Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
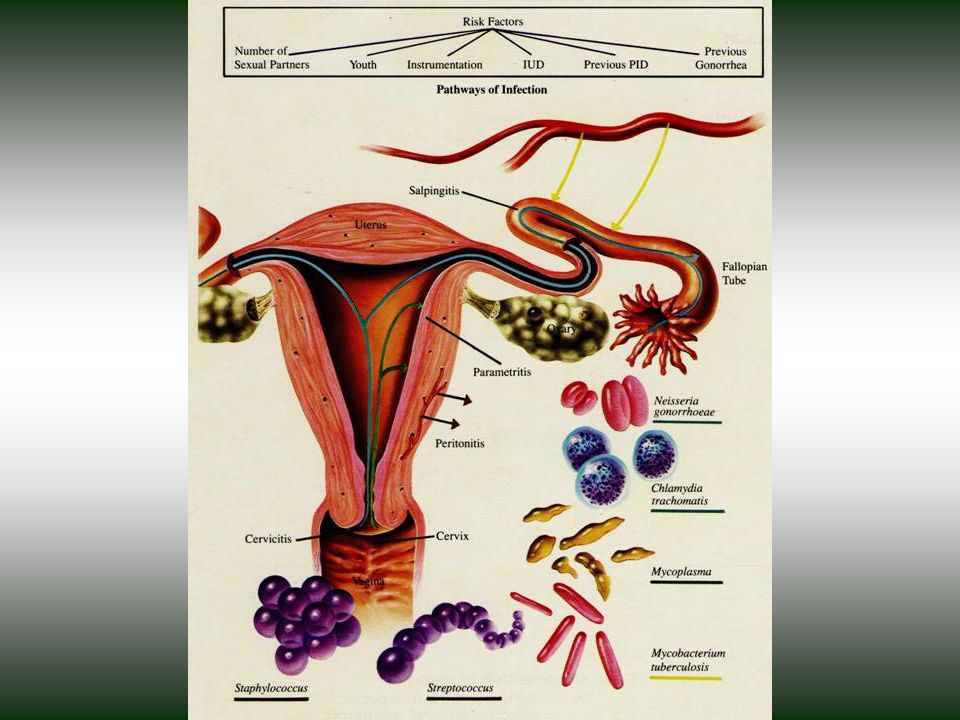
GONOCOCCIE Maladie bactérienne quasi exclusivement STI ou à transmission périnatale due à Neisseria gonorrohoeae 2. Atteintes muqueuses surtout uréthrales et cervicales mais aussi, rectale, oro-pharyngée, conjonctivale 3. Responsable d’infections génitales hautes causes de GEU et d`infertilité 4. Dissémination possible: arthrites, endocardites

2
Neisseria gonorrohoeae
Diplocoque Gram- en grain de café non mobile, ne formant pas de spores: - ressemble beaucoup à N meningitidis - fragile au déssechement: inoculation rapide - max 6 hres dans milieu de transport - culture sur gélose chocolat (Thayer Martin modifié), sans vancomycine si résistance élevés, en présence de 5% de CO2. - strictement aéorobies en conditions normales peuvent pousser en anaérobiose (trompes de Fallope) 2. Structure d’enveloppe proche des autres BGN
, sans vancomycine si résistance élevés, en présence de 5% de CO2. - strictement aéorobies en conditions normales peuvent pousser en anaérobiose (trompes de Fallope) 2. Structure d’enveloppe proche des autres BGN.")
3
FIGURE Schematic representation of the surface structure of Neisseria gonorrhoeae, showing the major components that contribute to pathogenicity. Opa, Por, and Rmp are the designations of the major outer membrane proteins. (see text); LOS, lipo-oligosaccharide. Schematic representation of the surface structure of Neisseria gonorrhoeae, showing the major components that contribute to pathogenicity. Opa, Por, and Rmp are the designations of the major outer membrane proteins. LOS, lipo-oligosaccharide.

4
FIGURE Nesseria gonorrhoeae with numerous pili extending from the cell surface. (Courtesy of Dr. Gour Biswas, Chapel Hill, NC.)
.")
5
FIGURE 209-3A. Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. A, Attachment of the piliated gonococci to the surface of a nonciliated host cell. B, Endocytosis of gonococci and loss of cilia on adjacent cells, mediated by lipo-oligosaccharide (LOS). C, Transport of gonococci through an epithelial cell in an endocytotic vacuole, in which the organism may replicate; progression of LOS-associated cytotoxicity. D, Release of organisms into subepithelial space. (From Dallabetta G, Hook EW III. Gonococcal infections. Infect Dis Clin North Am 1987;1:25-54.) Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. A, Attachment of the piliated gonococci to the surface of a nonciliated host cell.

6
FIGURE 209-3B. Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. A, Attachment of the piliated gonococci to the surface of a nonciliated host cell. B, Endocytosis of gonococci and loss of cilia on adjacent cells, mediated by lipo-oligosaccharide (LOS). C, Transport of gonococci through an epithelial cell in an endocytotic vacuole, in which the organism may replicate; progression of LOS-associated cytotoxicity. D, Release of organisms into subepithelial space. (From Dallabetta G, Hook EW III. Gonococcal infections. Infect Dis Clin North Am 1987;1:25-54.) Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. B, Endocytosis of gonococci and loss of cilia on adjacent cells, mediated by lipo-oligosaccharide (LOS).
.")
7
FIGURE 209-3C. Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. A, Attachment of the piliated gonococci to the surface of a nonciliated host cell. B, Endocytosis of gonococci and loss of cilia on adjacent cells, mediated by lipo-oligosaccharide (LOS). C, Transport of gonococci through an epithelial cell in an endocytotic vacuole, in which the organism may replicate; progression of LOS-associated cytotoxicity. D, Release of organisms into subepithelial space. (From Dallabetta G, Hook EW III. Gonococcal infections. Infect Dis Clin North Am 1987;1:25-54.) Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. C, Transport of gonococci through an epithelial cell in an endocytotic vacuole, in which the organism may replicate; progression of LOS-associated cytotoxicity.

8
FIGURE 209-3D. Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. A, Attachment of the piliated gonococci to the surface of a nonciliated host cell. B, Endocytosis of gonococci and loss of cilia on adjacent cells, mediated by lipo-oligosaccharide (LOS). C, Transport of gonococci through an epithelial cell in an endocytotic vacuole, in which the organism may replicate; progression of LOS-associated cytotoxicity. D, Release of organisms into subepithelial space. (From Dallabetta G, Hook EW III. Gonococcal infections. Infect Dis Clin North Am 1987;1:25-54.) Schematic representation of the interaction between fallopian tube explant epithelial cells and Neisseria gonorrhoeae. D, Release of organisms into subepithelial space.

9
Neisseria gonorrohoeae
Beaucoup ont un plasmide de conjugaison de 24,5 mD et donc capables de transmettre avec grande efficience d’autres plasmides non tranferrables et à l’origine de hauts niveaux de résistance à la tétracycline (1985) 2. Les 2 plasmides Pcr les plus commune ont 3.2 et 4,4 mD et seraient originaires de H. ducreyi. Elles sont à l’origine d’une betalactamase (1970) 3. Mutations chromosomiques à l’origine de résistance à tetracycline, macrolides, péni G, céphalosporines, quinolones (1994) 4. Sélections résistance > chez MSM (s bil, ac G)
 2. Les 2 plasmides Pcr les plus commune ont 3.2 et 4,4 mD et seraient originaires de H. ducreyi. Elles sont à l’origine d’une betalactamase (1970) 3. Mutations chromosomiques à l’origine de résistance à tetracycline, macrolides, péni G, céphalosporines, quinolones (1994) 4. Sélections résistance > chez MSM (s bil, ac G)")
10
Résistance du gonocoque à la pénicilline

11
Résistance du gonocoque aux quinolones

12
Résistance du gonocoque à la ceftriaxone

13
Epidémiologie J Tapsall, session 1334, ICAAC, 2005 Gonocoque :
environ 60 millions de nouveaux cas par an pays en développement: incidence élevée, et qui reste élevée pays industrialisés: incidence plus faible, mais en augmentation Résistance aux antibiotiques en augmentation : pénicilline : années 1970s spectinomycine: années 1980s quinolones: années 1990s céphalosporines 3ème génération: années 2000s ? J Tapsall, session 1334, ICAAC, 2005

15
FIGURE Distribution of reported gonorrhea incidence according to age and sex, United States, (From Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, Atlanta, GA: U.S. Department of Health and Human Services, 2003.) Distribution of reported gonorrhea incidence according to age and sex, United States, 2002

17
FIGURE Incidence of reported gonorrhea per 100,000 residents, United States, (From Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, Atlanta, GA: U.S. Department of Health and Human Services, 2003.) Incidence of reported gonorrhea per 100,000 residents, United States,

18
TABLE Reported Cases and Rates of Gonorrhea According to Race and Ethnicity, United States, 2002

19
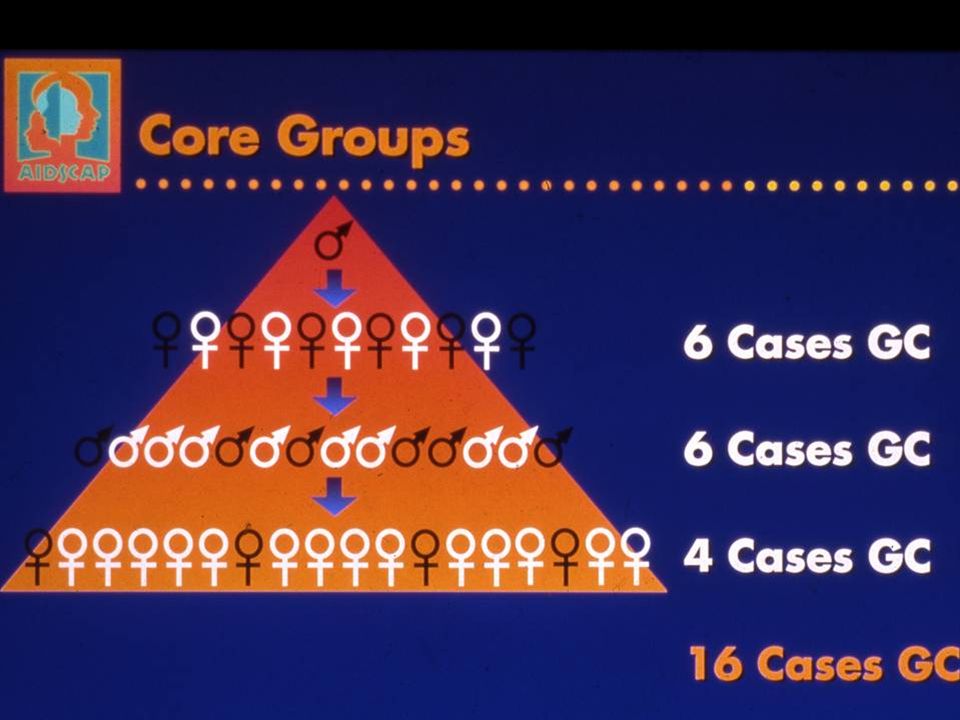
GA Dallabetta, M Laga, P Lamptey
GA Dallabetta, M Laga, P Lamptey. Control of STDs Handbook AIDSCAP, 1996

20
GA Dallabetta, M Laga, P Lamptey
GA Dallabetta, M Laga, P Lamptey. Control of STDs Handbook AIDSCAP, 1996

22
GA Dallabetta, M Laga, P Lamptey
GA Dallabetta, M Laga, P Lamptey. Control of STDs Handbook AIDSCAP, 1996

23
GA Dallabetta, M Laga, P Lamptey
GA Dallabetta, M Laga, P Lamptey. Control of STDs Handbook AIDSCAP, 1996

24
FIGURE Estimated incidence of gonorrhea in men who have sex with men (MSM) and in the remainder of the population, King County, Washington, The incidence in MSM is an underestimate, based on cases in men attending a public STD clinic who acknowledged sex with other men, plus reported cases of rectal gonococcal infection in men diagnosed in other clinical settings, and on an estimate that 42,500 MSM reside in King County. (Author’s unpublished data.) Estimated incidence of gonorrhea in men who have sex with men (MSM) and in the remainder of the population, King County, Washington,
 and in the remainder of the population, King County, Washington,")
25
Fig. 1. Increases in risky behavior and the usage of antiretroviral therapy. (a) Relationship between antiretroviral usage, increases in risky behavior (in both infected and uninfected individuals) and HIV incidence rates after 5 years of antiretroviral usage. HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug resistance strains) are plotted, the data points show the area in which the HIV incidence rates are stable. The green, pink and blue data show prevalence one, 5 and 10 years, respectively, after the introduction of antiretroviral treatment
 Relationship between antiretroviral usage, increases in risky behavior (in both infected and uninfected individuals) and HIV incidence rates after 5 years of antiretroviral usage. HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug resistance strains) are plotted, the data points show the area in which the HIV incidence rates are stable. The green, pink and blue data show prevalence one, 5 and 10 years, respectively, after the introduction of antiretroviral treatment.")
26
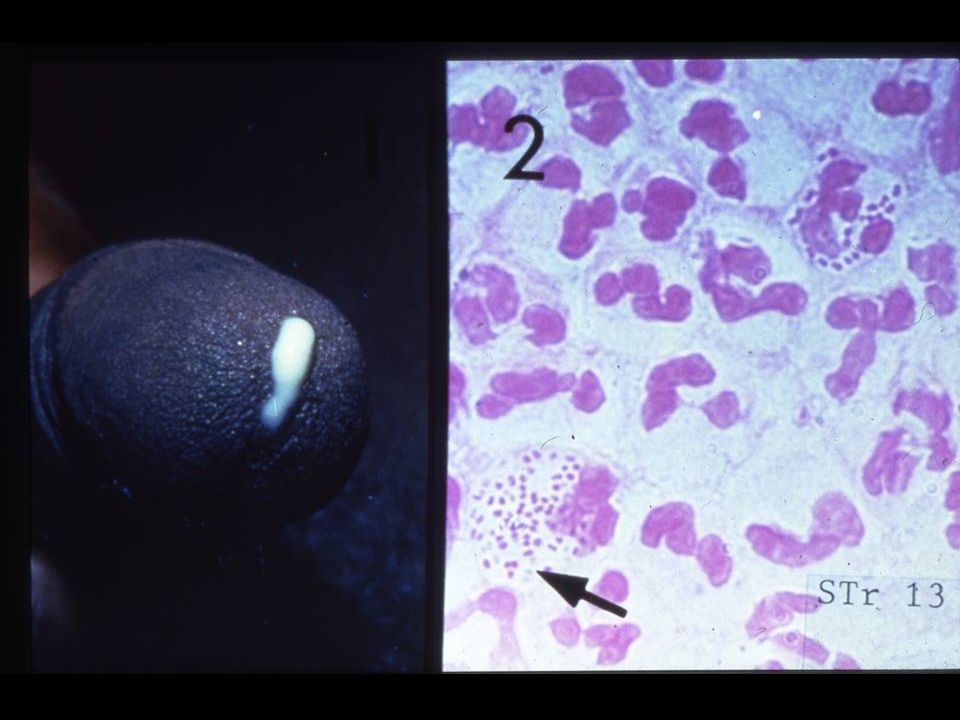
GONOCOCCIE Uréthrite aiguë chez l’homme
- incubation: 2-5 jours (jusquà 10 jours) écoulement et dysurie - écoulement séreux puis purulent en 1 jour - en général plus aigue que dans les uréthrites non gonococciques - avec certaines souches tableau discret ou asymptomatique 2. Infection urogénitale chez la femme: - 80% asymtomatique - incubation 10 jours - pertes vaginales, dysurie, saignements
 écoulement et dysurie. - écoulement séreux puis purulent en 1 jour. - en général plus aigue que dans les uréthrites non gonococciques. - avec certaines souches tableau discret ou asymptomatique. 2. Infection urogénitale chez la femme: - 80% asymtomatique. - incubation 10 jours. - pertes vaginales, dysurie, saignements.")
27
FIGURE 209-8. Incubation period in 44 men with gonococcal urethritis
FIGURE Incubation period in 44 men with gonococcal urethritis. (From Harrison WO, Hooper RR, Weisner PJ, et al. A trial of minocycline given after exposure to prevent gonorrhea. N Engl J Med 1979;300: ) Incubation period in 44 men with gonococcal urethritis. (From Harrison WO, Hooper RR, Weisner PJ, et al. N Engl J Med 1979;300: )
 Incubation period in 44 men with gonococcal urethritis. (From Harrison WO, Hooper RR, Weisner PJ, et al. N Engl J Med 1979;300: )")
30
FIGURE 209-9B. Gonococcal urethritis
FIGURE 209-9B. Gonococcal urethritis. A, Purulent exudates due to gonorrhea. B, Mucopurulent discharge mimicking the usual appearance of nongonococcal urethritis due to Chlamydia trachomatis and other pathogens.

31
FIGURE 209-9B. Gonococcal urethritis
FIGURE 209-9B. Gonococcal urethritis. A, Purulent exudates due to gonorrhea. B, Mucopurulent discharge mimicking the usual appearance of nongonococcal urethritis due to Chlamydia trachomatis and other pathogens.

32
GONOCOCCIE Uréthrite aiguë chez l’homme
- incubation: 2-5 jours (jusquà 10 jours) écoulement et dysurie - écoulement séreux puis purulent en 1 jour - en général plus aigue que dans les uréthrites non gonococciques - avec certaines souches tableau discret ou asymptomatique 2. Infection urogénitale chez la femme: - 80% asymtomatique - incubation 10 jours - pertes vaginales, dysurie, saignements
 écoulement et dysurie. - écoulement séreux puis purulent en 1 jour. - en général plus aigue que dans les uréthrites non gonococciques. - avec certaines souches tableau discret ou asymptomatique. 2. Infection urogénitale chez la femme: - 80% asymtomatique. - incubation 10 jours. - pertes vaginales, dysurie, saignements.")
33
FIGURE 209-10. Purulent endocervical exudate in gonococcal cervicitis
FIGURE Purulent endocervical exudate in gonococcal cervicitis. (From Handsfield HH. Color Atlas and Synopsis of Sexually Transmitted Diseases. 2nd ed. New York, McGraw-Hill, 2001; courtesy of King K. Holmes.)
")
37
GONOCOCCIE 4. Pharyngite
- plus efficacement par fellation > cunilingus > baisers (rares) - 3 à 7% des hommes hétéro avec uréthrite - 10 à 20% des femmes hétéro avec gonorrhée et > chez femmes enceintes - 10 à 25% des MSM avec gonorrhée - le plus souvent asymptomatique 5. Rectite - 40% chez femmes et MSM infectés - souvent seul site pour MSM - habituellement asymptomatique - proctite aiguë: prurit, tenesme, suppuration, saignement muqueux plus communs MSM
 - 3 à 7% des hommes hétéro avec uréthrite à 20% des femmes hétéro avec gonorrhée et > chez femmes enceintes à 25% des MSM avec gonorrhée. - le plus souvent asymptomatique. 5. Rectite. - 40% chez femmes et MSM infectés. - souvent seul site pour MSM. - habituellement asymptomatique. - proctite aiguë: prurit, tenesme, suppuration, saignement muqueux plus communs MSM.")
38
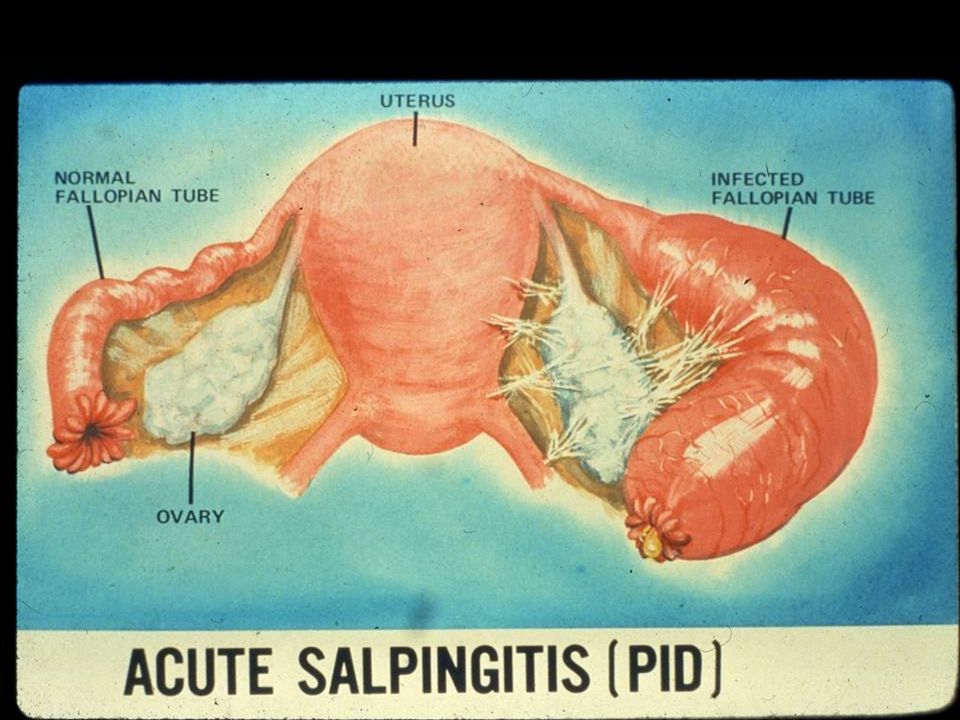
GONOCOCCIE 6. PID/salpyngite aiguë - 10 à 20% des femmes infectées
- infertilité 15-20% ou 20-80% si 1 ou plus de 3ème épisode 7. Périhépatite: - Syndrome de Fitz Hugh Curtis: extension de l’infection des trompes de fallope à la capsule hépatique et péritoine environnant (rares cas masculins par bactériémie) - souvent confoncues avc cholécystite ou hépatite virale - laparoscopie: adhérences péritonéales typiques en cordes de violon
 - souvent confoncues avc cholécystite ou hépatite virale. - laparoscopie: adhérences péritonéales typiques en cordes de violon.")
39
GONOCOCCIE 8. Infection disséminée - 0.5 à 3% des patients
- difficiles à différentier de méningococcémie - favorisée par déficit en Complément: 13% - Syndrome polyarthrite + dermatite (papules et pustules à composantes hémorrhagiques et parfois nécrotique, 75%) - Puis arthrites septiques, asymétriques - Répéter les hémoc au moins 3 fois - Devenues rares: endocardites (valve aortique) , méningites, ostéomyélites, choc septique
 - Puis arthrites septiques, asymétriques. - Répéter les hémoc au moins 3 fois. - Devenues rares: endocardites (valve aortique) , méningites, ostéomyélites, choc septique.")
40
FIGURE 209-12B. Cutaneous lesions in disseminated gonococcal infection
FIGURE B. Cutaneous lesions in disseminated gonococcal infection. A, Early papular lesions. B, Pustular lesion associated with subungual hemorrhage. C, Ulcerated pustular lesion.

41
FIGURE 209-12C. Cutaneous lesions in disseminated gonococcal infection
FIGURE C. Cutaneous lesions in disseminated gonococcal infection. A, Early papular lesions. B, Pustular lesion associated with subungual hemorrhage. C, Ulcerated pustular lesion.

42
FIGURE 209-12C. Cutaneous lesions in disseminated gonococcal infection
FIGURE C. Cutaneous lesions in disseminated gonococcal infection. A, Early papular lesions. B, Pustular lesion associated with subungual hemorrhage. C, Ulcerated pustular lesion.

43
Arthrite gonococcique chez un séropositif sans porte d’entrée retrouvée

44
Arthrite gonococcique chez un séropositif sans porte d’entrée retrouvée

45
Arthrite gonococcique chez un séropositif sans porte d’entrée retrouvée

47
GONOCOCCIE 9. Infection néonatale et pédiatrique
- Ophtalmie cause fréquente de cécité dans PVD - Prévenue par la prophylaxie de Crédé avec collyre au Nitrate d’argent - Extension systémique rare - Rares rectites - Répéter les hémoc au moins 3 fois - Devenues rares: endocardites (valve aortique) , méningites, ostéomyélites, choc septique
 , méningites, ostéomyélites, choc septique.")
48
FIGURE 209-11. Acute gonococcal conjunctivitis in an adult
FIGURE Acute gonococcal conjunctivitis in an adult. (From Handsfield HH. Color Atlas and Synopsis of Sexually Transmitted Diseases, 2nd ed. New York, McGraw-Hill, 2001.)
")
49
GONOCOCCIE: Diagnostic
Cultures: - Sensibilité = 95% prélèvement uréthral - Sensibilité = 80-90% prélèvement cervix - milieux sélectifs et non sélectifs pour cervix - meilleure technique pour rectum, pharynx - 5% des souches isolées sont des Neisseria meningitidis 2. Tests amplificateurs d’acides nucléiques (NAATs): plusieurs technologies (Gen-Probe, Amplicor, Probe Tec…). Ont remplacé les cultures pour les asymptomatiques (spécificité=99%, bonne sensibilité sur urines et autoprélèvements vaginaux)
: plusieurs technologies (Gen-Probe, Amplicor, Probe Tec…). Ont remplacé les cultures pour les asymptomatiques (spécificité=99%, bonne sensibilité sur urines et autoprélèvements vaginaux)")
50
GONOCOCCIE: Diagnostic
Examens directs: a- Bleu de méthylène: rapide et spécifique pour uréthrite masculines b- Gram: sensibilité = 95% prélèvements uréthraux masculins avec haute spécificité d- Gram: sensibilité = 50% pour rectum, cervix, pharynx et uréthrites masculines asymptomatiques 2. Elisa et Immunofluorescente directe: faible sensibilité et peu utilisés

52
FIGURE Gram-stained smear of urethral exudates showing intracellular gram-negative diplococci that is characteristic of gonorrhea.

53
(Urethre, endocol, rectum)
GONOCOCCIE (Urethre, endocol, rectum) Ciprofloxacin 500 mg orally in a single dose OR Ceftriaxone 125 mg IM in a single dose, Cefixime 400 mg orally in a single dose, Spectinomycin 2g IM x 1 (WHO,2004)
 Ciprofloxacin 500 mg orally in a single dose. OR. Ceftriaxone 125 mg IM in a single dose, Cefixime 400 mg orally in a single dose, Spectinomycin 2g IM x 1. (WHO,2004)")
54
(Urethre, endocol, rectum)
GONOCOCCIE (Urethre, endocol, rectum) Ceftriaxone 125 mg IM in a single dose, OR Cefixime 400 mg orally in a single dose, Ciprofloxacin 500 mg orally in a single dose Ofloxacin 400 mg orally in a single dose Levofloxacin 250 mg orally in a single dose + Tt anti-chlamydia Azithromycin 1 g orally in a single dose Doxycycline 100 mg orally twice a day for 7 days. (CDC,2006)
 Ceftriaxone 125 mg IM in a single dose, OR. Cefixime 400 mg orally in a single dose, Ciprofloxacin 500 mg orally in a single dose. Ofloxacin 400 mg orally in a single dose. Levofloxacin 250 mg orally in a single dose. + Tt anti-chlamydia. Azithromycin 1 g orally in a single dose. Doxycycline 100 mg orally twice a day for 7 days. (CDC,2006)")
55
GONOCOCCIE (alternatives)
(Urethre, endocol, rectum) Spectinomycine 2g IM x 1 Single-dose cephalosporin regimens (other than ceftriaxone 125 mg IM and cefixime 400 mg orally) include ceftizoxime (500 mg, administered IM), cefoxitin (2 g, administered IM with probenecid 1 g orally), and cefotaxime (500 mg, administered IM). Single-dose quinolone regimens include gatifloxacin 400 mg orally, norfloxacin 800 mg orally, and lomefloxacin 400 mg orally + Traitement anti-chlamydia x 7 jours (CDC,2006)
 Spectinomycine 2g IM x 1. Single-dose cephalosporin regimens (other than ceftriaxone 125 mg IM and cefixime 400 mg orally) include ceftizoxime (500 mg, administered IM), cefoxitin (2 g, administered IM with probenecid 1 g orally), and cefotaxime (500 mg, administered IM). Single-dose quinolone regimens include gatifloxacin 400 mg orally, norfloxacin 800 mg orally, and lomefloxacin 400 mg orally. + Traitement anti-chlamydia x 7 jours. (CDC,2006)")
56
GONOCOCCIE PHARYNGEE Ceftriaxone 125mg IM x 1
Ciprofloxacine 500mg p os x 1 + Tt anti-chlamydia si diagnostic non éliminé Azithromycin 1 g orally in a single dose OR Doxycycline 100 mg orally twice daily for 7 days. (CDC, 2006)
")
57
TABLE 209-2 Treatment of Uncomplicated Gonorrhea in Adults
*May be reconstituted in 1% lidocaine solution to minimize injection pain. †Ce.xime is the recommended cephalosporin for oral treatment, but availability has been intermittent in the United States. Limited data support the use of cefpodoxime as an oral alernative. ‡Fluoroquinolone-resistant strains of Neisseria gonorrhoeae are spreading in the United States, and widespread resistance may preclude routine use in the near future; see text. §Recommended only if both cephalosporins and .uoroquinolones are contraindicated; see text. ||Not effective against pharyngeal gonococcal infection. ¶Unnecessary if azithromycin, 2.0 g, is used for initial single-dose treatment. Modi.ed from Centers for Disease Control and Prevention. Sexually Transmitted Diseases Treatment Guidelines MMWR Morb Mortal Wkly Rep 2002;51(No. RR-6).
.")
58
TABLE 209-3 Recommended Treatment of Acute Pelvic Inflammatory Disease

59
TABLE 209-3 Recommended Treatment of Acute Pelvic Inflammatory Disease

60
Fig. 1. Increases in risky behavior and the usage of antiretroviral therapy. (a) Relationship between antiretroviral usage, increases in risky behavior (in both infected and uninfected individuals) and HIV incidence rates after 5 years of antiretroviral usage. HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug resistance strains) are plotted, the data points show the area in which the HIV incidence rates are stable. The green, pink and blue data show prevalence one, 5 and 10 years, respectively, after the introduction of antiretroviral treatment
 Relationship between antiretroviral usage, increases in risky behavior (in both infected and uninfected individuals) and HIV incidence rates after 5 years of antiretroviral usage. HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug resistance strains) are plotted, the data points show the area in which the HIV incidence rates are stable. The green, pink and blue data show prevalence one, 5 and 10 years, respectively, after the introduction of antiretroviral treatment.")
Présentations similaires












>")









