Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
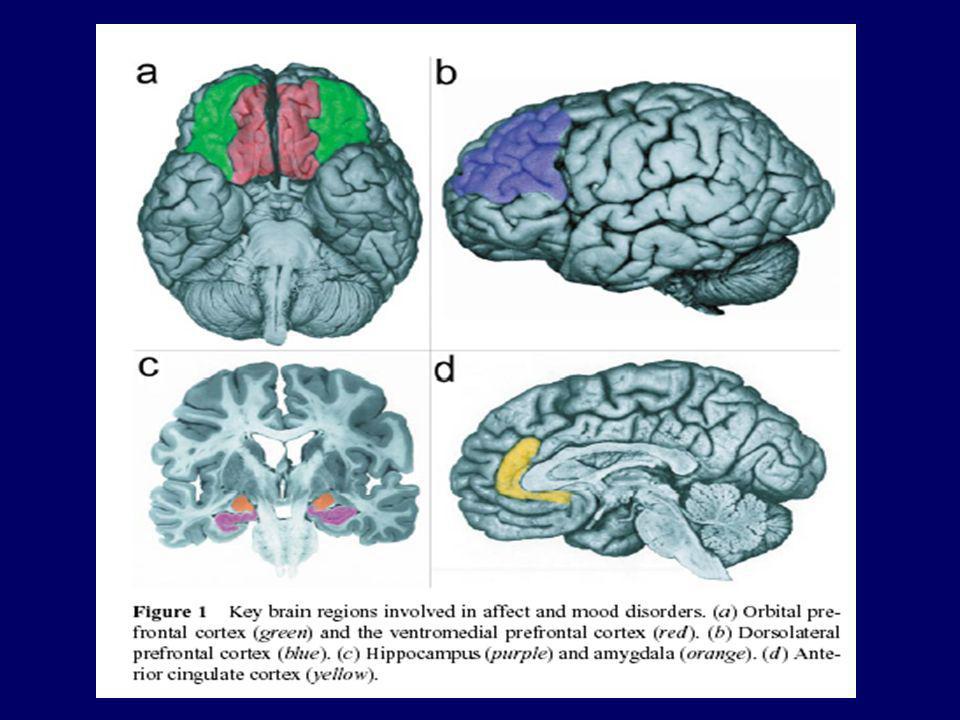
Bases anatomo-fonctionnelles de la dépression
Fossati, P; Allilaire, J.F CNRS UMR 7593, Service de Psychiatrie d’Adultes, GH Pitié-Salpétrière Paris

2
Hippocampus, Parahippocampal C
ABNORMALITIES OF METABOLISM, STRUCTURE IN MDD Dorsal Anterior Cingulate Dorsal Caudate Dorsal Medial / Anterolateral PFC Posterior Cingulate Ventral Anterior Cingulate Medial Thalamus Orbital C, Ventrolateral PFC, Anterior Insula Medial Cerebellum OFC: promotes extincition of fear conditioning PFC:promotes extincition of fear conditioning Inhibits acquisition of fear conditioning. Hippocampus, Parahippocampal C Ventral Striatum Amygdala Areas where neuropathological / morphometric changes reported Indicates direction of metabolic abnormality relative to control or

3
Other Neuromorphometric Abnormalities in Mood Disorders
Corpus callossal areas reduced in MDD and BD mothers and their high risk, female offspring Third ventricle enlarged in BD May implicate medial dorsal, paraventricular thalamic nuclei Raphe size (area stained by 8-OH-DPAT) decreased in depressed suicides Lateral ventricle enlargement in bipolar type I, psychotic, and late-onset depression * Reviewed in Drevets, Dialogues Clin Neurosci, 6(2): , 2004
 decreased in depressed suicides. Lateral ventricle enlargement in bipolar type I, psychotic, and late-onset depression. * Reviewed in Drevets, Dialogues Clin Neurosci, 6(2): ,")
4
Limitations to the Sensitivity of Neuroimaging
Small effect size of abnormalities (generally < 1) Low spatial resolution Small signal size Measurement variability Anatomical variability Variability imposed by clinical/ biological heterogeneity within samples identified using current nomenclature Diagnostic specificity not established Sensitivity to medication effects Limited number of radioligands available
 Low spatial resolution. Small signal size. Measurement variability. Anatomical variability. Variability imposed by clinical/ biological heterogeneity within samples identified using current nomenclature. Diagnostic specificity not established. Sensitivity to medication effects. Limited number of radioligands available.")
5
METABOLIC CHANGES ASSOCIATED WITH EFFECTIVE
ANTIDEPRESSANT-DRUG TREATMENT Drevets et al, Eur Neuropsychoparmacology, 2002 & Neurobiological Found- ation of Mental Illness, Oxford, 2004; Kennedy et al Am J Psychiatry, 2001

6
METABOLIC CHANGES ASSOCIATED WITH EFFECTIVE
ANTIDEPRESSANT-DRUG TREATMENT Drevets et al, Eur Neuropsychoparmacology, 2002 & Neurobiological Found- ation of Mental Illness, Oxford, 2004; Kennedy et al Am J Psychiatry, 2001

7
Treatment Effects on Ventral Prefrontal Cortex (PFC), Anterior Cingulate Cortex (ACC) Activity in MDD Treatment Change: post- vs pre-Tx Brody et al 2001 Paroxetine Buchsbaum et al 1997 Setraline Ventral ACC Cohen et al 1992 Phototherapy Medial Orbital C Drevets & Raichle 1992 Desipramine Left VLPFC Drevets et al VLPFC and Orbital C, Ventral ACC Drevets et al 2002 Citalopram Duan et al. 2004 Pramipexole Ebert et al 1991 Sleep deprivation Orbital C- responders Malizia et al. 1994 Subcaudate Tractotomy Ventral PFC, Ventral ACC Mayberg et al 1999 Various AD drugs Orbital/Ant insula, Ventral ACC Nobler et al 1994 ECT Left VLPFC, responders Kennedy et al 2002 Fluoxetine Left Lateral Orbital/ Ant insula Rubin et al 1994 Nortriptyline or sertraline Trivedi et al 1994 Orbital C Wu et al 1992 ACC, responders VLPFC, Orbital C

8
Models of Mood Disorders (II)
Need to explain recurrent and episodic nature of mood disorders progressive nature of the disorder over time persistent impairment in cognition and emotion regulation New Framework: impairment in structural plasticity and cellular resilience Chronicbrain changes may be associated with depression or bipolar disorder Models of mood disorders need to explain these chronic brain changes in patients as well as the persistent impairment in cognition and emotion regulation and the progressive nature of the disorder over time Recent framework suggest that impairment in structural plasticity and.... May be relevant in mood disorders Pllasticity defines how brain adapts his structure to internal and external stimuli and how it repairs itself In this talk I would like to review evidence from imaging and cognitive studies supporting this framework and the neural network

10
Structural findings in Bipolar Disorder (I)
Increase of Amygdala volume Decrease of subgenual volume Change in left dorsal cingulate volume No change in temporal and hippocampus volume Whitematter hyperintensities in young patients Structural brain imaging studies using MRI in bipolar disorder have shown ..have been described in patients with early depression and familial bipolar depression - Unlike depressed patients, bipolar did not show - in untreated patients compared to patients with lithium Finally These White matter intensities disrupt neural connectivity necessary for normal affective and cognitive functioning

11
Structural findings in Bipolar Disorder (II)
Contradictory findings Definition of anatomical regions Small samples Sample heterogeneity bipolar I and II with or without psychotic symptoms Trait vs state Comorbidity: alcohol or substance abuse Treatment Imaging studies produced contradictory results Several factors may explain these contradictory findings The treatment is also a major factor as some recent studies showed than chronic administration of lithium may increase the gray matter volume

12
Structural findings in Bipolar Disorder (III)
Meta-Analysis (Mac Donald et al, Biol Psy, 2004) Age between years 26 studies 404 patients DSMIII-R or DSM-IV bipolar disorder Recurrent illness Metaanalyses tried to control the effects of these factors A recent metanalysis included 26 studies using quantitative MRI techniques 404 Patients aged …were included Patients had… All subject had a recurrent illness with at least two affective episodes
 Age between years. 26 studies. 404 patients. DSMIII-R or DSM-IV bipolar disorder. Recurrent illness. Metaanalyses tried to control the effects of these factors. A recent metanalysis included 26 studies using quantitative MRI techniques. 404 Patients aged …were included. Patients had… All subject had a recurrent illness with at least two affective episodes.")
13
Structural findings in Bipolar Disorder (IV)
Right lateral Ventricular enlargement Hippocampus normal (250 patients) Great heterogeneity and publication bias Only the right later ventricular enlargement distinguished controls from bipolar patients The hippocampus was normal and this analysis included 250 patients The authors emphasized the great….
 Great heterogeneity and publication bias. Only the right later ventricular enlargement distinguished controls from bipolar patients. The hippocampus was normal and this analysis included 250 patients. The authors emphasized the great….")
14
Structural findings in Depression
Whitematter hyperintensities in elderly Abnormalities in prefrontal cortex: orbital, medial, ventral and dorsolateral Reduction of subgenual volume Reduction of caudate nucleus Amygdala? Smaller hippocampal volume Studies in depression have shown Or in patient with late onset depression Abnormalities… was found in The reduction..; has been described in pure familial depressive disease Findings on amydala are more inconsistent with some studies reporting increase, normal or decrease volume Finally the most robust finding is the reduction of hippcampal volume rangign from 9 to 19 %

15
Structural findings in Depression (II)
Hippocampus atrophy Length of illness and duration of depression (Sheline et al, 1999) The hippocampus atrophy has been related to the duration of depression as shown on that picture
 The hippocampus atrophy has been related to the duration of depression as shown on that picture.")
16
Structural findings in Depression (III)
Hippocampus and contradictory findings Duration of depression Number of depressive episode (Mc Queen, 2003) Treatment Gender (women > men) Sexual abuse Slice thickness Clinical characterstics have been implicated in hippocampal volume differences in depression Atrophy of hippocampus has been related to the.. Some recent data suggest that the duration of exposure to antidepressant treatment is negatively correlated to the hippocampal volume Finally parameters of MRI such as the slice thickness may also explain divergent findings…
 Treatment. Gender (women > men) Sexual abuse. Slice thickness. Clinical characterstics have been implicated. in hippocampal volume differences in depression. Atrophy of hippocampus has been related to the.. Some recent data suggest that the duration of exposure to antidepressant treatment is negatively correlated to the hippocampal volume. Finally parameters of MRI such as the slice thickness may also explain divergent findings…")
17
Structural findings in Depression (IV)
Meta-Analysis (Campbell et al, 2004) 434 patients and 379 controls Age from 23 to 86 years Smaller hippocampus if analysis does not include amygdala A recent meta analysis of structural changes of hippocampus in depression included… The hippocampus of depressed patients were smaller than controls if the analysis does not … No other variables were significant moderators of the results
 434 patients and 379 controls. Age from 23 to 86 years. Smaller hippocampus if analysis does not include amygdala. A recent meta analysis of structural changes of hippocampus in depression included… The hippocampus of depressed patients were smaller than controls if the analysis does not … No other variables were significant moderators of the results.")
18
Summary of Structural Imaging studies
Implication of a cortico-limbic network in depression and bipolar disorder Morphometric distinction within the affective spectrum: Amygdala and Bipolar disorder Hippocampus and depression Consistent with post-mortem studies: reduction in number, density and size of glia cells + /- neurons in the same neural network There is a morphometric distinction These brain imaging findings are consistent with

19
Depression and hippocampus
Cause of atrophy? Specificity of atrophy? Functional and clinical signification of atrophy? In the last part of this talk I would like to focus on the hippocampus and depression We have previously said that there is hippocampal volumetric changes in depression

20
We don’t know yet if the hippocampus changes in depression reflect developmental abnormalities, compensatory changes or consequences of the recurrence of depressive episodes per se One main hypothesis relates hippocampus atrophy in depression to Stress and corticosteroids The so-called neurotoxic hypothesis relies on animal studies and studies on Cortisol dysregulation in depression INdeed There are Several corticosteroids receptors in the hippocampus

21
Cause of Hippocampus atrophy
Tissue loss Neuronal loss due to stress and steroids Stress induced reduction of neurotrophic factor (CREB, BDNF) and neurogenesis Glial loss due to glutamate toxicity According to this hypothesis Hippocampal damage in depression…
 and neurogenesis. Glial loss due to glutamate toxicity. According to this hypothesis Hippocampal damage in depression…")
22
Specificity of the hippocampus atrophy
Borderline Personality Disorder PTSD Depression Cushing’ s syndrome The hippocampus is involved in …..

23
Signification of the hippocampus atrophy
Hippocampus function Learning and Memory Regulation of stress response - Emotion regulation The hippocampus is involved in …..

24
Signification of the hippocampus atrophy (II)
Memory deficits and acute depression Depression with HPA abnormalities Patients with multiple episode compared to first episode (Fossati et al, 2004) Persistent deficits in euthymic phase associated with the number of depressive episode (Kessing et al, 1998) Correlation of memory deficits and hippocampus volume? Cortisol reduces blood flow in hippocampus during retrieval (De quervain, 2000) Memory deficits have been found in Recently we demonstrated Correlation od memory deficits and hippocampus changes in structural and function remains to be determined A recent fMRI study shows acute administration of cortisol
 Persistent deficits in euthymic phase associated with the number of depressive episode (Kessing et al, 1998) Correlation of memory deficits and hippocampus volume Cortisol reduces blood flow in hippocampus during retrieval (De quervain, 2000) Memory deficits have been found in. Recently we demonstrated. Correlation od memory deficits and hippocampus changes in structural and function remains to be determined. A recent fMRI study shows acute administration of cortisol.")
25
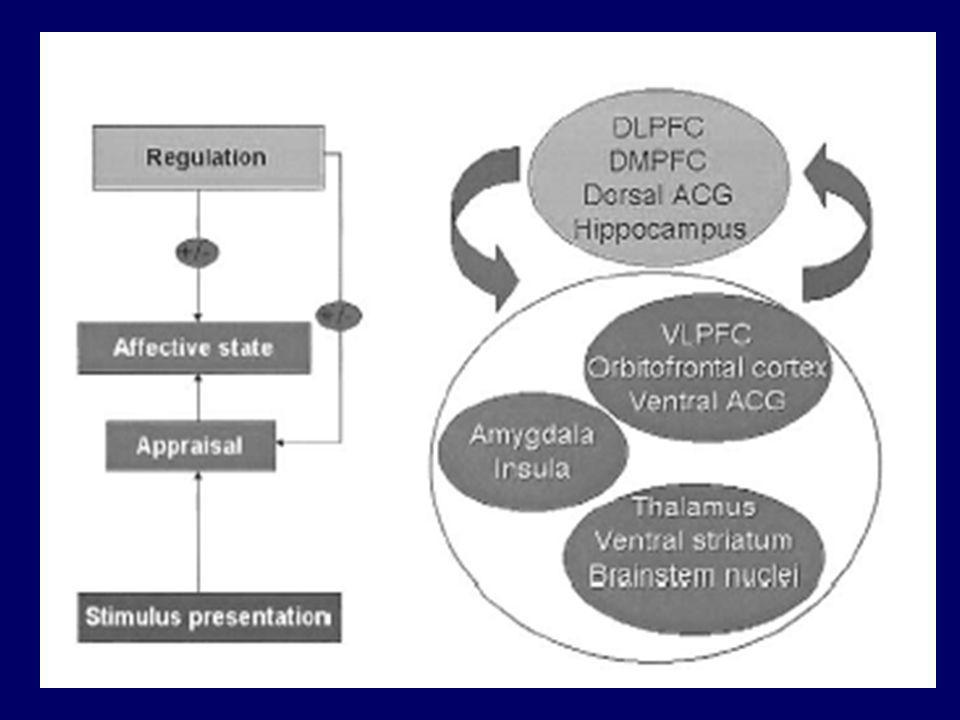
Régulation émotionnelle
Processus: Maintien, diminution ou augmentation des réactions émotionnelles (expérience, expression) Modulation de la réponse comportementale ou neurovégétative Fonction sociale (ex. inhibition des réactions d’agressivité, de colère; contextualisation des réponses émotionnelles)
 Modulation de la réponse comportementale ou neurovégétative. Fonction sociale (ex. inhibition des réactions d’agressivité, de colère; contextualisation des réponses émotionnelles)")
27
Capacité de régulation émotionnelle
- niveau réflectif inférieur : processus automatiques (non conscients, capacités d’adaptation, mécanismes de défense) - niveau réflectif supérieur : conscience des émotions et des émotions et pensées envers les émotions = mode méta-émotif - Processus cognitifs: réévaluation, suppression…. Mayer & Gaschke (1988); Charron et al. (2003)
 - niveau réflectif supérieur : conscience des émotions et des émotions et pensées envers les émotions = mode méta-émotif. - Processus cognitifs: réévaluation, suppression…. Mayer & Gaschke (1988); Charron et al. (2003)")
28
DEPRESSION: TROUBLE MULTIDIMENSIONNEL
Motor symptoms Symptômes moteurs Dérégulation Humeur Symptômes végétatifs Depression is a common disorder Many symptoms define a Depressive episode Those symptoms include… Thinking the depression as a multidimensional disorder implies At a first level there is not a ‘unique cognitive or biological model explaining all the symptoms of depression At the brain level we can hypothesize that the depression does not involve discrete brain areas but nmplies multiple neural systems in interaction Troubles cognitifs

29
Dérégulation de l’humeur et dépression
Tristesse intense et durable Labilité de l’humeur Dysphorie Mood dysregulation in depression is characterized by an intense and persistent sadness not adapted to the context We can also observe mood lability, frequent mood swings especially in bipolar patients finally many depressed patients complain about loss of pleasure and interest during activity This anhedonia is more pronounced for sensorial pleasure rather than social pleasure What are the neural structures that regulate normal mood changes in normal subjects? Are these structures involved in the pathophysiology of depression?

30
Expérience d’induction d’une tristesse
Méthodes Scripts autobiographiques Musique films Déplétion en tryptophane TMS Mood induction are experimental techniques used to study mood regulation in normal controls and patients Mood induction technique has a long history in experimental psychology Several methods combined with brain imaging technique (especially PET scan) have been used o provoke sadness Mayberg et al, asked subjecct to retrieve personal sad events during scanning The images of PET scan were acquired only after the sad state was reached in order to avoid confounding effect of due to the memory stategies
 have been used o provoke sadness. Mayberg et al, asked subjecct to retrieve personal sad events during scanning. The images of PET scan were acquired only after the sad state was reached in order to avoid confounding effect of due to the memory stategies.")
31
Induced Sadness Healthy Volunteers
F9 F9 F9 F9 Rt Cg25 cd Cg25 ins ins ins ins Cg25 + 4 z-score - 4 31 pCg pCg In that study published in the American Journal of Psychiatry Helen Mayberg using a memory technique asked normal subject to get sad and maintain that sadness during scanning So we observe here not the acute change from euthymia to sadness but how the brain maintain an acute sadness during a short time What did she observe? she found An increase of cerebral blood flow in ventral areas especially the insula, the subgenual cingulate associated with a decrease in dorsal cortical areas namely -dorso-lateral prefrontal areas (usually involved in working memory task and executive task) posterior cingulate region The acute change in normal controls was similar to changes observed when depressed patients recover from their depression This result suggest that these regional interactions mediate the behavioral relationships between cognition and emotion Ant 25 hth hth Cg25 Cg25 Cg25 x= 0 Healthy Volunteers
 posterior cingulate region. The acute change in normal controls was similar to changes observed when depressed patients recover from their depression. This result suggest that these regional interactions mediate the behavioral relationships between cognition and emotion. Ant. 25. hth. hth. Cg25. Cg25. Cg25. x= 0. Healthy Volunteers.")
32
Lévesque et al, 2003

33
Induced Sadness Depression Recovery Healthy Volunteers
F9 F9 F9 F9 Rt Cg25 cd Cg25 ins ins ins ins Cg25 + 4 z-score - 4 31 pCg pCg In that study published in the American Journal of Psychiatry Helen Mayberg using a memory technique asked normal subject to get sad and maintain that sadness during scanning So we observe here not the acute change from euthymia to sadness but how the brain maintain an acute sadness during a short time What did she observe? she found An increase of cerebral blood flow in ventral areas especially the insula, the subgenual cingulate associated with a decrease in dorsal cortical areas namely -dorso-lateral prefrontal areas (usually involved in working memory task and executive task) posterior cingulate region The acute change in normal controls was similar to changes observed when depressed patients recover from their depression This result suggest that these regional interactions mediate the behavioral relationships between cognition and emotion Ant 25 hth hth Cg25 Cg25 Cg25 x= 0 Healthy Volunteers Depressed Patients
 posterior cingulate region. The acute change in normal controls was similar to changes observed when depressed patients recover from their depression. This result suggest that these regional interactions mediate the behavioral relationships between cognition and emotion. Ant. 25. hth. hth. Cg25. Cg25. Cg25. x= 0. Healthy Volunteers. Depressed Patients.")
34
Régulation de l’humeur et dépression (2)
Tristesse aigue active les mêmes structures neurales impliquées dans la tristesse chronique de la dépression Régions Corticales (préfrontale) et Limbiques (subgénuale, hippocampe) This ‘emotional task’ involves cognitive and emotional brain regions and is associated with Cortical and limbic interactions
 et Limbiques (subgénuale, hippocampe) This ‘emotional task’ involves cognitive and emotional brain regions and is associated with. Cortical and limbic interactions.")
35
Vulnérabilité à la dépression
Trait ou dimension de personnalité Génétique Environnement Mesures de ces traits de personnalité: TCI or NEO ‘Neuroticism’: sensibilité accrue aux affects négatifs et un facteur de risque de nombreux états psychopathologiques An other way to investigate the neural structures involved in normal and pathologic mood regulation is to investigate subjects at risk for depression Many risk factors for depression have been described including genetic and environmental factorsPersonality trait or dimension have been associated with an increase susceptibility to depression Neuroticism, defined as an increased sensitivity to negative affect, a risk factor for depression Individual variability in emotional reactivity is an area of growing research interest, as suggested by recent studies examining genetic links to the personality trait Neuroticism (Lesch and Mossner, 1998; Neumeister et al., 2002), the temperamental hypersensitivity to negative stimuli or the tendency to experience exaggerated negative mood states in situations of emotional instability or dissonance (Santor et al., 1997). High trait levels of neuroticism are of potential clinical interest, as this temperament marker has been suggested to increase vulnerability to psychopathology such as depression, anxiety, biopolar disorder and aggression (Beck et al., 1979; Henriques et al., 1994; Teasdale, 1999; Segal et al., 1999) In both groups there was a common pattern of increased activity in subgenual cingulate (Cg25) and hippocampus, along with decreased activity in dorsolateral prefrontal cortex (BA9) associated with acute sadness. This pattern is consistent with previously reported findings in unselected healthy controls (George et al., 1995; Mayberg et al., 1999; Damasio et al., 2000; Liotti et al., 2002) suggesting that these regions are critical to the normal regulation of acute changes in mood state. A second, group-specific pattern was seen only in the hiNloE group under emotional stress (i.e. with sad mood provocation). This pattern again involved increased activity in Cg25 but in association with decreased medial prefrontal activity, a pattern not seen in the loNhiE group. .
, the temperamental hypersensitivity to negative stimuli or the tendency to experience exaggerated negative mood states in situations of emotional instability or dissonance (Santor et al., 1997). High trait levels of neuroticism are of potential clinical interest, as this temperament marker has been suggested to increase vulnerability to psychopathology such as depression, anxiety, biopolar disorder and aggression (Beck et al., 1979; Henriques et al., 1994; Teasdale, 1999; Segal et al., 1999) In both groups there was a common pattern of increased activity in subgenual cingulate (Cg25) and hippocampus, along with decreased activity in dorsolateral prefrontal cortex (BA9) associated with acute sadness. This pattern is consistent with previously reported findings in unselected healthy controls (George et al., 1995; Mayberg et al., 1999; Damasio et al., 2000; Liotti et al., 2002) suggesting that these regions are critical to the normal regulation of acute changes in mood state. A second, group-specific pattern was seen only in the hiNloE group under emotional stress (i.e. with sad mood provocation). This pattern again involved increased activity in Cg25 but in association with decreased medial prefrontal activity, a pattern not seen in the loNhiE group. .")
36
Figure 1. Seed PLS LV1 – + Keightley et al, Neuroimage, 2003 PAS NAS
Neutral Sad dlpf9 oF11 47 mF10 Ins pm6 pcg31 rcg24 11 Z= -12 Z= 0 Z= 24 Keightley et al, Neuroimage, 2003

37
Mood Induction in Depression
Rem UPD F9 F9 F9 F10 Cg Cg F10 F10 Memory induced sadness/tearful PET - signal + Liotti et al, 2002

38
Résumé des études d’induction de l’humeur
Tristesse aigüe normale et tristesse pathologique engagent les mêmes structures cérébrales Régions corticales, limbiques et paralimbiques (hippocampe, cingulum subgénual) Test d’induction de l’humeur révèle une vulnérabilité à la dépression Neuroticism, defined as an increased sensitivity to negative affect, a risk factor for depression Vulnerability mediated by cognition and mood dysregulation Cognitive model of depression (Beck) Ruminative coping style (Noelen-Hoeksema, 1987)
 Test d’induction de l’humeur révèle une vulnérabilité à la dépression. Neuroticism, defined as an increased sensitivity to negative affect, a risk factor for depression. Vulnerability mediated by cognition and mood dysregulation. Cognitive model of depression (Beck) Ruminative coping style (Noelen-Hoeksema, 1987)")
39
Cortex Médian Préfrontal (CMPF)
Cortex préfrontal ventro-médian: intégration des émotions dans les processus de prise de décision (Damasio) Représentation des états d’activation périphérique du SNA (‘cardiovascular arousal’; Critchley et al, 2000) Evaluation émotionnelle (Phan, 2002) Théories de l’esprit (Gallagher et al, 2003) Among these different studies we discussed about a specific region The medial prefrontal cortex What is the function of this region? Many functional imaging studies activated that regions and several functions have been proposed
 Représentation des états d’activation périphérique du SNA (‘cardiovascular arousal’; Critchley et al, 2000) Evaluation émotionnelle (Phan, 2002) Théories de l’esprit (Gallagher et al, 2003) Among these different studies we discussed about a specific region. The medial prefrontal cortex. What is the function of this region Many functional imaging studies activated that regions and several functions have been proposed.")
40
Anhedonia and depression
Controls Depressed

41
Goldapple et al 2003

42
Sommaire sur le CMPF dans la dépression
CMPF: traitement selon une perspective personnelle des stimuli émotionnels Déprimés ont du mal à moduler l’activité du CMPF Activité anormale du CMPF: corrélat neuronal des biais de traitement dans la dépression

43
Contrôle cognitif Fonctions exécutives: planification, monitoring des erreurs, inhibition, allocation des ressources attentionnelles Régulation émotionnelle: distraction, rumination, changement de perspective….

44
Pochon, J.B., Levy, R., Fossati et al, PNAS, 2002
- Subjects performed a letter variant of the « n-back » procedure, during fMRI scanning - the n-back tasks were performed in association with different monetary rewarding values (up to 240 €) v X t p P g n-back 100 % instruction performance temps We conducted a series of behavioral and fMRI studies in normal subjects and depressed patients using a task known to require executive and attentional resources The task we selected is the n-back task according to which subjects were to indicate whether a letter presented on the screen (the "target" stimulus) is similar of different from a letter previously presented (the "cue stimulus"; see Figure 1). This procedure requires the participant to maintain and permanently update the relevant pieces of information in WM. Load and mental manipulation within WM were incremented by using three different levels of the n-back task : 1-back (maintenance of one piece of information in WM within the interval between the cue and the target stimuli) and 2- and 3-back (interposition of one or two distractors between the cue and the target stimuli, each distractor becoming a cue for the next trial). In a first experiment, in order to assess the influence of the context, we introduced trials rewarded with money Therefore there was three levels of complexity And two type of trials: rewarded or non rewarded
 v. X. t. p. P. g. n-back % instruction. performance. temps. We conducted a series of behavioral and fMRI studies in normal subjects and depressed patients using a task known to require executive and attentional resources. The task we selected is the n-back task. according to which subjects were to indicate whether a letter presented on the screen (the target stimulus) is similar of different from a letter previously presented (the cue stimulus ; see Figure 1). This procedure requires the participant to maintain and permanently update the relevant pieces of information in WM. Load and mental manipulation within WM were incremented by using three different levels of the n-back task : 1-back (maintenance of one piece of information in WM within the interval between the cue and the target stimuli) and 2- and 3-back (interposition of one or two distractors between the cue and the target stimuli, each distractor becoming a cue for the next trial). In a first experiment, in order to assess the influence of the context, we introduced trials rewarded with money. Therefore there was three levels of complexity. And two type of trials: rewarded or non rewarded.")
45
DEPRESSION: TROUBLE MULTIDIMENSIONNEL
Motor symptoms Symptômes moteurs Humeur + Émotions anormales Symptômes végétatifs Depression is a common disorder Many symptoms define a Depressive episode Those symptoms include… Thinking the depression as a multidimensional disorder implies At a first level there is not a ‘unique cognitive or biological model explaining all the symptoms of depression At the brain level we can hypothesize that the depression does not involve discrete brain areas but nmplies multiple neural systems in interaction Troubles cognitifs

46
Population Témoins Déprimés Age 29 ans 33,8 ans 5 H / 5 F 3 H / 7 F
Sex ratio Education 14,6 ans 14,7 ans Beck / MADRS 0 / 0 17,8 / 26 Nb d’épisodes 2,4 (1 - 4)
")
47
Repeated-measures Anova (3x2)
0-Back : Student t-test T= 0.24, ns Repeated-measures Anova (3x2) Pas d’effet Groupe : F(1,18)=0.28, ns Effet complexité : F(2,17)=63.9, p<0.001 Pas d’interaction G x C : F(2,17)=0.13, ns 0-Back : 99,1% / 98,8% 2-Back : 80,9% / 78,7% 1-Back : 96% / 93,6% 3-Back : 75,6% / 74,6%
 Pas d’effet Groupe : F(1,18)=0.28, ns. Effet complexité : F(2,17)=63.9, p< Pas d’interaction G x C : F(2,17)=0.13, ns. 0-Back : 99,1% / 98,8% 2-Back : 80,9% / 78,7% 1-Back : 96% / 93,6% 3-Back : 75,6% / 74,6%")
48
Repeated-measures Anova (3x2)
Pas d’effet groupe : F(1,18)=0.41, ns Effet complexité : F(2,17)=84.7, p<0.001 Pas d’interaction G x C : F(2,17)=0.23, ns N.S.
=0.41, ns. Effet complexité : F(2,17)=84.7, p< Pas d’interaction G x C : F(2,17)=0.23, ns. N.S.")
49
Effet principal du Groupe
Two samples t-tests (contrastes 1vs0+2vs0+3vs0) p < 0.001, uncorrected ; cluster-size 5 voxels * Aucune activation pour la comparaison Témoins vs Déprimés Cluster-level : Prémoteur médian/ CCA (BA 6/32) : p=0.013 ; CPFDL (BA46) : p=0.046 ; Prémoteur/Broca (BA 6/44) : p=0.005
 p < 0.001, uncorrected ; cluster-size 5 voxels. * Aucune activation pour la comparaison Témoins vs Déprimés. Cluster-level : Prémoteur médian/ CCA (BA 6/32) : p=0.013 ; CPFDL (BA46) : p=0.046 ; Prémoteur/Broca (BA 6/44) : p=")
50
Résultats IRMf : Tâche N-Back Effet aléatoire
Témoins Déprimés Uncorrected; p< 0.001, cluster size 5 voxels

51
Résultats IRMf : Désactivations RFX
1-Back 2-Back 3-Back Témoins Déprimés Uncorrected; p< 0.001, cluster size : 5 voxels

52
Modulation du CPFVL avec l’augmentation de la complexité
CPFVL gauche – ROI 10 mm ( ) Augmentation de l’activité p/r au 0-Back 0,28 0,36 0,29 0,26 0,16 0,13 Sujets témoins Patients déprimés
 Augmentation de l’activité p/r au 0-Back. 0,28. 0,36. 0,29. 0,26. 0,16. 0,13. Sujets témoins. Patients déprimés.")
53
Courbe HDR dans le CPFDL (BA 46)
CPFDL gauche (BA46) – ROI 5 mm ( ) Augmentation de l’activité p/r au 0-Back 0,41 0,27 0,34 0,26 0.24 0,24 0,16 Sujets témoins Patients déprimés
 – ROI 5 mm ( ) Augmentation de l’activité p/r au 0-Back. 0,41. 0,27. 0,34. 0, ,24. 0,16. Sujets témoins. Patients déprimés.")
54
Modulation du CPFM avec l’augmentation de la complexité
CPFM – ROI 10 mm (0 54 3) Diminution de l’activité p/r au 0-Back -0,32 -0,23 -0,38 -0,59 -0,45 -0,62 Sujets témoins Patients déprimés
 Diminution de l’activité p/r au 0-Back. -0,32. -0,23. -0,38. -0,59. -0,45. -0,62. Sujets témoins. Patients déprimés.")
55
Résumé des études avec le n-back
Sujet normal: effort cognitif associé avec des interactions cortico-limbiques Déprimé: interactions cortico-limbiques anormales lors d’un effort cognitif To summarize these fMRI studies using cognitive challenge

56
Interactions cortico-limbiques et dépression
dérégulation de l’humeur Augmentation de la sensibilité à l’effort cognitif Biais Emotionnel: anomalie du CMPF To summarize the studies presented Abnormal cortical limbic interactions May subserve

57
Models of Mood disorders (1)
genetic gender temperament HPA, SERT Biological Vulnerability ExogenousStressors environment early insults life events acute v. chronic homeostasis family hx HPA reactivity gene polymorph NEO inventory brain lesions Brain treatment decompensation Several factors are implicated in the pathophysiology in depression including genetic, environnemental and the capacity of brain to adapt to cognitive and emotional demands Affective episode phenotype Adapted from Mayberg & Fossati, in press, 2004

58
Philipps et al, 2003

59
Rostral Cingulate Activity
Prognostic Marker: Rostral Cingulate Activity A B C Cg24a 24a 24a Among these subregion One area has been described as a predictor of clinical remission of depressive symptoms after six week of antidepressant (fluoxetine) Non-Responders Responders Full Remission Patients vs Controls
 Non-Responders. Responders. Full Remission. Patients vs Controls.")
60
Saxena et al, 2003

61
Baseline Path Differences with Response to Specific Interventions
Parox-R CBT-R Multiple Drug Failures PF9 mF10 PF9 mF10 aTh aTh Cg24a Cg24a Cg25 Cg25 oF11 oF11 Hpc Hpc

Présentations similaires














 Optic radiations Area V1 OPTIC CHIASMA.>")




