Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

2
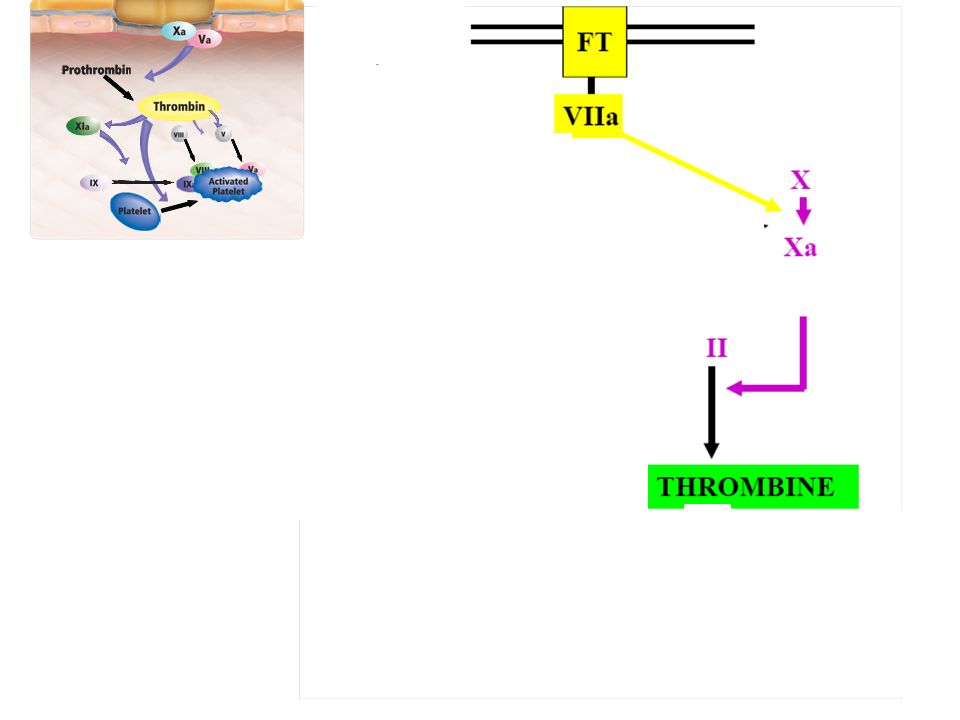
Processus complexe échelle cellulaire +++ (test en phase liquide) Maintenir le sang liquide et à l’interieur des vaisseaux
 Maintenir le sang liquide et à l’interieur des vaisseaux.")
3
Facteurs de Coagulation Inhibiteurs de la Coagulation
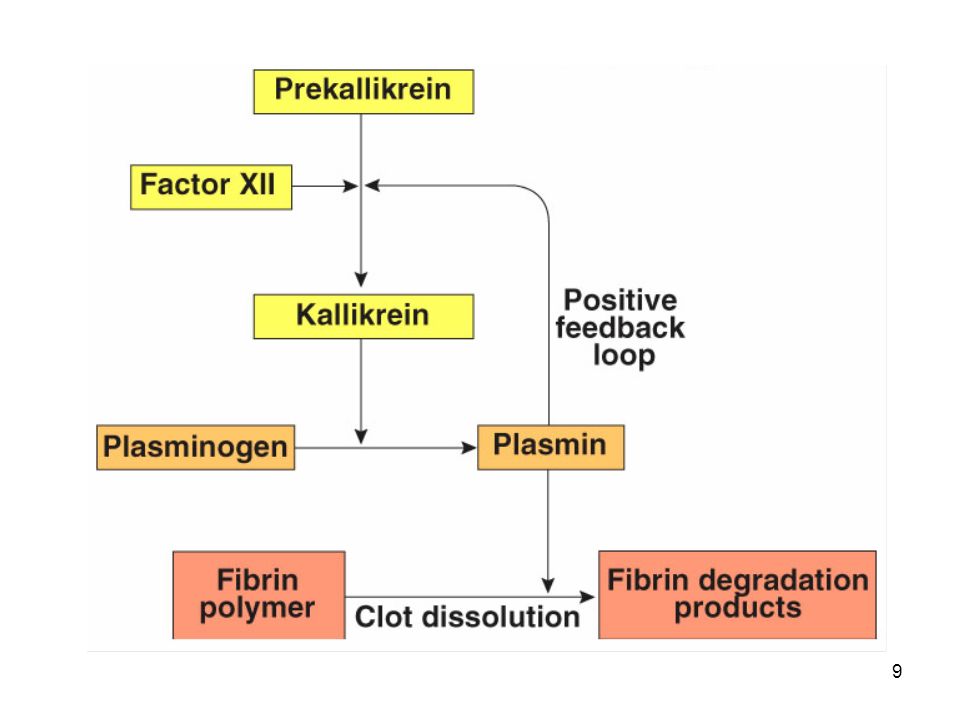
Inhibiteurs de la Fibrinolyse Activateurs de la fibrinolyse

4
Injured blood vessel releases ADP, which attracts platelets (PLT)
Local vascoconstriction is due to local spasm of the smooth muscle (symp. reflex) can be maintained by platelet vasoconstrictors PLT comming in contact with exposed collagen release: serotonin, ADP, TXA2, which accelerate vasoconstriction and causes PLT to swell and become more sticky
 can be maintained by platelet vasoconstrictors. PLT comming in contact with exposed collagen release: serotonin, ADP, TXA2, which accelerate vasoconstriction and causes PLT to swell and become more sticky.")
7
7

8
8

11
Tranexanic acid

12
Wheeler AP, Chest 2010

13
CONDITIONS PREANALYTIQUES TRES IMPORTANTES
prélèvement sur tube citraté (chélateur du calcium) ponction veineuse franche, garrot < 1 min si possible prélever un tube sec avant ne pas prélever le tube citrate après un tube contenant un autre anticoagulant (EDTA, héparine… ) remplir le tube correctement (Rapport 1:9) agitation douce délai d’acheminement + réalisation < 4H
 ponction veineuse franche, garrot < 1 min. si possible prélever un tube sec avant. ne pas prélever le tube citrate après un tube contenant un autre anticoagulant (EDTA, héparine… ) remplir le tube correctement (Rapport 1:9) agitation douce. délai d’acheminement + réalisation < 4H.")
14
Que faites vous en première intention ?
H 76 ans Ecchymoses + hématomes diffus Hémarthrose du genou droit Absence de défaillance viscérale Que faites vous en première intention ?

15
H 76 ans Traitement : HTA sous ARA-II ATCD Appendicectomie enfance Cholecystectomie il y a 10 ans Chirurgie sans complication ni particularité

16
Résultats des tests d’hémostase :
NP 264 x 109/L TCA 112 s (T= 38 s) TP 11 sec (> 80%) Fibrinogène 2,4 g/L Quel(s) test(s) d’hémostase complémentaire proposez vous ? A 76-year-old man presents to the emergency department with numerous ecchymoses and bleeding from the gums. He has been previously well, and he takes no medications. There is a history of uncomplicated appendectomy and cholecystectomy. On physical examination, he has extensive bruising, and there is oozing from intravenous puncture sites. In addition, he has a swollen, painful left knee TCA M+T / dosage des cofacteurs
 TP 11 sec (> 80%) Fibrinogène 2,4 g/L. Quel(s) test(s) d’hémostase complémentaire proposez vous A 76-year-old man presents to the emergency department with numerous ecchymoses and bleeding from the gums. He has been previously well, and he takes no medications. There is a history of uncomplicated appendectomy and cholecystectomy. On physical examination, he has extensive bruising, and there is oozing from intravenous puncture sites. In addition, he has a swollen, painful left knee. TCA M+T / dosage des cofacteurs.")
17
Le diagnostic le plus probable :
NP 264 x 109/L TCA 112 s (T= 38 s) TP 11 sec (> 80%) Fibrinogène 2,4 g/L TCA M+T = 100 sec FVIII = 5% Le diagnostic le plus probable : (A) CIVD (B) Anticoagulant lupique (C) Déficit en Factor XII (D) Inhibiteur du complexe prothrombinique (E) Anti-VIII acquis Traitement spécifique en cas d’hémorragie ?
 TP 11 sec (> 80%) Fibrinogène 2,4 g/L. TCA M+T = 100 sec. FVIII = 5% Le diagnostic le plus probable : (A) CIVD. (B) Anticoagulant lupique. (C) Déficit en Factor XII. (D) Inhibiteur du complexe prothrombinique. (E) Anti-VIII acquis. Traitement spécifique en cas d’hémorragie")
18
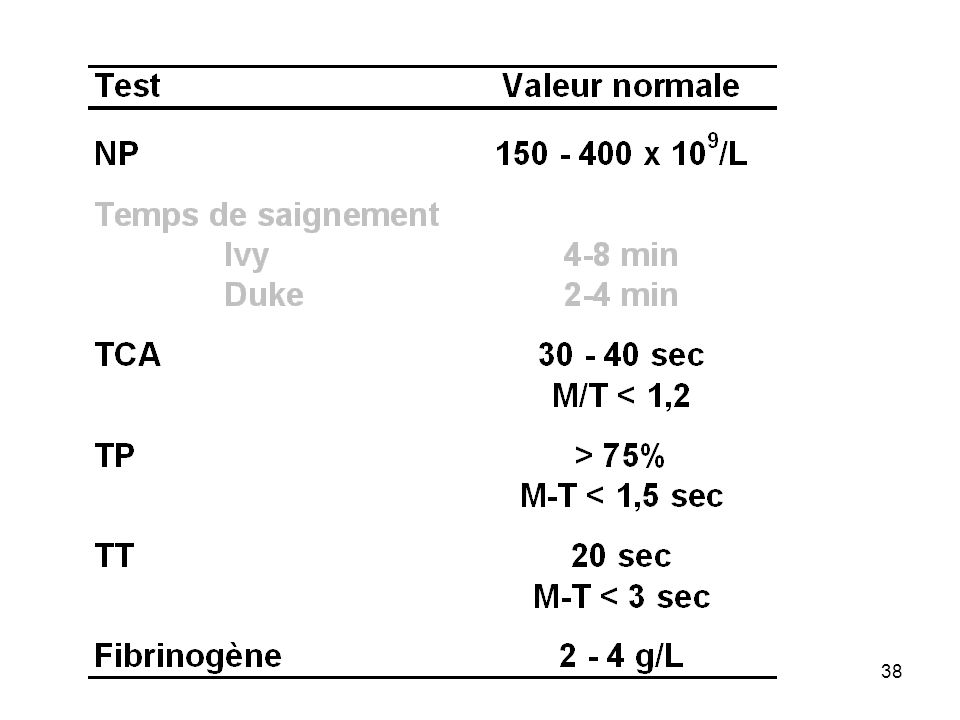
Tests de coagulation

19
Test d’hémostase Production destruction Mécanismes consommation
distribution inhibition

20
Insuffisance hépatique
Test d’hémostase Hypovitaminose K Etiologies Fibrinolyse LA / SCAP CIVD Insuffisance hépatique

21
Test d’hémostase Tests chronométriques Tests amidolytiques
Tests immunologiques Tests moléculaires Tests globaux Test spécifiques (cofacteur)
")
22
Tests chronométriques
Tests d’hémostase Tests chronométriques Temps de coagulation après addition d’inducteurs Vitesse de formation du caillot = automatique Tests globaux ou mesure d’un Facteur de Coag Tests fonctionnels

23
Test chromogénique (amidolytique)
Chromophore : para-nitroaniline (pNA), spectrophotomètrie (405 nm fixé à oligopeptide structure spécifique / enzyme Activité de l’enzyme scinde le peptide et libère PNa Coloration // activit enzyme Test fonctionnel +++ Enzymatic activity of coagulation proteins and other substances can be measured by the chromogenic method in two ways: Direct measurement- the greater the change in optical density, the higher the level of the analyte. In essence, the change in optical density is proportional to the amount of the substance being measured (e.g., protein C activity assays). Primary assays, in which a substrate specific for the enzyme to be measured is used. Secondary assays, in which the enzyme or proenzyme measured is used to activate a second protease for which a specific substrate is available. Indirect measurement-the substance being measured has an inhibitory effect on another target enzyme that has activity directed toward the synthetic substrate. In this case, the change in optical density is inversely proportional to the amount of the substance being measured (e.g., heparin antifactor Xa assays). Specific substrates are available for many coagulation enzymes. However, the substrate specificity is not absolute and most kits include inhibitors of other enzymes capable of cleaving the substrate to improve specificity.
, spectrophotomètrie (405 nm. fixé à oligopeptide structure spécifique / enzyme. Activité de l’enzyme scinde le peptide et libère PNa. Coloration // activit enzyme. Test fonctionnel +++ Enzymatic activity of coagulation proteins and other substances can be measured by the chromogenic method in two ways: Direct measurement- the greater the change in optical density, the higher the level of the analyte. In essence, the change in optical density is proportional to the amount of the substance being measured (e.g., protein C activity assays). Primary assays, in which a substrate specific for the enzyme to be measured is used. Secondary assays, in which the enzyme or proenzyme measured is used to activate a second protease for which a specific substrate is available. Indirect measurement-the substance being measured has an inhibitory effect on another target enzyme that has activity directed toward the synthetic substrate. In this case, the change in optical density is inversely proportional to the amount of the substance being measured (e.g., heparin antifactor Xa assays). Specific substrates are available for many coagulation enzymes. However, the substrate specificity is not absolute and most kits include inhibitors of other enzymes capable of cleaving the substrate to improve specificity.")
24
Tests immunologiques ELISA Latex …. Facteurs de coagulation
Dosage quantitatif +++

25
Tests globaux Temps de céphaline Activé Temps de Quick (exprimé en TP)
Temps de thrombine ACT

26
Tests spécifiques Facteurs de coagulation dosage fonctionnel
dosage immunologique tests moléculaires Dans cet atelier : hors thrombophilie constitutionnelle

27
Temps de coagulation sur sang total
Reflète le temps requis pour générer IIa Ia Le verre active la phase contact : « voie intrinsèque » Interaction cellules / plasma 4-10 mins.

28
Temps de coagulation d’un PRP
Citrate / PRP (Howell) Ca2+ Reflète le temps requis pour générer IIa Ia / « voie intrinsèque » Interactions Plts / plasma 2 mins.
 Ca2+ Reflète le temps requis pour générer IIa Ia / « voie intrinsèque » Interactions Plts / plasma. 2 mins.")
29
Temps de coagulation d’un PPP citraté
Phase liquide et non cellulaire Phase « déplaquettée » En excès de l’agoniste Système fermé

30
Temps de coagulation d’un PPP
Citrate / PPP Activateur + analogue phospholipide Ca2+ Reflète le temps requis pour générer IIa Ia / « voie intrinsèque » 32-35 sec

31
Temps de céphaline activé
XII XI IX VIII X V II I The activated partial thromboplastin time (aPTT) is a test performed to investigate bleeding disorders and to monitor patients taking an anticlotting drug such as heparin which inhibits factors X and thrombin, while activating anti-thrombin. The aPTT test uses blood which is decalcified to prevent clotting before the test begins. The plasma is separated by centrifugation. (Ionized) Calcium and activating substances are added to the plasma to start the intrinsic pathway of the coagulation cascade. The substances are: kaolin (hydrated aluminum silicate) and cephalin. Kaolin serves to activate the contact-dependent Factor XII, and cephalin substitutes for platelet phospholipids. The partial thromboplastin time is the time it takes for a clot to form, measured in seconds. Normally, the sample will clot in 35 seconds. PTT measures the integrity of the intrinsic system (Factors XII, XI, VIII, IX) and common clotting pathways. A particulate contact activator (eg, ellagic acid, kaolin, celite, or silica), is added to platelet-poor, citrated plasma substrate, hence the designation “activated.” A “partial thromboplastin” (lacking tissue factor) is added, followed by reversal of the citrate effect with calcium. Maybe because the sequence is lengthier or the concentration of each factor is lower, single factors unique to the contact activation pathway must decline to only 15% to 30% of normal before the aPTT is prolonged. Heparin is the prototypical example as it binds to antithrombin and thereby inhibits the actions of factors XII, XI, IX, X, and II. Because three of these factors (IX, XI, XII) are exclusive to the contact activation pathway and are more sensitive to heparin effects than the two factors in the common pathway (X and II), heparin alters the aPTT to a greater degree than the PT. In Increased levels in a person with a bleeding disorder indicate a clotting factor may be missing or defective. At this point, further investigation is needed and warrants the use of sensitive assays for specific coagulation factors. Liver disease decreases production of factors, increasing the PTT. The PT test is used to monitor patients taking certain medications as well as to help diagnose clotting disorders. A sample of the patient's blood is obtained by venipuncture. The blood is decalcified (by collecting it into a tube with oxalate or citrate ions) to prevent the clotting process from starting before the test. The blood cells are separated from the liquid part of blood (plasma) by centrifugation. The PT test is performed by adding the patient's plasma to some source of Tissue Factor (e.g.: a protein, thromboplastin, from homogenized brain tissue) that converts prothrombin to thrombin. The mixture is then kept in a warm water bath at 37°C for one to two minutes. Calcium chloride (excess quantities of ionized calcium) is added to the mixture in order to counteract the sodium citrate and allow clotting to start. The test is timed from the addition of the calcium chloride until the plasma clots. This time is called the Prothrombin Time The prothrombin test specifically evaluates the presence of factors VII, V, and X, prothrombin, and fibrinogen. A prothrombin time within the second range (depends on the source of thromboplastin used) indicates that the patient has normal amounts of the above clotting factors. A prolonged prothrombin time indicates a deficiency in any of factors VII, X, V, prothrombin, or fibrinogen. It may mean that the patient has a vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II (prothrombin), VII, IX and X) or a liver disease (the liver is the site of synthesis of the plasma protein factors). The prothrombin time of patients receiving a vitamin K-competing coumarin drug such as warfarin (anticoagulation therapy used in deep venous thrombophlebitis) will also be prolonged, usually in the range of one and one half to two times the normal PT time.
 is a test performed to investigate bleeding disorders and to monitor patients taking an anticlotting drug such as heparin which inhibits factors X and thrombin, while activating anti-thrombin. The aPTT test uses blood which is decalcified to prevent clotting before the test begins. The plasma is separated by centrifugation. (Ionized) Calcium and activating substances are added to the plasma to start the intrinsic pathway of the coagulation cascade. The substances are: kaolin (hydrated aluminum silicate) and cephalin. Kaolin serves to activate the contact-dependent Factor XII, and cephalin substitutes for platelet phospholipids. The partial thromboplastin time is the time it takes for a clot to form, measured in seconds. Normally, the sample will clot in 35 seconds. PTT measures the integrity of the intrinsic system (Factors XII, XI, VIII, IX) and common clotting pathways. A particulate contact activator (eg, ellagic acid, kaolin, celite, or silica), is added to platelet-poor, citrated plasma substrate, hence the designation activated. A partial thromboplastin (lacking tissue factor) is added, followed by reversal of the citrate effect with calcium. Maybe because the sequence is lengthier or the concentration of each factor is lower, single factors unique to the contact activation pathway must decline to only 15% to 30% of normal before the aPTT is prolonged. Heparin is the prototypical example as it binds to antithrombin and thereby inhibits the actions of factors XII, XI, IX, X, and II. Because three of these factors (IX, XI, XII) are exclusive to the contact activation pathway and are more sensitive to heparin effects than the two factors in the common pathway (X and II), heparin alters the aPTT to a greater degree than the PT. In. Increased levels in a person with a bleeding disorder indicate a clotting factor may be missing or defective. At this point, further investigation is needed and warrants the use of sensitive assays for specific coagulation factors. Liver disease decreases production of factors, increasing the PTT. The PT test is used to monitor patients taking certain medications as well as to help diagnose clotting disorders. A sample of the patient s blood is obtained by venipuncture. The blood is decalcified (by collecting it into a tube with oxalate or citrate ions) to prevent the clotting process from starting before the test. The blood cells are separated from the liquid part of blood (plasma) by centrifugation. The PT test is performed by adding the patient s plasma to some source of Tissue Factor (e.g.: a protein, thromboplastin, from homogenized brain tissue) that converts prothrombin to thrombin. The mixture is then kept in a warm water bath at 37°C for one to two minutes. Calcium chloride (excess quantities of ionized calcium) is added to the mixture in order to counteract the sodium citrate and allow clotting to start. The test is timed from the addition of the calcium chloride until the plasma clots. This time is called the Prothrombin Time. The prothrombin test specifically evaluates the presence of factors VII, V, and X, prothrombin, and fibrinogen. A prothrombin time within the second range (depends on the source of thromboplastin used) indicates that the patient has normal amounts of the above clotting factors. A prolonged prothrombin time indicates a deficiency in any of factors VII, X, V, prothrombin, or fibrinogen. It may mean that the patient has a vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II (prothrombin), VII, IX and X) or a liver disease (the liver is the site of synthesis of the plasma protein factors). The prothrombin time of patients receiving a vitamin K-competing coumarin drug such as warfarin (anticoagulation therapy used in deep venous thrombophlebitis) will also be prolonged, usually in the range of one and one half to two times the normal PT time.")
32
Temps de coagulation d’un PPP
Citrate / PPP FT (thromboplastine… ) Ca2+ Reflète le temps requis pour générer IIa Ia / « voie extrinsèque » 10-15 sec
 Ca2+ Reflète le temps requis pour générer IIa Ia / « voie extrinsèque » sec.")
33
Temps de Quick (TP) VII X V II I
The PT test is used to monitor patients taking certain medications as well as to help diagnose clotting disorders. A sample of the patient's blood is obtained by venipuncture. The blood is decalcified (by collecting it into a tube with oxalate or citrate ions) to prevent the clotting process from starting before the test. The blood cells are separated from the liquid part of blood (plasma) by centrifugation. The PT test is performed by adding the patient's plasma to some source of Tissue Factor (e.g.: a protein, thromboplastin, from homogenized brain tissue) that converts prothrombin to thrombin. The mixture is then kept in a warm water bath at 37°C for one to two minutes. Calcium chloride (excess quantities of ionized calcium) is added to the mixture in order to counteract the sodium citrate and allow clotting to start. The test is timed from the addition of the calcium chloride until the plasma clots. This time is called the Prothrombin Time The prothrombin test specifically evaluates the presence of factors VII, V, and X, prothrombin, and fibrinogen. A prothrombin time within the second range (depends on the source of thromboplastin used) indicates that the patient has normal amounts of the above clotting factors. A prolonged prothrombin time indicates a deficiency in any of factors VII, X, V, prothrombin, or fibrinogen. It may mean that the patient has a vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II (prothrombin), VII, IX and X) or a liver disease (the liver is the site of synthesis of the plasma protein factors). The prothrombin time of patients receiving a vitamin K-competing coumarin drug such as warfarin (anticoagulation therapy used in deep venous thrombophlebitis) will also be prolonged, usually in the range of one and one half to two times the normal PT time. Perhaps because there are fewer steps in the sequence or because factor VII circulates in the highest concentration of any factor, the PT is relatively resistant to change, typically requiring single-factor levels to fall to 10% of normal or less before becoming prolonged. As seen in Figure 1 , there is only a single factor unique to this pathway, and selective factor VII deficiency is the only way the PT can be prolonged without impacti ng the aPTT. Because the sensitivity of reagen ts varies between laboratories and sometimes even within a hospital over time, PT is referenced to an international standard (the international normalized ratio [INR]). 1
 to prevent the clotting process from starting before the test. The blood cells are separated from the liquid part of blood (plasma) by centrifugation. The PT test is performed by adding the patient s plasma to some source of Tissue Factor (e.g.: a protein, thromboplastin, from homogenized brain tissue) that converts prothrombin to thrombin. The mixture is then kept in a warm water bath at 37°C for one to two minutes. Calcium chloride (excess quantities of ionized calcium) is added to the mixture in order to counteract the sodium citrate and allow clotting to start. The test is timed from the addition of the calcium chloride until the plasma clots. This time is called the Prothrombin Time. The prothrombin test specifically evaluates the presence of factors VII, V, and X, prothrombin, and fibrinogen. A prothrombin time within the second range (depends on the source of thromboplastin used) indicates that the patient has normal amounts of the above clotting factors. A prolonged prothrombin time indicates a deficiency in any of factors VII, X, V, prothrombin, or fibrinogen. It may mean that the patient has a vitamin K deficiency (vitamin K is a co-factor in the synthesis of functional factors II (prothrombin), VII, IX and X) or a liver disease (the liver is the site of synthesis of the plasma protein factors). The prothrombin time of patients receiving a vitamin K-competing coumarin drug such as warfarin (anticoagulation therapy used in deep venous thrombophlebitis) will also be prolonged, usually in the range of one and one half to two times the normal PT time. Perhaps because there are fewer steps in the sequence or because factor VII circulates in the highest concentration of any factor, the PT is relatively resistant to change, typically requiring single-factor levels to fall to 10% of normal or less before becoming prolonged. As seen in Figure 1 , there is only a single factor unique to this pathway, and selective factor VII deficiency is the only way the PT can be prolonged without impacti ng the aPTT. Because the sensitivity of reagen ts varies between laboratories and sometimes even within a hospital over time, PT is referenced to an international standard (the international normalized ratio [INR]). 1.")
34
International Normalised Ratio (INR)
Le TQ exprimé en % du rapport M/T (TP) Echelle de temps / « indexe TRT étroit » / hétérogénéité des thrombolastines limite dans l’interprétation Standardisation (ISI) INR. Traitement AVK +++
 Echelle de temps / « indexe TRT étroit » / hétérogénéité des thrombolastines limite dans l’interprétation. Standardisation (ISI) INR. Traitement AVK +++")
35
Traitement par AVK précoce de PC / PS
½ vie (h) 7 24 48 60 Facteurs VII IX X II précoce de PC / PS Wheeler AP, Chest 2010
 Facteurs. VII. IX. X. II. précoce de PC / PS. Wheeler AP, Chest")
36
Temps de coagulation d’un PPP
Citrate / PPP Thrombine Ca2+ Reflète le temps requis pour I Ia sec

37
Temps de Thrombine

39
Dosage spécifique (test fonctionnel ou Ig)
PDF / D-Dimères ….

40
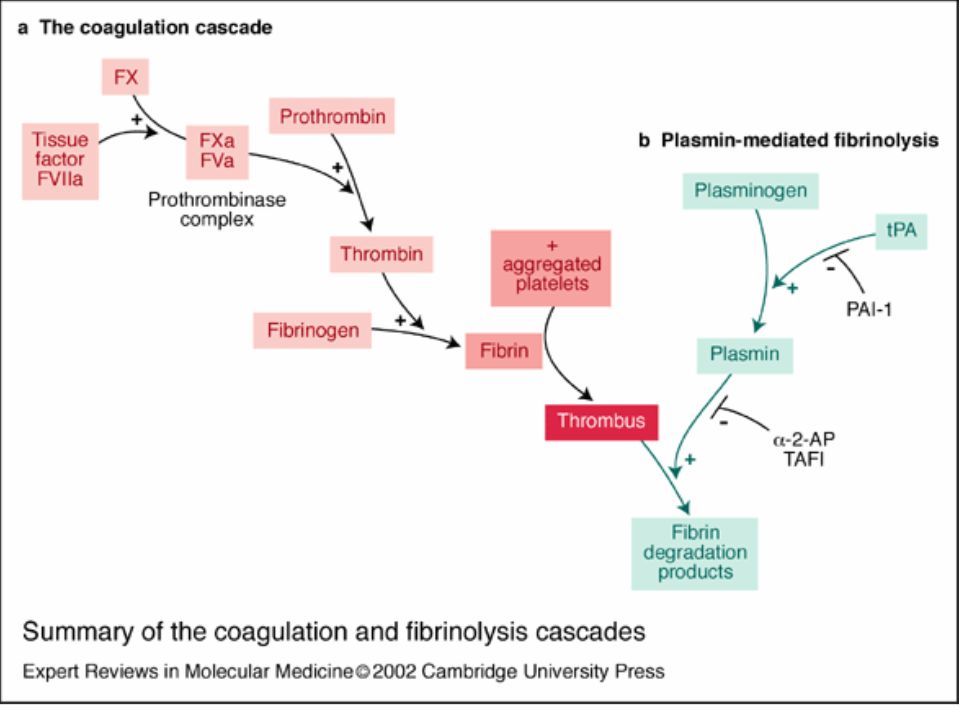
Fibrinolysis Enzymatic degradation of fibrin
Begins within a few hours of fibrin polymerization and stabilization Tracks at pace of wound healing Primary protease = plasmin Catalytic product of plasminogen activation Fibrin degradation products (FDPs) X Y D E D-D = D-dimer
 X. Y. D. E. D-D = D-dimer.")
42
Gando S, Crit Care Med 2006

43
Bakhtiari, K Crit Care Med 2004

44
Dosage spécifique (test fonctionnel ou Ig)
PDF / D-Dimères …. Facteurs de coagulation I II / V / VII / X PC / AT TCA M+T (>15%) VIII / IX / XI XII /
 VIII / IX / XI. XII /")
45
Test de coagulation VII activation / phase contact
thromboplastine tissulaire (FT) INTRINSEQUE EXTRINSEQUE XII XI IX VIII VII TCA 25-35 sec 10-15 sec TP X V II I TRONC COMMUN TRONC COMMUN Fibrine
 INTRINSEQUE. EXTRINSEQUE. XII. XI. IX. VIII. VII. TCA sec sec. TP. X. V. II. I. TRONC. COMMUN. TRONC. COMMUN. Fibrine.")
46
Test de coagulation TCA TP X V II I M/T > 1,35 TP < 70% tronc
Levi M Crit Care 2006 TCA M/T > 1,35 TP < 70% TP X V II I tronc commun Fibrine

47
Test de coagulation activation / phase contact XII XI IX VIII TP TCA
INTRINSEQUE XII XI IX VIII TP TCA M/T > 1,35 > 70% Levi M Crit Care 2006

48
Test de coagulation VII thromboplastine tissulaire (FT) TCA 25-35 sec
EXTRINSEQUE VII TCA 25-35 sec < 70% TP Levi M Crit Care 2006

50
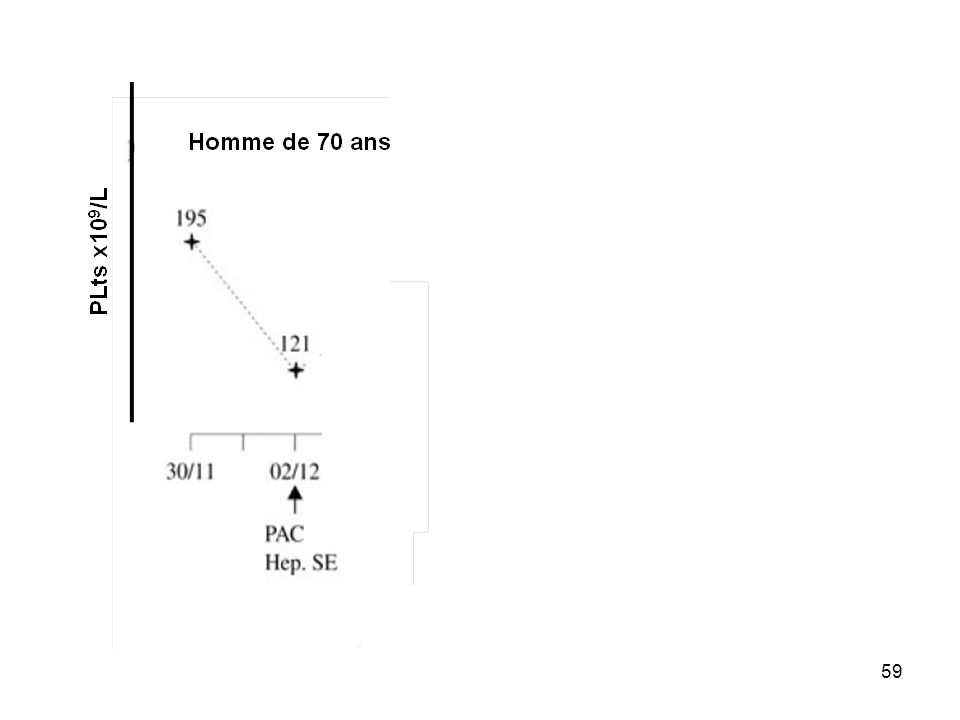
Homme de 77 ans traité au long cours par IEC pour une HTA
Admis le 4 déc pour nécrose antérieure étendue, angioplastie et anticoagulants + antiagrégants

51
2 1 Thrombopénie NP > 50 % ou NP entre 20 et 100 gigas /L NP entre 30 et 50 % ou NP entre 10 et 20 gigas /L Absence de NP ou NP < 10 gigas /L Délai de survenue 5-10 j après introduction d’une héparine ou dans les 24 h si héparinothérapie < 30 j >10 j après introduction d’une héparine ou dans les 24 h si héparinothérapie entre j Autre condition Thrombose Nouvelle thrombose, réaction systémique, nécrose cutanée Extension ou rechute d’une thrombose Aucun signe Diagnostic alterne Aucun Possible certain

52
X 5 x 109 /L X J 3 X hémorragie 1 4Ts = 1

53
Homme de 77 ans traité au long cours par IEC pour une HTA
Admis le 4 déc pour nécrose antérieure étendue, angioplastie et anticoagulants + antiagrégants PLts x109/L

54
Reopro Homme de 77 ans traité au long cours par IEC pour une HTA
Admis le 4 décembre pour nécrose antérieure étendue, angioplastie et anticoagulants + antiagrégants PLts x109/L Remontent en 15 j en moyenne ne contre indiquent pas l’administration ultérieure de Réopro (Cas 19) Reopro
 Reopro.")
55
Réaction Immunologique HNF > HBPM (?) chir > médecine (PF4)
NP (HIT) +/- thromboses (HITT) Thromboses artère / veine Territoire Facteur déclenchant Incidence 1-5% CCV M/S ICU (O,2-0,4%) J5-J10 dès J1 si expo préalable HIT risque de thromboses sans TRT = 20% DC si HITT 20% HIT risque de thrombose si arrêt du trt et pas de DNP curatif 50% HITT à M1 avec mortalité de HITT dans séries = 20%, morbidité ++++ *:Kelleng S, Semininars in Thrombosis and Hemostais 2008
 +/- thromboses (HITT) Thromboses artère / veine. Territoire. Facteur déclenchant. Incidence. 1-5% CCV. M/S ICU (O,2-0,4%) J5-J10 dès J1 si expo préalable. HIT risque de thromboses sans TRT = 20% DC si HITT 20% HIT risque de thrombose si arrêt du trt et pas de DNP curatif 50% HITT à M1 avec mortalité de HITT dans séries = 20%, morbidité ++++ *:Kelleng S, Semininars in Thrombosis and Hemostais")
56
Thrombocytopaenia is the lesser concern, Bleeding is very uncommon
Thrombosis is often severe and life-threatening, Venous thrombi more common except in pts with underlying arterial vascular disease, Mortality ~20%, Limb amputation ~10% % of patients will develop thrombosis on cession of heparin if alternate anticoagulation is not initiated J5-J10 de l’exposition pic jusqu’à J20, plus tôt si exposition préalable; + fqt avec HNF que HBPM mais entraîne exclusuion des héparines. Baisse des Plts avec Thoses veineuses et artérielles dans territoires diff et avec facteur favorisant : lésion vasculaire Survenue de thoses sous HNF ou HBPM Rare mais potentiellement grave Dès suspicion arrêt de l’HNF et débuter DNP pas d’avk en phase aiguë, HIT 1-2% >30% HITT

57
Il faut / il est recommandé
TIH Accord fort Il faut / il est recommandé Accord faible Il faut probablement Si HNF ou HBPM : NP à l’initiation ou à H24 Et NP bihebdomadaire les 3ères semaines Utiliser le score 4T pour évaluer le degré de susispicion de TIH Si exposition à une héparine 3 mois, NP à l’initiation de l’héparinothérapie et à H24 RFE Thrombopénie, SRLF Janvier 2011

58
Pre-test probality of HIT, 4T score
Among 111 patients with low pre-test probability; one had HIT (0.9%) Intermediate scores: 11.4% with HIT High scores: 34% with HIT Lo GK, Julh D, Warkentin TE, et al. Evaluation of pretest clinical score (4 T’s) for the diagnosis of heparin-induced thrombocytopenia in two clinical settings. J Thromb Haemost 2006. Lo GK, J Thromb Haemost 2006
 Intermediate scores: 11.4% with HIT. High scores: 34% with HIT. Lo GK, Julh D, Warkentin TE, et al. Evaluation of pretest clinical score (4 T’s) for the diagnosis of heparin-induced thrombocytopenia in two clinical settings. J Thromb Haemost Lo GK, J Thromb Haemost")
60
4Ts > 5 Plts >50% et > 20x109/L J5-J10 Thrombose
Autre diagnostic 2 1 4Ts > 5

61
Attitude diagnostique

62
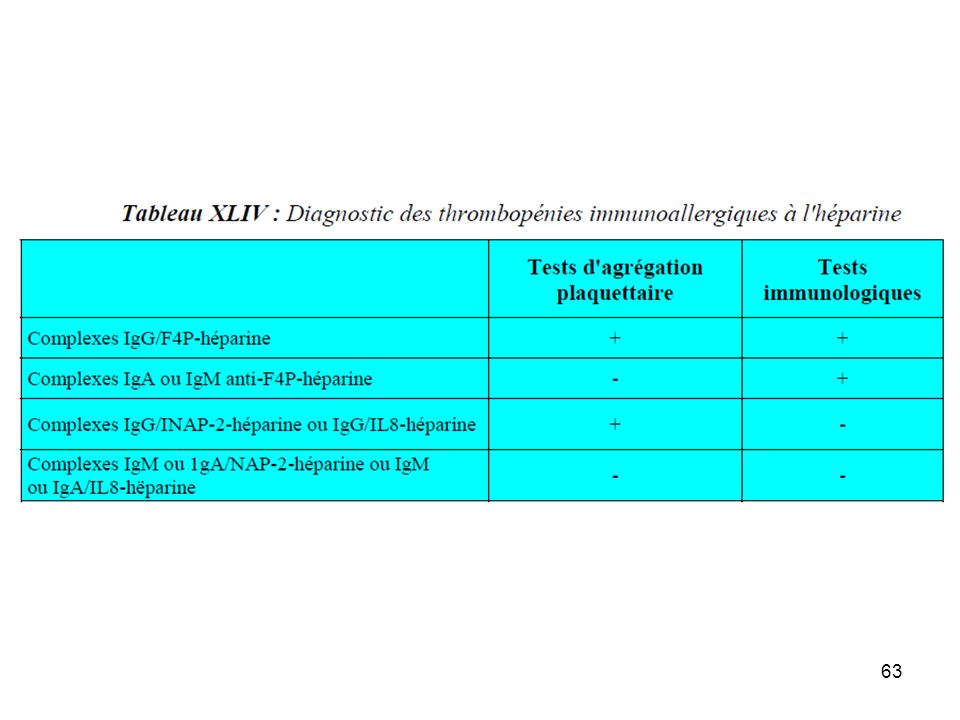
Salicylate IPP Tests fonctionnels et ELISA

65
Tests biologiques diagnostiques
ELISA anti F4P (Se >97%, Sp =74-86%) FP >50% post CCV FP : 10% patients médicaux Tests fonctionnels (Se = SP > 95%)
 FP >50% post CCV. FP : 10% patients médicaux. Tests fonctionnels (Se = SP > 95%)")
66
Il faut / il est recommandé
TIH Accord fort Il faut / il est recommandé Accord faible Il faut probablement Si HNF ou HBPM : NP à l’initiation ou à H24 Et NP bihebdomadaire les 3ères semaines Utiliser le score 4T pour évaluer le degré de susispicion de TIH Si exposition à une héparine 3 mois, NP à l’initiation de l’héparinothérapie et à H24 Si score 4T<2 : pas de test de TIH Si test bio pour suspicion de TIH combiner test fonctionnel + ELISA RFE Thrombopénie, SRLF Janvier 2011

67
Arepally G, N Engl J Med 20

68
combiner les deux tests
Stop héparines danaparoïde combiner les deux tests RFE Thrombopénie, SRLF Janvier 2011

69
Attitude diagnostique
Attitude thérapeutique Créatininémie Fonction hépatique

70
Il faut / il est recommandé
TIH Accord fort Il faut / il est recommandé Accord faible Il faut probablement Utiliser le score 4T pour évaluer le degré de susispicion de TIH Si score 4T 4, substituer immédiatement l’héparine par Orgaran®, Refludan®, voire Angiox® à posologie curative Si score 4T<2 : pas de test de TIH Si test bio pour suspicion de TIH combiner test fonctionnel + ELISA Si ATCD de TIH : proscrire HNF et HBPM et utiliser le Danaparoïde comme anticoagulant en 1ère intention Si score 4T 4 arrêt de l’héparine Pas de Fondaparinux à la phase aiguë de la TIH RFE Thrombopénie, SRLF Janvier 2011

71
Salicylate IPP

72
Hirsh J, Arch Intern Med 2004

74
Stephen M, J Crit Care 2009

75
TIH Rare (très rare hors CCV) Ne pas méconnaître
Ne pas attribuer par excès : 4Ts Diagnostic TRT substitutif Prévention secondaire

76
Insuffisance hépatique
TCA / TP / TT / Fg / Plts D-Dimères – PDF / Cofacteurs II / V / VII / X TCA M+T, cofacteurs VIII / IX / XI Désordres hémostatiques acquis +++ Multiples étiologies Impact des traitements Hypovitaminose K Etiologies Fibrinolyse LA / SCAP CIVD Insuffisance hépatique DTI / Héparine

77
Wheeler AP, Chest 2010

78
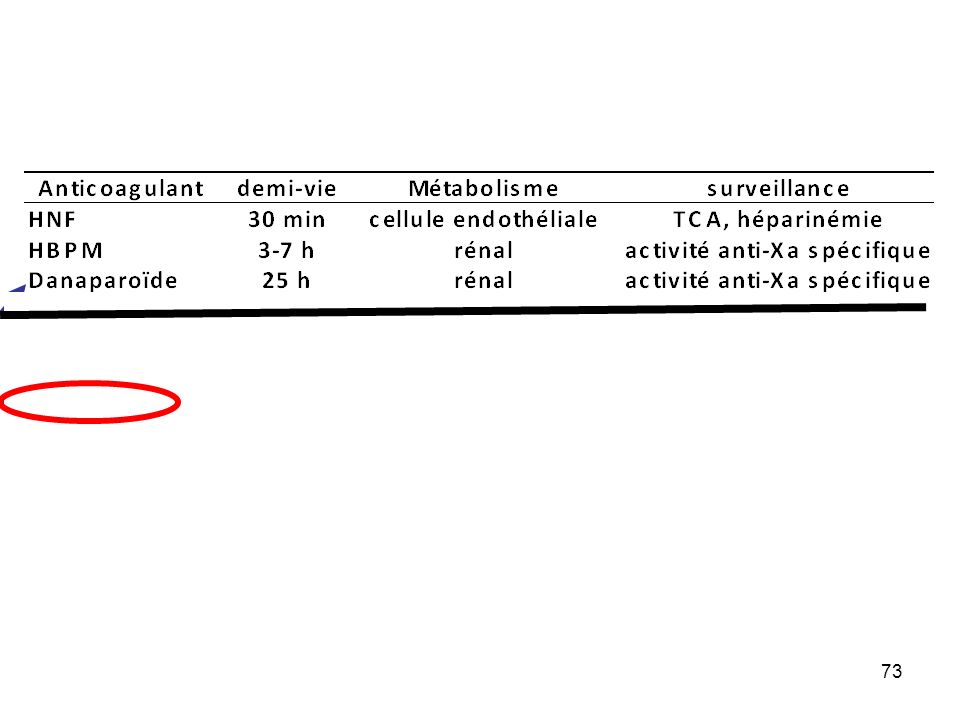
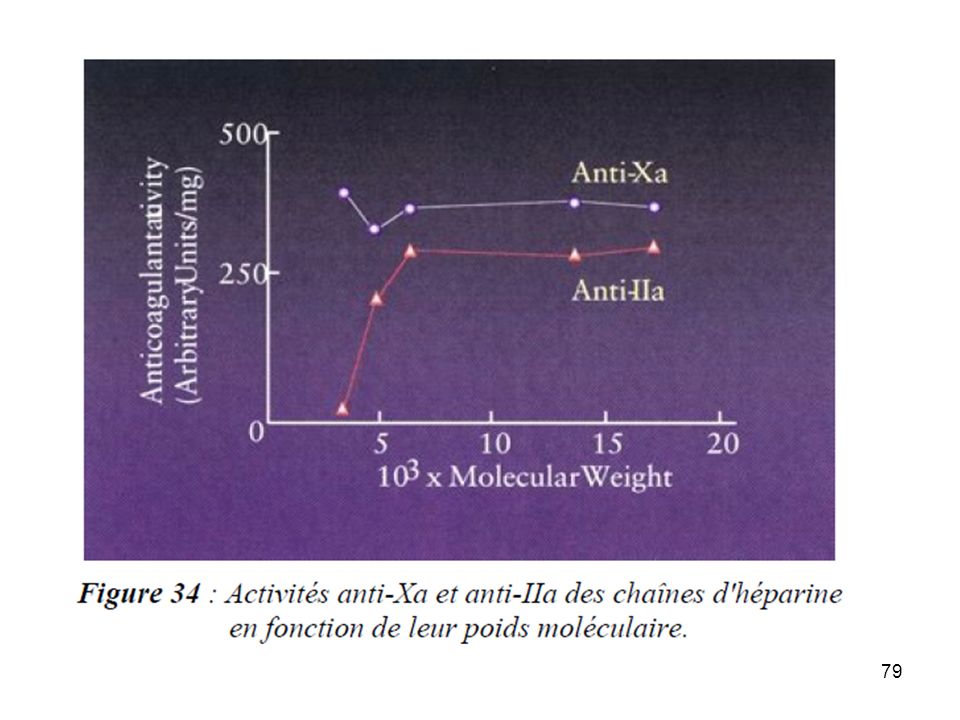
Traitement héparinique
TCA : mauvais test surtout en réanimation I VIII RAC HBPM ! Résistance à l’héparine ? Problème de dosage (TCA) Grossièrement : TCA = 1,5-2 x T activité anti-Xa (0,3-0,7 UI/L) DFG : Activité anti-Xa some PT assay systems contain a heparinneutralizing compound, and in assays that do not remove heparin, heparin interacts with more components of the contact activation pathway than the tissue factor pathway. The aPTT is not an ideal monitoring tool for heparinoids because it is subject to numerous nonheparin infl uences. For example, many acute phase reactants, includ ing fi brinogen, can bind and neutralize UFH. In addition, factor VIII is not only an acute phase reactant, but also shortens the aPTT in vitro , occasionally leading clinicians to conclude that patients are resistant to the effects of UFH. the appearance of heparin resistance is much more likely to be the result of inadequate dosing or nonspecific acute phase reactants than from antithrombin defi ciency. 37 Although there is some variation by laboratory, the typical aPTT target is 1.5 to 2.5 times the average normal aPTT and roughly corresponds to an anti-Xa level of 0.3 to 0.7 units/mL. Wheeler AP, Chest 2010
 Grossièrement : TCA = 1,5-2 x T activité anti-Xa (0,3-0,7 UI/L) DFG : Activité anti-Xa. some PT assay systems contain a heparinneutralizing compound, and in assays that do not remove heparin, heparin interacts with more components of the contact activation pathway than the tissue factor pathway. The aPTT is not an ideal monitoring tool for heparinoids because it is subject to numerous nonheparin infl uences. For example, many acute phase reactants, includ ing fi brinogen, can bind and neutralize UFH. In addition, factor VIII is not only an acute phase reactant, but also shortens the aPTT in vitro , occasionally leading clinicians to conclude that patients are resistant to the effects of UFH. the appearance of heparin resistance is much more likely to be the result of inadequate dosing or nonspecific acute phase reactants than from antithrombin defi ciency. 37. Although there is some variation by laboratory, the typical aPTT target is 1.5 to 2.5 times the average normal aPTT and roughly corresponds to an anti-Xa level of 0.3 to 0.7 units/mL. Wheeler AP, Chest")
82
Anticoagulants injectables en réanimation = héparines
Héparine non fractionnée (HNF) Sodée IV Calcique S/C Héparines de bas poids moléculaire (HBPM) S/C (mais aussi IV…) Faible dose « prophylactique » HNF : UI/kg, HBPM standard, si IMC > 35 : 50 UI/kg (?) Dose élevée « curative » HNF : 80 UI/kg bolus + 18UI/kg/h HBPM : 200 UI/kg en une ou deux injections
 Sodée IV. Calcique S/C. Héparines de bas poids moléculaire (HBPM) S/C (mais aussi IV…) Faible dose « prophylactique » HNF : UI/kg, HBPM standard, si IMC > 35 : 50 UI/kg ( ) Dose élevée « curative » HNF : 80 UI/kg bolus + 18UI/kg/h. HBPM : 200 UI/kg en une ou deux injections.")
83
Efficacité biologique de l’HNF
Efficacité biologique héparinémie Activité anti-IIa ou anti-Xa, par défaut : TCA Objectif thérapeutique Faible dose : pas de surveillance (anti-Xa entre 0,1 et 0,4 UI/L, TCA < 1,5xT) Forte dose : anti-Xa entre 0,4 - 0,7 UI/L au pic et < 0,4 UI/L en vallée anti-IIa entre 0,2 et 0,4 UI/L ou TCA correspondant (1,5 à 2,5xT) HNF calcique : à mi-course entre deux injections HNF sodée : PSE ( > 4-6 h après modification de posologie)
 Forte dose : anti-Xa entre 0,4 - 0,7 UI/L au pic et < 0,4 UI/L en vallée. anti-IIa entre 0,2 et 0,4 UI/L. ou TCA correspondant (1,5 à 2,5xT) HNF calcique : à mi-course entre deux injections. HNF sodée : PSE ( > 4-6 h après modification de posologie)")
84
Efficacité biologique des HBPM
Efficacité biologique : héparinémie Activité anti-Xa spécifique Objectif thérapeutique Faible dose : pas de surveillance (anti-Xa entre 0,1 et 0,4 UI/L) Forte dose : Administration biquotidienne anti-Xa entre 0,4 - 1 UI/L au pic et < 0,4 UI/L en vallée Administration unique quotidienne Anti-Xa entre 1 et 2 UI/L au pic et <0,4 UI/L en vallée HBPM Pic H+4 de l’injection sous cutanée
 Forte dose : Administration biquotidienne. anti-Xa entre 0,4 - 1 UI/L au pic et < 0,4 UI/L en vallée. Administration unique quotidienne. Anti-Xa entre 1 et 2 UI/L au pic et <0,4 UI/L en vallée. HBPM. Pic H+4 de l’injection sous cutanée.")
85
Anticoagulation injectable en réanimation = héparinothérapie
HBPM élimination rénale risque d’accumulation (hémorragie ++) si IR à forte dose (curatif) HBPM contre-indiqués si clairance créat < 20 ml/min à faible dose (préventif)
 si IR. à forte dose (curatif) HBPM contre-indiqués si clairance créat < 20 ml/min. à faible dose (préventif)")
86
Serial anti-factor Xa testing levels following 5,000 U of subcutaneous dalteparin prophylaxis
Maximal peak value Cook D, Cur Op Crit Care 2009

87
Bioaccumulation was defined by a trough anti-Xa level > 0.4 IU/mL
Multicenter single arm study in ICU patients with creatinine clearance < 30 mL/min Bioaccumulation was defined by a trough anti-Xa level > 0.4 IU/mL 136 patients included with a mean creatinine clearance of 18 mL/min Douketis J Arch Intern Med 2008

88
Douketis J Arch Intern Med 2008

89
Douketis J Arch Intern Med 2008

90
inhibiteurs directs de la thrombine
Anti II : TCA +++ (1,5 – 3 x T) argatropan (foie) hirudine, lipérudine, bvalirudine Fandaparinux (pas en réa cf ½ vie), ACT (!) bivalirudine some PT assay systems contain a heparinneutralizing compound, and in assays that do not remove heparin, heparin interacts with more components of the contact activation pathway than the tissue factor pathway. The aPTT is not an ideal monitoring tool for heparinoids because it is subject to numerous nonheparin infl uences. For example, many acute phase reactants, includ ing fi brinogen, can bind and neutralize UFH. In addition, factor VIII is not only an acute phase reactant, but also shortens the aPTT in vitro , occasionally leading clinicians to conclude that patients are resistant to the effects of UFH. the appearance of heparin resistance is much more likely to be the result of inadequate dosing or nonspecific acute phase reactants than from antithrombin defi ciency. 37 Although there is some variation by laboratory, the typical aPTT target is 1.5 to 2.5 times the average normal aPTT and roughly corresponds to an anti-Xa level of 0.3 to 0.7 units/mL. Wheeler AP, Chest 2010
 argatropan (foie) hirudine, lipérudine, bvalirudine. Fandaparinux (pas en réa cf ½ vie), ACT (!) bivalirudine. some PT assay systems contain a heparinneutralizing compound, and in assays that do not remove heparin, heparin interacts with more components of the contact activation pathway than the tissue factor pathway. The aPTT is not an ideal monitoring tool for heparinoids because it is subject to numerous nonheparin infl uences. For example, many acute phase reactants, includ ing fi brinogen, can bind and neutralize UFH. In addition, factor VIII is not only an acute phase reactant, but also shortens the aPTT in vitro , occasionally leading clinicians to conclude that patients are resistant to the effects of UFH. the appearance of heparin resistance is much more likely to be the result of inadequate dosing or nonspecific acute phase reactants than from antithrombin defi ciency. 37. Although there is some variation by laboratory, the typical aPTT target is 1.5 to 2.5 times the average normal aPTT and roughly corresponds to an anti-Xa level of 0.3 to 0.7 units/mL. Wheeler AP, Chest")
91
ACT

92
Principe du temps d'écarine.
Activated coagulation time (ACT) - blood drown w/o anticoagulant is transferred to the tube with contact activator (silica or kaolin) and mixed at 37oC until coagulum is present (normal about 150 s). - Routine use for the heparinization control of extracorporeal circulation or hemodialysis (required s; heart surgery > 600 s) Principe du temps d'écarine. La prothrombine est transformée par l'écarine en meizothrombine qui s'autocatalyse en alpha-thrombine. Cette réaction se fait en l'absence de phospholipides et d'ions calcium.
 - blood drown w/o anticoagulant is transferred to the tube with contact activator (silica or kaolin) and mixed at 37oC until coagulum is present (normal about 150 s). - Routine use for the heparinization control of extracorporeal. circulation or hemodialysis (required s; heart surgery > 600 s) Principe du temps d écarine. La prothrombine est transformée par l écarine en meizothrombine qui s autocatalyse en alpha-thrombine. Cette réaction se fait en l absence de phospholipides et d ions calcium.")
93
2 assays for separate applications

94
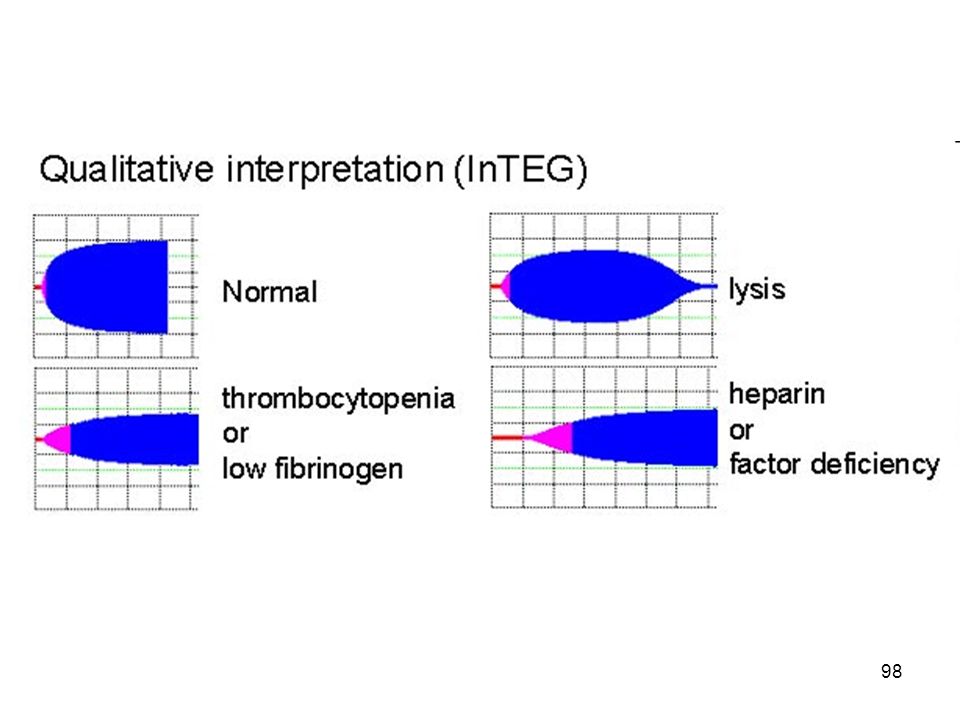
TEG

97
the Alfa & K parameters Indicate the speed of the aggregation fibrin-platelets.

Présentations similaires