Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
VNI - Insuffisance Respiratoire Aiguë
G. HILBERT Département de Réanimation médicale, CHU Bordeaux EA 518, Université Bordeaux 2 CMU Insuffisance Respiratoire Aiguë / 04 / 08

2
Ventilation Non Invasive !!
EXACERBATIONS AIGUES de BPCO = Motif fréquent d’admission à l ’Hôpital DÉCOMPENSATIONS AIGUES de BPCO [ pH < 7.35 ] = RÉANIMATION – SOINS INTENSIFS RESPIRATOIRES < IRA : Standard = INTUBATION-Ventilation Mécan. EFFETS SECONDAIRES ++ Ventilation Non Invasive !!

3
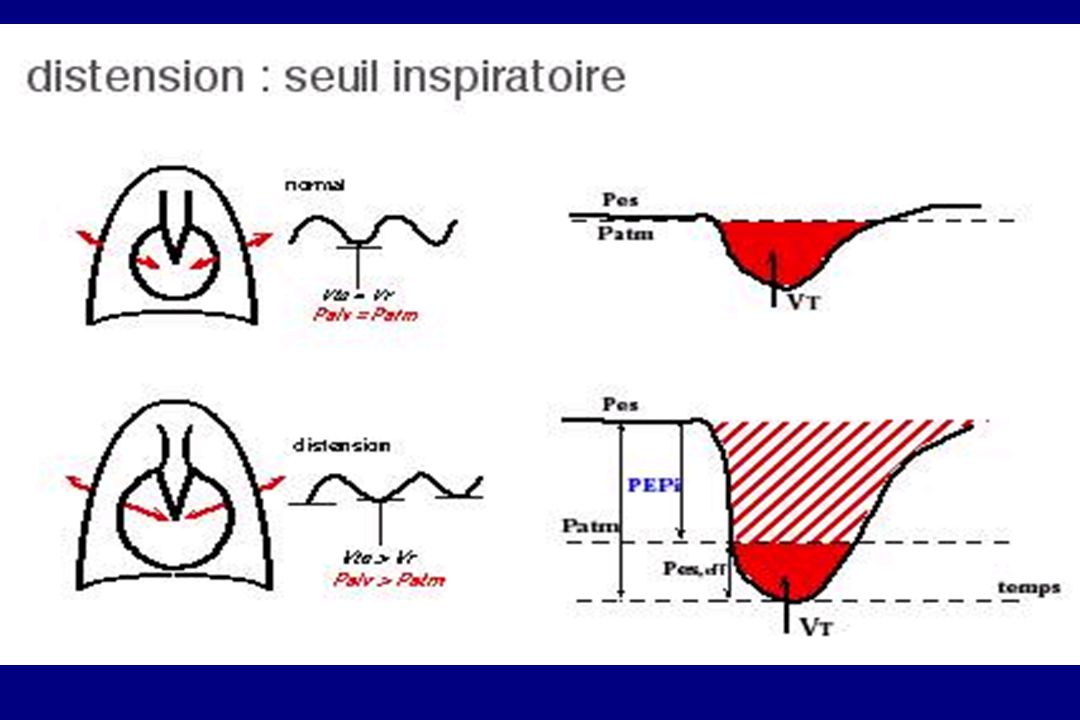
V télé-Exp. = V0 x e- texp/T
SYNCHRONISATION PATIENT-VENTILATEUR !! L’un des principaux obstacles ( ++ PATIENTS BPCO) : PEP INTRINSÈQUE Palv = 0 V télé-Exp. = CRF Pao = 0 Situation normale Palv > 0 V télé-Exp. > CRF Hyper-inflation dyn. PEPi Pao = 0 V télé-Exp. = V0 x e- texp/T V0 : volume en début d’expiration T : Compliancepulm X Résistancepulm
 : PEP INTRINSÈQUE. Palv = 0. V télé-Exp. = CRF. Pao = 0. Situation normale. Palv > 0. V télé-Exp. > CRF. Hyper-inflation dyn. PEPi. Pao = 0. V télé-Exp. = V0 x e- texp/T. V0 : volume en début d’expiration. T : Compliancepulm X Résistancepulm.")
5
CPAP / PEP ACIDOSE VPPI

6
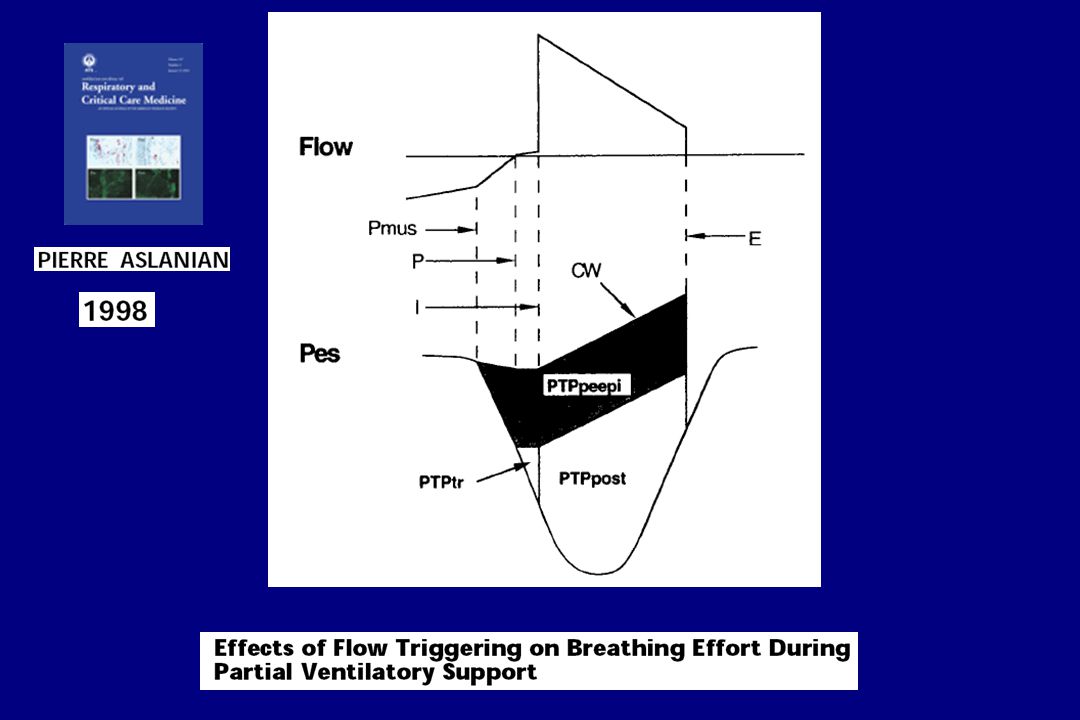
Mechanical Chemical Reflex Behavioral Respiratory Centers VT RR Pmusc INSPIRATORY EFFORT Neural Time Pao (PRESSURE APPLIED VENTILATOR AT THE AIRWAY OPENING) RESPONSE Pmus(t) = Pel,rs(t) + Pres (t) = [( V(t) x Ers ) + ( V’(t) x Rtot )] - Pao
 RESPONSE. Pmus(t) = Pel,rs(t) + Pres (t) = [( V(t) x Ers ) + ( V’(t) x Rtot )] - Pao.")
7
Dans l’IRA des BPCO, la VNI permet elle d’ ATTEINDRE ces OBJECTIFS ?

8
FACTORS THAT CAN IMPROVE ADAPTATION AND OUTCOME
VENTILATORY MODE ? + PEEP PRESSURE SUPPORT

9
FR AI PO.1 VO2 Musc. Resp. W Respiratoire «Stress» Musc. Resp.
VNI : Mode VS-AI-PEP VT FR AI PO.1 VO2 Musc. Resp. W Respiratoire «Stress» Musc. Resp.

10
Efforts respiratoires inutiles Asynchronie patient/ ventilateur
Poes Situation normale PEPi Poes extPEEP PEEPi WOB Eff.Poes time VT end-Exp.V = V0 x e - texp/T Efforts respiratoires inutiles Asynchronie patient/ ventilateur

12
Importance de l’hypoxémie : PaO2/FiO2
IRA hypoxémique Importance de l’hypoxémie : PaO2/FiO2

13
Modifications du rapport VA / Q dans une unité pulmonaire
SHUNT Modifications du rapport VA / Q dans une unité pulmonaire

14
SHUNT : IMPACTS THERAPEUTIQUES
Diminuer le % d’alvéoles non ventilées SaO2 (%) 100 Augmenter la SvO2 80 60 40 20 PaO2 (mmHg) 100 200 300 400 Redistribuer le débit sanguin pulmonaire
 100. Augmenter. la SvO PaO2 (mmHg) Redistribuer le débit sanguin pulmonaire.")
15
LA PEP Shunt HYPOXÉMIE
RECRUTEMENT ALVÉOLAIRE Stabilisation des petites voies aériennes comprimées ATÉLECTASIES Distribution H2O pulmonaire extra-vasculaire Shunt Amélioration VA/Q HYPOXÉMIE

16
VS-PPC = CPAP Ventilation Spontanée en Pression Positive Continue
Continuous Positive Airway Pressure t P (cm H2O) 7.5 t P (cm H2O) 7.5 I
 7.5. t. P. (cm H2O) 7.5. I.")
17
VS-AI-PEP t P (cm H2O) 7.5 20 AI I PEP
 AI I PEP")
18
IRA HYPOXÉMIQUE : Objectif PaO2
Nombreuses études : VS-PPC : oxygénation, FR, dyspnée AI + PEP Antonelli et al. N Engl J Med 1998 EPRC : 64 patients avec indication de ventilation mécanique

19
D'OÙ VENONS-NOUS ? OÙ EN SOMMES-NOUS ? OÙ ALLONS-NOUS ?
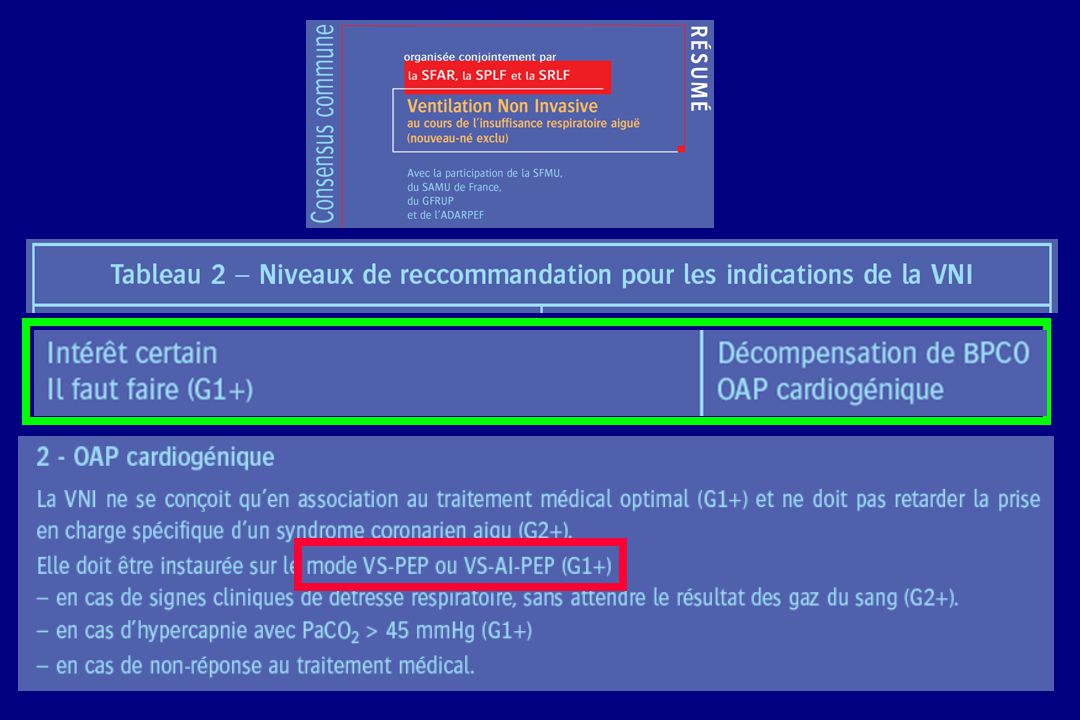
VNI : PRINCIPALES INDICATIONS dans l’IRA INSUFFISANCE RESPIRATOIRE HYPERCAPNIQUE : DÉCOMPENSATION A. de BPCO D'OÙ VENONS-NOUS ? OÙ EN SOMMES-NOUS ? OÙ ALLONS-NOUS ? INSUFFISANCE RESPIRATOIRE HYPOXÉMIQUE : OAP CARDIOGENIQUE IMMUNODÉPRIMÉS IMMUNOCOMPÉTENTS VNI Post-EXTUBATION

20
France - enquête VNI 2002 indications de la VNI * *
Demoule et Coll. Intensive Care Med 2006

21
VNI : POSSIBLE À DIFFERENTS STADES D’IRA
7.35 < pH < 7.38 200 < PaO2/FiO2 < 300 S Y T É M A I Q U E pH < 7.35 PaO2/FiO2 < 200 PaO2/FiO2 < 80 TRAITER IRA Alternative Intubation ? TRAITER IRA Post-Extub ? Prévenir IRA Post-Extub. ? Prévenir IRA ? Sevrage ?

22
Décompensation A. de BPCO : VNI vs Traitement Standard
* Etudes Randomisées contrôlées

23
Bott J, et al. Randomized controlled trial of nasal ventilation in
acute ventilatory failure due to chronic obstructive airways disease. Lancet 1993;341: 60 patients BPCO VNI : masque nasal, VAC Comparée au Traitement standard, la VNI : Améliore significativement : les paramètres physiologiques initiaux le score de dyspnée Réduit la mortalité Mais : Contexte du Royaume‑Uni Dans le groupe contrôle un certain nombre de patients s'aggravant ne sont pas pris en charge par intubation et ventilation artificielle.

24
la durée de séjour hospitalier
Brochard L, et al. Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease. 1995;333: 85 patients BPCO VNI : masque facial, AI Comparée au Traitement standard, la VNI permet de Réduire : la nécessité d’ intubation de 74 à 26 % la durée de séjour hospitalier les complications observées en réanimation de 48 à 16 % la mortalité de 29 à 9 %

25
236 patients BPCO : acidose respiratoire modérée à sévère (7,25‑7,35)
Plant PK, et al. Early use of NIV for acute exacerbations of COPD on general respiratory wards: a multicentre randomised controlled trial. Lancet 2000;355: 236 patients BPCO : acidose respiratoire modérée à sévère (7,25‑7,35) Comparée au Traitement standard, la VNI permet de Réduire : la nécessité d’ intubation de 27 à 15 % la mortalité de 20 à 10 % VNI administrée par les IDE dans 13/14 centres IDE/ Patients= 1/11 22/25 services : aucune expérience de la VNI FORMATION : 3 mois = 7.6 h. en moyenne Puis = 0.9 h. / mois, en moyenne Charge de W premières H. : de 26 min / traitement standard > 8 premières H. : aucune différence
 Comparée au Traitement standard, la VNI permet de Réduire : la nécessité d’ intubation de 27 à 15 % la mortalité de 20 à 10 % VNI administrée par les IDE dans 13/14 centres IDE/ Patients= 1/11. 22/25 services : aucune expérience de la VNI. FORMATION : 3 mois = 7.6 h. en moyenne. Puis = 0.9 h. / mois, en moyenne. Charge de W 8 premières H. : de 26 min / traitement standard. > 8 premières H. : aucune différence.")
26
Noninvasive Positive Pressure Ventilation
International CONSENSUS Conferences in Intensive Care Medicine : Noninvasive Positive Pressure Ventilation in Acute Respiratory Failure A J R C C M 2001; 163: I C M 2001; 27: « Patients hospitalized for EXACERBATIONS of COPD with rapid clinical deterioration should be considered for NPPV to prevent further deterioration in gas exchange, respir. workload, and the need for endotracheal intubation » « Larger, controlled studies are required to determine the potential benefit of adding NPPV to standard medical treatment in the avoidance of endotracheal intubation in HYPOXEMIC Acute Respiratory Failure »

27
Intérêt des « NOUVEAUX MODES » ventilatoires en Réanimation ?
VACI VPAC Automode VC VAC SIMV VAPS VA VS PA VCRP Autoflow APV VS-AI-Vt mini VAC+ VACI+ VPC VPS SPAP MMV AVAPS VAIV VIV APRV VS-PPV BIPAP BILEVEL VPL ATC TC ASV PAV PPS PC PAC PACI AI CPAP IPAP EPAP PSV ASB PRVC APL

28
? VNI – BPCO : PERSPECTIVES HÉLIUM ÉTUDES PHYSIO-PATH
ÉTUDES/IMPACT CLINIQUES Modes ventilatoires / PAV HÉLIUM ?

29
PAV (n=21) vs. PSV (n=23)
 vs. PSV (n=23)")
31
prospective, randomised, multicenter study
123 acutely decompensated COPD patients requiring NIV Patients were randomised to receive every NIV treatment from study inclusion with either Air/O2 or He/O2 He/O2 contained in a He/O2 78:22 cylinder connected to the air inlet of either a Hamilton Veolar or a Siemens 300 Servo ventilator.

33
123 patients

34
Impaired secretion clearance occasionally causes NIV to fail.
INTRAPULMONARY PERCUSSIVE VENTILATION ? CPAP / PEEP NIV ACIDOSIS

35
17 % 75 % 8 %

36
pH : seuil de 7.28 7.25 7.25 0.07 7.20 0.08

37
Early use of NIV for acute exacerbations of COPD on general respiratory wards: a multicentre randomised controlled trial. 236 patients Plant et al Lancet 2000; 355:1931-5

38
2005

40
Parfois, dans la “VRAIE VIE” :

45
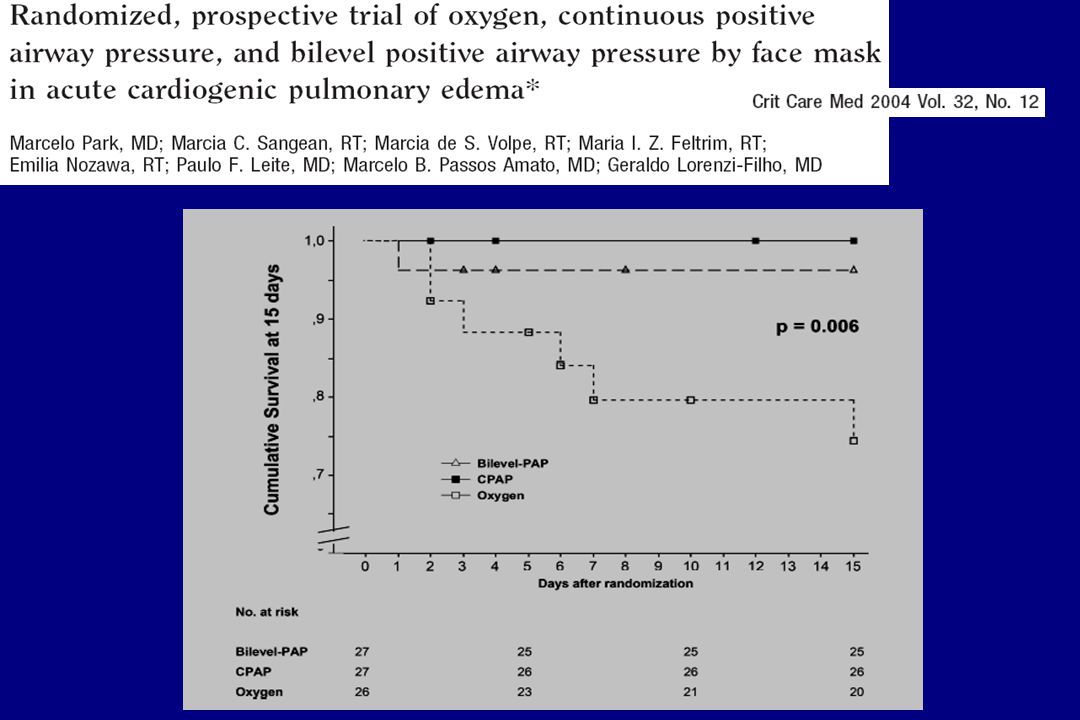
Masip, Lancet Patients PS-PEEP Standard p % Intubation

47
Ventilation Invasive MORTALITÉ
VNI chez l’IMMUNODÉPRIMÉ D'OÙ VENONS-NOUS ? IMMUNODÉPRESSION : Ventilation Invasive MORTALITÉ Classiquement SIDA : > 60 % Cancer SOLIDE : > 70 % Cancer HÉMATOLOGIQUE : > % Amélioration du pronostic des patients avec cancer admis en réanimation Azoulay E. ‘The intensive care support of patients with malignancy: do everything that can be done.’ ICM 2006

48
Plus le % de patients sous VM est bas, plus le taux de survie est élevé
Survie Réa. % 45 39 61 Patients Avec VM % 19 45 37 MICU Surv 45 19

49
IRA, surtout chez l’Immunodéprimé
EVITER OBJECTIVF L’INTUBATION MAJEUR !

50
NIV / IMMUNOSUPPRESSED PATIENTS
STUDIES * = R.C.T n Particularities Mask Mode SUCCESS AIDS (Pneumocystis) Bedos CCM F CPAP % Confalonieri ICM intubation criteria F PS/PEEP % Antonelli * JAMA Solid Organ Transpl F PS/PEEP % (vs 30 %) HEMATOLOGICAL Tognet Clin I C N F PS/PEEP % Conti ICM intubation criteria N PS/PEEP % Depuydt Chest intubation criteria F CPAP PS/PEEP % Hilbert CCM Neutropenia F CPAP % Azoulay CCM CANCER F PS/PEEP % Azoulay Medicine CANCER (++ Hemato) F PS/PEEP % Hilbert * NEJM HEMATO-Neutropenia F PS/PEEP % DrugIsup. AIDS (vs 23%) Rocco Chest Hem. SolidOT. AIDS F/Helmet PS/PEEP %
 Bedos CCM F CPAP 66 % Confalonieri ICM intubation criteria F PS/PEEP 67 % Antonelli * JAMA Solid Organ Transpl. F PS/PEEP 80 % (vs 30 %) HEMATOLOGICAL. Tognet Clin I C N F PS/PEEP 33 % Conti ICM intubation criteria N PS/PEEP 69 % Depuydt Chest intubation criteria F CPAP PS/PEEP 31 % Hilbert CCM Neutropenia F CPAP 25 % Azoulay CCM CANCER F PS/PEEP 44 % Azoulay Medicine CANCER (++ Hemato) F PS/PEEP 43 % Hilbert * NEJM HEMATO-Neutropenia F PS/PEEP 54 % DrugIsup. AIDS (vs 23%) Rocco Chest Hem. SolidOT. AIDS F/Helmet PS/PEEP 58 %")
51
n = 26, > 5 ans PaO2 / FiO2 72 « NTBR » 42% Intubation 69 %
Groupe VNI n = 26, > 5 ans PaO2 / FiO Vasopresseurs % « NTBR » % Intubation % Décès Hôpital %

52
ÉCHEC INTUBATION = 92 % DÉCÈS
NONINVASIVE CONTINUOUS POSITIVE AIRWAY PRESSURE in NEUTROPENIC PATIENTS with ACUTE RESPIRATORY FAILURE REQUIRING ICU ADMISSION HILBERT G, GRUSON D, VARGAS F, et al. 2000 N = PaO2 / FiO2 = 128 SAPS II = 56 16 Masque FACIAL CPAP SUCCÈS = 25 % ÉCHEC INTUBATION = 92 % DÉCÈS

53
PaO2 / FiO2 141 24 136 23 VNI Traitement Standard
NONINVASIVE VENTILATION in IMMUNOSUPPRESSED PATIENTS with PULMONARY INFILTRATES, FEVER, and ACUTE RESPIRATORY FAILURE HILBERT G, GRUSON D, VARGAS F, et al * NEUTROPÉNIE HÉMOPATHIE MALIGNE * IMMUNOSUPPRESEURS * SIDA VNI Traitement Standard ( n = 26 ) ( n = 26 ) PaO2 / FiO 23
 ( n = 26 ) PaO2 / FiO2 141 23.")
54
V.A.P. / Sinusitis -no. (%) 3 (12) 9 (35) 0.05
NIV Standard treatment p Intubation - no./total no.(%) /26 (46) /26 (77) Hematological malignancy 8/15 (53) /15 (93) Drug-Immunosuppression /9 (33) /9 (56) AIDS /2 (50) /2 (50) Complications- no. (%) (50) (81) Complications ICU death (38) (69) V.A.P. / Sinusitis -no. (%) (12) (35) ICU Deaths - no./total no.(%) /26 (38) /26 (69) Hematological malignancy 7/15 (47) /15 (87) Hospital Deaths -no./tot.no. (%) 13/26 (50) /26 (81) Hematological malignancy 8/15 (53) /15 (93)
 12/26 (46) 20/26 (77) Hematological malignancy 8/15 (53) 14/15 (93) Drug-Immunosuppression 3/9 (33) 5/9 (56) AIDS 1/2 (50) 1/2 (50) Complications- no. (%) 13 (50) 21 (81) Complications ICU death 10 (38) 18 (69) V.A.P. / Sinusitis -no. (%) 3 (12) 9 (35) ICU Deaths - no./total no.(%) 10/26 (38) 18/26 (69) Hematological malignancy 7/15 (47) 13/15 (87) Hospital Deaths -no./tot.no. (%) 13/26 (50) 21/26 (81) Hematological malignancy 8/15 (53) 14/15 (93)")
55
Groupe VNI no. (%) Diagnostic + Diagnostic - p (n = 17) (n = 9)
Hilbert G, et al Groupe VNI no. (%) Diagnostic + Diagnostic p (n = 17) (n = 9) Intubation (29) (78) Décès 4 (24) (67) - Réa Décès 5 (29) (89) - Hôpital Un diagnostic positif de pneumopathie pourrait être l’un des déterminants du succès de la méthode.
 Diagnostic + Diagnostic - p (n = 17) (n = 9) Intubation 5 (29) 7 (78) Décès 4 (24) 6 (67) Réa. Décès 5 (29) 8 (89) Hôpital. Un diagnostic positif de pneumopathie pourrait être. l’un des déterminants du succès de la méthode.")
56
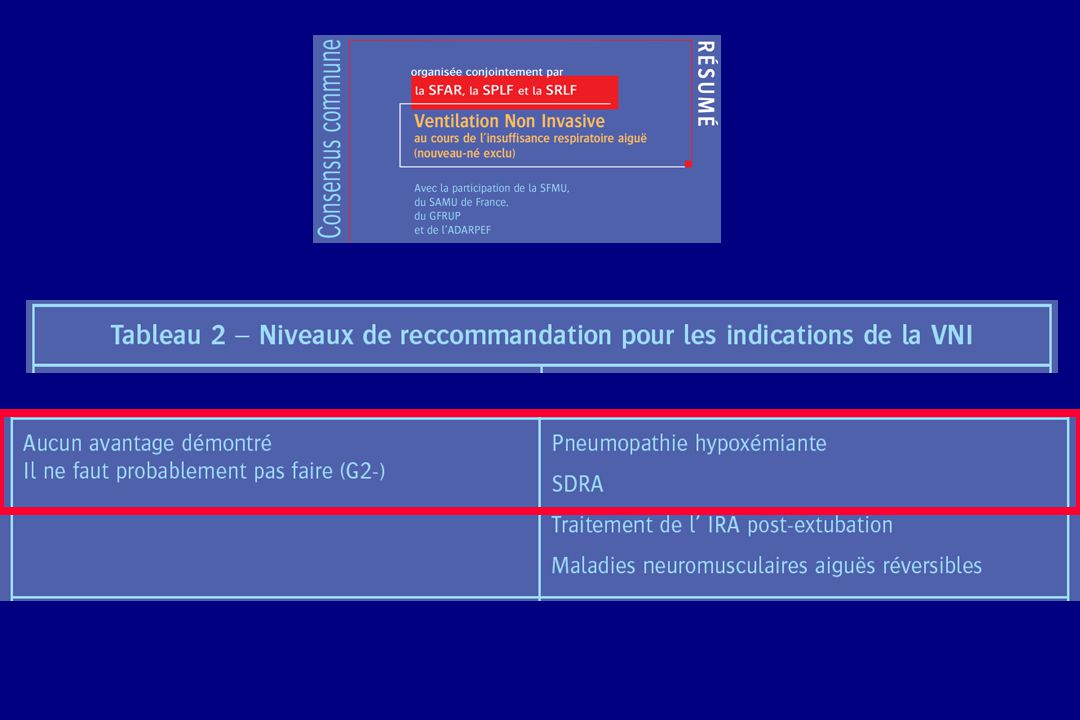
VNI / IRA Hypoxémique - PNEUMOPATHIES - Patients IMMUNOCOMPÉTENTS
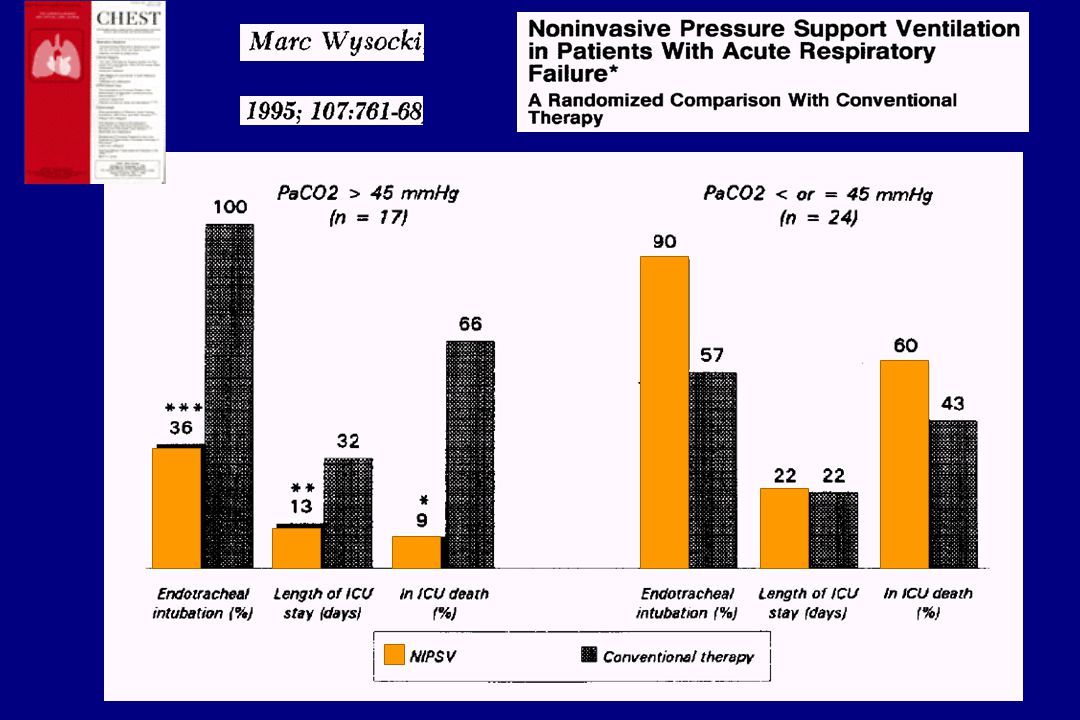
ETUDES [ * = R. C. ] n Particularités Masque Mode SUCCÈS Benhamou Chest F AI/PEP % Wysocki Chest 1995 * / ± Hypercapnie F AI/PEP ?/38 % (vs 30 %) Meduri Chest F AI/PEP % Pollack Ann Em M N/F AI/PEP % Alsous ICM PaO2/FiO2 = F AI/PEP % Antonelli NEJM 1998 * 5/ critères intubation F AI/PEP 80/69 % Confalonieri AJRCCM * Pneumop. Com. ± BPCO F AI/PEP % (vs 50 %) Delclaux JAMA 2000 * / ALI F VS-PPC ?/63 %(vs 56 %) Jolliet ICM Pneumop. Com. F AI/PEP % Antonelli ICM Pp. Com + noso + inh F AI/PEP % Domenighetti ICM Pneumop. Com. F AI/PEP % Smailes Burns Brûlés F AI/PEP % Ferrer AJRCCM * F AI/PEP % (vs 27 %) Cheung Chest SARS (Coronarovirus) F AI/PEP %
 Meduri Chest F AI/PEP 71 % Pollack Ann Em M N/F AI/PEP 80 % Alsous ICM PaO2/FiO2 = 89 F AI/PEP 50 % Antonelli NEJM 1998 * 5/32 critères intubation F AI/PEP 80/69 % Confalonieri AJRCCM 1999 * 28 Pneumop. Com. ± BPCO F AI/PEP 79 % (vs 50 %) Delclaux JAMA 2000 * 26/40 ALI F VS-PPC /63 %(vs 56 %) Jolliet ICM Pneumop. Com. F AI/PEP 34 % Antonelli ICM Pp. Com + noso + inh F AI/PEP 58 % Domenighetti ICM Pneumop. Com. F AI/PEP 62 % Smailes Burns Brûlés F AI/PEP 74 % Ferrer AJRCCM 2003 * 19 F AI/PEP 74 % (vs 27 %) Cheung Chest SARS (Coronarovirus) F AI/PEP 70 %")
58
A comparison of Noninvasive Positive Pressure Ventilation and conventional M V in patients with acute respiratory failure. Antonelli M., et al

59
Treatment of Acute Hypoxemic Nonhypercapnic Respiratory Insufficiency With Continuous Positive Airway Pressure Delivered by a Face Mask Delclaux C. et al. 2000;284: Oxygène + CPAP N = 62 Oxygène seul N = 61 p Âge 60 (18-88) 56 (19-85) NS Infection 42 (68 %) 37 (61% ) Pathologie Cardiaque 23 (37%) 28 (46 %) SUCCÈS 41 (66 %) 37 (61 %) Durée hospit. 15 j 16 j DÉCÈS 19 (30 %) 18 (29,5 %)
 56 (19-85) NS. Infection. 42 (68 %) 37 (61% ) Pathologie. Cardiaque. 23 (37%) 28 (46 %) SUCCÈS. 41 (66 %) 37 (61 %) Durée hospit. 15 j. 16 j. DÉCÈS. 19 (30 %) 18 (29,5 %)")
60
14/19 (74 %) 4/15 (27 %) 3/19 8/15 Pneumonia 0.017 0.030 NIV N = 51
Control N = 54 p SUCCESS :all 38 (75 %) 26 (48 %) 0.010 Pneumonia 14/19 (74 %) 4/15 (27 %) 0.017 ICU-Death :all 9 (18 %) 21 (39 %) 0.028 3/19 8/15 0.030
 26 (48 %) Pneumonia. 14/19 (74 %) 4/15 (27 %) ICU-Death :all. 9 (18 %) 21 (39 %) /19. 8/")
62
Durée Ventilation 6 +/- 4 11 +/- 8 < 0.01
BPCO VNI Contrôle p (n = 30) (n = 30) Durée Ventilation / / < 0.01 Sevrage (j) Séjour Réa. (j) / / < 0.01 Réintubation (%) < 0.01 Décès (%) Hilbert G. Eur Respir J 1998
 (n = 30) Durée Ventilation 6 +/ /- 8 < Sevrage (j) Séjour Réa. (j) 8 +/ /- 8 < Réintubation (%) < Décès (%) Hilbert G. Eur Respir J")
63
2006 Patients at risk (but successfully extubated): Age > 65 yrs
98 % COPD Patients at risk (but successfully extubated): Age > 65 yrs Cardiac failure as cause of ETI APACHE II > 12 at extubation day
: Age > 65 yrs. Cardiac failure as cause of ETI. APACHE II > 12 at extubation day.")
64
Au total : pas de différence
Noninvasive positive pressure ventilation (NPPV) for post-extubation respiratory distress: a randomized controlled trial. Keenan S, Powers C, McCormack D, Block G. Réintubation ns Mortalité ns Au total : pas de différence
 for post-extubation. respiratory distress: a randomized controlled trial. Keenan S, Powers C, McCormack D, Block G. Réintubation. ns. Mortalité. ns. Au total : pas de différence.")
65
Extubation – Resp.Fail. (hr)
ns * INTUBATION (%) ICU Mortality (%) Extubation – Resp.Fail. (hr) NIV
 ICU Mortality (%) Extubation – Resp.Fail. (hr) NIV.")
66
ESSAI VNI 1-2 heures

67
354 patients with hypoxemic ARF
86 of them with ARDS

68
COPD : NIV’ failure Ambrosino N. Thorax 1995 1-2 h 7.34 7.25
pH at: SUCCESS FAILURE Ambrosino N. Thorax h Hilbert G. ICM min Plant PK. Thorax h OR 1.23 per nmol/l, 95 % CI 1.05 à 1.43 Hilbert G. CCM min Carlucci A. ICM h

69
VNI dans l’IRA Expérience de l’équipe
“Bonne” Indication Pas de Contre-Indication QUELS PARAMÈTRES PEUVENT ÊTRE OPTIMISÉS ? Dépend de : type d’IRA stade d’IRA co-morbidités Expérience de l’équipe …

70
FACTORS THAT CAN IMPROVE ADAPTATION AND OUTCOME ?
Ventilator Pressure Support PEEP I. Trigger Expiratory Trigger LEAKS Monitoring Alarm limits Pt/Ventil. Synchrony Humidification Interface Modest sedation ? Reassurance Education Training Protocol

71
BPCO : MODE VS-AI-PEP / BiPAP
I REGLAGES INITIAUX : AI : 8 cm H2O progressive / Vte = 7-9 ml/kg - FR < 25 PEP = cm H2O FIO2 88 % < SaO2 < 92 % II Gaz du Sang à 30 min de VNI : III 2° Séance de 45 min de VNI - Gaz du Sang EFFICACITE ? - OPTIMISATION G. HILBERT, et al.

72
BPCO : MODE VS-AI-PEP / BiPAP
ANALYSE DE L’HEMATOSE Baisse PaCO2 ≥ 10 % AI Baisse PaCO2 < 10 % AI à 8 PEP PaCO2 Idem ou G. HILBERT, et al.

73
MODE SEQUENTIEL : PERIODES DE VENTILATION 30 min :
Hilbert G. et al. BPCO IRA IR post-extubation AI (cm H2O) / /- 4 PEP (cm H2O) / /- 1 O2 - FIO /- 2 l/min /- 5 % MODE SEQUENTIEL : PERIODES DE VENTILATION 30 min : Décompensation aiguë = toutes les 3 h Monitorage Continu : SaO2 , FR , FC, PA Reprise systématique de VNI si : SaO2< 85 % ; Dyspnée et FR > /min
 16 +/ /- 4. PEP (cm H2O) 6 +/ /- 1. O2 - FIO2 3 +/- 2 l/min 28 +/- 5 % MODE SEQUENTIEL : PERIODES DE VENTILATION 30 min : Décompensation aiguë = toutes les 3 h. Monitorage Continu : SaO2 , FR , FC, PA. Reprise systématique de VNI si : SaO2< 85 % ; Dyspnée et FR > /min.")
74
Échecs de Déclenchement Inspiratoire
3 -2 Flow L/sec 20 cm H2O Paw 5 -10 cm H2O Pes * 10 20 30 Leung et al, AJRCCM 1997

75
Déterminants des Échecs de Déclenchement Inspiratoire
Tidal Volume Expiratory Time PEEPI,dyn, cm H2O 4.5 4.0 3.5 3.0 0.5 0.0 510 480 450 100 1.6 1.4 1.2 1.0 Breaths Preceding Non-Triggering p < 0.02 p < 0.001 p < 0.001 Breaths Preceding Triggering Efforts Leung et al, AJRCCM 1997

76
V0 : volume en début d’expiration
V télé-Exp. = V0 x e- texp/T V0 : volume en début d’expiration

78
« Wasted » inspiratory effort
monitoring « Wasted » inspiratory effort

79
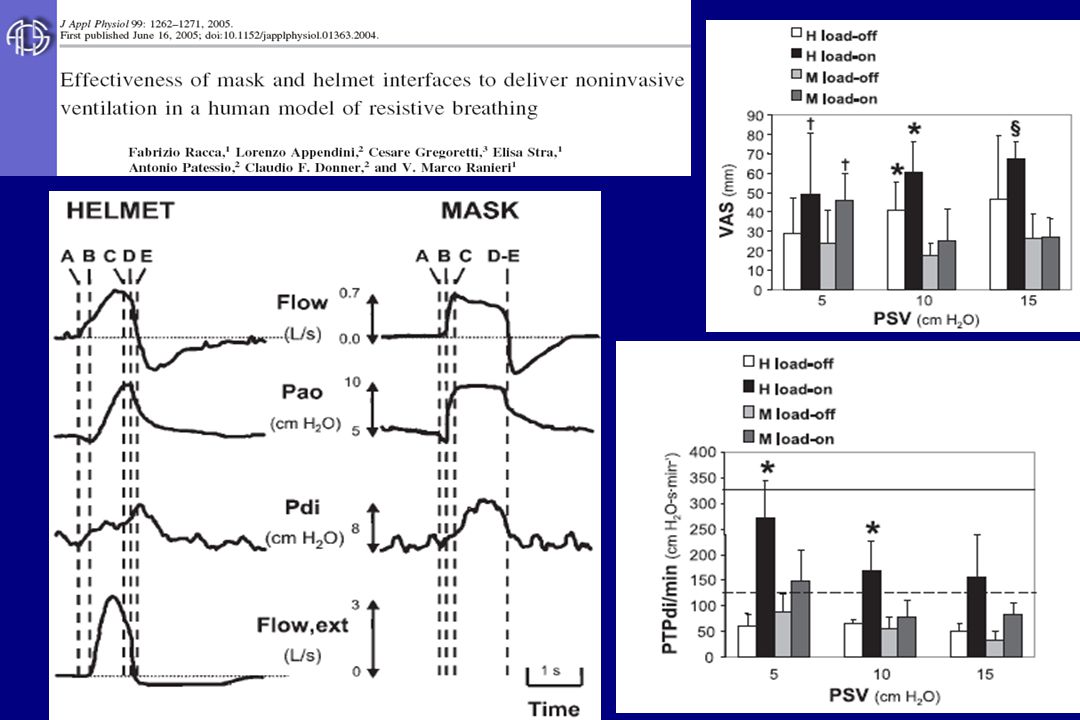
Ventilation au masque facial

80
EN DEHORS de la Réa. : en Service d’HÉMATOLOGIE
Noninvasive continuous positive airway pressure delivered by helmet in hematological malignancy patients with hypoxemic acute respiratory failure Principi T. et al TOLERANCE SCORE : 0 (bad) to 3 (very good) Helmet 17 patients Mask P INTUBATION 0 (0%) 7 (41%) <0.01 In Hospital DEATH 4 (23%) 8 (47%) <0.05 Tolerance, level 0 Tolerance, level 1 1 (6%) Tolerance, level 2 3 (18%) 2 (12%) 1.00 Tolerance, level 3 13 (76%) <0.0001 EN DEHORS de la Réa. : en Service d’HÉMATOLOGIE
 to 3 (very good) Helmet. 17 patients. Mask. P. INTUBATION. 0 (0%) 7 (41%) <0.01. In Hospital DEATH. 4 (23%) 8 (47%) <0.05. Tolerance, level 0. Tolerance, level 1. 1 (6%) Tolerance, level 2. 3 (18%) 2 (12%) Tolerance, level (76%) < EN DEHORS de la Réa. : en Service d’HÉMATOLOGIE.")
82
Modification of the threshold of decrease of insp. Flow!
LEAKS Patient-Ventilator Asynchrony time-cycling flow-cycling “traditional” Flow-Cycling Modification of the threshold of decrease of insp. Flow!

83
FACTORS THAT CAN IMPROVE ADAPTATION AND OUTCOME
HUMIDIFICATION ?

84
Essai VNI: 26 patients Sur > 5 années
Groupe VNI PaO2 / FiO Vasopresseurs 27% « NTBR » 42% Intubation 69% Décès Hôpital 65% Essai VNI: 26 patients Sur > 5 années

85
VNI : formation du personnel !!!

86
CONCLUSION (I) 1995 1998 2001
")
87
IRA Réanimation VNI !! Chaque fois que possible : Précoce STADE IRA ?
CONCLUSION (II) IRA Réanimation Chaque fois que possible : VNI !! INTUBATION VM EVALUATION : à 1-2 heures , régulière IRA non améliorée ? Précoce STADE IRA ? Tardif QUELS PARAMÈTRES PEUVENT ÊTRE OPTIMISÉS ? Expérience Formation … Protocole Interface Monitoring
 IRA Réanimation. Chaque fois que possible : VNI !! INTUBATION. VM. EVALUATION : à 1-2 heures , régulière. IRA non améliorée Précoce. STADE IRA Tardif. QUELS PARAMÈTRES PEUVENT ÊTRE OPTIMISÉS Expérience Formation … Protocole Interface Monitoring.")
Présentations similaires