Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Transplantation hépatique chez les patients coinfectés VIH VHB
Rodolphe SOBESKY MD, PhD Centre Hepato-Biliaire Inserm Unit 785

2
Mr R. (1) Traitement ? 53 ans, pas de consommation d’alcool
Infection VIH connue depuis Traitement anti-rétroviral par VIDEX + ZERIT de 1997 à 2002. Arrêt pour lipodystrophie et remontée des CD4. Infection par le VHB connue depuis 1990, non suivie, non traitée Hospitalisée en Janvier 2010 pour asthénie avec ictère AST = 4N, ALT = 7N TP = 43%, Bili T = 180 µmol/l Créat = 72 µmol/l ADN VHB = 8 log ARN VIH = 4 log CD4 = 150/mm3 Echo : foie dysmorphique Pas de CHC Traitement ? 2

3
Impact du VIH sur le VHB Augmente risque évolution chronique
Augmente réplication virale Diminue séroconversion anti Hbe et HBs Augmente risque réactivation (CD4?) Accélère la progression de la fibrose Augmente le risque décompensation hépatique et la mortalité hépatique
 Accélère la progression de la fibrose. Augmente le risque décompensation hépatique et la mortalité hépatique.")
4
Traitement réactivation cirrhose B décompensée?
Utilisation de puissants analogues avec de bon profils de résistance (entecavir ou tenofovir). Cependant, il existe peu de données sur la tolérance de ces traitements dans la cirrhose décompensée (B1) EASL Clinical Practice Guidelines. J. Hepatol 2009 Etude TDV, TDF+FTC, ETV sur les cirrhoses B décompensées : - bien tolérés - efficacité virologique - amélioration clinique et Child Liaw YF, Hepatology 2011 Cas du VIH VHB Débuter le TARV chez tous les patients co-infectés par le VIH/VHB qui nécessitent un traitement pour leur infection à VHB quel que soit le taux de CD4 ou le stade clinique OMS. Anti viral actif contre VHB et VIH : TDF + FTC + autre antiviral (A1) EASL Clinical Practice Guidelines. J. Hepatol 2009 Recommandation OMS
. Cependant, il existe peu de données sur la tolérance de ces traitements dans la cirrhose décompensée (B1) EASL Clinical Practice Guidelines. J. Hepatol Etude TDV, TDF+FTC, ETV sur les cirrhoses B décompensées : - bien tolérés. - efficacité virologique. - amélioration clinique et Child. Liaw YF, Hepatology Cas du VIH VHB. Débuter le TARV chez tous les patients co-infectés par le VIH/VHB qui nécessitent un traitement pour leur infection à VHB quel que soit le taux de CD4 ou le stade clinique OMS. Anti viral actif contre VHB et VIH : TDF + FTC + autre antiviral (A1) EASL Clinical Practice Guidelines. J. Hepatol Recommandation OMS.")
5
Sous Tenofovir/Emtricitabine + Lopinavir/Ritonavir
Mr R. (2) Sous Tenofovir/Emtricitabine + Lopinavir/Ritonavir Baisse progressive de l’ADN du VHB Baisse progressive de l’ARN du VIH ADN VHB (log) 8 ARN VIH (log) 7 1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 Semaines 1 2 3 4 Semaines TP Bili T Dégradation de la fonction hépatique 1 2 3 4 Semaines 100% 75% 50% 25% 100 200 400 500 300 Que proposer vous ? 5
 Sous Tenofovir/Emtricitabine + Lopinavir/Ritonavir. Baisse progressive de l’ADN du VHB. Baisse progressive de l’ARN du VIH. ADN VHB. (log) 8. ARN VIH. (log) Semaines Semaines. TP. Bili T. Dégradation de la fonction hépatique Semaines. 100% 75% 50% 25% Que proposer vous 5.")
6
Mr R. (3) Adressé en Février 2010 à Paul Brousse. Poursuite traitement
Bilan pré TH simplifié Prévention récidive en pré TH : Un traitement pré-transplantation avec un puissant analogue ayant une barrière de résistance élevée est recommandé chez tous les patients AgHBs-positifs subissant une transplantation hépatique suite à une maladie hépatique avancée ou un CHC liés au VHB, afin d’atteindre le niveau d’ADN VHB le plus bas possible avant la transplantation (A1) (EASL Clinical Practice Guidelines, J. Hepatol ) Que proposez vous? Majoration de l’insuffisance hépatique (MELD = 40) - TP = 12%, - Bili T = 540 µmol/l - Créat = 230 µmol/l - Apparition d’une ascite - Apparition d’une encéphalopathie (CD4 = 180, ARN VIH indétectable, ADN VHB = 3,8 log) 6
 (EASL Clinical Practice Guidelines, J. Hepatol ) Que proposez vous Majoration de l’insuffisance hépatique (MELD = 40) - TP = 12%, - Bili T = 540 µmol/l. - Créat = 230 µmol/l. - Apparition d’une ascite. - Apparition d’une encéphalopathie. (CD4 = 180, ARN VIH indétectable, ADN VHB = 3,8 log) 6.")
7
Mr R. (4) Transplantation hépatique en Mars 2010
Suites immédiates : pneumopathie à CMV (réa = 3 semaines) Traitement préventif récidive VHB (post TH précoce) ? Traitement par Fuzeon +Truvada à J+16 et IM Glob anti HBs Recommandations post-TH : les données d’efficacité et de tolérance avec les analogues plus récents, plus puissants et avec des taux de résistances plus bas (entecavir ou tenofovir), n’ont pas été publiés mais ces traitements doivent être envisagés, car une suppression importante et des faibles taux de résistance sont préférables (B1). Ces traitements son donnés en association avec des IM Glob anti HBs. 7
 Traitement préventif récidive VHB (post TH précoce) Traitement par Fuzeon +Truvada à J+16 et IM Glob anti HBs. Recommandations post-TH : les données d’efficacité et de tolérance avec les analogues plus récents, plus puissants et avec des taux de résistances plus bas (entecavir ou tenofovir), n’ont pas été publiés mais ces traitements doivent être envisagés, car une suppression importante et des faibles taux de résistance sont préférables (B1). Ces traitements son donnés en association avec des IM Glob anti HBs. 7.")
8
Risque réactivation après transplantation ?
Risque récidive élevé si : Particules VHB circulantes (ou site extra hépatique) Mutants S VHB (pt recevant HBIG) Risque spontané de récidive = 80% (si ADN VHB +) Avec prévention reposant sur : Administration d’HBIG Agents antiviraux Actuellement risque récidive infection VHB < 10% Shouval D, Samuel D. Hepatology 2000;32: Samuel D, Digestive and Liver Disease 2009:41S:S185 8
 Mutants S VHB (pt recevant HBIG) Risque spontané de récidive = 80% (si ADN VHB +) Avec prévention reposant sur : Administration d’HBIG. Agents antiviraux. Actuellement risque récidive infection VHB < 10% Shouval D, Samuel D. Hepatology 2000;32: Samuel D, Digestive and Liver Disease 2009:41S:S")
9
Mr R. (4) Traitement préventif récidive en post TH tardif ?
Suites à M3 favorables : TP = 100% ALT = N, AST = N, GGT = N Créat = 85 µmol/l IM sup : Ciclosporine, Corticoïdes, MMF Greffon morphologiquement normal HBIG pour titrage > 500 UI/L ADN VHB indétectable (Tenofovir/Emtricitabine + Ritonavir + Darunavir) Traitement préventif récidive en post TH tardif ? 9
 Traitement préventif récidive en post TH tardif 9.")
10
Prévention réactivation après transplantation
Combinaison HBIG + Antiviral Prévention récidive avec Ac anti HBs > 150 UI/L Antiviral (TDF + FTC avec autre antiviral contre VIH) Shouval D, Samuel D. Hepatology 2000;32: Samuel D, Digestive and Liver Disease 2009:41S:S185 EASL Clinical Practice Guidelines. J. Hepatol 2009 Alternatives combinaison HBIG – Antiviraux ? Questions non résolues Prévention récidive avec faible posologie d’HBIG ? Monothérapies (arrêt des HBIG?) 10
 Shouval D, Samuel D. Hepatology 2000;32: Samuel D, Digestive and Liver Disease 2009:41S:S185. EASL Clinical Practice Guidelines. J. Hepatol Alternatives combinaison HBIG – Antiviraux Questions non résolues. Prévention récidive avec faible posologie d’HBIG Monothérapies (arrêt des HBIG ) 10.")
11
Maladies hépatiques et infection VIH
Alcohol NAFLD cART Immune reconstitution HCV HBV HAV 10 20 30 40 50 60 70 HCV HBV cART 66% 17% 3% Mortalité With the successful introduction of HAART therapy, HIV is now regarded as a disease with excellent long-term outcomes. However coinfection with Hepatitis B and Hepatitis C viruses and drug toxicity secondary to HAART have resulted in increasing rates of mortality and morbidity due to end-stage liver disease. HIV/HCV co-infected patients experience more rapid fibrosis progression and have poorer survival rates in comparison with HCV-monoinfected patients. Joshi D et al. Lancet 2011 Weber et al. Arch Intern Med 2006 Salmon-Ceron D. et al. J Hepatol 2005

12
Proportion de décès lié au CHC :
Mortalité liée à une maladie du foie chez patients infectés par le VIH (GERMIVIC) Proportion de décès lié au CHC : 2000: 15% 2005: 25% Salmon-Ceron D et al. J Hepatol 2009
 Proportion de décès lié au CHC : 2000: 15% 2005: 25% Salmon-Ceron D et al. J Hepatol")
13
Potentiels candidats pour la transplantation hépatique chez les patients infectés par le VIH
Patients avec une cirrhose décompensée Patient avec un CHC dans les critères de TH Charge virale VIH indédectable CD4 > 150 / mm3 Pas d’infection opportuniste (pas d’évènement SIDA) Bonne complience au traitement HIV disease is no longer considered an absolute contraindication to liver transplantation by most transplant centers wordlwide. French concensus conference 2005, Liver transplant 2006
 Bonne complience au traitement. HIV disease is no longer considered an absolute contraindication to liver transplantation by most transplant centers wordlwide. French concensus conference 2005, Liver transplant")
14
Post-Liver Transplantation Survival Reports of the litterature
HIV+/HBV+ HIV+/HCV+ Author/ Journal/Year n Patient survival (%) 3 yrs 5 yrs Ragni et al. J Infect Dis 2003 15 57 - De Vera et al. Am J Transpl 2007 27 56 33 Schreibman et al. Transplantation 2007 73 Vennrecci et al. Transpl Proc 2007 12 58 Duclos-Vallée et al. Hepatology 2008 35 51 Terrault et al. Hepatology 2009 81 59 Author/ Journal/Year n Patient survival (%) 1yr 3 yrs Fung et al. Liver Transplant 2004 3 100 - Norris et al. 4 Duclos-Vallée et al. J Hepatol 2006 5 Schreibman et al. Transplantation 2007 8 75 Roland et al. Am J Transplant 2007 Tateo, et al. AIDS 2009 13 HIV disease is no longer considered an absolute contraindication to liver transplantation by most transplant centers wordlwide. HIV/HBV coinfected patients have excellent survival outcomes after liver transplantation. However current data indicate poorer outcomes for HIV/HCV coinfected patients. The survival rates range from 33% to 51 % at 5 years;
 3 yrs. 5 yrs. Ragni et al. J Infect Dis De Vera et al. Am J Transpl Schreibman et al. Transplantation Vennrecci et al. Transpl Proc Duclos-Vallée et al. Hepatology Terrault et al. Hepatology Author/ Journal/Year. n. Patient survival (%) 1yr. 3 yrs. Fung et al. Liver Transplant Norris et al. 4. Duclos-Vallée et al. J Hepatol Schreibman et al. Transplantation Roland et al. Am J Transplant Tateo, et al. AIDS HIV disease is no longer considered an absolute contraindication to liver transplantation by most transplant centers wordlwide. HIV/HBV coinfected patients have excellent survival outcomes after liver transplantation. However current data indicate poorer outcomes for HIV/HCV coinfected patients. The survival rates range from 33% to 51 % at 5 years;")
15
12 ans d’expérience de prise en charge des patients VIH après TH
Collaboration étroite avec des spécialistes du VIH Gestion des interactions IS – ARV - Arrêt ART 2 à 3 semaines après la TH - Ciclosporine (1/2 vie plus courte que Tacrolimus) - Arret temporaire de la ciclosporine avant réintrocuction des IP - Controle quotidien des résiduels après réintroduction des ARV (T20, Raltegravir pour passer un cap difficile) Teicher, Liver transplant 2010 Teicher, Am J Transplant 2009 Teicher, Clin Pharmacokinet 2007
 - Arret temporaire de la ciclosporine avant réintrocuction des IP. - Controle quotidien des résiduels après réintroduction des ARV. (T20, Raltegravir pour passer un cap difficile) Teicher, Liver transplant Teicher, Am J Transplant Teicher, Clin Pharmacokinet")
16
Experience of > 100 Patients Transplanted Between December 1999 and March 2010 Indications of Liver Transplantation n=59* 56% * HCV/EtOh cirrh: : n= 4 60 50 ** HCV cirrh: n=15 HCV/EtOh cirrh: : n= 1 HCV/HBV cirrh: n=2 HBV cirrh: n=2 40 ** n=20 19% 30 *** n=12 11% 20 n=8 8% HCV cirrhosis was the most prevalent indication of liver transplantation; 59 (56 percent) patients were transplanted because of end stage liver disease due to HCV cirrhosis. HCC represented the second indication of LT and concerned 20 (19%) patients. Other indications were as follows: nodular regenerative hyperplasia in four patients, …. n=5 4.5% n=1 1% *** Nodular Regenerative Hyperplasia: n=4 Hepatopulmonary Sd: n=3 Fulminant Hepatitis: n=2 Secondary biliary cirrhosis: n=2 Hemochromatosis: n=1 10 HCV HCC HBV HBV/HCV HBV/HDV Others Cirrh. Cirrh. Cirrh.
 patients were transplanted because of end stage liver disease due to HCV cirrhosis. HCC represented the second indication of LT and concerned 20 (19%) patients. Other indications were as follows: nodular regenerative hyperplasia in four patients, …. n=5. 4.5% n=1. 1% *** Nodular Regenerative Hyperplasia: n=4. Hepatopulmonary Sd: n=3. Fulminant Hepatitis: n=2. Secondary biliary cirrhosis: n=2. Hemochromatosis: n= HCV. HCC. HBV. HBV/HCV. HBV/HDV. Others. Cirrh. Cirrh. Cirrh.")
17
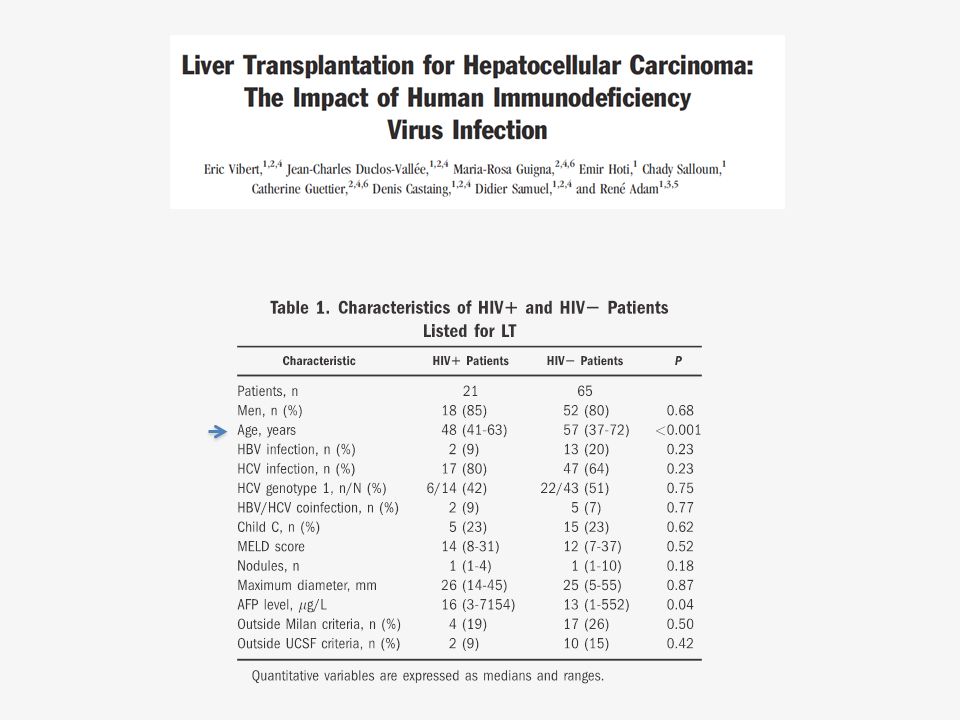
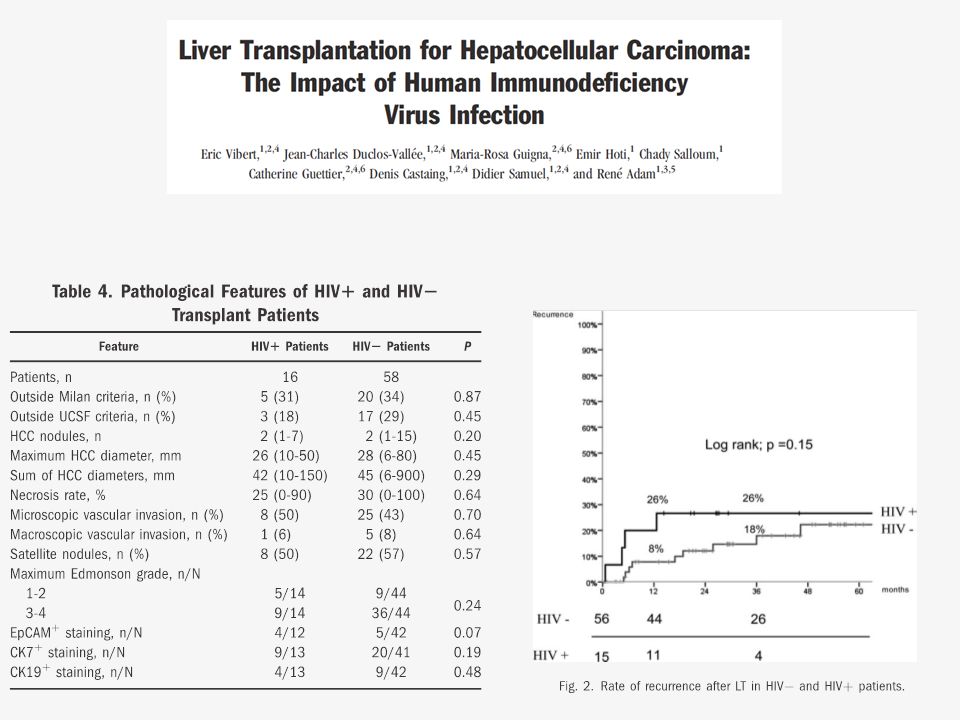
Transplantation pour CHC chez les patients VIH

20
Sortie de liste : 23% chez patients HIV+ contre 10% chez patients HIV- (p<0.08)
")
21
Morbidité et mortalité après TH

22
Characteristics of Deaths after LT
Total number 40 HCV recurrence HCC recurrence Sepsis Myocardial infarction Cerebrovascular events Lactic acidosis Pancreas adenocarcinoma Pulmonary embolism Digestive hemorrhage Rupture of the hepatic artery De novo cholangiocarcinoma 20 (50%) 5 (12.5%) 5 (12.5 %) 2 (5%) 1 (2.5 %) 1 (2.5 %) Fifty percent of the deaths were due to HCV recurrence
 5 (12.5%) 5 (12.5 %) 2 (5%) 1 (2.5 %) 1 (2.5 %) Fifty percent of the deaths were due to HCV recurrence.")
23
Morbidity After LT (1) Id Type Delay post LT (Mo) HIV (Log IU/mL)
Opportunistic complications: Id Type Delay post LT (Mo) HIV (Log IU/mL) CD4 cell count HAART Isupp. Therapy 1 Oes. Candidosis 11 3.7 180 3TC/d4T/EFV Tac. 2 23 4 190 TDF/ABC/LPV Tac+MMF+Ster. 3 CMV infect. <1.6 130 Ciclosp. 14 390 TDF/FTC/FPV/RTV Ciclosp. + MMF + Ster. 5 CMV colitis 21 80 3TC/ABC/ATV/RTV 6 Gg tubercul. 12 410 3TC/ABC/FPV/RTV We observed oppotunistic infections after LT in 6 patients 23
 HIV (Log IU/mL) CD4 cell. count. HAART. Isupp. Therapy. 1. Oes. Candidosis TC/d4T/EFV. Tac TDF/ABC/LPV. Tac+MMF+Ster. 3. CMV infect. < Ciclosp TDF/FTC/FPV/RTV. Ciclosp. + MMF + Ster. 5. CMV colitis TC/ABC/ATV/RTV. 6. Gg tubercul TC/ABC/FPV/RTV. We observed oppotunistic infections after LT in 6 patients. 23.")
24
Rectum Adenocarcinoma
Morbidity After LT (2) De novo malignancies: Id Type Delay post LT (Mo) HIV (Log IU/mL) CD4 cell count HAART Isupp. Therapy 1 Rectum Adenocarcinoma 32 <1.6 210 3TC/d4T/EFV Ciclo + Everolimus 2 Cholangiocarcinoma 120 ATZ/TDF/FTC Tac 24
 De novo malignancies: Id. Type. Delay post LT (Mo) HIV (Log IU/mL) CD4 cell. count. HAART. Isupp. Therapy. 1. Rectum Adenocarcinoma. 32. < TC/d4T/EFV. Ciclo + Everolimus. 2. Cholangiocarcinoma ATZ/TDF/FTC. Tac. 24.")
25
Evolution après TH pour coinfection VIH VHC

26
De la cohorte VIH+/VHC+
Survie cumulée après TH d’une cohorte de 105 patients infectés par le VIH Survie des patients : De la cohorte VIH+/VHC+ Mediane : ± [ ] Months Survie des patients : De la cohorte VIH+/VHB+ 24 48 72 96 2yrs: 94% 5yrs: 89% HBV+ p=0.001 HBV- 5 ans: 75% HCV- Survie cumulée 5 ans: 58% p=0.04 In the HIV/HCV coinfected group, The 2-year and 5 year patient survival estimates were 75% and 58% respectively HCV+ Months Récidive de l’infection VHC 26

27
Récidive de l’infection VHC après TH
Biopsies hépatiques systématiques Progression vers une fibrose ≥ F2 après TH chez les patients VIH+/VHC+ et VIH-/VHC+ Pas de HFC (n=48) HFC (n=11) 19% Survie avec ou sans HFC P=0.004 Antonini et al. Am J Transplant 2011 Survie médiane: 26 ± 4.7 mois mois ,2 ,4 ,6 ,8 1 6 12 18 24 30 36 42 48 54 60 Intervalle après TH (mois) % without F2 to F4 HIV-/HCV+ HIV+/HCV+ 94% 91% 82% 77% 46% 83% 74% 24% Log rank p<0.0001 A more accelarated HCV recurrence after liver transplantation has been noted in HIV/HCV coinfected patients. Particularly, the agressive, severe cholestatic form and sepsis are the leading causes of death after liver transplantation. Duclos-Vallée et al. Hepatology 2008
 HFC (n=11) 19% Survie avec ou sans HFC. P= Antonini et al. Am J Transplant Survie médiane: 26 ± 4.7 mois. mois. ,2. ,4. ,6. , Intervalle après TH (mois) % without F2 to F4. HIV-/HCV+ HIV+/HCV+ 94% 91% 82% 77% 46% 83% 74% 24% Log rank p< A more accelarated HCV recurrence after liver transplantation has been noted in HIV/HCV coinfected patients. Particularly, the agressive, severe cholestatic form and sepsis are the leading causes of death after liver transplantation. Duclos-Vallée et al. Hepatology")
28
Efficacité du traitement contre le VHC
N = 36 / 59 patients traités 5 10 15 20 25 SVR PR NR Rechute n=6 (16.6%) n=24 (64%) n=1 (3%) Nécessité urgente de traitements efficaces contre le VHC
 n=24. (64%) n=1. (3%) Nécessité urgente de traitements efficaces contre le VHC.")
29
Traitement antiviral avec INF-Peg + Riba + antiviraux directs (Télaprévir ou Bocéprévir)
Quels sont les problèmes rencontrés? Interactions médicamenteuses? Effets secondaires (anémie, infections)? Résistance (Charge virale élevée)?
 Résistance (Charge virale élevée)")
30
Evolution après TH pour coinfection VIH-VHB

31
Données cliniques et virologiques lors de la TH chez les patients VIH-VHB
Tateo Aids 2009

32
Evolution après la TH chez les patients coinfectés VIH-VHB
Tateo Aids 2009

33
Considération générale chez le patient VIH candidat à la TH
Evaluation pré TH du statut VIH avec un spécialiste du VIH - CD4 > 150 / mm3 - Recherche infection CMV, candidose oesophagienne, mycobacterie - Evaluation cardiovasculaire (insuffisance coronarienne) - Recherche du papilloma virus chez les hommes homosexuels (risque de cancer épidermoïde de l’anus)
 - Recherche du papilloma virus chez les hommes homosexuels (risque de cancer épidermoïde de l’anus)")
34
Considérations spécifiques pour le patient VIH-VHB
Peu de différence avec patient monoinfecté VHB Coordination avec spécialiste VIH pour traitement Possible hépatites fulminantes (réactivation VHB, reconstitution immune). TH possible avec ARN VIH +. Risque infections opportunistes Pas de modification du traitement VIH sans tenir compte du VHB Information de la nécessité d’une prophylaxie à long terme contre le VHB
. TH possible avec ARN VIH +. Risque infections opportunistes. Pas de modification du traitement VIH sans tenir compte du VHB. Information de la nécessité d’une prophylaxie à long terme contre le VHB.")
35
Conclusion Résultats de la TH pour VIH VHB (et VHD) excellents
Prévention de la récidive par Nuc + IM Glob anti HBs Pas de récidive de l’infection par le VHB mais patients à risque Pas de progression du VIH après TH Patients CHC : - Possible risque plus élevé de sortie de liste - Récidive après TH liés au critères du CHC (Milan…)
")
36
Acknowledgements Medical and Surgical Team Centre Hépato-Biliaire
Pathology Unit M Sebagh C Guettier Virology Unit AM Roque-Afonso E Dussaix Infectious Diseases Unit E Teicher D Vittecoq

Présentations similaires