Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Serge BRACARD CHU Nancy 2009
Place de la Radiologie dans le traitement des AVC ischémiques: La revascularisation cérébrale Serge BRACARD CHU Nancy 2009

2
Plan Techniques Indications Organisation

3
Techniques Thrombolyses chimiques Thrombolyses mécaniques Associations
Thrombolyse IV Thrombolyse IA Thrombolyse IV + IA Anti Gp IIb-IIIa Thrombolyses mécaniques Associations

4
Résultats Taux de reperméabilisation % parenchyme sauvé
concept: la restauration du flux permet les conditions favorables à la récupération… % parenchyme sauvé Résultats cliniques Complications

6
Augmentation de la pénétration du thrombolytique dans le thrombus par application trans-crânienne d’ultrasons CLOTBURST 126 Patients rTpa IV Randomisation +/- ultra-sons (DTC continu 2 MHz) Reperméabilisation 49% versus 30% Pas de différence sur la récupération clinique Alexandrov NEJM 2004,351,2170-8 Intérêt des microbulles Molina stroke 2006,37, MUST (Microbubbles and Ultrasound in Stroke Study) Etude multicentrique, française (PHRC), contrôlée, randomisée Occlusions M1, alteplase iv <3h vs alteplase + Doppler transcrânien + microbulles iv < 3h Augmentation du risque hémorragique ?
 Reperméabilisation 49% versus 30% Pas de différence sur la récupération clinique Alexandrov NEJM 2004,351, Intérêt des microbulles Molina stroke 2006,37, MUST (Microbubbles and Ultrasound in Stroke Study) Etude multicentrique, française (PHRC), contrôlée, randomisée. Occlusions M1, alteplase iv <3h vs alteplase + Doppler transcrânien + microbulles iv < 3h. Augmentation du risque hémorragique")
7
Thrombolyse IA: PROACT II
180 patients avec occlusion ACM < 6h R-proUK IA + héparine vs héparine Pas de thrombolyse mécanique R-proUK + héparine Héparine TIMI 2-3 >2h 66% 27% TIMI 3 > 2h 19% 2% mRs 0-2 à 3 mois 40% 25% ICH sympto 10% Door to ia treatment time : 5,3 h

8
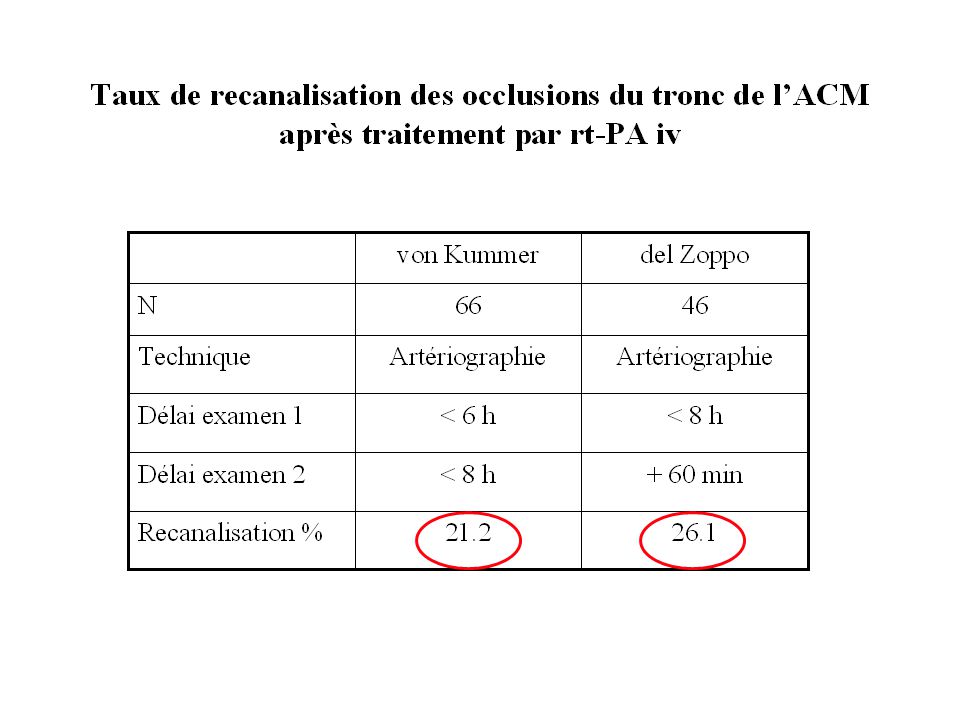
Recanalisation

9
Association IV +IA IA est plus efficace en termes de reperméabilisation mais nécessite 1h pour sa mise en route IV est moins efficace mais plus rapide à mettre en œuvre IV +IA devrait associer les bénéfices des deux…

10
Interventional Management Study (IMS)
Rt-PA iv 0.45 mg/kg < 3 h + ia 22 mg en 2 h 80 patients Seulement 5% des patients étaient recanalisés après traitement iv Injection dans thrombus TIMI 3 : 11% TIMI 2-3 : 56% Délai traitement ia : 217+/-46.7 min

11
Interventional Management Study II (IMS II)
Rt-PA iv 0.6 mg/kg < 3 h + ia 22 mg en 2 h 76 patients Injection dans thrombus + sonde à ultrasons EKOS TIMI 2-3 : 69% Récupération, mortalité= NINDS Interventional Management Study III (IMS III) IV vs IV+IA+ EKOS ou MERCI (en cours)
 IV vs IV+IA+ EKOS ou MERCI (en cours)")
12
Exposition de thrombine
Association de produits avec des cibles différentes Thrombus rt-PA Fibrinolyse Exposition de thrombine Activation plaquettaire Anti-GP IIb-IIIa Thrombus fibrino-plaquettaire Libération PAI-1

13
En cardiologie: TIMI 14 Traitement TIMI 3 % (90 min)
Hémorragie majeure % Alteplase 100 mg 57 6 Abciximab 32 3 SK faible + abciximab 34 10 SK fort + abciximab 46 Alteplase 50 mg+ abciximab 77 7 (1) Rien n’est démontré en neurologie…
 Rien n’est démontré en neurologie…")
14
Efficacité: taux de reperméabilisation
Variable rTpa IV seul d’autant plus efficace que l’occlusion est distale insuffisant pour les « gros troncs » rTpa IA plus efficace Associations +++ Limite actuelle : 60-70%

15
Efficacité :Résultats cliniques
Study N Fibrinolytic Time window Mortality ________________ Active Placebo Rankin 0-1 _______________ Active Placebo ECASS 620 rt-PA- 1.1 mg/kg 6 h 17.9%£ %£ (14.6%) (11.7%) 22.4%££ %££ (19.4%) (14.8%) 0 difference (0 difference) NINDS 624 rt-PA – 0.9 mg/kg 3 h 17%££ %££ + 13% ECASS II 800 10.3%££ %££ 54,3%* ,1% ATLANTIS 547 3-5 h 11%££ %££ 36% % SK: Streptokinase; UK: Urokinase; rt-PA: recombinant tissue plasminogen activator; : intent-to-treat population, ( ): target population (intent-to-treat population less protocol violations); ECASS II : analyse post hoc ( but initial: Rankin 0, pas de différence)
 (11.7%) 22.4%££ 15.8%££ (19.4%) (14.8%) 0 difference. (0 difference) NINDS rt-PA – 0.9 mg/kg. 3 h. 17%££ 21%££ + 13% ECASS II %££ 10.5%££ 54,3%* 46,1% ATLANTIS h. 11%££ 6.9%££ 36% 34% SK: Streptokinase; UK: Urokinase; rt-PA: recombinant tissue plasminogen activator; : intent-to-treat population, ( ): target population (intent-to-treat population less protocol violations); ECASS II : analyse post hoc ( but initial: Rankin 0, pas de différence)")
16
Méta analyses Nombre de malades Mort (OR) Mort ou dépendance
Tous les essais 5216 1,31 0,83 rt-Pa < 6h 2688 1,24 0,79 rt-Pa < 3h 869 0,95 0,55

17
Study N Fibrinolytic Time window Mortality ________________ Active Placebo Symptomatic ICH _______________ Active Placebo MAST-E 310 SK M 6 h 34%* %* 45%§ %§ 21%* %* MAST-I 622 Aspirin 27%* %* 36%$ %$ 8% % ASK 340 4 h 36%££ %££ 12.6% % ECASS 620 rt-PA- 1.1 mg/kg 17.9%£ %£ (14.6%) (11.7%) 22.4%££ %££ (19.4%) %) 19.8%£ %£ (19.4%) (6.8%) NINDS 624 rt-PA – 0.9 mg/kg 3 h 17%££ %££ 6.4% % ECASS II 800 10.3%££ %££ 8.8% % ATLANTIS 547 3-5 h 11%££ %££ 7% % PROACT II 180 IA Pro-UK 25%££ %££ 10% % Cleveland group 54 IA UK 24%££ 17% SK: Streptokinase; UK: Urokinase; rt-PA: recombinant tissue plasminogen activator; IA: intra-arterial;*: at day 10; § : at day 108; $: at 6 months; : intent-to-treat population, ( ): target population (intent-to-treat population less protocol violations); £ at 1 month; ££: at 3 months; : no placebo group; only PROACT II and the Cleveland group’s study evaluated intra-arterial thrombolysis while the other studies reported in this table evaluated intravenous thrombolysis.
 (11.7%) 22.4%££ 15.8%££ (19.4%) 14.8%) 19.8%£ 6.5%£ (19.4%) (6.8%) NINDS rt-PA – 0.9 mg/kg. 3 h. 17%££ 21%££ 6.4% 0.6% ECASS II %££ 10.5%££ 8.8% 3.4% ATLANTIS h. 11%££ 6.9%££ 7% 1.1% PROACT II IA Pro-UK. 25%££ 27%££ 10% 2% Cleveland group 54. IA UK. 24%££ - 17% - SK: Streptokinase; UK: Urokinase; rt-PA: recombinant tissue plasminogen activator; IA: intra-arterial;*: at day 10; § : at day 108; $: at 6 months; : intent-to-treat population, ( ): target population (intent-to-treat population less protocol violations); £ at 1 month; ££: at 3 months; : no placebo group; only PROACT II and the Cleveland group’s study evaluated intra-arterial thrombolysis while the other studies reported in this table evaluated intravenous thrombolysis.")
19
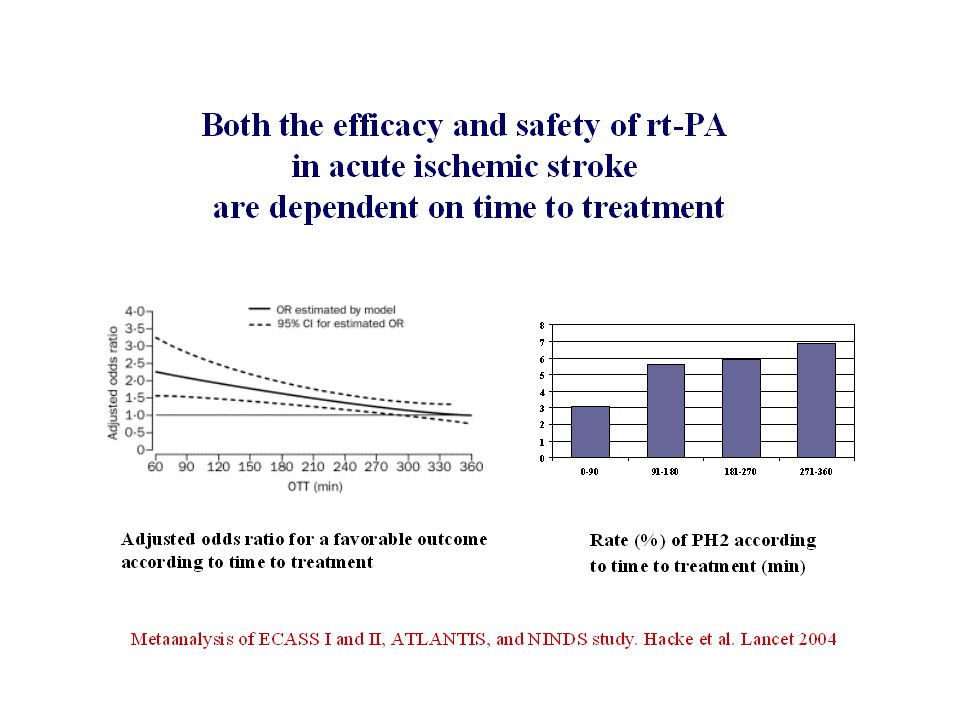
Thrombolyse IV: délai de 3h?
Délai légal AMM Méta analyse Hacke 2004 bénéfice au delà? ECASS III: efficacité entre 3 et 4h30 821 patients rTpa vs placebo Rankin 0-1 à 90 jours: 52,4% vs 45,2% p=0,04 Hémorragies symptomatiques: 2,4 vs 0,12 p=0,008 Mortalité: 7,66 vs 8,44% Hacke NEJM 2008,359, 1317 EPITHET Thrombolyse IV 3-6h chez des patients avec un mismatch en IRM. A 3 mois volume infarctus non diminué mais pronostic meilleur Davis Lancet neurol 2008, 7,

20
PROACT II - Patients

21
Intracranial hemorrhage

22
90-day Modified Rankin Outcome
control 25% 41% 34% 40% 26% 35% rProUK P=0,043

23
Autres études Urokinase: rTpa MELT Iv vs IA nancy
Ogawa Stroke 2007,38, 2633 Iv vs IA nancy Ducrocq 2005 J of Neuroradiology Etude cas témoin (mRs 0-2: 50,5 vs 34%) Inoue cerebrovasc dis 2005 rTpa Études observationnelles
 Inoue cerebrovasc dis rTpa. Études observationnelles.")
24
IV ou IA Pas d’étude randomisée importante
Etude de 83 patients avec une ACM hyperdense Thrombolyse IV: meilleur pronostic avec IV si pas de MCA hyperdense Thrombolyse IA: pas de différence Agarwal Cerebrovas Dis 2004, 17, 182

25
Association IV+IA: rt-PA iv 0.45 mg/kg < 3 h + ia 22 mg en 2 h

26
Efficacité sur le plan clinique
Limite actuelle: 40% de patients autonomes à 3 mois - IV Toutes occlusions confondues - IA et associations : sur les « gros troncs »

27
FACTEURS PRONOSTIQUES
CIRCULATION COLLATERALE DELAI TOPOGRAPHIE

28
VALEUR PREDICTIVE du CBF
CBF >55% : récupérable > 6 heures CBF > 35%: récupérable < 6 heures CBF< 35% : Résultats ? Risques d’hémorragie Ueda, J Cereb Blood Flow Metab 1999,19,99-108

29
Thrombolyse: localisations
Other factors: NIHSS <20, LIT started <4h Gonner F Stroke 1998,29,

31
Thrombolysis - results

32
IU IU IU J7

34
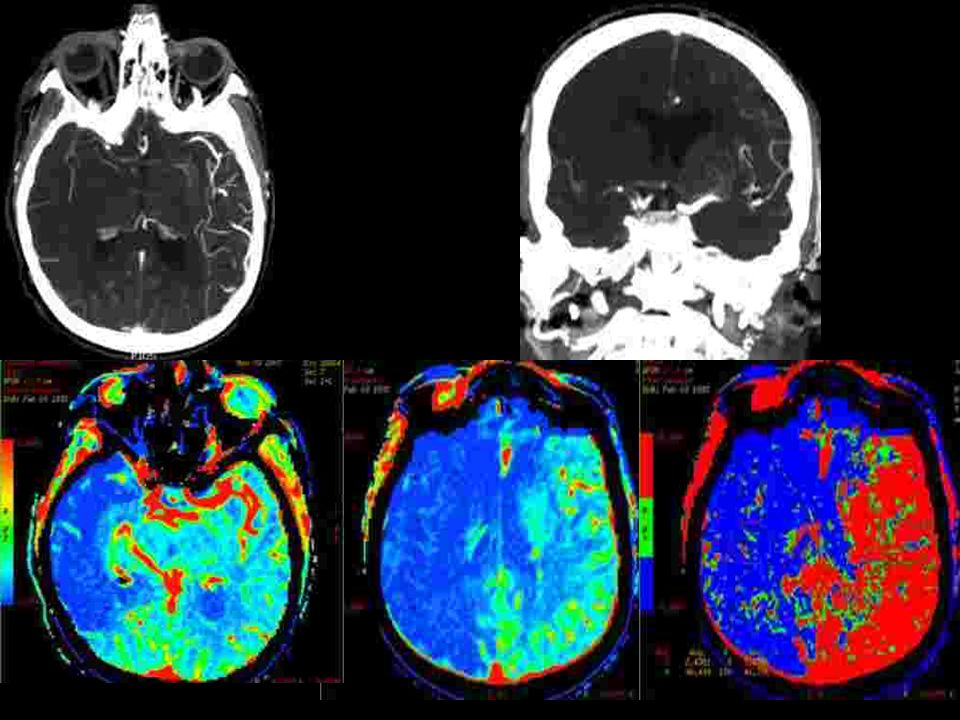
CBF CBV MTT

38
Occlusion en T de la carotide: pronostic effroyable
Evolution spontanée : mortalité : 41-50%, dépendance sévère : 29-51% Control group of the Duplex sonography in acute stroke study (27 patients avec traitement médical seul ) Recanalisation (6h) 1/27 Hémorragies 6/27 (18%) Évolution clinique (3 mois) mRS 0-2 0 mRS /27 (63%) décès 10/27 (37%) Wunderlich MT et al Cerebrovascular diseases 2005;20: T occlusion of the carotid siphon has a poor prognosis. with an overall mortality of 41-50% and severe dependency mRs 4 or 5 in another 29-51%. In the control group of the Duplex sonography in acute stroke study of 27 patients. Only one recanaliezd in the first 6 hours. Spontaneaous hemmorrhage occur in 18% and the functional outcome was very poor. With a dependancy in 63% and the death in 37%
 Recanalisation (6h) 1/27. Hémorragies 6/27 (18%) Évolution clinique (3 mois) mRS mRS /27 (63%) décès 10/27 (37%) Wunderlich MT et al Cerebrovascular diseases 2005;20: T occlusion of the carotid siphon has a poor prognosis. with an overall mortality of 41-50% and severe dependency mRs 4 or 5 in another 29-51%. In the control group of the Duplex sonography in acute stroke study of 27 patients. Only one recanaliezd in the first 6 hours. Spontaneaous hemmorrhage occur in 18% and the functional outcome was very poor. With a dependancy in 63% and the death in 37%")
39
Occlusion en T de la carotide: pronostic effroyable
Pourquoi? Deux facteurs principaux Intéresse les artères lenticulostriées Pauvreté de la circulation collatérale: l’artère communicante antérieure est elle perméable? Why this poor prognosis. Two main factors are well known. When the lenticulostriate arteries are involved the good results of thrombolysis decrease dramatically and the hemorrhagic risk increase when thrombolysis is performed after 4 hours. The second factor is the leptomeningeal collateral blood flow which depends in this location on the anterior communicating artery patency. If there is no ACOA there is no leptomeningeal collateral circulation and probably a worst prognosis

40
Etude rétrospective de 21 patients traités dans les 6 heures
OCCLUSION du « T » CAROTIDIEN : RESULTATS DE LA THROMBOLYSE INTRA-ARTERIELLE CHEZ 21 PATIENTS Etude rétrospective de 21 patients traités dans les 6 heures 14 femmes, 7 hommes Age: ans (31-84) NIHSS à l’admission: 18.9 (12-33) Délai de traitement: minutes (180 – 330) maladie cardio-embolique : 10 patients (47,7%) So in order to evaluate the results of intra arterial thrombolysis in this location we retrospectively studied 21 patients treated in the first 6 hours after the onset
 NIHSS à l’admission: 18.9 (12-33) Délai de traitement: minutes (180 – 330) maladie cardio-embolique : 10 patients (47,7%) So in order to evaluate the results of intra arterial thrombolysis in this location we retrospectively studied 21 patients treated in the first 6 hours after the onset.")
41
circulation collatérale
OCCLUSION du « T » CAROTIDIEN : RESULTATS DE LA THROMBOLYSE INTRA-ARTERIELLE CHEZ 21 PATIENTS circulation collatérale Artère communicante antérieure Présente 14 Absente 7 Opacification rétrograde de l’ACM Jusqu’à la région insulaire 3 cas Incompléte cas Absence cas Technique thrombolyse Mécanique 6 cas Mécanique +chimique 15 cas * Urokinase ( UI): 7 cases * Actilyse (0,9 mg/kg): cases + 1/15 stenting carotidien cervical (sténose >90%)
: 7 cases. * Actilyse (0,9 mg/kg): 8 cases. + 1/15 stenting carotidien cervical (sténose >90%)")
42
+ 70 mg rTpa Thrombectomie mécanique « Catch , Balt»

43
Résultats Recanalisation Immediate en Angiographie : DTC à 24 heures:
TIMI 0 6/21 TIMI 1 5/21 TIMI /21 DTC à 24 heures: Recanalisation - 13 cas (62%) Hémorragies 9 cas Transformation hémorragique 2/9 à 3 mois mRS /2 Hématome symptomatique /9 mRS / mRS / décès 3/7
 Hémorragies 9 cas. Transformation hémorragique 2/9 à 3 mois mRS 1 2/2. Hématome symptomatique 7/9 mRS 1 1/7 mRS 3-4 3/7 décès 3/7.")
44
EVOLUTION CLINIQUE résultats A J7
7 morts (33,3 %) (3 complications hémorragique) 14 patients survivants avec un score NIH de 6.8 A 3 mois (Modified Rankin Scale –mRS) mRS patients mRS patient mRS patients résultats 10 patients were autonomous mRS 0-1 mRS 2 mRS 3-4 mRS 6 47.7 % 4.8 % 14.2 % 33.3 %
 (3 complications hémorragique) 14 patients survivants avec un score NIH de 6.8. A 3 mois (Modified Rankin Scale –mRS) mRS patients. mRS 2 1 patient. mRS patients. résultats. 10 patients were autonomous. mRS 0-1. mRS 2. mRS 3-4. mRS % 4.8 % 14.2 % 33.3 %")
45
Recanalisation / Evolution Clinique
These good results were obtained quite only for patients with TIMI 2 or 3 recanalization. 80 % of patients with insifficient or without recanalization died or had a poor clinical evolution

46
Conclusions Le pronostic des occlusions en T de la carotide interne reste sévère recanalisation (TIMI 2 and 3) moins fréquente que pour M1 complications hémorragiques plus fréquentes (7/21) La thrombolyse intra artérielle améliore le pronostic La thrombectomie mécanque améliore le taux de recanalisation et son délai
 La thrombolyse intra artérielle améliore le pronostic. La thrombectomie mécanque améliore le taux de recanalisation et son délai.")
47
Carotide cervicale For cervical ICA occlusion the problem is more chalenging. We have to reopen both the ICA and MCA. Here an example with a sub occlusive stenis of ICA. And any collateral supply through the ophtalmic artery

48
And a poor collateral pial supply
And a poor collateral pial supply. The patient is young and the risk of malignant infacrt very high

49
This is the result after thrombo aspiration with a good filling of MCA

50
Après THROMBO ASPIRATION
But we have to treat the ICA stenosis Après THROMBO ASPIRATION

51
stent + protection device + angioplastie
With a stent placement on the bifurcation and post stent angioplasty stent + protection device + angioplastie

52
The final result is satisfactory with a quite good clinical evolution

53
Destruction mécanique du caillot
Thrombo-aspiration Fragmentation Injections pulsées Guides Ballons: angioplasties Stents Ultrasons Retrait

54
AVANTAGES THÉORIQUES Temps: la thrombectomie peut être réalisée en quelques minutes alors que la dissolution chimique peut prendre jusqu’à 2 heures Extension de la fenêtre thérapeutique Pas d’effet anti thrombotique Moins de complications hémorragiques Moins de contre indications (chirurgie, saignement récent…) Efficacité en termes de reperméabilisation
 Efficacité en termes de reperméabilisation.")
55
Merci à René Chapot!

56
The MERCI retrieval system :
- a retriever in a microcatheter - a 9F balloon guide catheter 1st step: the retriever is deployed inside the clot to ensnared the thrombus 2nd step: The ensnared clot is withdrawn - occlusion of the carotid or vertebral artery - continuous aspiration

57
151 patients treated 10 adverse events: 3 dissections, 3 arterial perforations and 2 distal embolisation. 2 patients died Hemorrhages Symptomatic hemorrhage rate: 7.8% Asymptomatic hemorrhage rate: 28.9% Recanalization: 46% (69/151) Overall mortatity at 90 days: % Patients successfully revascularised: 32% Patients not revascularised: 54% Modified Rankin score at 90 days 46% of patients successfully revascularised had a mRs from 0 to 2 10% of patients not revascularised
 Overall mortatity at 90 days: % Patients successfully revascularised: 32% Patients not revascularised: 54% Modified Rankin score at 90 days. 46% of patients successfully revascularised had a mRs from 0 to 2. 10% of patients not revascularised.")
58
Thrombus Debulking and Aspiration
Reperfusion Catheter and Separator™ System Operator motion of Separator clears catheter tip to allow continuous entry of thrombus Three sizes to match the site of occlusion: 041, 032, 026 Optimizes inner diameter and flexibility for maximum aspiration & navigation Neuro-designed Separator tip softness Faster, easier revascularization when time is brain The Penumbra System™

60
Baseline Characteristics
No. of Patients Screened 856 No. of Patients Enrolled 125 Age ( Years) 63.5 ± 13.5 Female 49% NIHSS at Baseline mRS at Baseline Target Vessel Locations: ICA 18% (23/125) MCA 70% (87/125) Vertebrobasilar 9% (11/125) Other 3% (4/125) TIMI 0 96% (120/125) TIMI 1 4% (5/125) Mean Time to Presentation (Hrs)
 63.5 ± Female. 49% NIHSS at Baseline mRS at Baseline Target Vessel Locations: ICA. 18% (23/125) MCA. 70% (87/125) Vertebrobasilar. 9% (11/125) Other. 3% (4/125) TIMI 0. 96% (120/125) TIMI 1. 4% (5/125) Mean Time to Presentation (Hrs)")
61
Primary Endpoint TIMI Scores (N = 125)
Baseline Post Treatment TIMI 0 96% 10% TIMI 1 4% 9% TIMI 2 54% TIMI 3 27% TIMI 2 & 3 82% (102/125)
")
62
Primary Endpoint Procedural SAEs
Event N=125 N % Perforation 2 1.6% ICH Total 4 3.2% All 4 events were adjudicated by the Clinical Events Committee as not device related. There were no incidents of device malfunction or breakage.

63
Related Trial Comparisons* Revascularization
1 2 3 4 1. Stroke 2005;36: AJNR 2006;27: JAMA1999;282: N. Eng J M 2004;351:2170 * Population observation rates, and 95% Exact Binomial Confidence Intervals

64
Secondary Endpoints Clinical And Functional Outcome
% ≥4 point improvement in NIHSS at discharge 58% ≥ 10 point improvement in NIHSS, or NIHSS 0-1 at discharge 27% mRS ≤ 2 at 90 days 25% Death at 30 days 26% Death at 90 days 33%

65
Related Trial Comparisons* mRS ≤ 2 at 90 Days
1 2 3 4 1. Stroke 2005;36: AJNR 2006;27: JAMA1999;282: N. Eng J M 2004;351:2170 * Population observation rates, and 95% Exact Binomial Confidence Intervals

66
Related Trial Comparisons* Symptomatic ICH
1 2 3 4 1. Stroke 2005;36: AJNR 2006;27: JAMA1999;282: N. Eng J M 2004;351:2170 * Population observation rates, and 95% Exact Binomial Confidence Intervals

67
Time to Revascularization (N=125)
Median Time from Symptom Onset to Arterial Puncture 4.1 hrs Median Time Required for Revascularization 45 mins

68
INDICATIONS SELECTION DES PATIENTS CONTRE INDICATIONS

69
Sélection des patients
Être efficace : y a t’il du parenchyme a sauver ? Diffusion : nécrose définitive! discutable: diminution des zones d’anomalies de diffusion après thrombolyse IA Hétérogénéité des niveaux de baisse d’ADC à l’intérieur de la zone anormale diminution progressive de l’ADC de la périphérie vers le centre: notion de seuil? < 50 % : évolution vers la nécrose certaine >70-80% : récupérable si recanalisation Importance de l’évaluation de l’ischémie: collatéralité en angiographie perfusion en IRM ou en scanner

70
Sélection des patients imagerie
Efficace Est ce un AVC? Ischémique ou hémorragique? Mismatch? Occlusion persistante? Rapide < 15 minutes Time is brain!! MRI: Diffusion+3d TOF MRA+ PerfusionMR CT scanner+angio CT+ perfusion CT

71
Sélection des patients
Ne pas être dangereux: identifier les patients à haut risque d’hémorragie Localisation profonde Délai Baisse de l’ADC: risques si ADC< 33% Hypoperfusion sévère : CBF< 33%

74
Stroke survey 46 centers Belgium 2 Czech Republic 1 France 10
Germany 5 Hungary 1 Italy 8 Latvia 1 Norway 2 Portugal 2 Romania 1 Spain 4 Sweden 1 Switzerland 2 Serbia 1 Turkey 2 United Kingdom 3

75
Diagnosis in emergency
75% use CT scan always or frequently!

76
Angio CT Perfusion CT Most often without CT angio or CT perfusion. Only 24% used systematically CTA and 19% CT perfusion

77
MRI in emergency MRI is less often used in emergency with 43% using MRI always or frequently MRI is less often used in emergency with 43% using MRI always or frequently

78
With a cerebral MRAngiography in the same session in 79%
In these centers using MRI cerebral vascular evaluation is performed in 80% of cases

79
Perfusion MRI With an MR perfusion study in 60% of cases
The mismatch evaluation in 81% even in the first 3 hours in 50% of cases And MR perfusion study in 60% with a mismatch evaluation even in the first 3 hours

80
Sécurité La sélection sur l’IRM augmente t’elle la sécurité de la thrombolyse? Ringleb et al JNNP 2007;78: 90 octogénaires Hémorragies 9,4% avec CT , 0 avec IRM 0 influence sur l’évolution globale Schellinger et al Stroke 2007 1210 patients (CT<3H:714, MRI<3h:316, MRI >3 h:180) Hémorragies symptomatiques : 5,3%, 2,8% et 4,4% mortalité: 13,7% vs 11,7% avant 3h Influence sur le taux d’évolution favorable après 3h
 Hémorragies symptomatiques : 5,3%, 2,8% et 4,4% mortalité: 13,7% vs 11,7% avant 3h. Influence sur le taux d’évolution favorable après 3h.")
81
INDICATIONS Thrombolyse à la carte ! Ou plutôt indication personnalisée: Clinique Diffusion Perfusion Angio-RM

83
Quelle technique pour quels patients?
IV: NINDS tous type d’AVC (résultats moins bons pour les artères principales) < 3h IA : PROACT II NIHSS > 10 < 6h Mismatch ? Risque hémorragique?
 < 3h. IA : PROACT II. NIHSS > 10. < 6h. Mismatch Risque hémorragique")
84
Quelle(s) technique(s) pour quels patients?
NIHSS < 10 < 3h IRM/CT ? rTpa IV +Abciximab? + Ultrasons? NIHSS > 10 < 3h IRM rTpa IA +Abciximab? rTpa IV? NIHSS > 10 > 3h IRM Mécanique ± rTpa IA ±Abciximab?

85
Quelle(s) technique(s) pour quels patients? Attitude nancéenne 2007
IV < 3heures « mismatch » ? M1 distal et au delà IA > 3 heures : toutes localisations < 3 heures : TB, ACI, M1 proximal Mismatch diff/perf

86
Stroke survey 46 centers Belgium 2 Czech Republic 1 France 10
Germany 5 Hungary 1 Italy 8 Latvia 1 Norway 2 Portugal 2 Romania 1 Spain 4 Sweden 1 Switzerland 2 Serbia 1 Turkey 2 United Kingdom 3

87
Techniques 42 of these 46 centers performed IV or IA rTPA thrombolysis, 31 mechanical thrombolysis and 14 have a combined IV and IA protocol

88
Indications It’s interesting to evaluate the technical choices In M2 occlusion IV T is often preferred in the first 3 hours and IA rTpa after 3 hours

89
In M1 occlusion, IVT is preferred in the first 3 hours, often associated with IA thrombolysis. After 3 hours a mechanical thrombectomy is proposed alone or combined with IA rTpa in 20 centers

90
In the same way, IA mechanical thrombolysis is proposed in 21 centers for T occlusion of ICA and only 4 centers used an IVT alone!

91
For a basilar tip occlusion an IVT is proposed in only 2 centers and IA in 33 with a mechanical device in 18.

92
Organisation: EN PRATIQUE !
Priorité de l ’établissement ! Organisation simple et économe en temps: un seul point d’entrée accès direct à l’imagerie 24h/24 un nombre limité d’intervenants

93
Objectifs Aller vite! aller vite! aller vite… Rester dans les délais
PROACT II 5,3 h Nancy IA/IV 5,2 h IA/ 4,25 IV Efficacité: récupération fonction du délai

94
Objectifs 1er médecin consulté Aller vite! aller vite! aller vite…?
Hôpital de proximité SAU neurologue Thrombolyse IRM scanner

95
Objectifs Patient-famille 1er médecin consulté Hôpital de proximité
15 - SAMU IRM scanner neurologue Thrombolyse

Présentations similaires











![[number 1-100].](/1/172887/big_thumb.jpg "[number 1-100].>")













