Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

2
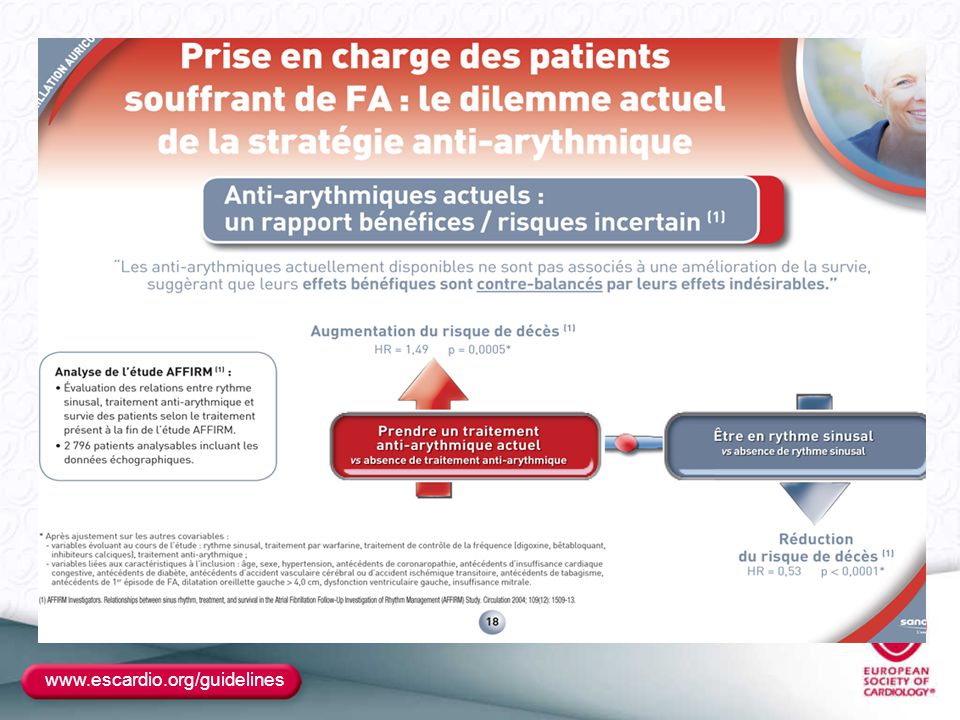
Prise en charge de la FA Triple Problématique
Le Traitement Anticoagulant Indications Les nouveaux Anti-coagulants Le Traitement Rythmologique Un dilemme : Contrôle du rythme ou de la fréquence Le Traitement Anti-arythmique Place du traitement médicamenteux Place du traitement non médicamenteux Ablation

3
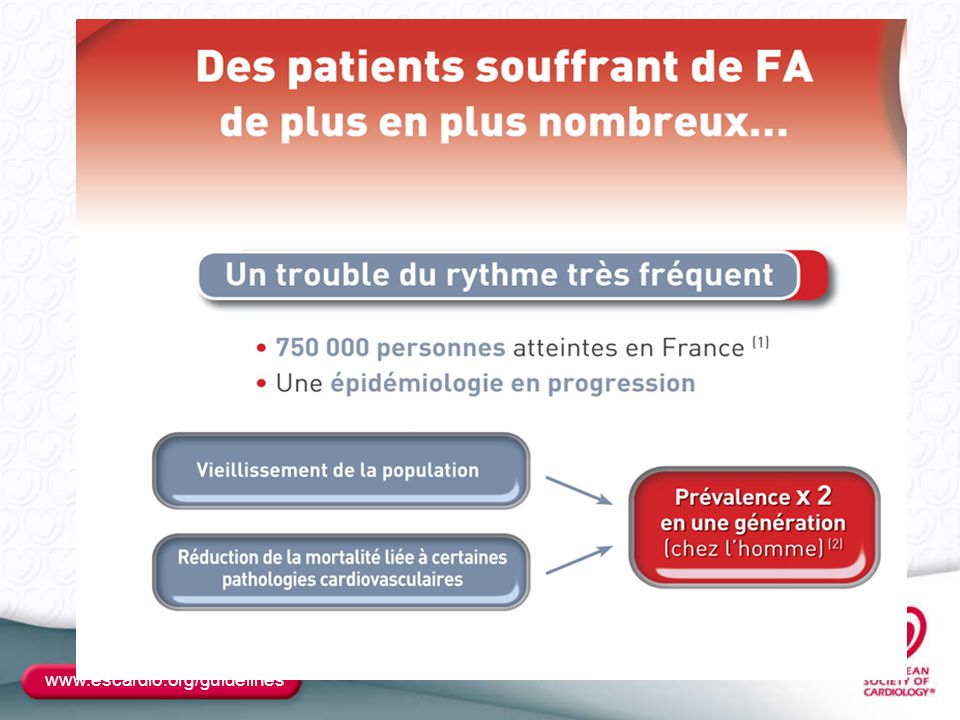
Prévalence de la fibrillation atriale
ÉPIDÉMIOLOGIE 1 Prévalence de la fibrillation atriale Influence de l’âge et du sexe 0,1 0,4 1 1,7 3,4 5,0 7,2 9,1 0,2 0,9 3,0 7,3 10,3 11,1 2 4 6 8 10 12 < 55 55-59 60-64 65-69 70-74 75-79 80-84 > 85 Femmes Hommes Âge Femmes Hommes Prévalence (%) La prévalence de la fibrillation atriale est proche de 0,1 % avant 55 ans, puis augmente rapidement et de façon exponentielle après l’âge de 70 ans, pour atteindre plus de 11 % chez l’homme et 9 % chez la femme, après 85 ans. La prévalence de la FA augmente régulièrement avec l’âge, à partir de 55 ans, avec une prédominance masculine à chaque tranche d’âge ESC D’aprs Go AS et al., 2001, cité par Raatikainen P et al., présentation 1942 actualisée 3
 La prévalence de la fibrillation atriale est proche de 0,1 % avant 55 ans, puis augmente rapidement et de façon exponentielle après l’âge de 70 ans, pour atteindre plus de 11 % chez l’homme et 9 % chez la femme, après 85 ans. La prévalence de la FA augmente régulièrement avec l’âge, à partir de 55 ans, avec une prédominance masculine à chaque tranche d’âge. ESC D’aprs Go AS et al., 2001, cité par Raatikainen P et al., présentation 1942 actualisée. 3.")
8
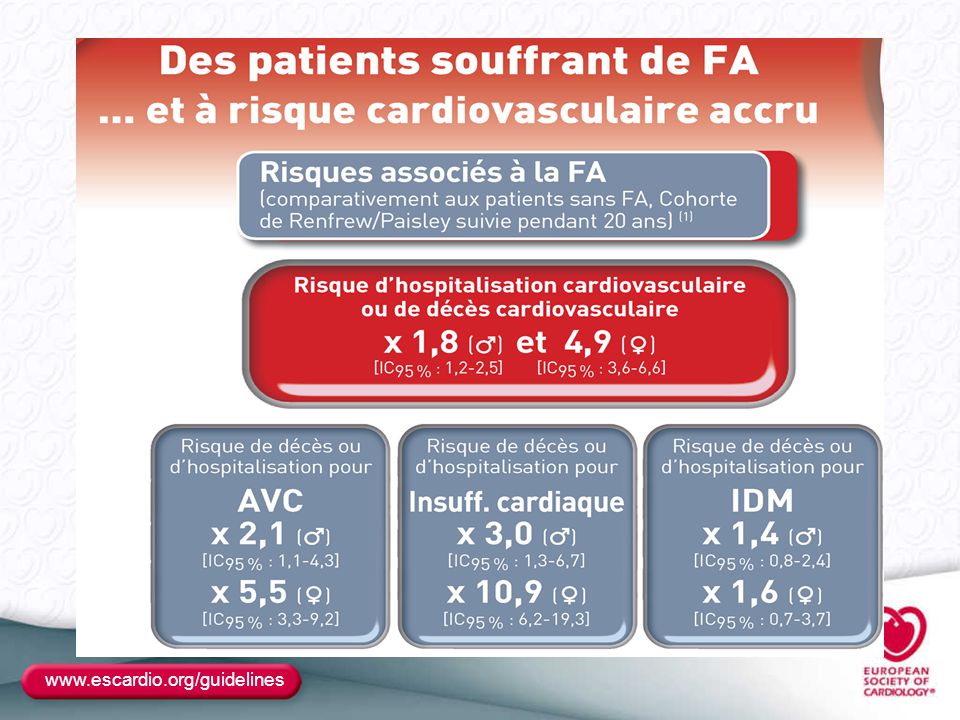
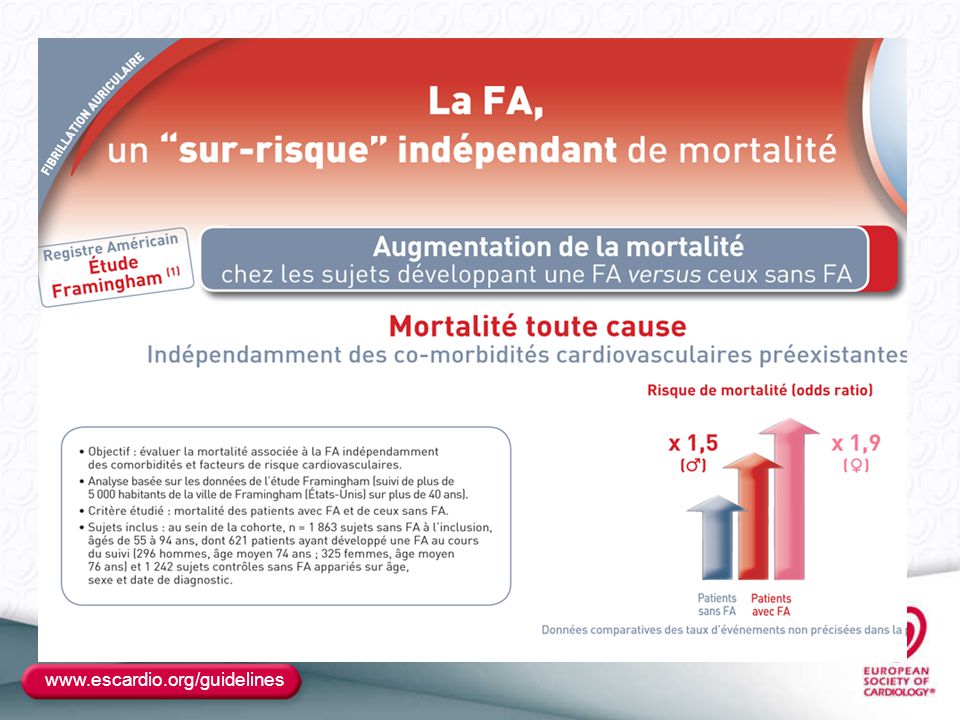
Augmentation de la morbi-mortalité des patients avec FA
ÉPIDÉMIOLOGIE 2 Augmentation de la morbi-mortalité des patients avec FA 2 4 6 8 Framingham Whitehall Manitoba Regional Heart Disease 7 5 2,5 2,1 1,9 1,6 AVC Mortalité RR Plusieurs études épidémiologiques de grande ampleur ont confirmé la surmortalité des patients avec fibrillation atriale par rapport à des groupes contrôles sans arythmie atriale. Ces éléments justifient, pour cette pathologie, une prise en charge médicamenteuse et non médicamenteuse soutenue. ESC D’après Pappone C et al., présentation 296 actualisée 8

26
Prévention TE: Autres points clés
AC Efficace 3 semaines avant et 4 semaines après la cardioversion ++++ Règles identiques si TSA ou Flutter L'association Aspirine/clopidogrel autorisée Si AVK non utilisables Risque Hémorragique Identique quelque-soit le traitement HASBLED systématique : prudence si> 3 Si récidive ischémique sous AVK Majoration du niveau d'hypocoagulation à préférer a l'association d'un anti-agrégant

27
Prévention TE: Autres points clés
Si AVC ischémique Indroduction des AVK à J 15 en absence d'hémorragie AVK CI si hémorragie Si Accident ischémique périphérique AVK dès que possible Si prothése valvulaire INR > 2 en position aortique INR > 2.5 en position mitrale En cas d'intervention a risque hémorragique Si Pt à bas risque TE : interruption sans relais Si Pt à haut risque : Relais par HNF ou HBPM

37
Les Points clés du traitement anti-arythmique
Son but essentiel est la réduction des symptômes liés à la FA+++ Efficacité limitée pour maintenir le rythme sinusal Réduction de la fréquence des récidives En cas d'échec de l'un des traitements on peut en choisir un autre Fréquence des effets secondaires et surtout des effets pro-arythmique ++ Le choix du traitement repose plus sur la sécurité du traitement que sur son efficacité

42
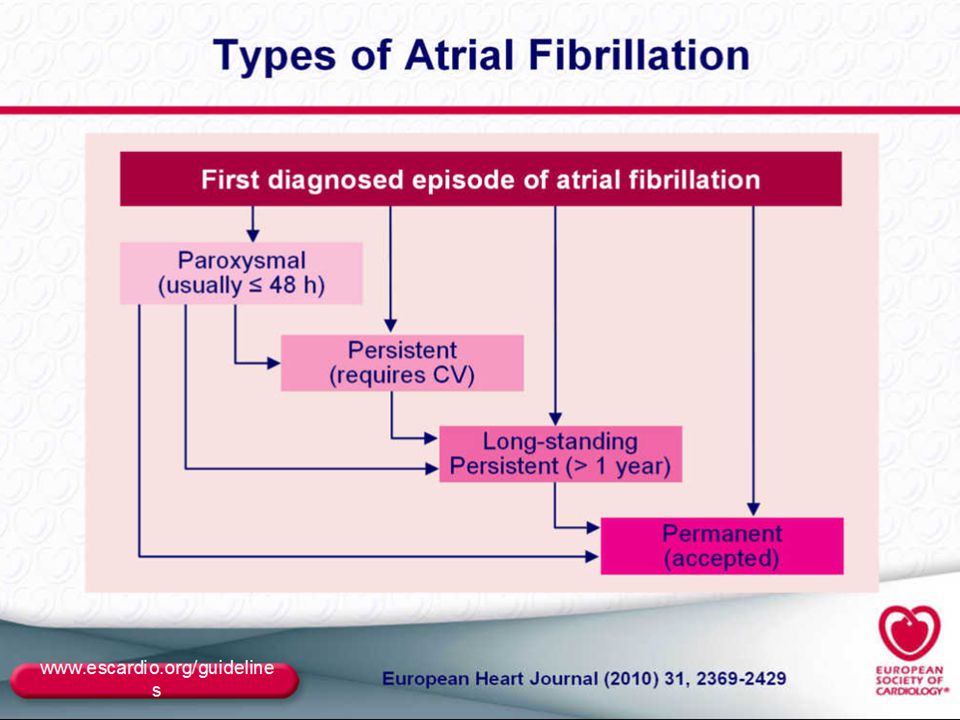
Régularisation de la FA > 48 h
Doit être envisagée si l'on opte pour la stratégie du contrôle du rythme au long cours Par CEE après AC efficace précédée ou non par un TT Anti-arythmique pour augmenter les chances de succès Peut être renouveler chez les Pts hautements symptomatiques Cardioversion pharmacologique: Stratégie « pill in the pocket » En urgence Si FC très rapide et qui répond mal au TT bradycardisant chez un Pt symptomatique En cas de Pré-excitation ventriculaire

43
Traitement préventif des récidives
Dépend de l'existence ou non d'une cardiopathie sous sous-jacente En son absence : Dronédarone Flécainide Propafenone Sotalol Amiodarone : Plus efficace mais ses effets secondaires doivent la faire réserver aux échecs des précédentes En sa présence: Dronédarone et Amiodarone Dronédarone: Efficacité pour réduire les hospitalisations++ Contre-indiquée en stade 3 et 4 de la NYHA ou récemment déstabilisé

50
Stratégie contrôle de fréquence
En aigu Béta-Bloquants et Calcium bloquants Amiodarone et Digilaline si ICC ou HypoTA En cas de WPW CI des BB des CA et de la digitaline Au long cours TT identique sauf la Cordarone Poso a adapter aux symptômes (EE Holter) en évitant les bradycardies et en permettant une bonne adaptation chronotrope Objectif : FC <110/mn initialement ou > 80 au repos et < 110 à l'effort si Pt symptomatique ou si IVG
 en évitant les bradycardies et en permettant une bonne adaptation chronotrope. Objectif : FC <110/mn initialement ou > 80 au repos et < 110 à l effort si Pt symptomatique ou si IVG.")
58
Choix entre contrôle du rythme et de la fréquence
Le contrôle de la FC: PT âgé peu symptomatique si co-morbidités Long passé de FA Le contrôle du rythme: Pt symptomatique malgré un bon contrôle de la FC Pt jeune +/- symptomatique avant une solution radicale (ablation) Si FA secondaire à un facteur déclenchant traité Si le maintient d'un rythme sinusal peut améliorer la situation hemodynamique
 Si FA secondaire à un facteur déclenchant traité. Si le maintient d un rythme sinusal peut améliorer la situation hemodynamique.")
61
Ablation de la FA Ablation d'un Flutter est toujours indiquée
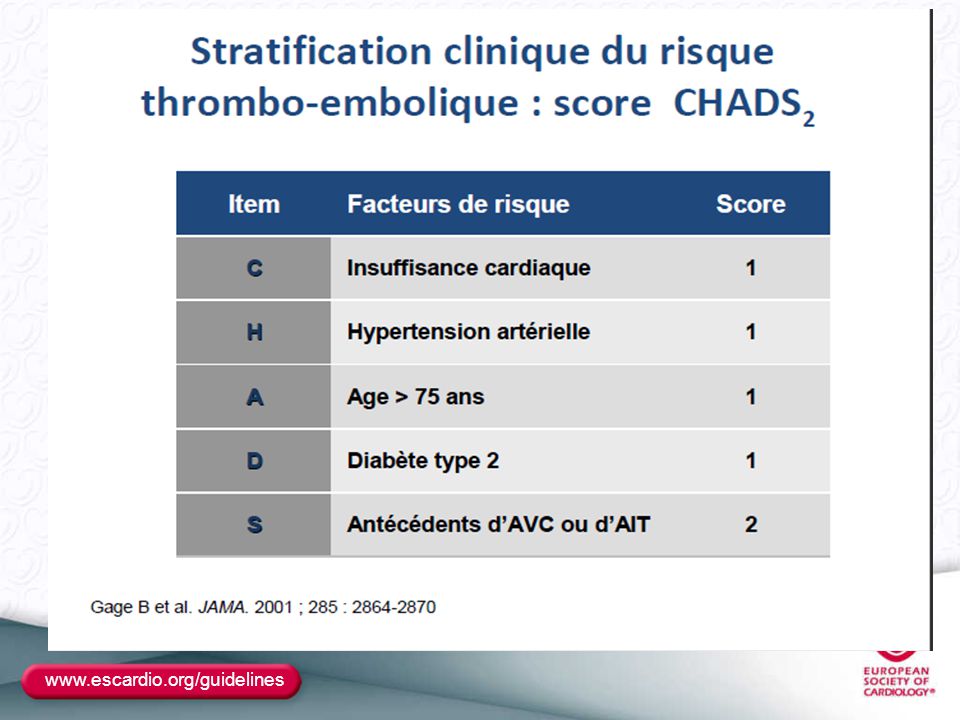
Chez les PT symptomatiques après échec des TT anti-arythmiques FA paroxystiques ou persistante ou prolongée Si IC et FC mal contrôlée malgré le Tt Le traitement anticoagulant doit être poursuivi pendant au moins 3 mois ou plus en fonction du score CHAD2

78
Fibrillation Auriculaire et SCA
Régularisation en urgence si Instabilité hémodynamique Souffrance ischémique persistante malgré le Tt bradycardisant BB ou Amiodarone IV

79
AF in Coronary stenting

80
AF in Coronary stenting

90
New and Emerging Anticoagulants
Anti – Xa : direct Rivaroxaban (oral) Apixaban (oral) Betrixiban (oral) Edoxaban (oral) Otamixaban (parenteral) LY – (oral) DU – 176B (oral) DX – 9065a (parenteral) PRT (oral) Anti – Xa : indirect Idraparinux biotinylated (parenteral) Anti – IIa Dabigatran (oral) Odiparcil (oral) Flovagatran (parenteral) Pegmusirudin (parenteral) Peg Hirudin Desiruidin 90
 Apixaban (oral) Betrixiban (oral) Edoxaban (oral) Otamixaban (parenteral) LY – (oral) DU – 176B (oral) DX – 9065a (parenteral) PRT (oral) Anti – Xa : indirect. Idraparinux biotinylated (parenteral) Anti – IIa. Dabigatran (oral) Odiparcil (oral) Flovagatran (parenteral) Pegmusirudin (parenteral) Peg Hirudin. Desiruidin. 90.")
91
Site of Action for New Anti-thrombotic Agents
Extrinsic XII Intrinsic XI Tissue Factor IX VII VIII AT Indirect Xa Inhibitors “-parinux” X Direct Xa Inhibitors “-xaban” V Factor Xa Inhibitors: block thrombin generation - Direct - Indirect: requires the binding of antithrombin Factor IIa Inhibitors: block the activity of thrombin = the enzyme that catalyzes the conversion of fibrinogen to fibrin - Whether you are inhibiting Factor Xa or Factor IIa = the net effect is a reduction in thrombin activity and fibrin formation, events that result in inhibition of coagulation. Direct Thrombin Inhibitors “-gatran” warfarin II Fibrinogen Fibrin Clot 91

92
Direct Factor Xa Inhibitors
XII Intrinsic Extrinsic XI TF IX VII VIII Direct Xa Inhibitors “-xaban” X V MOA: Direct, selective, and reversible inhibitor of factor Xa. It inhibits factor Xa bound within the prothrombinase complex as well as the free enzyme. It inhibits free and fibrin-bound factor Xa activity and prothrombinase activity - Does not directly inhibit thrombin, but inhibits thrombin generation via direct inhibition of factor Xa activity II Fibrinogen Fibrin Clot 92

93
Rivaroxaban Brand name Xarelto®, Bayer Oral tablet
High oral bioavailability (>80%) Onset of action 2-4 hours Half-life 9-12 hours No observed effects on agonist-induced platelet aggregation Primarily renal elimination No laboratory monitoring required No dosage adjustment for gender, age, extreme body weight Approved by Europe and Canadian agencies, and under FDA review currently Potent selective inhibitor of factor Xa. Absorption: well absorbed from GI tract with Bioavail > 80% The terminal t1/2 is ~ 5-9 hrs in young individual and hrs in the elderly Dual mechanism of excretion. 66% in the kidneys and the remainder in the feces 30-40% excreted unchanged in the urine and excreted via a combination of glomerular filtration and tubular secretion and the remainder reflects metabolites. Use in caution for pts with renal insufficiency. Intestinal excretion of rivaroxaban appears to be mediated, by P-glyp (transport protein) The drug is contraindicated in pts with severe liver dx b/c of metabolic inactivation may be impaired. Also caution should be used in patients receiving tratment with potent inhibitors of both CYP3A$ and P-glyp (ketoconazole/ritonovir) Reduced fecal and renal clearance of rivaroxaban by these drugs can cause exaggerated anticoagulant effect Rivaroxaban prolongs the PT and aPTT, with the PT being more sensitive than the aPTT depending on the reagents used for testing. The effect of the drug on these tests is short-lived with prolongation only seen at peak drug levels. Factor Xa inhibition is the best test to monitor drug concentrations in plasma. 93
 Onset of action 2-4 hours. Half-life 9-12 hours. No observed effects on agonist-induced platelet aggregation. Primarily renal elimination. No laboratory monitoring required. No dosage adjustment for gender, age, extreme body weight. Approved by Europe and Canadian agencies, and under FDA review currently. Potent selective inhibitor of factor Xa. Absorption: well absorbed from GI tract with Bioavail > 80% The terminal t1/2 is ~ 5-9 hrs in young individual and hrs in the elderly. Dual mechanism of excretion. 66% in the kidneys and the remainder in the feces % excreted unchanged in the urine and excreted via a combination of glomerular filtration and tubular secretion and the remainder reflects metabolites. Use in caution for pts with renal insufficiency. Intestinal excretion of rivaroxaban appears to be mediated, by P-glyp (transport protein) The drug is contraindicated in pts with severe liver dx b/c of metabolic inactivation may be impaired. Also caution should be used in patients receiving tratment with potent inhibitors of both CYP3A$ and P-glyp (ketoconazole/ritonovir) Reduced fecal and renal clearance of rivaroxaban by these drugs can cause exaggerated anticoagulant effect. Rivaroxaban prolongs the PT and aPTT, with the PT being more sensitive than the aPTT depending on the reagents used for testing. The effect of the drug on these tests is short-lived with prolongation only seen at peak drug levels. Factor Xa inhibition is the best test to monitor drug concentrations in plasma. 93.")
94
Indirect Factor Xa Inhibitors
XII Intrinsic Extrinsic XI TF IX VII VIII AT Indirect Xa Inhibitors “-parinux” X V Idraparinux: it has to bind to anti-thrombin before activating factor Xa (indirect Factor Xa Inhibitor) II Fibrinogen Fibrin Clot 94
 II. Fibrinogen. Fibrin Clot. 94.")
95
Idraparinux Once weekly SC injection 100% SC bioavailability
Half-life ~ hours Renal elimination No monitoring required Manufactured by Sanofi-Aventis Plan to file for U.S. approval in 2009

96
Direct Thrombin Inhibitors
XII Intrinsic Extrinsic XI TF IX VII VIII X V Direct Thrombin Inhibitors “-gatran” Synthetic DTIs are a new therapeutic class of antithrombotic agents that interact directly with thrombin and block its interaction with its substrates. Univalent DTIs such as argatroban, melagatran, and dabigatran etexilate, bind exclusively to the active site of thrombin and inactivate fibrin-bound thrombin. Reversible DTIs, such as argatroban, bivalirudin, melagatran, and dabigatran, dissociate relatively quickly from thrombin, thereby leavinga small amount of free, enxymatically active thrombin available for control of haemostasis. Reversible binding may contribute towards safer and more predictable anticoagulant treatment compared with irreversible, non-covalent binding, like that reported with the first DTI, hirudin. Ximelagatran (Exanta – AstraZeneca) the prodrug of melagtran, was the first orally available small-molecule reversible DTI to undergo clinical evaluation. II Fibrinogen Fibrin Clot 96
 the prodrug of melagtran, was the first orally available small-molecule reversible DTI to undergo clinical evaluation. II. Fibrinogen. Fibrin Clot. 96.")
97
Dabigatran No dietary/food interactions Oral capsule
Brand name Rendix™ or Pradaxa®, Boehringer- Ingelheim Approved in Europe March 2008; plans are to obtain U.S. FDA approval by 2010 Oral capsule Rapid onset of action Half-life hours Renal elimination No routine monitoring required P-gp substrate—use with caution when administered concomitantly with P-gp inhibitors Absorption: very low bioavailability (3.5-5%) Has very low probability with drug-drug interactions. The administration of PPI tends to decrease the area under the curve due to a decrease in absorption. (Needs an acidic environment for absorbtion) Approved by both Europe and Canada: short=term thromboprophylaxis in pts undergoing orthopedic procedures
 Has very low probability with drug-drug interactions. The administration of PPI tends to decrease the area under the curve due to a decrease in absorption. (Needs an acidic environment for absorbtion) Approved by both Europe and Canada: short=term thromboprophylaxis in pts undergoing orthopedic procedures.")
Présentations similaires













>")

>")










 1-IEC 2-B Bloquant 3-ARA 2 4-Anti-aldostérone.>")

>")