Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Recos RESURCOR 07 STEMI Les traitements « adjuvants »…

3
Prise en charge de l’IDM à la phase aigue en dehors des services de cardiologie

4
Si angioplastie primaire
Les stratégies de reperfusion et les traitements adjuvants à mettre en œuvre pour un SCA ST+ SCA ST+ Aspirine 160 à 500 mg Clopidogrel : < 75 ans 4 cps >75 ans 1cp Morphine titration Si thrombolyse Si angioplastie primaire < 75 ans Enoxaparine 30 mg IV 1mg/kg/12h SC >75ans HNF 60 UI/kg IV (<4000UI) 12 UI/kg/h (<1000UI) HNF 60 UI/kg IV (<4000UI) 12 UI/kg/h (<1000UI) Anti GPIIbIIIa
 12 UI/kg/h. (<1000UI) HNF 60 UI/kg IV (<4000UI) 12 UI/kg/h (<1000UI) Anti GPIIbIIIa.")
5
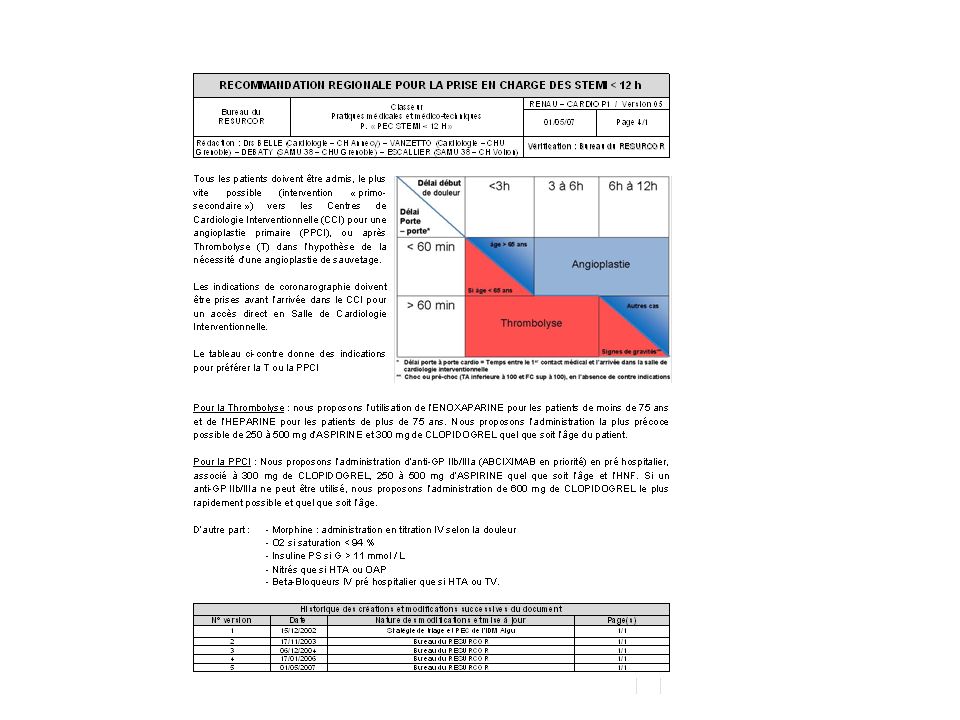
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
6
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
9
Lovenox réduit significativement les décès toute cause ou récidives d’infarctus du myocarde non fatals vs HNF à 30 jours (ITT) Enoxaparine (n=10 256) HNF (n=10 223) p= .0 2694 RRR 17% RR: 0.83, 95% CI: 0.77–0.90 ITT: Intent-to-treat , RRR: réduction risque relatif, RR: risque relatif
 Enoxaparine (n=10 256) HNF (n=10 223) p= RRR 17% RR: 0.83, 95% CI: 0.77–0.90. ITT: Intent-to-treat , RRR: réduction risque relatif, RR: risque relatif.")
10
Hémorragies à J 30 Patients (%) 10 Enoxaparine (n=10 176)
HNF (n=10 151) Patients (%) p<0.0001 p<0.0001 2.6 2.1 p=0.14 1.8 1.4 0.8 0.7 Hémorragies majeures * Hémorragies intra-crâniennes Hémorragies mineures Augmentation des hémorragies majeures sous enoxaparine vs HNF mais pas de différence entre les 2 groupes sur les hémorragies intra-crâniennes *y compris les Hémorragies intra-crâniennes
 Patients (%) p< p< p= Hémorragies majeures * Hémorragies. intra-crâniennes. Hémorragies mineures. Augmentation des hémorragies majeures sous enoxaparine vs HNF. mais pas de différence entre les 2 groupes sur les hémorragies intra-crâniennes. *y compris les Hémorragies intra-crâniennes.")
11
Bénéfice clinique net à J 30
HNF (%) Enox (%) RRR (%) Décès / IDM non fatal / AVC 12.3 10.1 18 Décès / IDM non fatal / Hémorragies majeures 12.8 11.0 14 Décès /IDM Nonfatal / Hémorragies intra-crâniennes 12.2 10.1 17 0.8 0.9 1 1.25 Enox Meilleure RR HNF Meilleure
 Enox (%) RRR (%) Décès / IDM non fatal / AVC Décès / IDM non fatal / Hémorragies majeures Décès /IDM Nonfatal / Hémorragies intra-crâniennes Enox Meilleure. RR. HNF Meilleure.")
12
Key data presented at ACC New Orleans March 2007
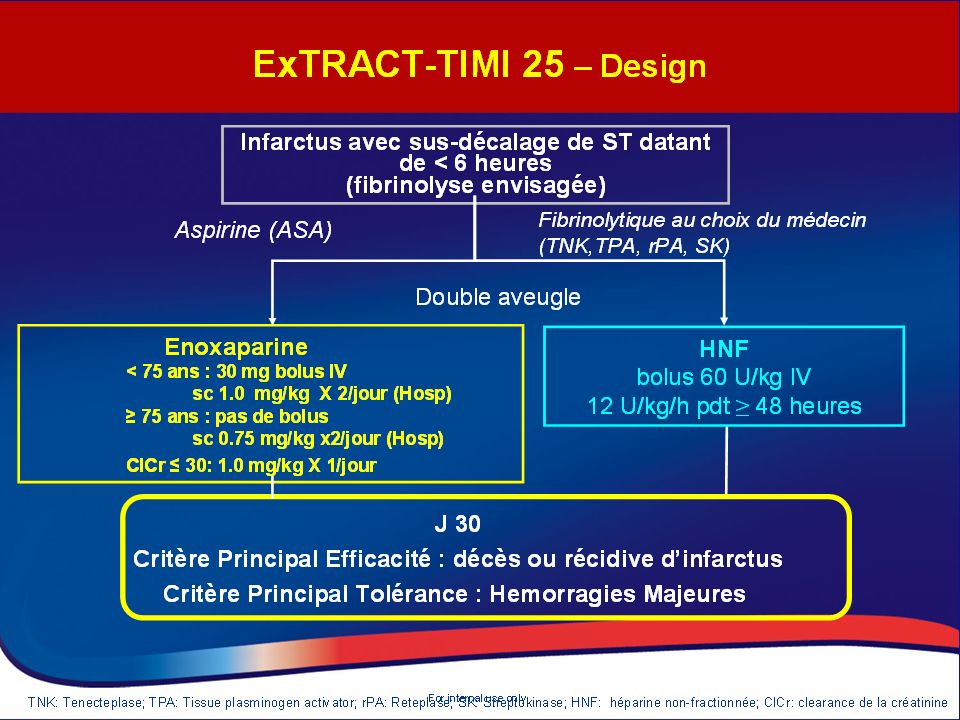
Enoxaparin and Thrombolysis Reperfusion for Acute Myocardial Infarction ExTRACT-TIMI 25 Key data presented at ACC New Orleans March 2007

13
TIMI major bleeding Stratified by age
ARD 0.8% RR 1.67 ( ) p=<0.0001 ARD 0.4% RR 1.15 ( ) p=0.53
 p=< ARD 0.4% RR 1.15 ( ) p=0.53.")
14
Enoxaparin versus UFH in STEMI A Meta-Analysis of 27,000 Patients

15
CLARITY : HBPM VS HNF Sabatine MS et al Circulation 2005;112:

16
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
17
Additional efficacy of antiplatelet therapy: ISIS-2
1986: GISSI, first demonstration of the role of IV thrombolysis 1988: ISIS-2 pts with suspected MI < 24 h Factorial design: SK (1,5 M U over1 h) aspirin (160 mg) combination placebo Lancet1988
 aspirin (160 mg) combination. placebo. Lancet1988.")
18
CLopidogrel as Adjunctive ReperfusIon TherapY – Thrombolysis In Myocardial Infarction (TIMI) 28
 28")
19
The Clarity Ambulance Substudy
Prehospital Fibrinolysis with Double Antiplatelet Therapy in Acute ST-Elevation Myocardial Infarction: The Clarity Ambulance Substudy In CLARITY, the addition of clopidogrel to aspirin in fibrinolytic therapy for ST-elevation MI improved coronary patency and reduced ischemic events. As just presented, early clopidogrel treatment was also associated with improved clinical outcomes in patients undergoing PCI after the initial lytic therapy. In CLARITY, a subgroup of patients was randomized in the ambulance and treated earlier than the other patients; we present here the analysis of this subgroup Verheugt F et al. J Thromb Thrombolysis 2007;23:

20
Randomised to clopidogrel or placebo in the ambulance or on admission
3491 patients aged <76 years with STEMI, receiving fibrinolytic therapy Randomised to clopidogrel or placebo in the ambulance or on admission p=0.05 p=0.02 Patients with ST-segment resolution at ECG (%) Off-label: Use when asked about pre-hospital treatment A prespecified subgroup analysis of the CLARITY-TIMI 28 trial. At 11 ambulance sites in France, Sweden, and Northern Ireland 216 patients randomised between February and October received fibrinolysis, aspirin, and heparin together with study drug in the ambulance before hospital admission. The proportion of patients with early (90 min) ST-segment resolution was higher in the group randomised in the ambulance than in the group randomised upon administration. This is the first trial to evaluate different oral antiplatelet strategies in the pre-hospital treatment of ST-elevated myocardial infarction. This sub-study suggests that, in comparison with aspirin alone, dual antiplatelet therapy combined with a fibrin-specific lytic given in a pre-hospital setting is associated with a better patency of the infarct-related artery at follow-up angiography. The mechanism by which clopidogrel is helpful in lytic therapy is probably prevention of reocclusion rather than better early reperfusion. Also shown in this trial, pre-hospital fibrinolysis reduces time to treatment by approximately 55 minutes, which would result in a 15% relative risk reduction in early mortality based on a meta-analysis published in Similar to the main CLARITY-TIMI 28 trial, no increase in severe bleeding (especially intracranial haemorrhage) was seen. Additionally, the data may support the feasibility of pre-hospital clopidogrel in patients before transfer for primary percutaneous coronary intervention. Key message: Clopidogrel, given in the ambulance, is associated with more rapid ST-segment resolution than aspirin alone Time after administration of loading dose Clopidogrel given in the ambulance is associated with ST-segment resolution Verheugt F et al. J Thromb Thrombolysis 2007;23: Verheugt F et al. J Thromb Thrombolysis 2006;Dec 6 [epub]
 Off-label: Use when asked about pre-hospital treatment. A prespecified subgroup analysis of the CLARITY-TIMI 28 trial. At 11 ambulance sites in France, Sweden, and Northern Ireland 216 patients randomised between February and October received fibrinolysis, aspirin, and heparin together with study drug in the ambulance before hospital admission. The proportion of patients with early (90 min) ST-segment resolution was higher in the group randomised in the ambulance than in the group randomised upon administration. This is the first trial to evaluate different oral antiplatelet strategies in the pre-hospital treatment of ST-elevated myocardial infarction. This sub-study suggests that, in comparison with aspirin alone, dual antiplatelet therapy combined with a fibrin-specific lytic given in a pre-hospital setting is associated with a better patency of the infarct-related artery at follow-up angiography. The mechanism by which clopidogrel is helpful in lytic therapy is probably prevention of reocclusion rather than better early reperfusion. Also shown in this trial, pre-hospital fibrinolysis reduces time to treatment by approximately 55 minutes, which would result in a 15% relative risk reduction in early mortality based on a meta-analysis published in Similar to the main CLARITY-TIMI 28 trial, no increase in severe bleeding (especially intracranial haemorrhage) was seen. Additionally, the data may support the feasibility of pre-hospital clopidogrel in patients before transfer for primary percutaneous coronary intervention. Key message: Clopidogrel, given in the ambulance, is associated with more rapid ST-segment resolution than aspirin alone. Time after administration of loading dose. Clopidogrel given in the ambulance is associated with ST-segment resolution. Verheugt F et al. J Thromb Thrombolysis 2007;23: Verheugt F et al. J Thromb Thrombolysis 2006;Dec 6 [epub]")
21
Death, re-MI or stroke (%)
COMMIT: Effects of clopidogrel on death, re-MI or stroke Placebo + ASA: 2310 with event (10.1%) Days since randomisation (up to 28 days) Death, re-MI or stroke (%) 7 14 21 28 1 2 3 4 5 6 8 9 Clopidogrel + ASA: 2121 with event (9.2%) 9% (SE3) relative risk reduction (2p=0.002)
 Days since randomisation (up to 28 days) Death, re-MI or stroke (%) Clopidogrel + ASA: 2121 with event (9.2%) 9% (SE3) relative risk. reduction (2p=0.002)")
22
Bleeding Outcome Clopidogrel (%) Placebo (%) P 1.3 1.1 NS 1.0 0.5 0.7
Through angiography TIMI major 1.3 1.1 NS TIMI minor 1.0 0.5 Intracranial hemorrhage 0.7 Through 30 days 1.9 1.7 In those undergoing CABG 7.5 7.2 CABG w/in 5 d of study med 9.1 7.9 1.6 0.9 Sabatine et al. NEJM 2005; 352: 1179

23
Clopidorel in ExTRACT TIMI 25
ARR 2.4% (-0.5, 5.3%) ARR 1.7% (0.5, 3.0%) UFH ENOX Pinteraction=0.61 (1083) (1090) (6528) (6390) Clopidogrel No Clopidogrel ExTRACT-TIMI 25
 ARR 1.7% (0.5, 3.0%) UFH. ENOX. Pinteraction=0.61. (1083) (1090) (6528) (6390) Clopidogrel. No Clopidogrel. ExTRACT-TIMI 25.")
24
Régression du ST ≥ 70 % OPTIMAL Début douleur / thrombolyse ≤ 1 h
ORs ajustés associés à la probabilité de présenter une régression du ST ≥ 70 % Début douleur / thrombolyse ≤ 1 h OR = 1,62 Diabète 0,60 Fumeur / ex fumeur 1,5 Sus décalage max ≤ 2 mm 1,75 IDM non antérieur * 1,65 Thiénopyridine ** 2,13 Nitré ** 0,72 * Inférieur, latéral, antéro-latéral, antéro-inférieur ** Lors de la prise en charge pré-hospitalière OPTIMAL

25
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
26
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
27
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
28
Clopidogrel data CURE Death/MI/Stoke at 1yr PCI-CURE Death/MI at 1 yr
CREDO CLARITY Death/MI/RI at 1mth Death at 1mth COMMIT D/MI/stroke at 3yrs CAPRIE

29
1-year incidence of MACE (%)
ACOS: STEMI patients receiving clopidogrel had a lower incidence of events after 1 year Prospective multicentre observational registry of 5886 STEMI patients 15.4 20.7 10.4 10.9 7.1 13.1 6.1 6.4 5 10 15 20 25 Total group No reperfusion Fibrinolysis Primary PCI 1-year incidence of MACE (%) ASA-alone (n=2091) Clopidogrel + ASA (n=3795) Topic: Clopidogrel duration of therapy in STEMI This analysis sought to assess the effect of clopidogrel on clinical events 1 year after discharge in survivors of ST-elevation myocardial infarction (STEMI) in clinical practice. The authors analysed data of consecutive survivors of acute STEMI and either concomitant therapy with acetylsalicylic acid (ASA) or ASA plus clopidogrel at discharge, who were prospectively enrolled in the Acute Coronary Syndromes (ACOS) registry between July 2000 and November A total of 5886 (3795 with and 2091 without clopidogrel) patients were included into this analysis. Patients were divided into three groups according to the initial reperfusion therapy: no reperfusion therapy (n=1445), fibrinolysis (n=1734), or primary percutaneous coronary intervention (PCI) (n=2707). The multivariable analysis for 12 plus 2-month mortality after discharge using the propensity score with adjustment for baseline characteristics and treatments showed that mortality was significantly lower in the ASA plus clopidogrel group compared with the ASA alone group, and in patients with reperfusion therapy [total group, OR 0.48, no reperfusion therapy, OR 0.96, fibrinolysis, OR 0.53, primary PCI, OR 0.38]. This analysis is the first evaluation of a large registry with STEMI patients that investigates the effect of clopidogrel after STEMI. The reduction of mortality was approximately 5% in patients with fibrinolysis and primary PCI, and remained significant after adjustment in the multivariable analysis. These registry results are the first showing a mortality advantage for clopidogrel. As ACOS is a clinical registry for acute coronary syndromes (ACS) and not a randomised clinical trial, reasons for the findings cannot be certain. The mortality in these patients was higher than that in the CURE and CREDO Trials, which means that these patients belong to a higher risk group. Therefore, the absolute benefit might be more pronounced than in the trial patients. Since drug-eluting stents were not used in these patients, late stent thrombosis does not account for the difference in events in patients after stenting. Clopidogrel given for up to 1 year after planned PCI and in non-STE ACS patients has been shown to be cost effective. In the light of these results, clopidogrel might be a cost-effective therapy in STEMI patients. In clinical practice, adjunctive therapy with clopidogrel, in addition to ASA, in survivors after STEMI is associated with a reduction in 1-year mortality in patients treated with early reperfusion therapy. STEMI, ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; ASA, acetylsalicylic acid; MACE = death, non-fatal re-infarction, non-fatal stroke Patients receiving clopidogrel had improved outcomes at 1 year Zeymer U et al. Eur Heart J. 2006;27(22): Zeymer U et al. Eur Heart J. 2006;27(22):
 ASA-alone (n=2091) Clopidogrel + ASA (n=3795) Topic: Clopidogrel duration of therapy in STEMI. This analysis sought to assess the effect of clopidogrel on clinical events 1 year after discharge in survivors of ST-elevation myocardial infarction (STEMI) in clinical practice. The authors analysed data of consecutive survivors of acute STEMI and either concomitant therapy with acetylsalicylic acid (ASA) or ASA plus clopidogrel at discharge, who were prospectively enrolled in the Acute Coronary Syndromes (ACOS) registry between July 2000 and November A total of 5886 (3795 with and 2091 without clopidogrel) patients were included into this analysis. Patients were divided into three groups according to the initial reperfusion therapy: no reperfusion therapy (n=1445), fibrinolysis (n=1734), or primary percutaneous coronary intervention (PCI) (n=2707). The multivariable analysis for 12 plus 2-month mortality after discharge using the propensity score with adjustment for baseline characteristics and treatments showed that mortality was significantly lower in the ASA plus clopidogrel group compared with the ASA alone group, and in patients with reperfusion therapy [total group, OR 0.48, no reperfusion therapy, OR 0.96, fibrinolysis, OR 0.53, primary PCI, OR 0.38]. This analysis is the first evaluation of a large registry with STEMI patients that investigates the effect of clopidogrel after STEMI. The reduction of mortality was approximately 5% in patients with fibrinolysis and primary PCI, and remained significant after adjustment in the multivariable analysis. These registry results are the first showing a mortality advantage for clopidogrel. As ACOS is a clinical registry for acute coronary syndromes (ACS) and not a randomised clinical trial, reasons for the findings cannot be certain. The mortality in these patients was higher than that in the CURE and CREDO Trials, which means that these patients belong to a higher risk group. Therefore, the absolute benefit might be more pronounced than in the trial patients. Since drug-eluting stents were not used in these patients, late stent thrombosis does not account for the difference in events in patients after stenting. Clopidogrel given for up to 1 year after planned PCI and in non-STE ACS patients has been shown to be cost effective. In the light of these results, clopidogrel might be a cost-effective therapy in STEMI patients. In clinical practice, adjunctive therapy with clopidogrel, in addition to ASA, in survivors after STEMI is associated with a reduction in 1-year mortality in patients treated with early reperfusion therapy. STEMI, ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; ASA, acetylsalicylic acid; MACE = death, non-fatal re-infarction, non-fatal stroke. Patients receiving clopidogrel had improved outcomes at 1 year. Zeymer U et al. Eur Heart J. 2006;27(22): Zeymer U et al. Eur Heart J. 2006;27(22):")
30
Early use of clopidogrel prior to PCI
206 consecutive patients admitted with STEMI before PCI 18% had spontaneous ST-segment resolution (STR) Spontaneous STR p=0.70 p=0.96 p=0.045 p=0.33 Patients receiving treatment before angiography (%) Off-label: Use when asked about pre-treatment in primary PCI Spontaneous ST-segment resolution (STR) after acute ST-elevation myocardial infarction (STEMI) is associated with favourable outcomes. Effect on STR of newer, more powerful antiplatelet and anti-thrombotic agents is unclear. The aim of this study was to identify independent clinical and angiographic predictors of STR in patients with STEMI before (percutaneous coronary intervention) PCI. We studied 206 patients admitted with STEMI, of whom 37 (18%) had STR. Emergency room clopidogrel loading dose was administered to 103 patients. Patients with STR had shorter hospital stays and reduced incidence of in-hospital arrhythmias or death. Administration of aspirin, heparin, or eptifibatide before PCI was not an independent predictor of STR. However, independent predictors of STR were early clopidogrel administration (OR 2.10, p=0.045), single-vessel disease (OR 2.85, p=0.02), chest pain duration (OR 0.98, p<0.0001), collaterals (OR 4.3, p=0.002), circumflex as a culprit vessel (OR 4.74, p=0.008), and coronary thrombus noted on angiography (OR 5.76, p=0.006). In conclusion, early clopidogrel administration is associated with, and likely causal for, STR. Patients with thrombus, collateral flow, and circumflex culprit vessel are more likely to have STR. In addition, our study confirms previous findings that patients with STR have preserved left ventricular function and better hospital outcomes compared with those without STR. Our study shows that early administration of loading dose of clopidogrel 300 mg plus aspirin, rather than aspirin alone, to patients with STEMI in the ambulance or emergency room doubled the rate of STR before PCI. Our data show that clopidogrel given with aspirin in the emergency department approximately 1 hour before PCI is associated with a higher frequency of STR. It is likely that clopidogrel is causal for increased STR in our study. Until definitive data are obtained, it is reasonable to recommend that patients with coronary disease have aspirin 325 mg and clopidogrel 300 mg available for administration on their way to the emergency room for severe chest pain unresponsive to nitroglycerin. Key message: Early use of clopidogrel prior to PCI is associated with a significant increase in the frequency of STR p=94 PCI, percutaneous coronary intervention; STEMI, ST-elevated myocardial infarction Early use of clopidogrel appears causal for increased STR Jabaren M et al. Am J Cardiol 2006;98:1435–1438 Jabaren M et al. Am J Cardiol 2006;98:1435–1438
 Spontaneous STR. p=0.70. p=0.96. p= p=0.33. Patients receiving treatment. before angiography (%) Off-label: Use when asked about pre-treatment in primary PCI. Spontaneous ST-segment resolution (STR) after acute ST-elevation myocardial infarction (STEMI) is associated with favourable outcomes. Effect on STR of newer, more powerful antiplatelet and anti-thrombotic agents is unclear. The aim of this study was to identify independent clinical and angiographic predictors of STR in patients with STEMI before (percutaneous coronary intervention) PCI. We studied 206 patients admitted with STEMI, of whom 37 (18%) had STR. Emergency room clopidogrel loading dose was administered to 103 patients. Patients with STR had shorter hospital stays and reduced incidence of in-hospital arrhythmias or death. Administration of aspirin, heparin, or eptifibatide before PCI was not an independent predictor of STR. However, independent predictors of STR were early clopidogrel administration (OR 2.10, p=0.045), single-vessel disease (OR 2.85, p=0.02), chest pain duration (OR 0.98, p<0.0001), collaterals (OR 4.3, p=0.002), circumflex as a culprit vessel (OR 4.74, p=0.008), and coronary thrombus noted on angiography (OR 5.76, p=0.006). In conclusion, early clopidogrel administration is associated with, and likely causal for, STR. Patients with thrombus, collateral flow, and circumflex culprit vessel are more likely to have STR. In addition, our study confirms previous findings that patients with STR have preserved left ventricular function and better hospital outcomes compared with those without STR. Our study shows that early administration of loading dose of clopidogrel 300 mg plus aspirin, rather than aspirin alone, to patients with STEMI in the ambulance or emergency room doubled the rate of STR before PCI. Our data show that clopidogrel given with aspirin in the emergency department approximately 1 hour before PCI is associated with a higher frequency of STR. It is likely that clopidogrel is causal for increased STR in our study. Until definitive data are obtained, it is reasonable to recommend that patients with coronary disease have aspirin 325 mg and clopidogrel 300 mg available for administration on their way to the emergency room for severe chest pain unresponsive to nitroglycerin. Key message: Early use of clopidogrel prior to PCI is associated with a significant increase in the frequency of STR. p=94. PCI, percutaneous coronary intervention; STEMI, ST-elevated myocardial infarction. Early use of clopidogrel appears causal for increased STR. Jabaren M et al. Am J Cardiol 2006;98:1435–1438. Jabaren M et al. Am J Cardiol 2006;98:1435–1438.")
31
In-hospital mortality according to pre-hospital antiplatelet agents
FAST MI 2005

32
Guidelines for percutaneous coronary interventions EHJ 15 march 2005
« Une dose de charge de 300 mg de Clopidogrel doit etre donnée au moins 6 heures avant une angioplastie coronaire, sinon, une dose de 600mg est requise… »

33
Inhibition of platelet aggregation (%)
ALBION: Clopidogrel 600 mg provides more rapid inhibition of platelet aggregation 103 patients with NSTE ACS randomised to receive 300, 600 or 900 mg clopidogrel 50 5 μmol/L ADP * 900 mg 600 mg * 40 30 300 mg Inhibition of platelet aggregation (%) 20 10 *p<0.05 vs 300 mg 1 2 3 4 5 6 Time (hours) Greater loading doses are associated with a significantly faster onset of inhibition Montalescot G et al. J Am Coll Cardiol 2006;48:931–938. Montalescot et al. JACC 2006;48:931-8
 *p<0.05 vs 300 mg Time (hours) Greater loading doses are associated with a significantly faster onset of inhibition. Montalescot G et al. J Am Coll Cardiol 2006;48:931–938. Montalescot et al. JACC 2006;48:")
34
Clopidogrel 600 mg vs. 300 mg loading dose
292 consecutive NSTE ACS stent patients received 300 or 600 mg loading dose of clopidogrel 100 Events (%) 12.5 2.5 7.5 10.0 5.0 600 mg 300 mg 95 600 mg 90 p<0.0024 CV event-free survival (%) 85 300 mg 80 10 20 30 CV events ACS events ST Stroke CV death Time (days) Using a loading dose of clopidogrel 600 mg reduced the occurrence of events vs. 300 mg Cuisset T et al. J Am Coll Cardiol 2006;48:1339–1345. Cuisset et al. J Am Coll Cardiol 2006; 48:1339–45
 mg. 300 mg mg. 90. p< CV event-free survival (%) mg CV events. ACS events. ST. Stroke. CV death. Time (days) Using a loading dose of clopidogrel 600 mg reduced the occurrence of events vs. 300 mg. Cuisset T et al. J Am Coll Cardiol 2006;48:1339–1345. Cuisset et al. J Am Coll Cardiol 2006; 48:1339–45.")
35
CIPAMI: Study design R Treatment according to investigator n=327
Clopidogrel 600 mg Treatment according to investigator n=654 with STEMI Acute STEMI <6h Angina >20 min ST elevation >2 leads or new/presumed LBBB Primary angiography Primary endpoint PCI (Secondary endpoints) Death, Re-MI, TVR R ASA + UFH/enoxaparin Topic: Pre-treatment with clopidogrel in primary PCI Clopidogrel, in combination with acetylsalicylic acid (ASA), has become a mainstay of the pharmacological therapy for patients with acute coronary syndromes, especially in those undergoing percutaneous coronary interventions (PCI). Although studies have shown that pre-treatment with a loading dose of clopidogrel 300 or 600 mg before PCI is effective in reducing cardiovascular complications, the optimal dose and timing in various patient groups is still unclear. The primary objective of the present randomised, open-label Clopidogrel to Improve Primary percutaneous coronary Intervention in Acute Myocardial Infarction (CIPAMI) study is to evaluate the efficacy and the safety of a 600 mg loading dose of clopidogrel in addition to standard ASA/heparin treatment in the pre-hospital setting in 654 patients with acute ST-elevation myocardial infarction scheduled for primary PCI. The primary efficacy endpoint is the TIMI 2/3 patency of the infarct-related artery immediately prior to PCI. n=327 No loading Clopidogrel loading prior to PCI strongly recommended Pre-hospital Hospital until discharge or day 7 Zeymer U et al. Cardiology 2007;108:265–272 Zeymer U et al. Cardiology 2007;108:265–272
 Death, Re-MI, TVR. R. ASA + UFH/enoxaparin. Topic: Pre-treatment with clopidogrel in primary PCI. Clopidogrel, in combination with acetylsalicylic acid (ASA), has become a mainstay of the pharmacological therapy for patients with acute coronary syndromes, especially in those undergoing percutaneous coronary interventions (PCI). Although studies have shown that pre-treatment with a loading dose of clopidogrel 300 or 600 mg before PCI is effective in reducing cardiovascular complications, the optimal dose and timing in various patient groups is still unclear. The primary objective of the present randomised, open-label Clopidogrel to Improve Primary percutaneous coronary Intervention in Acute Myocardial Infarction (CIPAMI) study is to evaluate the efficacy and the safety of a 600 mg loading dose of clopidogrel in addition to standard ASA/heparin treatment in the pre-hospital setting in 654 patients with acute ST-elevation myocardial infarction scheduled for primary PCI. The primary efficacy endpoint is the TIMI 2/3 patency of the infarct-related artery immediately prior to PCI. n=327. No loading. Clopidogrel loading prior to PCI strongly recommended. Pre-hospital. Hospital until discharge or day 7. Zeymer U et al. Cardiology 2007;108:265–272. Zeymer U et al. Cardiology 2007;108:265–272.")
36
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
38
Association between hyperglycemia and the No-Reflow phenomenon in patients with acute myocardial infarction % P < 0.001 With hyperglycemia With hyperglycemia > 160 mg/dL < 160 mg/dL Iwakura K et al. JACC. 2003;41:1-7.

39
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
41
Régression du ST ≥ 70 % OPTIMAL Début douleur / thrombolyse ≤ 1 h
ORs ajustés associés à la probabilité de présenter une régression du ST ≥ 70 % Début douleur / thrombolyse ≤ 1 h OR = 1,62 Diabète 0,60 Fumeur / ex fumeur 1,5 Sus décalage max ≤ 2 mm 1,75 IDM non antérieur * 1,65 Thiénopyridine ** 2,13 Nitré ** 0,72 * Inférieur, latéral, antéro-latéral, antéro-inférieur ** Lors de la prise en charge pré-hospitalière OPTIMAL

42
Multivariable analysis of predictors of in-hospital death
95% CI P value Age (vs <65 yrs) 65-74 75+ 2.45 6.52 0.011 0.0001 Admission HR 1.02 Admission SBP 0.98 use of nitrates 2.30 0.002 Family history 0.42 0.025 FAST MI 2005
 Admission HR Admission SBP use of nitrates Family history FAST MI")
43
Pour la Thrombolyse : nous proposons l’utilisation de l’ENOXAPARINE pour les patients de moins de 75 ans et de l’HEPARINE pour les patients de plus de 75 ans. Nous proposons l’administration la plus précoce possible de 250 à 500 mg d’ASPIRINE et 300 mg de CLOPIDOGREL quel que soit l’âge du patient. Pour la PPCI : Nous proposons l’administration d’anti-GP IIb/IIIa (ABCIXIMAB en priorité) en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP Beta-Bloqueurs IV pré hospitalier que si HTA ou TV.
 en pré hospitalier, associé à 300 mg de CLOPIDOGREL, 250 à 500 mg d’ASPIRINE quel que soit l’âge et l’HNF. Si un anti‑GP IIb/IIIa ne peut être utilisé, nous proposons l’administration de 600 mg de CLOPIDOGREL le plus rapidement possible et quel que soit l’âge. D’autre part : - Morphine : administration en titration IV selon la douleur - O2 si saturation < 94 % - Insuline PS si G > 11 mmol / L - Nitrés que si HTA ou OAP - Beta-Bloqueurs IV pré hospitalier que si HTA ou TV..")
Présentations similaires






>")













