined on clinical criteria. In a cross-sectional survey of 2000 men and women aged 25-74, randomly sampled from one geographical area, we assessed left-ventricular systolic function by echocardiography. METHODS: 1640 (83%) of those invited took part. They completed a questionnaire on current medication, history, and symptoms of breathlessness. Blood pressure was measured and electrocardiography (ECG) and echocardiography were done. Left-ventricular ejection fraction was measurable in 1467 (89.5%) participants by the biplane Simpson's rate method. FINDINGS: The mean left-ventricular ejection fraction was 47.3%. The prevalence of definite left-ventricular systolic dysfunction (defined as a left-ventricular ejection fraction<or = 30%) was 2.9% overall (43 participants); it increased with age and was higher in men than in women (4.0 vs 2.0%). The left-ventricular systolic dysfunction was symptomatic in 1.5% of participants and asymptomatic in 1.4%, 83% of participants with left-ventricular systolic dysfunction had evidence of ischaemic heart disease (IHD) from history or ECG criteria compared with 21% of those without this abnormality (p<0.001). Hypertension was also more common in those with left-ventricular systolic dysfunction (72 vs 38%, p<0.001), but there was no difference between those with and without left-ventricular systolic dysfunction in the rate of hypertension without IHD. INTERPRETATION: Left-ventricular systolic dysfunction was at least twice as common as symptomatic heart failure defined by clinical criteria. The main risk factors are IHD and hypertension in the presence of IHD; screening of such high-risk groups for left-ventricular systolic dysfunction should be considered. Lancet. 1997;350(9081):829.
 the disorder has been defined on clinical criteria. In a cross-sectional survey of 2000 men and women aged 25-74, randomly sampled from one geographical area, we assessed left-ventricular systolic function by echocardiography. METHODS: 1640 (83%) of those invited took part. They completed a questionnaire on current medication, history, and symptoms of breathlessness. Blood pressure was measured and electrocardiography (ECG) and echocardiography were done. Left-ventricular ejection fraction was measurable in 1467 (89.5%) participants by the biplane Simpson s rate method. FINDINGS: The mean left-ventricular ejection fraction was 47.3%. The prevalence of definite left-ventricular systolic dysfunction (defined as a left-ventricular ejection fraction<or = 30%) was 2.9% overall (43 participants); it increased with age and was higher in men than in women (4.0 vs 2.0%). The left-ventricular systolic dysfunction was symptomatic in 1.5% of participants and asymptomatic in 1.4%, 83% of participants with left-ventricular systolic dysfunction had evidence of ischaemic heart disease (IHD) from history or ECG criteria compared with 21% of those without this abnormality (p<0.001). Hypertension was also more common in those with left-ventricular systolic dysfunction (72 vs 38%, p<0.001), but there was no difference between those with and without left-ventricular systolic dysfunction in the rate of hypertension without IHD. INTERPRETATION: Left-ventricular systolic dysfunction was at least twice as common as symptomatic heart failure defined by clinical criteria. The main risk factors are IHD and hypertension in the presence of IHD; screening of such high-risk groups for left-ventricular systolic dysfunction should be considered. Lancet. 1997;350(9081):829.")
12
Echocardiography has been used to diagnose LV dysfunction in community-based studies and clinical trials. However, echocardiography is expensive and serial testing would be required if the initial test is negative. Furthermore, the yield is very low in patients with no risk factors (1 of 444 [0.2 percent] in one report) [15]. Thus, routine screening with echocardiography is not recommended [7].
 [15]. Thus, routine screening with echocardiography is not recommended [7]..")
13
Atherton, J. J. J Am Coll Cardiol Img 2010;3:421-428
Kaplan-Meier Curves for Survival of Participants From the Framingham Study Atherton, J. J. J Am Coll Cardiol Img 2010;3: Copyright ©2010 American College of Cardiology Foundation. Restrictions may apply.

15
Diagnostic d’IC Référence :
1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
16
Principes de la pharmacothérapie
Les médicaments dont les effets ont été prouvés lors d’essais cliniques à grande échelle sont recommandés, car ils ont des doses cibles efficaces reconnues (Classe I, Niveau A) Il faut utiliser les doses issues d’essais cliniques à grande échelle ou une dose inférieure correspondant à la dose maximale tolérée (voir tableau de la diapositive suivante) Références : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. 2. Packer M et al. Comparative effects of low and high doses of the angiotensin-converting enzyme inhibitor, lisinopril, on morbidity and mortality in chronic heart failure. Circulation 1999;100: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
 Il faut utiliser les doses issues d’essais cliniques à grande échelle ou une dose inférieure correspondant à la dose maximale tolérée (voir tableau de la diapositive suivante) Références : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1): Packer M et al. Comparative effects of low and high doses of the angiotensin-converting enzyme inhibitor, lisinopril, on morbidity and mortality in chronic heart failure. Circulation 1999;100: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
17
Quelle dose de médicament doit-on utiliser?
Référence : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. * L’essai Healing and Early Afterload Reduced Therapy (HEART) a montré que la dose efficace pour atténuer le remodelage du ventricule gauche était de 10 mg od. † Non disponible au Canada. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
: * L’essai Healing and Early Afterload Reduced Therapy (HEART) a montré que la dose efficace pour atténuer le remodelage du ventricule gauche était de 10 mg od. † Non disponible au Canada. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
18
SOLVD (Studies of Left Ventricular Dysfunction)
Enalapril vs placebo in 6,794 patients Ejection fraction < 35% End points include : Delaying the progression of heart failure Improving signs and symptoms Reducing mortality Treatment arm - 2,568 symptomatic class II-III patients most on digitalis and diuretics Prevention arm - 4,226 asymptomatic class I-II patients, most on no concomitant therapy N Engl J Med 1991:325:

19
Prevention Trial All Cause Mortality
SOLVD Prevention Trial All Cause Mortality Risk Reduction 8% P=0.30 N Engl J Med 1992;327:685-91

20
SOLVD Prevention Trial Death or Development of CHF
Risk Reduction 29% p<0.001 N Engl J Med 1992;327:685-91

21
SOLVD Prevention Trial First Hospitalization for CHF
Risk Reduction 36% p<0.001 N Engl J Med 1992;327:685-91

22
SOLVD Prevention Trial
N Engl J Med 1992;327:685-91

23
SOLVD Prevention- Enalapril Asymptomatic HF Patients w/ LVD (EF < 35%)
(NYHA Class I-II) 32% Fewer First Hospitalizations p<0.001 273 184 Number of First Hospitalizations for Heart Failure The SOLVD Investigators, N Engl J Med, 1992.
 32% Fewer First. Hospitalizations. p< Number of First Hospitalizations for Heart Failure. The SOLVD Investigators, N Engl J Med,")
24
SOLVD Prevention Trial Morbidity and Combined Outcomes

25
Par où commencer? Une pharmacothérapie combinée fondée sur des preuves scientifiques est recommandée pour la majorité des patients souffrant d’IC (Classe I, Niveau A) Tous les patients souffrant d’IC avec une FEVG < 40 % doivent être traités avec un IECA et un bêta- bloquant, sauf dans le cas d’une contre-indication particulière Référence : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
 Tous les patients souffrant d’IC avec une FEVG < 40 % doivent être traités avec un IECA et un bêta- bloquant, sauf dans le cas d’une contre-indication particulière. Référence : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1): Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
26
Quand doit-on utiliser des inhibiteurs de l’ECA?
Tous les patients souffrant d’IC avec une FEVG < 40 % doivent être traités avec un IECA et un bêta-bloquant, sauf dans le cas d’une contre-indication particulière (Classe I, Niveau A) CONSENSUS Trial. N Engl J Med 1987;316: SOLVD Investigators. N Engl J Med 1991;325: Flather MD et al. Lancet 2000;355: Références : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. 2. The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med 1987;316: 3. The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med 1991;325: 4. Flather MD et al. Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patients. Lancet 2000;355: Ces études constituent le fondement de l’utilisation des IECA chez les insuffisants cardiaques avec une FEVG < 40 % ou chez les patients post-IM présentant une FEVG réduite ou une IC. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
 CONSENSUS Trial. N Engl J Med 1987;316: SOLVD Investigators. N Engl J Med 1991;325: Flather MD et al. Lancet 2000;355: Références : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1): The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure: results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N Engl J Med 1987;316: The SOLVD Investigators. Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. N Engl J Med 1991;325: Flather MD et al. Long-term ACE-inhibitor therapy in patients with heart failure or left-ventricular dysfunction: a systematic overview of data from individual patients. Lancet 2000;355: Ces études constituent le fondement de l’utilisation des IECA chez les insuffisants cardiaques avec une FEVG < 40 % ou chez les patients post-IM présentant une FEVG réduite ou une IC. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
27
Quand doit-on utiliser des inhibiteurs de l’ECA?
Les inhibiteurs de l’ECA préviennent la survenue de l’IC chez les patients à risque References: 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. 2. The SOLVD Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med 1992;327: 3. Arnold JMO et al. Prevention of heart failure in patients in the Heart Outcomes Prevention Evaluation (HOPE) study. Circulation 2003;107: Arnold JMO et al. Circulation 2003;107: SOLVD Investigators. N Engl J Med 1992;327: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
: The SOLVD Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomatic patients with reduced left ventricular ejection fractions. N Engl J Med 1992;327: Arnold JMO et al. Prevention of heart failure in patients in the Heart Outcomes Prevention Evaluation (HOPE) study. Circulation 2003;107: Arnold JMO et al. Circulation 2003;107: SOLVD Investigators. N Engl J Med 1992;327: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
28
Des études additionnelles soulignent les avantages prolongés des inhibiteurs des ECA
Traitement Ramipril Énalapril Énalapril Ramipril Suivi 5-10 ans 10 ans 12 ans 7,2 ans Caractéristique IC clinique, IC de classe IV IC, dysfonctionnement Risque CV élevé post-IM (NYHA) du VG sans dysfonctionnement du VG, sans IC Résultats RRR de mortalité Survie générale Survie prolongée Réduction du nombre de 36 % prolongée de 9,4 mois d’événements CV majeurs de 50 % et de nouveaux cas de diabète Résumé Importante réduction de Effets bénéfiques Meilleure survie Avantages CV et mortalité à long terme maintenus pendant à long terme métaboliques à long avec le traitement IECA au moins 4 ans terme chez les patients post-IM ne souffrant ni d’insuffisance cardiaque ni d’un dysfonctionnement du VG Références : 1. Hall AS et al. Follow-up study of patients randomly allocated ramipril or placebo for heart failure after acute myocardial infarction: AIRE Extension (AIREX) study. Lancet 1997;349: 2. Swedberg K et al. Long-term survival in severe heart failure in patients treated with enalapril: ten year follow-up of CONSENSUS I. Eur Heart J 1999;20: 3. Jong P et al. Effect of enalapril on 12-year survival and life expectancy in patients with left ventricular systolic dysfunction: a follow-up study. Lancet 2003;361: 4. HOPE/HOPE-TOO Study Investigators. Long-term effects of ramipril on cardiovascular events and on diabetes: results of the HOPE study extension. Circulation 2005;112: Hall AS et al. Lancet 1997;349: Swedberg K et al. Eur Heart J 1999;20:136-9. Jong P et al. Lancet 2003;361: HOPE/HOPE-TOO Study Investigators. Circulation 2005;112:
 du VG sans dysfonctionnement du VG, sans IC. Résultats RRR de mortalité Survie générale Survie prolongée Réduction du nombre de 36 % prolongée de 9,4 mois d’événements CV majeurs de 50 % et de nouveaux cas de diabète. Résumé Importante réduction de Effets bénéfiques Meilleure survie Avantages CV et mortalité à long terme maintenus pendant à long terme métaboliques à long avec le traitement IECA au moins 4 ans terme chez les patients. post-IM ne souffrant ni d’insuffisance cardiaque ni d’un. dysfonctionnement du VG. Références : 1. Hall AS et al. Follow-up study of patients randomly allocated ramipril or placebo for heart failure after acute myocardial infarction: AIRE Extension (AIREX) study. Lancet 1997;349: Swedberg K et al. Long-term survival in severe heart failure in patients treated with enalapril: ten year follow-up of CONSENSUS I. Eur Heart J 1999;20: Jong P et al. Effect of enalapril on 12-year survival and life expectancy in patients with left ventricular systolic dysfunction: a follow-up study. Lancet 2003;361: HOPE/HOPE-TOO Study Investigators. Long-term effects of ramipril on cardiovascular events and on diabetes: results of the HOPE study extension. Circulation 2005;112: Hall AS et al. Lancet 1997;349: Swedberg K et al. Eur Heart J 1999;20: Jong P et al. Lancet 2003;361: HOPE/HOPE-TOO Study Investigators. Circulation 2005;112:")
29
Les avantages à long terme des inhibiteurs d’ECA sur la mortalité
Références : 1. Swedberg K et al. Long-term survival in severe heart failure in patients treated with enalapril: ten year follow-up of CONSENSUS I. Eur Heart J 1999;20:136-9. 2. Jong P et al. Effect of enalapril on 12-year survival and life expectancy in patients with left ventricular systolic dysfunction: a follow-up study. Lancet 2003;361: Hall AS et al. Lancet 1997;349: Jong P et al. Lancet 2003;361:

30
Les avantages à long terme des inhibiteurs d’ECA sur la mortalité
Références : 1. HOPE/HOPE-TOO Study Investigators. Long-term effects of ramipril on cardiovascular events and on diabetes: results of the HOPE study extension. Circulation 2005;112: 2. Hall AS et al. Follow-up study of patients randomly allocated ramipril or placebo for heart failure after acute myocardial infarction: AIRE Extension (AIREX) study. Lancet 1997;349: HOPE/HOPE-TOO Study Investigators. Circulation 2005;112: Swedberg K et al. Eur Heart J 1999;20:136-9.
 study. Lancet 1997;349: HOPE/HOPE-TOO Study Investigators. Circulation 2005;112: Swedberg K et al. Eur Heart J 1999;20:")
31
Quand utiliser les bêta-bloquants?
Chez tous les patients souffrant d’IC avec une FEVG ≤ 40 % (utiliser des bêta- bloquants ayant fait l’objet de preuves scientifiques) (Classe I, Niveau A) Chez tous les patients stabilisés présentant des symptômes de classe IV NYHA (Classe I, Niveau C) Références : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. 2. MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999;353: 3. CIBIS II Investigators and Committee. The Cardiac Insufficiency Bisoprolol Study II: a randomized trial. Lancet 1999;353:9-13. 4. Packer M, Fowler MB, Roecker EB, et al, for the Carvedilol prospective randomised cumulative survival (COPERNICUS) study group. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomised cumulative survival (COPERNICUS) study. Circulation 2002;106: MERIT-HF Study Group. Lancet 1999;353: CIBIS II Investigators Lancet 1999;353:9-13. Packer M et al. Circulation 2002;106: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
 (Classe I, Niveau A) Chez tous les patients stabilisés présentant des symptômes de classe IV NYHA (Classe I, Niveau C) Références : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1): MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomized Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999;353: CIBIS II Investigators and Committee. The Cardiac Insufficiency Bisoprolol Study II: a randomized trial. Lancet 1999;353: Packer M, Fowler MB, Roecker EB, et al, for the Carvedilol prospective randomised cumulative survival (COPERNICUS) study group. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the carvedilol prospective randomised cumulative survival (COPERNICUS) study. Circulation 2002;106: MERIT-HF Study Group. Lancet 1999;353: CIBIS II Investigators Lancet 1999;353:9-13. Packer M et al. Circulation 2002;106: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
32
Stratégies de traitement de l’IC
Asymptomatique Légère/Mod. Grave Réfractaire CRT (LBBB), CPAP Digoxine/Dérivés nitrés Spironolactone Risque de mort subit — AICD Ajustement des BB IECA/(ARA) Aucun sel ajouté 2 gm Na Programme de style de vie personnalisé Suivi clinique de l’IC
, CPAP. Digoxine/Dérivés nitrés. Spironolactone. Risque de mort subit — AICD. Ajustement des BB. IECA/(ARA) Aucun sel ajouté. 2 gm Na. Programme de. style de vie. personnalisé. Suivi clinique de l’IC.")
33
Treatment Approach for the Patient with Heart Failure
Stage A At high risk, no structural disease Stage B Structural heart disease, asymptomatic Stage C Structural heart disease with prior/current symptoms of HF Stage D Refractory HF requiring specialized interventions Therapy Treat Hypertension Treat lipid disorders Encourage regular exercise Discourage alcohol intake ACE inhibition Therapy All measures under stage A ACE inhibitors in appropriate patients Beta-blockers in appropriate patients Therapy All measures under stage A Drugs: Diuretics ACE inhibitors Beta-blockers Digitalis Dietary salt restriction Therapy All measures under stages A,B, and C Mechanical assist devices Heart transplantation Continuous (not intermittent) IV inotropic infusions for palliation Hospice care Hunt, SA et al. ACC/AHA Guidelines CHF, 2001.
 IV inotropic infusions for palliation. Hospice care. Hunt, SA et al. ACC/AHA Guidelines CHF,")
34
Treatment Approach for the Patient with Heart Failure
Stage A At high risk, no structural disease Stage B Structural heart disease, asymptomatic Therapy Treat Hypertension Treat lipid disorders Encourage regular exercise Discourage alcohol intake ACE inhibition Therapy All measures under stage A ACE inhibitors in appropriate patients Beta-blockers in appropriate patients Hunt, SA et al. ACC/AHA Guidelines CHF, 2001.

35
Treatment Overview Jessup and Brozena. Heart Failure; N Engl Med. 2003;348:

37
Mortality Trials in Systolic Heart Failure: 1986-2004
ACE inhibitors CONSENSUS-II V-HeFT-II SOLVD-T SOLVD-P SAVE AIRE TRACE ATLAS -Blockers MDC U.S. Carvedilol ANZ Carvedilol MERIT-HF CIBIS-II BEST COPERNICUS CAPRICORN Inotropic agents PROMISE VEST DIG OPTIME-II Cytokine antagonists RENAISSANCE RECOVER Vasodilators V-HeFT FIRST PRAISE-I/-II ARBs ELITE-II Val-HeFT OPTIMAAL CHARM VALIANT Endothelin antagonists ENABLE-2 Sympatholytic agents MOXCON Aldosterone antagonists RALES EPHESUS Positive Borderline/Neutral Negative ACE/NEP Inhibitors OVERTURE Slide courtesy of G. Francis

38
Traitement de l’insuffisance cardiaque
Référence : 1. Arnold JMO, Liu P et al. Canadian Cardiovascular Society consensus conference recommendations on heart failure 2006:diagnosis and management. Can J Cardiol 2006;22(1):23-45. Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):23-45.
: Arnold JMO, Liu P et al. Can J Cardiol 2006;22(1):")
39
ACE inhibition, angiotensin receptor blockade and aldosterone antagonism
Recommendations Consensus conference recommendations on heart failure 2006 ACE inhibitors should be used in all patients as soon as safely possible after acute myocardial infarction, and should be continued indefinitely if LVEF is less than 40% or if AHF complicated the myocardial infarction (class I, level A). Can J Cardiol Vol 22 No 1 January 2006
. Can J Cardiol Vol 22 No 1 January")
40
ACE inhibition, angiotensin receptor blockade and aldosterone antagonism
ACE inhibitors should be used in all asymptomatic patients with an LVEF less than 35% (class I, level A). ACE inhibitors should be used in all patients with symptoms of heart failure and an LVEF less than 40% (class I, level A). Consensus conference recommendations on heart failure 2006
. ACE inhibitors should be used in all patients with symptoms of heart failure and an LVEF less than 40% (class I, level A). Consensus conference recommendations on heart failure")
41
Beta-adrenoceptor blockade
Recommendations All heart failure patients with an LVEF equal to or less than 40% should receive a beta-blocker proven to be beneficial in large-scale clinical trials (class I, level A). Practical tips • Patients in NYHA class I or II can be safely initiated and titrated with a beta-blocker by nonspecialist physicians. New York Heart Association functional classification Class Definition I No symptoms Consensus conference recommendations on heart failure 2006
. Practical tips. • Patients in NYHA class I or II can be safely initiated and. titrated with a beta-blocker by nonspecialist physicians. New York Heart Association functional classification. Class Definition. I No symptoms. Consensus conference recommendations on heart failure")
42
Potential to Prevent HF Hospitalizations
Diet Noncompliance 24% Rx Noncompliance 24% 16% Inappropriate Rx 17% Other 19% Failure to Seek Care 42



 and associated factors in HIV-infected patients,>")







 What is the Present Tense ? In English and in French the present tense is used to talk about things which are.>")









 Nombres (1-100).>")