Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Traumatisme crânien: monitorage multimodal
Dr LOSSER Marie-Reine Dépt Anesthésie-Réanimation Hôpital Lariboisière – PARIS

2
Lésion initiale et ischémie secondaire
h PIC Perfusion Cérébrale Débit cérébral Oedème In brain injury, the consequences of initial insult is an increase of intracranial pressure. This increase of ICP induces an impaired cerebral perfusion That leads to secondary ischemia of parenchyma. The cellular response to ischemia is rapidly associated with oedema That makes the the cerebral perfusion worse and we enter in a vicious circle that leads to death of the patient Ischémie Secondaire aggravation décès

3
Louisiana State University Medical Center; New Orleans
Introduction The main objective of intensive monitoring in the head-injured patient is to help the physician maintain adequate cerebral perfusion and oxygenation and avoid medical and surgical complications as well as secondary injury while the brain recovers. Louisiana State University Medical Center; New Orleans

4
Multimodal Monitoring in Patients with Head Injury Deepak Awasthi, MDLouisiana State University Medical Center; New Orleans Monitoring Modality Abbrev . Determination Threshold for Treatment Treatment Options Intracranial Pressure ICP ICP monitor (placed in the ventricle; brain parenchyma; subarach, sub- dural, or epi-dural space); usually fiberoptic 20-25 mm Hg Hypervent. Head elev. Mannitol CSF drainage Sedation Paralysis Barb. coma Surgery (prn) Blood Pressure BP arterial line < 100mm Hg Vasopressors Fluids Blood Cerebral Perfusion Pressure CPP CPP=MAP-ICP; MAP: mean arterial pressure < 70 mm Hg ICP and BP control (see above) Jugular Bulb Venous Oxygen Saturation SjvO2 catheter (usually fiberoptic) inserted into the jugular bulb < 50% saturation ICP and CPP control (see above) Brain Tissue Oxygen Monitoring PtiO2 microcatheter inserted in frontal cerebral white matter < 8.5 mm Hg
; usually fiberoptic mm Hg. Hypervent. Head elev. Mannitol CSF drainage Sedation Paralysis Barb. coma Surgery (prn) Blood Pressure. BP. arterial line. < 100mm Hg. Vasopressors Fluids Blood. Cerebral Perfusion Pressure. CPP. CPP=MAP-ICP; MAP: mean arterial pressure. < 70 mm Hg. ICP and BP control (see above) Jugular Bulb Venous Oxygen Saturation. SjvO2. catheter (usually fiberoptic) inserted into the jugular bulb. < 50% saturation. ICP and CPP control (see above) Brain Tissue Oxygen Monitoring. PtiO2. microcatheter inserted in frontal cerebral white matter. < 8.5 mm Hg.")
5
PAM > Pvc > PIC > Psl
Artère Carotide parenchyme sinus veineux V jugulaire OD LCR Veine Cérébrale PAM Pvc PIC Psl In brain blood is going through cerebral arteries, vein and is collected in sinus to reach jugular vein The relation between arterial pressure, cerebral vein pressure, ICP and collecting vein pressure permit the circulation of the blood In brain injury, ICP is increased and determines the cerebral perfusion and limits cerebral perfusion Control of ICP is a therapeutic goal. Trauma crânien: PIC PIC devient un déterminant du débit sanguin cérébral Contrôle de PIC est un but thérapeutique car conditionnant la PPC

6
Strategie thérapeutique
Réduire la CMRO2 par: Sédation; hypothermie modérée, contrôle de la douleur et des stimuli exogènes Optimiser les déterminants du CBF: CPP; HR; PaCO2; SaO2; [Hb]

7
Multimodal monitoring
Doppler TC estime les variations CBF Systolique Vmax ; V fin Diastole des 2 ACM, comparées à CI à faire systématiquement si suspicion d’une HD cérébrale anormale SvjO2: estimer l’adéquation de l’apport à la demande métabolique (O2) PIC et PPC CT Scan répétés (EEG) Neuroprotéines S100? P tissulaires O2, CO2, microdialyse?
 PIC et PPC. CT Scan répétés. (EEG) Neuroprotéines S100 P tissulaires O2, CO2, microdialyse")
8
Multimodal monitoring
adapter la stratégie thérapeutique en confrontant les vélocités ACM et SjvO2 è Vélocités et èSvjO2 : HypoPCO2?? èCPP Vélocités et èSvjO2 : anémie?? désaturation Artérielle?? Hyperthermie?? Convulsions?? Pour chaque étiologie traitement spécifique évalué par le monitoring détection rapide de l’ischémie secondaire prévenir et/ou traiter l’ischémie caleéréb

9
PPC = PAM – PIC PIC « normale »: 7 mmHg ?
This schematic diagram represents a typical intracranial (ICP) waveform. "A" waves (not shown here) are also called plateau waves and there appearance correlates with a worsening clinical picture and very high intracranial pressure (> 50 mm Hg). Depicted in this figure are the more typical "B" waves (respiratory fluctuations in ICP; they occur at intervals of 30 secs to 2 minutes and range from mm Hg) and "C" waves (cardiac fluctuations in ICP; they are smaller).
 waveform. A waves (not shown here) are also called plateau waves and there appearance correlates with a worsening clinical picture and very high intracranial pressure (> 50 mm Hg). Depicted in this figure are the more typical B waves (respiratory fluctuations in ICP; they occur at intervals of 30 secs to 2 minutes and range from mm Hg) and C waves (cardiac fluctuations in ICP; they are smaller).")
10
PIC

11
PIC Parenchyme =85% LCR =10% Sang =5% Hématome Oedeme Vasodilatation
Hydrocéphalie Volume PIC

12
Concepts physiologiques
Autorégulation du débit sanguin cérébral: Altérée dans les zones lésées DSC PPC = PAM - PIC 50 150

13
Le cerveau SvO2 % c h a n g e Débit sanguin cérébral
Volume sanguin cérébral Taux d’extraction d’oxygène Consommation d’oxygène Diamètre des artères piemériennes 60 140 40 hyperhemia % c h a n g e C B F C B V O2 Extraction CMRO2 PIEMERIAL VESSEL DIAMETER C PP autoregulation ischemia oligemia Le cerveau SvO2

14
Cascade vasodilatation/vasoconstriction by Rosner (1990)
craniectomy This is the vasoconstriction cascade increase of systemic blood pressure increase CPP, leading to vasoconstriction of healthy area, regional reduction of blood volume and fall of ICP that mkes the PP better etc This phenomenon in healthy area may redistribute the blood towards injured and ischemic area and make there perfusion better There is different possibilities to enter in this benificial cascade: decreasing, edema, CSF withdrawal, reduction of metabolism, increase of systemic pressure with pharmacologic agents. Cascade vasodilatation/vasoconstriction by Rosner (1990)
")
15
Bottom: -15 min after hyperventilation - Pa CO2 of 30 mmHg
Xenon-enhanced computed tomography flow images from a child 16 hrs after a motor vehicle accident. Admission GCS: 5/15 Top: - Pa CO 2 of 45 mmHg - ICP 44 mm Hg - CPP 54 mm Hg - CBF 59 mL/min/100 g. Bottom: -15 min after hyperventilation - Pa CO2 of 30 mmHg - ICP 15 mmHg - CPP 82 mmHg - CBF 14 mL/min/100 g (Several local areas of this scan had regional cerebral blood flow rates lower than 10 mL/min/100 g.) Is it better to keep the perfusion or the ICP level? FANZCA, CCM, 1997 This slide from literature illustrate the difficulty to define goals for resuscitation. In this cas, the cocomittent elevation of ICP and PaCo2 allowed to reduce PaCO2. If hyperventilation was efficient for ICP level, such pressure improvement was not associated to a blood flow improvement.
 Is it better to keep the perfusion or the ICP level FANZCA, CCM, This slide from literature illustrate the difficulty to define goals for resuscitation. In this cas, the cocomittent elevation of ICP and PaCo2 allowed to reduce PaCO2. If hyperventilation was efficient for ICP level, such pressure improvement was not associated to a blood flow improvement.")
16
h PPC peut être utilisée pour contrôler PIC
This can be used in brain injuty for controlling ICP through the reactivity to perfusion pressure of healthy area of the brain Decrease of cerebral perfusion leads to vasodilation and increase of cerebral blood volume associated with increase of ICP When the PP goes up, the regional the vasoconstriction of healthy area permit the reduction of blood volume and the decrease of ICP Cascade vasodilatation/vasoconstriction by Rosner (1990)
")
17
Norepinephrine Hypothèse: PPC augmente de 22 mmHg à 93 mmHg
- Vasoconstriction VSC PIC - Perfusion améliorée ischémie PIC 100 30 70 Norepinephrine PPC augmente de 22 mmHg à 93 mmHg

18
pression => de PIC ( du VSC)
Autorégulation et PIC pression => de PIC ( du VSC) PA PIC PPC FC Vasodilatation VC delai
 PA. PIC. PPC. FC. Vasodilatation VC. delai.")
19
Autorégulation Nor augm PA VC baisse VSC baisse PIC Augm PPC
Noradrénaline Remplissage Nor augm PA VC baisse VSC baisse PIC Augm PPC

20
Perte d'autorégulation Montée de PA => montée de PIC (augmentation du compartiment sanguin)
FC Pas de VC --> P/Q dep 200 PA 40 PIC PPC

21
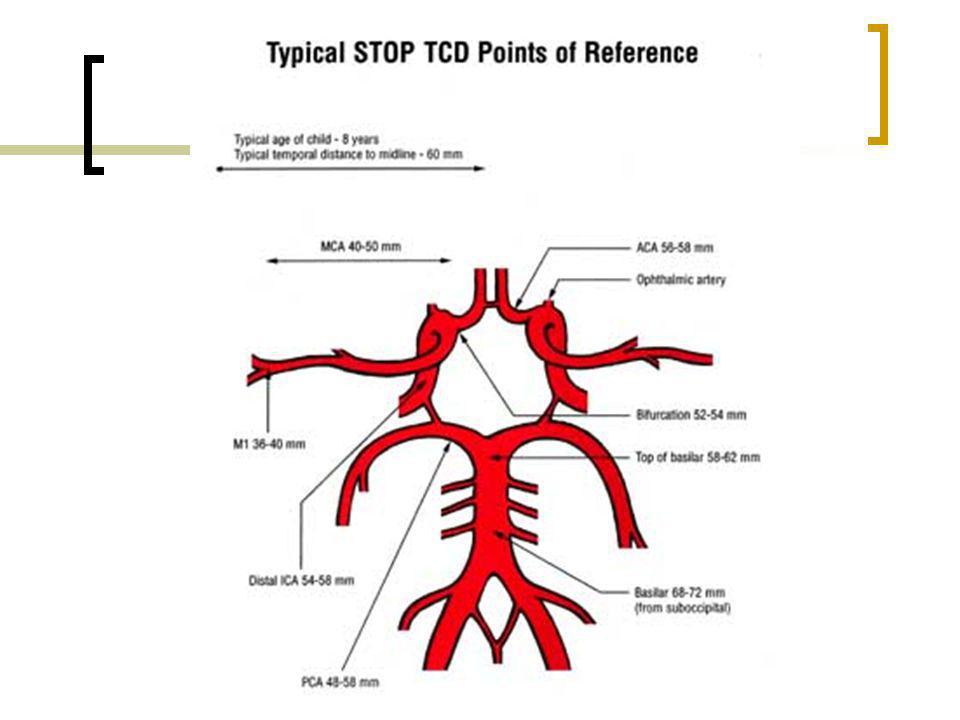
Doppler transcrânien Etudie la vitesse des GR dans les gros vx du
polygone de Willis Analyse phasique

23
Doppler trans crânien Index de résistance IR = (VS-VD )/VS
Vélocité systolique (VS) Vélocité diastolique (VD) débit passif fct de R V Index de résistance IR = (VS-VD )/VS tps S D
 Vélocité diastolique (VD) débit passif fct de R. V. Index. de résistance. IR = (VS-VD )/VS. tps. S. D.")
24
Résistance élevée (obstacle à l’écoulement)
D VS conservée VD Basse R très élevée Débit effondré

25
Vd basses => bas débit cérébral
DTC: Vd basses => bas débit cérébral IR élevé (0,84) Moniteur PIC élevée PPC basse Hypocapnie 35° ISCHEMIE
 Moniteur. PIC élevée. PPC basse. Hypocapnie. 35° ISCHEMIE.")
26
DTC: Flux conservé Moniteur PIC élevée PPC conservée

27
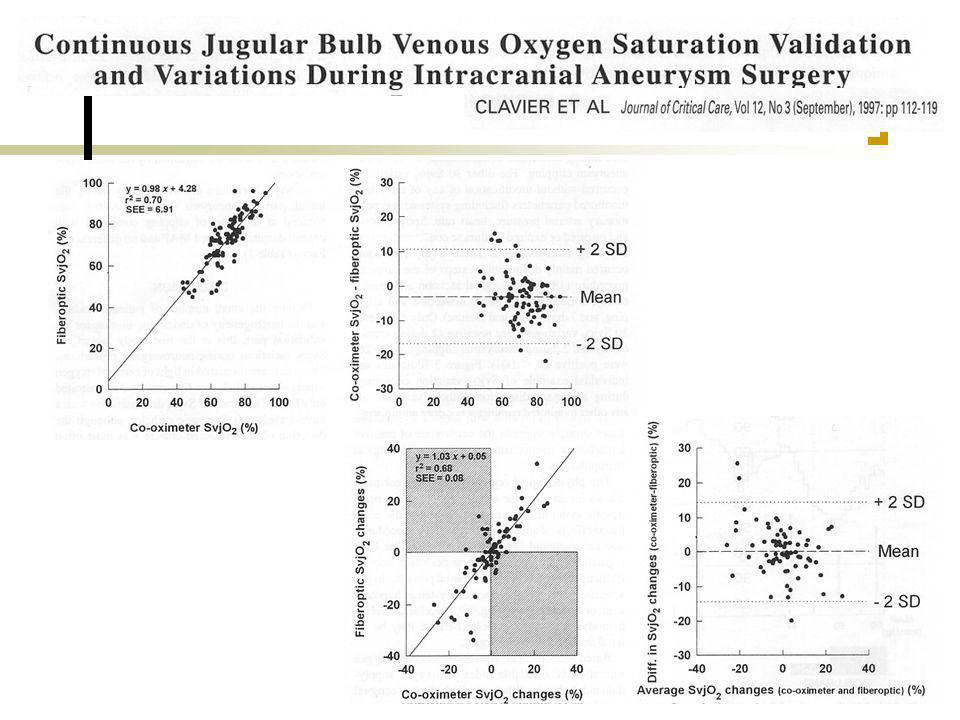
Saturation veineuse du golfe jugulaire (SvjO2) et laquelle?
Mélange anatomique Mais Différence 5,3% ± 5,1 50% des patients ont une différence > 15% Sans corrélation TDM Stocchetti N, Neurosurgery 1994

28
Rationel du monitorage SvjO2
Tissu cérébral très susceptible au déficit en oxygène Apport Oxygen dépendant du DSC DSC and CMRO2 sont couplés: DSC fonction de la demande Dans la lésion cérébrale, regulation du débit peut être altérée SvjO2 informe sur : Cerveau capable d’extraire l’oxygène. extraction O2 reflet de la CMRO2 et guide thérapeutique. Tant que Hb et SaO2 sont constants SvjO2 is LE PARAMETRE évaluant CMRO2 et CBF.

30
TC sévère Evolution de: SvjO2, PIC, PAM, doppler transcrânien (vélocité ACM) après un bolus de mannitol. avant PIC 33 mmHg PAM 89 mmHg PPC 56 mmHg SvjO2<60% après PIC 20 mmHg PAM 89 mmHg PPC 69 mmHg SvJO2>60% Mannitol

31
PIC et PEEP ?

32
Jugulaire interne :veine valvulée
Valve bicuspide ou tricuspide au niveau du bulbe jugulaire (2 cms au dessus de jonction avec veine sous clavière) Inconstante (environ 90% de la population) Parfois unilatérale
 Inconstante (environ 90% de la population) Parfois unilatérale.")
33
Brain Tissue pO2 Monitoring (PtiO2)
Intérêt: mesure de l’oxygène contenu dans le tissu MAIS: O2 disponible, utilisé ou non? Très (trop?) local, sensible FiO2
 local, sensible FiO2.")
34
Multimodal monitoring

37
Evaluation biologique de la gravité des lésions
Dosage de neuroprotéines, disponible et la plus étudiée: S100b (troponine du cerveau?) Taux sanguin relié à la gravité de la lésion initiale
 Taux sanguin relié à la gravité de la lésion initiale.")
38
C ri t are Med 2002; 30 : 1870 -1876 Objective: a) to examine variations in care of patients with severe head injury in academic trauma centers across the United States; b) to determine the proportion of patients who received care according to the Brain Trauma Foundation guidelines; c) to correlate the outcome from severe traumatic brain injury with the care received.
 to examine variations in care of patients with severe head injury in academic trauma centers across the United States; b) to determine the proportion of patients who received care according to the Brain Trauma Foundation guidelines; c) to correlate the outcome from severe traumatic brain injury with the care received.")
39
34 academic US Trauma centers GCS ≤ 8; multiple trauma; n = 182
ri t are Med 2002; 30 : 1870 -1876 8 months collection 34 academic US Trauma centers GCS ≤ 8; multiple trauma; n = 182 “aggressive” vs “non aggressive” centers: ICP monitoring > 50% and abnormal CT scan

40
Considerable variation across centers in the rates of:
are Med 2002; 30 : 1870 -1876 Considerable variation across centers in the rates of: Prehosp intubation ICP monitoring Head CT 37% overall mortality 7% indep at discharge 57% partially dependent 36% totally dependent “aggressive” centers : Significant reduction in the risk of mortality: 27% vs 45% (p<0.04) Shorter LOS for survivors (- 6 days) NS difference in functional status at the time of discharge for survivors.
 Shorter LOS for survivors (- 6 days) NS difference in functional status at the time of discharge for survivors.")
41
Comparative results for GCS ≤ 8: Lariboisiere vs CCM data (august 2002)
50 45 40 Lariboisiere 35 30 Global CCM (2002) 25 * * 20 * "Agressive" centers 15 "Non agressive" 10 centers 5 Mortality
 25. * * 20. * Agressive centers. 15. Non agressive 10. centers. 5. Mortality.")
42
Changes in the management of severe traumatic brain injury: 1991-1997
Changes in the management of severe traumatic brain injury: Marion, CCM, Janv 2000 Enquête anonyme chez 3256 neurochirurgiens US, avant (Ghajar 1991), et après diffusion des recommandations américaines pour la prise en charge des TC graves 1262 réponses (40 %) Ghajar, 1991(%) 1997 Monitorage de la PIC 40 83 Ventriculostomie préférentiellement 72 50 Hyperventilation prophylactique 36 Corticoïdes 64 19
, et après diffusion des recommandations américaines pour la prise en charge des TC graves réponses (40 %) Ghajar, 1991(%) Monitorage de la PIC Ventriculostomie préférentiellement Hyperventilation prophylactique. 36. Corticoïdes")
Présentations similaires

>")


















