Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
L’allègement thérapeutique est-il redevenu d’actualité ?
SFLS 2006 Dijon L’allègement thérapeutique est-il redevenu d’actualité ? Pr Gilles PIALOUX (APHP/Hôpital Tenon, Paris)
")
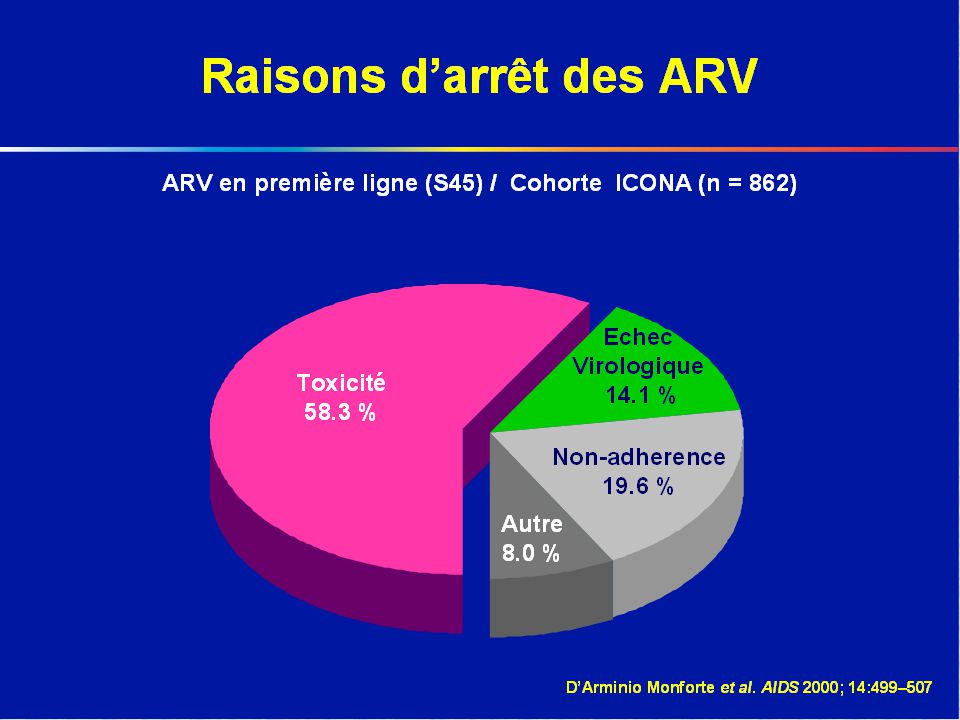
2
Les associations de lutte contre le sida
« Il faut adapter le traitement anti-VIH à la vie des personnes atteintes et non l’inverse ! » Les associations de lutte contre le sida

3
Simplification par l’allègement: mais pour quoi faire ?

4
Allèger, c’est … Moins de prises, moins de contraintes, moins de comprimés…. Moins d’effets secondaires et plus de qualité de vie Moins d’interactions médicamenteuses Mois de jours sous ARV (STI??) Moins de traitements lourds au long cours : induction-maintenance Moins de molécules utilisées ; épargne thérapeutique …
 Moins de traitements lourds au long cours : induction-maintenance. Moins de molécules utilisées ; épargne thérapeutique …")
5
Impact virologique du nombre de gelules
90 (r = –0.57, P = .0085) 80 70 60 Patients HIV RNA <50 cp/ml a S48 (%) 50 40 30 PI NRTI NNRTI This study assessed the correlation between antiretroviral pill burden and durability of virologic response, based on data from multiple clinical trials Analysis included only studies that were at least 24 weeks in duration and involved at least 30 chronically HIV-infected, adult patients who were ART-naive or who had very limited prior ART exposure Triple-combination therapy was defined as 2 NRTIs plus a PI, an NNRTI, or a third NRTI Regimens involving fewer pills per day were associated with superior virologic response. Results suggest that daily pill burden was the most significant predictor of antiretroviral response at 48 weeks 20 10 5 10 15 20 Nombre de gelules prescrites par jour Bartlett. AIDS 2001;15:1369.
 Patients HIV RNA <50 cp/ml a S48 (%) PI. NRTI. NNRTI. This study assessed the correlation between antiretroviral pill burden and durability of virologic response, based on data from multiple clinical trials. Analysis included only studies that were at least 24 weeks in duration and involved at least 30 chronically HIV-infected, adult patients who were ART-naive or who had very limited prior ART exposure. Triple-combination therapy was defined as 2 NRTIs plus a PI, an NNRTI, or a third NRTI. Regimens involving fewer pills per day were associated with superior virologic response. Results suggest that daily pill burden was the most significant predictor of antiretroviral response at 48 weeks Nombre de gelules prescrites par jour. Bartlett. AIDS 2001;15:1369.")
7
Lipoatrophie faciale

8
Bosse de bison

9
Photos: Service maladies infectieuses, Hôpital Tenon, Paris

10
Allègement galénique

11
Simplification au fil du temps * 1996 – 2006 (I)
1996: d4T/3TC/IDV 10 cp, TID 2002: AZT/3TC/EFV 3 cp, BID 1998: AZT/3TC/EFV 5 cp, BID 2004: TRUVADA /EFV 2 cp , QD 2006: ATRIPLA 1cp , QD * Liste non exhaustive

12
Simplification au fil du temps* 1996 – 2006 (II)
LPV/rtv Monothérapie/Meltrex: 4 comprimes/jour SQV: 500 mg/cp T 20: 1 injection/semaine ? Biojector® STI +/- vaccinothérapie : strategies ?… Sratégie Induction & Maintenance … *liste non exhaustive

13
Allègement d’emblée ?

14
LPV/r SGC 400/100 mg + AZT/3TC 300/150 mg) BID, n=53
MONARK Study Entry criteria Antiretroviral naïve HIV-1 RNA <100,000 c/mL CD4 > 100 cells/mm3 LPV/r SGC 400/100 mg BID, n=83 96 weeks Screening LPV/r SGC 400/100 mg + AZT/3TC 300/150 mg) BID, n=53 Primary efficacy endpoint Proportion of patients with HIV-1 RNA < 400 copies/mL at W24 AND <50 copies/mL at W48 Secondary endpoints Proportion of patients with HIV-1 RNA < 400 and < 50 copies/mL by week 48 Change in CD4 cell counts by week 48 Number of serious adverse events Sub-optimal virologic response defined as: failure to achieve a decline in VL of at least 1 log10 by W4 failure to achieve a VL < 400 copies/ml by W24 any viral rebound ≥ 1 log10, after VL < 400 copies/ml, confirmed in a second specimen Statistical methods Fisher’s exact test for comparing proportion Kruskal-Wallis for increase in CD4 cells count First patient September 2003 Wk 24 Wk 48 Primary efficacy analysis Proportion of subjects with HIV-1 RNA < 400 copies/mL at Week AND < 50 copies/mL at Week 48 Delfraissy JF. et al., XVI IAC, Toronto, 2006, #THLB0202
 BID, n=53. Primary efficacy endpoint. Proportion of patients with HIV-1 RNA < 400 copies/mL at W24 AND <50 copies/mL at W48. Secondary endpoints. Proportion of patients with HIV-1 RNA < 400 and < 50 copies/mL by week 48. Change in CD4 cell counts by week 48. Number of serious adverse events. Sub-optimal virologic response defined as: failure to achieve a decline in VL of at least 1 log10 by W4. failure to achieve a VL < 400 copies/ml by W24. any viral rebound ≥ 1 log10, after VL < 400 copies/ml, confirmed in a second specimen. Statistical methods. Fisher’s exact test for comparing proportion. Kruskal-Wallis for increase in CD4 cells count. First patient September Wk 24. Wk 48. Primary efficacy analysis. Proportion of subjects with HIV-1 RNA < 400 copies/mL at Week 24 AND < 50 copies/mL at Week 48. Delfraissy JF. et al., XVI IAC, Toronto, 2006, #THLB0202.")
15
Virologic Response HIV-1 RNA < 50 copies/mL (ITT, M=F)
20 40 60 80 100 4 8 12 16 24 28 32 36 44 48 Week AZT/3TC/LPVr, ITT, missing = failure LPVr, ITT, missing = failure 75% 71% % Patients < 50 c/mL (ITT, 95% CI) Sample Size LPV/r Arm Triple Arm 83 53 Delfraissy JF. et al., XVI IAC, Toronto, 2006, #THLB0202
 Sample Size. LPV/r Arm. Triple Arm Delfraissy JF. et al., XVI IAC, Toronto, 2006, #THLB0202.")
16
Change in CD4 Cell Count Delfraissy JF. et al., XVI IAC, Toronto, 2006, #THLB0202

17
Induction-Maintenance 1996-2006

18
Principes de l’allègement par induction-maintenance
S +F+L+S S Evaluation S 48 ou S 96 Randomisation à M ? si … Screening S+F+L+S PTs naifs HIV-1 RNA >1000 CD4 d’indication aux ARV Genotype vierge Global enrollment complete in early July, 2004 First Data Monitoring Committee meeting scheduled near CROI 2005 Large majority of subjects are eligible for deintensification (92/104) Resistance exclusion criteria: Trugene HIV-1 resistance report indicates resistance or possible resistance to the study RTIs (efavirenz, lamivudine, zidovudine) OR The presence of any mutation in the protease gene leading to an amino acid substitution at the following loci: 8, 30, 32, 46, 47, 48, 50, 54, 82, 84, or 90 Four or more mutations at the following loci: 10, 20, 24, 36, 53, 63, or 71 Objectif primaire : charge virale < 50 c/mL à S 48 ou S 96 (12 ou 24 mois)
 Resistance exclusion criteria: Trugene HIV-1 resistance report indicates resistance or possible resistance to the study RTIs (efavirenz, lamivudine, zidovudine) OR. The presence of any mutation in the protease gene leading to an amino acid substitution at the following loci: 8, 30, 32, 46, 47, 48, 50, 54, 82, 84, or 90. Four or more mutations at the following loci: 10, 20, 24, 36, 53, 63, or 71. Objectif primaire : charge virale < 50 c/mL. à S 48 ou S 96 (12 ou 24 mois)")
19
« Ca ne marchera jamais ! »
TRILEGE G. Pialoux et al : N Engl J Med, 1998;339: ACTG 343 D.Havlir et al : N Engl J Med, 1998;339: ADAM trial: Maintenance therapy after quadruple Induction therapy in HIV1- infected individuals: Amsterdam Duration of Antiretroviral Medication. Reijers MH et al. Lancet 1998, 352: ADAM

20
INDUCTION-MAINTENANCE Cahier des charges 2006
Partir de plus haut qu’en 1996 (Trilege) Maintenir la charge virale < 40 copies/ml Optimiser la qualité de vie et l’observance Inscrire le traitement ARV dans la durée (échec des STI?) Mieux s’adapter aux co-morbidités et aux complications des ARV antérieurs Préserver les autres stratégies ARV
 Maintenir la charge virale < 40 copies/ml. Optimiser la qualité de vie et l’observance. Inscrire le traitement ARV dans la durée (échec des STI ) Mieux s’adapter aux co-morbidités et aux complications des ARV antérieurs. Préserver les autres stratégies ARV.")
21
ESS40013 Study Design Open-label, 96-week, randomized, multicenter (40 US sites) study if HIV RNA <50 c/mL at weeks 36 and 44, randomized (n = 282) TZV+EFV (n = 141) TZV+EFV ART-naïve (n = 448) TZV (n=141) HIV RNA >5,000 c/mL No CD4 entry criteria Induction Phase: 48 weeks Maintenance Phase: 48 weeks Markowitz M, et al. J Acquir Immune Defic Syndr. 2005; 39:
 TZV+EFV. (n = 141) TZV+EFV. ART-naïve. (n = 448) TZV. (n=141) HIV RNA >5,000 c/mL. No CD4 entry criteria. Induction Phase: 48 weeks. Maintenance Phase: 48 weeks. Markowitz M, et al. J Acquir Immune Defic Syndr. 2005; 39:")
22
Maintenance Phase: HIV RNA <50 c/mL (ITT M=F)
ESS40013 Maintenance Phase: HIV RNA <50 c/mL (ITT M=F) P=0.697 79% 77% After a 48-week induction with TZV+EFV, non-inferiority of TZV compared to TZV+EFV was established during the 48-week maintenance phase Markowitz M, et al. J Acquir Immune Defic Syndr. 2005; 39:
 P= % 77% After a 48-week induction with TZV+EFV, non-inferiority of TZV compared. to TZV+EFV was established during the 48-week maintenance phase. Markowitz M, et al. J Acquir Immune Defic Syndr. 2005; 39:")
23
Median CD4 Cell Count (ITT Obs)
ESS40013 Median CD4 Cell Count (ITT Obs) Study Week TZV, n= TZV+EFV, n= Markowitz M, et al. J Acquir Immune Defic Syndr. 2005; 39: Data on file, GlaxoSmithKline [ESS40013 Final Study Report].
 Study Week. TZV, n= TZV+EFV, n= Markowitz M, et al. J Acquir Immune Defic Syndr. 2005; 39: Data on file, GlaxoSmithKline [ESS40013 Final Study Report].")
24
Study M03-613 LPV/r 400/100 mg BID LPV/r SGC 400/100 mg BID + ZDV/3TC (n=104) LPV/r 400/100 mg BID + ZDV/3TC 96 weeks Screening EFV 600 mg QD + ZDV/3TC (n=51) Rx naïve HIV-1 RNA >1000 Any CD4 count No evidence of resistance to study drugs Global enrollment complete in early July, 2004 First Data Monitoring Committee meeting scheduled near CROI 2005 Large majority of subjects are eligible for deintensification (92/104) Resistance exclusion criteria: Trugene HIV-1 resistance report indicates resistance or possible resistance to the study RTIs (efavirenz, lamivudine, zidovudine) OR The presence of any mutation in the protease gene leading to an amino acid substitution at the following loci: 8, 30, 32, 46, 47, 48, 50, 54, 82, 84, or 90 Four or more mutations at the following loci: 10, 20, 24, 36, 53, 63, or 71 Primary outcome: HIV-1 viral load < 50 c/mL at week 96 (24 months) Primary analysis: intention-to-treat, prior failure (> 50 c/mL x 2) = failure
 Rx naïve. HIV-1 RNA >1000. Any CD4 count. No evidence of. resistance to study drugs. Global enrollment complete in early July, First Data Monitoring Committee meeting scheduled near CROI Large majority of subjects are eligible for deintensification (92/104) Resistance exclusion criteria: Trugene HIV-1 resistance report indicates resistance or possible resistance to the study RTIs (efavirenz, lamivudine, zidovudine) OR. The presence of any mutation in the protease gene leading to an amino acid substitution at the following loci: 8, 30, 32, 46, 47, 48, 50, 54, 82, 84, or 90. Four or more mutations at the following loci: 10, 20, 24, 36, 53, 63, or 71. Primary outcome: HIV-1 viral load < 50 c/mL at week 96 (24 months) Primary analysis: intention-to-treat, prior failure (> 50 c/mL x 2) = failure.")
25
HIV-1 viral load < 50 c/mL (ITT, non-completer = failure)
Remember if D/C with all ITT, considered failure If undetectable with transient viral load rebound, success for ITT, NC=F (but failure for PF=F) If backbone regimen switch, then failure
 If backbone regimen switch, then failure.")
26
LPV/RTV Monotherapy as First-Line or Maintenance Therapy
Study MO3-613[1] MONARK[2] OK04[3] KALMO[4] Induction-maintenance monotherapy First-line monotherapy Simplification monotherapy Patient population Naive VL > 1000 Any CD4+ VL < 100,000 CD4+ > 100 Experienced w/o PI failure VL < 50 for > 6 months On LPV/r rx for > 1 month VL < 80 for > 6 months CD4+ > 200 Comparat. EFV + ZDV/3TC LPV/r + ZDV/3TC LPV/r + 2 NRTIs Continued HAART Primary endpoint VL < 50 at Wk 96 (ITT, prior failure = failure) VL < 400 at Wk 24 and < 50 at Wk 48 Therapeutic failure at Wk 48, defined as 2 VLs > wks apart w/o resuppression with added NRTIs VL < 80 by Wk 48 (with VF = confirmed VL > 1000) D/C, discontinued; Hx, history. 1. Cameron DW, et al. IAC Abstract THLB Delfraissy JF, et al. IAC Abstract THLB0202. 3. Arribas J et al. IAC Abstract THLB Nunez EP, et al. IAC Abstract THAB0102.
 VL < 400 at Wk 24 and < 50 at Wk 48. Therapeutic failure at Wk 48, defined as 2 VLs > wks apart w/o resuppression with added NRTIs. VL < 80 by Wk 48 (with VF = confirmed VL > 1000) D/C, discontinued; Hx, history. 1. Cameron DW, et al. IAC Abstract THLB Delfraissy JF, et al. IAC Abstract THLB Arribas J et al. IAC Abstract THLB Nunez EP, et al. IAC Abstract THAB0102.")
27
LPV/RTV Monotherapy as First-Line or Maintenance Therapy
Study MO3-613[1] MONARK[2] OK04[3] KALMO[4] Results VL < 50 copies/mL at Wk 96 (ITT, prior failure = failure): Mono: 50% EFV + ZDV/3TC: 61 % (p=0.23) VL < 400 at Wk 24 and <50 at Wk 48: Mono: 65% LPV/r + ZDV/3TC: 75% (p=0.25) Proportion w/o therapeutic failure at Wk 48: Mono: 94% HAART: 89.8% Noninferiority proven Time to VF not significantly different VL < 80 at Wk 96: Mono: 86% HAART: 83% 1. Cameron DW, et al. IAC Abstract THLB Delfraissy JF, et al. IAC Abstract THLB0202. 3. Arribas J et al. IAC Abstract THLB Nunez EP, et al. IAC Abstract THAB0102.
: Mono: 50% EFV + ZDV/3TC: 61 % (p=0.23) VL < 400 at Wk 24 and <50 at Wk 48: Mono: 65% LPV/r + ZDV/3TC: 75% (p=0.25) Proportion w/o therapeutic failure at Wk 48: Mono: 94% HAART: 89.8% Noninferiority proven. Time to VF not significantly different. VL < 80 at Wk 96: Mono: 86% HAART: 83% 1. Cameron DW, et al. IAC Abstract THLB Delfraissy JF, et al. IAC Abstract THLB Arribas J et al. IAC Abstract THLB Nunez EP, et al. IAC Abstract THAB0102.")
28
Les molécules en maintenance?
Kaletra® MM TMC 114 Fosamprénavir/r ? MK 0518 ? …etc

29
CONCLUSIONS AllègementS = possibles !
Induction-Maintenance : essais à reprendre avec le nouvelles molécules Allègement n’est pas dysobservance Entendre la demande (parole Associative)
")
Présentations similaires













 A.Compagnucci-A.Faye.>")



>")

