Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Études DICE : La maîtrise glycémique au Canada
Un patient atteint de diabète de type 2 sur deux au Canada n’atteint pas la valeur cible (< 7 %) Résultats de la mesure la plus récente du taux d’HbA1C (n = 2 337) HbA1C non maîtrisée 49 % HbA1C maîtrisée 51 % Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated. 1 DICE = Diabetes in Canada Evaluation Harris SB et al. Diabetes Res Clin Pract 2005; 70:90-7.
 Résultats de la mesure la plus récente du taux d’HbA1C (n = 2 337) HbA1C non maîtrisée 49 % HbA1C maîtrisée 51 % Summary: Combination Therapy With Sitagliptin Plus Metformin. Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated. 1. DICE = Diabetes in Canada Evaluation. Harris SB et al. Diabetes Res Clin Pract 2005; 70:90-7.")
2
Lignes directrices de pratique clinique 2008 de l’ACD
Évaluation clinique - Interventions liées au mode de vie (instauration du traitement nutritionnel et d’un programme d’activité physique) HbA1c < 9,0 % HbA1c ≥ 9,0 % Hyperglycémie symptomatique et décompensation métabolique Instauration immédiate de la pharmacothérapie sans attendre les bienfaits des interventions liées au mode de vie : Envisager d’instaurer le traitement à la metformine en association avec un agent d’une autre classe ou instaurer le traitement à l’insuline Instauration du traitement à l’insuline ± la metformine Instauration du traitement à la metformine Si les valeurs cibles ne sont pas atteintes Ajout d’un agent selon les caractéristiques du patient : Inhibiteur de l’alphaglucosidase Agents agissant sur les incrétines : Inhibiteur de la DPP-4 Insuline Sécrétagogue de l’insuline : Meglitinide, sulfonylurée Thiazolidinédione Agent amaigrissant Si les valeurs cibles ne sont pas atteintes : Ajout d’un médicament d’une autre classe ou Ajout d’insuline basale au coucher aux autres agents ou Intensification de l’insulinothérapie Lignes directrices de pratique clinique 2008 pour la prévention et la prise en charge du diabète au Canada
 HbA1c < 9,0 % HbA1c ≥ 9,0 % Hyperglycémie symptomatique et décompensation métabolique. Instauration immédiate de la pharmacothérapie sans attendre les bienfaits des interventions liées au mode de vie : Envisager d’instaurer le traitement à la metformine en association avec un agent d’une autre classe ou instaurer le traitement à l’insuline. Instauration du traitement à l’insuline ± la metformine. Instauration du traitement à la metformine. Si les valeurs cibles ne sont pas atteintes. Ajout d’un agent selon les caractéristiques du patient : Inhibiteur de l’alphaglucosidase. Agents agissant sur les incrétines : Inhibiteur de la DPP-4. Insuline. Sécrétagogue de l’insuline : Meglitinide, sulfonylurée. Thiazolidinédione. Agent amaigrissant. Si les valeurs cibles ne sont pas atteintes : Ajout d’un médicament d’une autre classe ou. Ajout d’insuline basale au coucher aux autres agents ou. Intensification de l’insulinothérapie. Lignes directrices de pratique clinique 2008 pour la prévention et la prise en charge du diabète au Canada.")
3
L’association sitagliptine-metformine agit sur trois grandes anomalies associées au diabète de type 2 de manière complémentaire La sitagliptine améliore la fonction des cellules bêta et augmente la synthèse et la libération de l’insuline. La metformine possède des propriétés qui augmentent la sensibilité à l’insuline. Dysfonction-nement des cellules bêta Insulino-résistance The Combination of Sitagliptin and Metformin Addresses the 3 Core Defects of Type 2 Diabetes in a Complementary Manner Speaker Notes The combination of sitagliptin and metformin improves glycemic control via complementary MOAs. [Build 1] Mechanism of action of sitagliptin: Sitagliptin improves beta-cell function1 and increases insulin synthesis and release. Sitagliptin indirectly reduces hepatic glucose overproduction through suppression of glucagon from alpha cells. [Build 2] Mechanism of action of metformin: Metformin increases insulin sensitivity by decreasing release of free fatty acids from fat to muscle and liver2 and by increasing insulin receptor activity in muscle.3 By increasing insulin sensitivity, metformin increases glucose uptake and utilization in muscle and fat.3,4 Metformin decreases hepatic glucose overproduction by directly targeting the liver to decrease gluconeogenesis and glycogenolysis.3 [Build 3] In combination, these agents help to improve glycemic control as a result of their complementary MOAs. Sitagliptin addresses beta-cell dysfunction, metformin addresses insulin resistance, and both sitagliptin and metformin address glucose overproduction but in different, complementary ways.1,3 La metformine réduit la surproduction de glucose par le foie par une réduction de la gluconéogenèse et de la glycogénolyse hépatiques. La sitagliptine réduit la surproduction de glucose par le foie en supprimant le glucagon des cellules alpha. Surproduction de glucose par le foie *Se référer aux notes correspondantes du conférencier pour les références.

4
Initial Combination Therapy With Sitagliptin Plus Metformin
24-week phase1 with 30-week continuation phase2 50-week extension study 3 Patients with T2DM not on therapy or on mono- or low-dose combo-OHA Sitagliptin 100 mg qd Eligible if HbA1c 7.5%–11% Metformin 500 mg bid Diet and exercise run-in period Single-blind placebo run-in period Initial Combination Therapy With Sitagliptin Plus Metformin This was a multinational, randomized, double-blind, placebo-controlled study. The primary end point of this study was HbA1c at 24 weeks. At screening1: Patients whose HbA1c ranged from 7.5% to 11% and who were not taking an oral antihyperglycemic agent (OHA) for ≥8 weeks were eligible to directly enter a 2-week, single-blind, placebo run-in period. Patients whose HbA1c was >11% and who were not taking an OHA entered a diet and exercise run-in period of up to 6 weeks. Patients who were taking an OHA and whose HbA1c ranged from 7% to 10.5% discontinued the agent and entered a washout period of 6 to 10 weeks (8–12 weeks for those taking thiazolidinediones). After the run-in period, patients whose HbA1c ranged from 7.5% to 11% entered a 2-week, single-blind, placebo run-in period. All patients with adequate compliance during the placebo run-in period were randomly assigned to 1 of 6 treatment regimens for 24 weeks.1 The continuation phase was a total of 30 weeks. Patients assigned to placebo in the 24-week phase were switched in a blinded manner to metformin 1,000 mg bid.2 Patients who completed both the 24-week and the 30-week phases and complied with all enrollment criteria were asked if they were willing to participate in a 50-week, factorial, parallel-group extension study. Treatment regimens were consistent with the 30-week continuation phase. Rescue criteria for the continuation phase and extension study were stricter than in the first 24-weeks. Patients whose HbA1c was >8% during the continuation phase were given rescue therapy. Patients whose HbA1c was >7.5% during the extension study were given rescue therapy (open-label glyburide or glibenclamide). Those who were unable to take rescue therapy were discontinued.3 There were no hypotheses associated with this extension study.3 Metformin 1,000 mg bid Screening period R Sitagliptin 50 mg bid + metformin 500 mg bid Sitagliptin 50 mg bid + metformin 1,000 mg bid If on OHA, discontinue therapy Placebo Metformin 1,000 mg bid 6–12 weeks Week –2 Day 1 Week 24 Week 54 Week 104 FPG criteria to week 24 HbA1c >8% to week 54 HbA1c >7.5% to week 104 Glycemic rescue criteria bid=twice a day; FPG=fasting plasma glucose; OHA=oral antihyperglycemic agent; qd=once a day; R=randomization; T2DM=type 2 diabetes mellitus. 1. Goldstein B et al. Diabetes Care. 2007;30(8):1979– Williams-Herman D, et al. Curr Med Res Opin. 2009;25(3):569– Data on file, MSD.
 for ≥8 weeks were eligible to directly enter a 2-week, single-blind, placebo run-in period. Patients whose HbA1c was >11% and who were not taking an OHA entered a diet and exercise run-in period of up to 6 weeks. Patients who were taking an OHA and whose HbA1c ranged from 7% to 10.5% discontinued the agent and entered a washout period of 6 to 10 weeks (8–12 weeks for those taking thiazolidinediones). After the run-in period, patients whose HbA1c ranged from 7.5% to 11% entered a 2-week, single-blind, placebo run-in period. All patients with adequate compliance during the placebo run-in period were randomly assigned to 1 of 6 treatment regimens for 24 weeks.1. The continuation phase was a total of 30 weeks. Patients assigned to placebo in the 24-week phase were switched in a blinded manner to metformin 1,000 mg bid.2. Patients who completed both the 24-week and the 30-week phases and complied with all enrollment criteria were asked if they were willing to participate in a 50-week, factorial, parallel-group extension study. Treatment regimens were consistent with the 30-week continuation phase. Rescue criteria for the continuation phase and extension study were stricter than in the first 24-weeks. Patients whose HbA1c was >8% during the continuation phase were given rescue therapy. Patients whose HbA1c was >7.5% during the extension study were given rescue therapy (open-label glyburide or glibenclamide). Those who were unable to take rescue therapy were discontinued.3 There were no hypotheses associated with this extension study.3. Metformin 1,000 mg bid. Screening period. R. Sitagliptin 50 mg bid + metformin 500 mg bid. Sitagliptin 50 mg bid + metformin 1,000 mg bid. If on OHA, discontinue therapy. Placebo. Metformin 1,000 mg bid. 6–12 weeks. Week –2. Day 1. Week 24. Week 54. Week 104. FPG criteria. to week 24. HbA1c >8% to week 54. HbA1c >7.5% to week 104. Glycemic rescue criteria. bid=twice a day; FPG=fasting plasma glucose; OHA=oral antihyperglycemic agent; qd=once a day; R=randomization; T2DM=type 2 diabetes mellitus. 1. Goldstein B et al. Diabetes Care. 2007;30(8):1979– Williams-Herman D, et al. Curr Med Res Opin. 2009;25(3):569– Data on file, MSD.")
5
Mean Change From Baseline, %
Initial Combination Therapy With Sitagliptin Plus Metformin Study: HbA1c Results by Baseline HbA1c at 54 Weeks Continuation All-Patients-Treated Population Baseline HbA1c <8 Mean 7.6%, n=172 8 to <9 Mean 8.4%, n=244 9 to <10 Mean 9.4%, n=163 ≥10 Mean 10.4%, n=78 n= 28 32 40 39 33 n= 43 39 53 49 60 n= 19 30 33 38 43 n= 16 8 21 17 –0.5 –0.5 Initial Combination Therapy With Sitagliptin Plus Metformin Study: HbA1c Results by Baseline HbA1c at 54 Weeks Mean reductions from baseline HbA1c were generally greater for patients with higher baseline HbA1c values.1 This 54-week study (a 24-week, double-blind, placebo-controlled period [Phase A] followed by an additional active-controlled 30-week continuation phase [Phase B]) evaluated the efficacy of the coadministration of sitagliptin and metformin, sitagliptin monotherapy, or metformin monotherapy.1 In a subgroup analysis, the study evaluated patients grouped by baseline HbA1c: those with HbA1c levels <8% (n=172), HbA1c levels ≥8% to <9% (n=244), HbA1c levels ≥9% to <10% (n=163), and HbA1c levels ≥10% (n=78).1 –1.0 –1.0 –1.5 –1.5 Mean Change From Baseline, % –2.0 –2.0 –2.5 –2.5 –3.0 –3.0 –3.5 –3.5 Sitagliptin 100 mg qd Metformin 500 mg bid Metformin 1000 mg bid Sitagliptin 50 mg + metformin 500 mg bid Sitagliptin 50 mg + metformin 1000 mg bid Williams-Herman D et al. Curr Med Res Opin. 2009;25(3):569–583.
 evaluated the efficacy of the coadministration of sitagliptin and metformin, sitagliptin monotherapy, or metformin monotherapy.1. In a subgroup analysis, the study evaluated patients grouped by baseline HbA1c: those with HbA1c levels <8% (n=172), HbA1c levels ≥8% to <9% (n=244), HbA1c levels ≥9% to <10% (n=163), and HbA1c levels ≥10% (n=78).1. –1.0. –1.0. –1.5. –1.5. Mean Change From Baseline, % –2.0. –2.0. –2.5. –2.5. –3.0. –3.0. –3.5. –3.5. Sitagliptin 100 mg qd. Metformin 500 mg bid. Metformin 1000 mg bid. Sitagliptin 50 mg + metformin 500 mg bid. Sitagliptin 50 mg + metformin 1000 mg bid. Williams-Herman D et al. Curr Med Res Opin. 2009;25(3):569–583.")
6
Initial Combination Therapy With Sitagliptin Plus Metformin Study: Mean HbA1c Levels Through 54 Weeks (APT) Continuation All-Patients-Treated Population 9.0 24-Week (Phase A) Continuation Phase (Phase B) 8.5 8.0 HbA1c, % 7.5 Initial Combination Therapy With Sitagliptin Plus Metformin: Mean HbA1c Levels Through 54 Weeks (APT) Note: The data presented on this slide (Phase B) are associated with the 24-week (Phase A) study shown on the previous slides. This 54-week study (a 24-week, double-blind, placebo-controlled period [Phase A] followed by an additional active-controlled 30-week continuation phase [Phase B]) evaluated the efficacy of the coadministration of sitagliptin and metformin, sitagliptin monotherapy, or metformin monotherapy. Patients in the placebo group in Phase A were switched to high-dose metformin in Phase B.1 This slide shows the change from baseline in HbA1c through week 54 of the APT population. The coadministration of sitagliptin and metformin resulted in a substantial reduction in HbA1c over the course of 54 weeks.1 Over the course of 54 weeks, combination therapy of sitagliptin with metformin provided a greater decrease in HbA1c than either monotherapy alone.1 7.0 6.5 6.0 6 12 18 24 30 38 46 54 Weeks Continuation (Phase B) APT Population Sita 100 mg qd (n=106) Met 500 mg bid (n=117) Met 1000 mg bid (n=134) Sita 50 mg + met 500 mg bid (n=147) APT=all-patients-treated; sita=sitagliptin; met=metformin. Values represent LSM±SE. Williams-Herman D et al. Curr Med Res Opin. 2009;25(3):569–583. Sita 50 mg + met 1000 mg bid (n=153)
 Continuation Phase (Phase B) HbA1c, % 7.5. Initial Combination Therapy With Sitagliptin Plus Metformin: Mean HbA1c Levels Through 54 Weeks (APT) Note: The data presented on this slide (Phase B) are associated with the 24-week (Phase A) study shown on the previous slides. This 54-week study (a 24-week, double-blind, placebo-controlled period [Phase A] followed by an additional active-controlled 30-week continuation phase [Phase B]) evaluated the efficacy of the coadministration of sitagliptin and metformin, sitagliptin monotherapy, or metformin monotherapy. Patients in the placebo group in Phase A were switched to high-dose metformin in Phase B.1. This slide shows the change from baseline in HbA1c through week 54 of the APT population. The coadministration of sitagliptin and metformin resulted in a substantial reduction in HbA1c over the course of 54 weeks.1. Over the course of 54 weeks, combination therapy of sitagliptin with metformin provided a greater decrease in HbA1c than either monotherapy alone Weeks. Continuation (Phase B) APT Population. Sita 100 mg qd (n=106) Met 500 mg bid (n=117) Met 1000 mg bid (n=134) Sita 50 mg + met 500 mg bid (n=147) APT=all-patients-treated; sita=sitagliptin; met=metformin. Values represent LSM±SE. Williams-Herman D et al. Curr Med Res Opin. 2009;25(3):569–583. Sita 50 mg + met 1000 mg bid (n=153)")
7
Initial Combination Therapy With Sitagliptin Plus Metformin Study: HbA1c Results at 104 Weeks (Extension Study) APT Population (Extension Study) Sitagliptin 100 mg qd (n=50) Sitagliptin 50 mg bid + metformin 500 mg bid (n=96) Metformin 500 mg bid (n=64) Sitagliptin 50 mg bid + metformin 1,000 mg bid (n=105) Metformin 1,000 mg bid (n=87) 24-week phase Continuation phase Extension Study 9.0 Initial Combination Therapy With Sitagliptin Plus Metformin Study: HbA1c Results at 104 Weeks (Extension Study) This slide demonstrates that after initial therapy with sitagliptin plus metformin, the HbA1c change from baseline was generally greater than that achieved with either agent alone.1 This all-patients-treateda analysis (extension study) included patients with a baseline measurement and at least 1 measurement in the extension study.1 Initial combination therapy or maintenance of combination therapy may not be appropriate for all patients. These management options should be left to the discretion of the health care provider. aResults include only randomized patients who agreed to enter the extension study, had not received glycemic rescue therapy through week 54, took at least 1 dose of study medication after week 54, and had at least 1 post-54-week HbA1c measurement. Mean baseline A1C = 8.5%–8.7% 8.5 8.0 –1.1 a LSM HbA1c Change From Baseline, % 7.5 a –1.1 –1.3 7.0 –1.4 6.5 –1.7 6.0 6 12 18 24 30 38 46 54 62 70 78 91 104 Weeks APT=all-patients-treated; bid=twice a day; LSM=least-squares mean; qd=daily. aValues represented are rounded. Actual values are 1.15 for sitagliptin 100 mg qd and 1.06 for metformin 500 mg bid. Data on file, MSD.
 Sitagliptin 100 mg qd (n=50) Sitagliptin 50 mg bid + metformin 500 mg bid (n=96) Metformin 500 mg bid (n=64) Sitagliptin 50 mg bid + metformin 1,000 mg bid (n=105) Metformin 1,000 mg bid (n=87) 24-week phase. Continuation phase. Extension Study Initial Combination Therapy With Sitagliptin Plus Metformin Study: HbA1c Results at 104 Weeks (Extension Study) This slide demonstrates that after initial therapy with sitagliptin plus metformin, the HbA1c change from baseline was generally greater than that achieved with either agent alone.1. This all-patients-treateda analysis (extension study) included patients with a baseline measurement and at least 1 measurement in the extension study.1. Initial combination therapy or maintenance of combination therapy may not be appropriate for all patients. These management options should be left to the discretion of the health care provider. aResults include only randomized patients who agreed to enter the extension study, had not received glycemic rescue therapy through week 54, took at least 1 dose of study medication after week 54, and had at least 1 post-54-week HbA1c measurement. Mean baseline A1C = 8.5%–8.7% –1.1. a. LSM HbA1c Change From Baseline, % 7.5. a. –1.1. – – – Weeks. APT=all-patients-treated; bid=twice a day; LSM=least-squares mean; qd=daily. aValues represented are rounded. Actual values are 1.15 for sitagliptin 100 mg qd and 1.06 for metformin 500 mg bid. Data on file, MSD.")
8
Taux d’HbA1c moyen de départ : 8,5 % à 8,7 %
Traitement d’association initial sitagliptine + metformine : après 54 semaines, jusqu’à 67 % et 77 % des patients avaient atteint l’objectif (HbA1c < 7 %) Sitagliptine 100 mg/jour Metformine 500 mg 2 f.p.j. Metformine mg 2 f.p.j. Sitagliptine 50 mg + metformine 500 mg 2 f.p.j. Sitagliptine 50 mg + metformine mg 2 f.p.j. 90 80 70 60 50 40 30 20 10 Taux d’HbA1c moyen de départ : 8,5 % à 8,7 % 77 % En plus de la phase de 24 semaines menée à double insu et avec un témoin placebo, l’étude comprenait également une phase de prolongation de 30 semaines avec un témoin actif, ce qui portait à 54 semaines la période d’observation totale. Dans le graphique à gauche de la diapositive, on voit les résultats de la phase de continuation pour tous les patients traités (TPT), c’est-à-dire tous les patients dont l’HbA1c avait été mesurée au début de l’étude et au moins une fois pendant la phase avec un témoin actif. Dans cette population de patients, 67 % ont reçu la dose plus forte de la combinaison sitagliptine + metformine et ils ont atteint leur objectif visé pour le taux d’HbA1c, soit < 7 %. Parmi les patients qui ont terminé l’étude, les taux de succès ont été plus élevés, plus des trois quarts des patients traités par la combinaison à doses fortes ayant atteint l’objectif pour l’ HbA1c. Référence : Williams-Herman D, Johnson J, Teng R, et coll. Efficacy and safety of initial combination therapy with sitagliptin and metformin in patients with type 2 diabetes: a 54-week study. Curr Med Res Opin 2009; 25(3): 67 % 63 % 57 % Patients (%) 48 % 44 % 41 % 35 % 25 % 23 % n = 106 117 134 147 153 58 77 101 106 124 Continuation Tous les patients traités (TPT) Patients ayant terminé l’étude Williams-Herman D, et coll. Curr Med Res Opin 2009; 25(3):
 Sitagliptine 100 mg/jour. Metformine 500 mg 2 f.p.j. Metformine mg 2 f.p.j. Sitagliptine 50 mg + metformine 500 mg 2 f.p.j. Sitagliptine 50 mg + metformine mg 2 f.p.j Taux d’HbA1c moyen de départ : 8,5 % à 8,7 % 77 % En plus de la phase de 24 semaines menée à double insu et avec un témoin placebo, l’étude comprenait également une phase de prolongation de 30 semaines avec un témoin actif, ce qui portait à 54 semaines la période d’observation totale. Dans le graphique à gauche de la diapositive, on voit les résultats de la phase de continuation pour tous les patients traités (TPT), c’est-à-dire tous les patients dont l’HbA1c avait été mesurée au début de l’étude et au moins une fois pendant la phase avec un témoin actif. Dans cette population de patients, 67 % ont reçu la dose plus forte de la combinaison sitagliptine + metformine et ils ont atteint leur objectif visé pour le taux d’HbA1c, soit < 7 %. Parmi les patients qui ont terminé l’étude, les taux de succès ont été plus élevés, plus des trois quarts des patients traités par la combinaison à doses fortes ayant atteint l’objectif pour l’ HbA1c. Référence : Williams-Herman D, Johnson J, Teng R, et coll. Efficacy and safety of initial combination therapy with sitagliptin and metformin in patients with type 2 diabetes: a 54-week study. Curr Med Res Opin 2009; 25(3): % 63 % 57 % Patients (%) 48 % 44 % 41 % 35 % 25 % 23 % n = Continuation Tous les patients traités (TPT) Patients ayant terminé l’étude. Williams-Herman D, et coll. Curr Med Res Opin 2009; 25(3):")
9
Sitagliptine + metformine vs sulfonylurée + metformine : Comparaison des effets sur le poids et l’hypoglycémie Tous les patients (analyse IDT) Variation de la MMC du poids initial Hypoglycémie Sulfonyluréea + metformine (n = 416) Sulfonyluréea + metformine (n = 584) 3 Sitagliptineb + metformine (n = 389) Sitagliptineb + metformine (n = 588) 50 2 40 À gauche, la figure illustre la variation du poids corporel observée pendant les 52 semaines de l’étude. La combinaison metformine + sitagliptine a été liée à une perte de poids moyenne de 1,5 kg, tandis que l’association metformine + glipizide a entraîné une hausse moyenne du poids de 1,1 kg. À droite, la figure décrit la proportion de patients qui ont manifesté au moins un épisode d’hypoglycémie pendant l’étude. Environ le tiers des patients traités par la combinaison metformine + glipizide ont manifesté une hypoglycémie, comparativement à 5 % dans le groupe ayant reçu la combinaison metformine + sitagliptine. Les taux de maîtrise de la glycémie ont été semblables dans le cas des deux combinaisons médicamenteuses. Référence : Nauck MA, Meininger G, Sheng D, et coll. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, double-blind, non-inferiority trial. Diabetes Obes Metab 2007; 9: 1 p < 0,001 p < 0,001 30 32 % Δ Entre les groupes à la semaine 52 = -2,5 kg Patients ayant eu ≥ 1 épisode sur 52 semaines (%) Poids corporel (kg ± ÉT) 20 −1 10 −2 5 % −3 12 24 38 52 Semaine 52 Semaines aC’est-à-dire le glipizide à la dose de 20 mg/jour ou moins. bSitagliptine (100 mg/jour) en association avec la metformine (1 500 mg/jour ou plus). Adapté de : Nauck MA, et coll. Diabetes Obes Metab 2007; 9:
 Variation de la MMC du poids initial. Hypoglycémie. Sulfonyluréea + metformine (n = 416) Sulfonyluréea + metformine (n = 584) 3. Sitagliptineb + metformine (n = 389) Sitagliptineb + metformine (n = 588) À gauche, la figure illustre la variation du poids corporel observée pendant les 52 semaines de l’étude. La combinaison metformine + sitagliptine a été liée à une perte de poids moyenne de 1,5 kg, tandis que l’association metformine + glipizide a entraîné une hausse moyenne du poids de 1,1 kg. À droite, la figure décrit la proportion de patients qui ont manifesté au moins un épisode d’hypoglycémie pendant l’étude. Environ le tiers des patients traités par la combinaison metformine + glipizide ont manifesté une hypoglycémie, comparativement à 5 % dans le groupe ayant reçu la combinaison metformine + sitagliptine. Les taux de maîtrise de la glycémie ont été semblables dans le cas des deux combinaisons médicamenteuses. Référence : Nauck MA, Meininger G, Sheng D, et coll. Efficacy and safety of the dipeptidyl peptidase-4 inhibitor, sitagliptin, compared with the sulfonylurea, glipizide, in patients with type 2 diabetes inadequately controlled on metformin alone: a randomized, double-blind, non-inferiority trial. Diabetes Obes Metab 2007; 9: p < 0,001. p < 0, % Δ Entre les groupes à la semaine 52 = -2,5 kg. Patients ayant eu ≥ 1 épisode sur 52 semaines (%) Poids corporel (kg ± ÉT) 20. − −2. 5 % − Semaine 52. Semaines. aC’est-à-dire le glipizide à la dose de 20 mg/jour ou moins. bSitagliptine (100 mg/jour) en association avec la metformine (1 500 mg/jour ou plus). Adapté de : Nauck MA, et coll. Diabetes Obes Metab 2007; 9:")
10
Pendant cette étude menée auprès de patients atteints de diabète de type 2,
l’adhésion au traitement par des antidiabétiques oraux a été évaluée par une analyse rétrospective des réclamations pharmaceutiques. Le taux d’adhésion était calculé comme suit : total du nombre de jours de réserve du médicament antidiabétique oral obtenu par le patient pendant la période de suivi, divisé par le nombre total de jours de la période de suivi désignée (180 jours). Chez les patients qui avaient été traités par le glyburide ou la metformine en monothérapie qui ont eu besoin de l’ajout d’un autre agent, c’est-à-dire d’un traitement d’association, les taux d’adhésion au traitement ont été significativement moins élevés (54 %; IC de 95 % 0,52-0,55) que dans le groupe des 105 patients qui sont passés au traitement par une combinaison à doses fixes (77 %; IC de 95 % 0,72-0,82). Référence : Melikian C, White TJ, Vanderplas A, et coll. Adherence to oral antidiabetic therapy in a managed care organization: a comparison of monotherapy, combination therapy, and fixed-dose combination therapy. Clin Ther 2002; 24(3):460-7.
. Chez les patients qui avaient été traités par le glyburide ou la. metformine en monothérapie qui ont eu besoin de l’ajout d’un autre agent, c’est-à-dire d’un traitement d’association, les taux d’adhésion au traitement ont. été significativement moins élevés (54 %; IC de 95 % 0,52-0,55) que dans le. groupe des 105 patients qui sont passés au traitement par une combinaison à. doses fixes (77 %; IC de 95 % 0,72-0,82). Référence : Melikian C, White TJ, Vanderplas A, et coll. Adherence to oral antidiabetic. therapy in a managed care organization: a comparison of monotherapy, combination therapy, and fixed-dose combination therapy. Clin Ther 2002; 24(3):")
11
Les effets indésirables gastro-intestinaux sont ceux qu’on observe le plus souvent
pendant une monothérapie par la metformine. Cette analyse montre que la combinaison sitagliptine + metformine a été reliée à un risque significativement moins élevé de diarrhée et de douleur abdominale, comparativement à la metformine en monothérapie; il n’y a pas eu de différence significative de l’incidence des nausées ou des vomissements. Selon des résultats de cette même analyse, le traitement initial par la combinaison sitagliptine + metformine a procuré des baisses plus marquées de la glycémie et aidé un plus grand nombre de patients à atteindre leur objectif pour l’HbA1c, comparativement à la monothérapie par la metformine. À la semaine 18, les réductions du taux moyen d’HbA1c, comparativement à la valeur de départ, étaient de -2,4 % dans le groupe recevant le traitement d’association et de -1,8 % dans le groupe sous monothérapie par la metformine (p < 0,001). Au total, 49 % des sujets du groupe recevant le traitement d’association ont atteint l’objectif pour l’HbA1c < 7 %, comparativement à 34 % des sujets du groupe traité seulement par la metformine (p < 0,001). Référence : Reasner C, Olansky L, Seck TL, et coll. Initial Therapy with the Fixed-Dose Combination (FDC) of Sitagliptin and Metformin (JANUMET™) in Patients with Type 2 Diabetes Mellitus Provides Superior Glycemic Control and Hemoglobin A1c Goal Attainment with Lower Rates of Abdominal Pain and Diarrhea versus Metformin Alone. Affiche présentée aux 69e Réunions scientifiques de l’American Diabetes Association, 5 au 9 juin Résumé no 610-P.
. Au total, 49 % des sujets du. groupe recevant le traitement d’association ont atteint l’objectif pour l’HbA1c < 7 %, comparativement à 34 % des sujets du groupe traité seulement par la metformine (p. < 0,001). Référence : Reasner C, Olansky L, Seck TL, et coll. Initial Therapy with the Fixed-Dose. Combination (FDC) of Sitagliptin and Metformin (JANUMET™) in Patients with Type. 2 Diabetes Mellitus Provides Superior Glycemic Control and Hemoglobin A1c Goal. Attainment with Lower Rates of Abdominal Pain and Diarrhea versus Metformin. Alone. Affiche présentée aux 69e Réunions scientifiques de l’American Diabetes. Association, 5 au 9 juin Résumé no 610-P.")
12
Efficacité des inhibiteurs de la DPP-4 en monothérapie
Variation moyenne, corrigée en fonction du placebo, des taux d’A1C par rapport au début Linagliptine1* 5 mg/jour 8,1 % 8,0 % Saxagliptine2 ≥ 7 % à ≤ 10 % Sitagliptine3* 100 mg/jour Posologie Taux d’A1C initial n=229 p<0,0001† n=193 n=103 n=69 p=0,0059† n=272 n=147 En tant que classe thérapeutique, les inhibiteurs de la DPP-4 comprennent divers groupes de composés qui peuvent en somme être répartis en agents mimétiques de la structure dipeptidique des substrats de la DPP-4, et en agents non-peptidomimétiques. La sitagliptine et la saxagliptine, qui sont des inhibiteurs à base de nitrile, appartiennent à la première classe, alors que la linagliptine (à base de xanthine) appartient à la seconde. Dans le cadre d’essais étudiant la monothérapie par chacun de ces agents, les trois inhibiteurs de la DPP-4 ont produit des réductions semblables du taux d’A1C (allant de 0,4-0,8 %), avec des valeurs initiales équivalentes du taux d’A1C. Références : Renseignements d’ordonnance des États-Unis sur la linagliptine, la saxagliptine, la sitagliptine. Monographie canadienne des produits suivants : linagliptine, saxagliptine et sitagliptine *18 semaines de traitement, 24 semaines autrement † Différence entre les groupes par rapport au placebo 1– 3, Renseignements d’ordonnance des États-Unis sur la linagliptine, la saxagliptine, la sitagliptine 38
 appartient à la seconde. Dans le cadre d’essais étudiant la monothérapie par chacun de ces agents, les trois inhibiteurs de la DPP-4 ont produit des réductions semblables du taux d’A1C (allant de 0,4-0,8 %), avec des valeurs initiales équivalentes du taux d’A1C. Références : Renseignements d’ordonnance des États-Unis sur la linagliptine, la saxagliptine, la sitagliptine. Monographie canadienne des produits suivants : linagliptine, saxagliptine et sitagliptine. *18 semaines de traitement, 24 semaines autrement. † Différence entre les groupes par rapport au placebo 1– 3, Renseignements d’ordonnance des États-Unis sur la linagliptine, la saxagliptine, la sitagliptine. 38.")
13
Pharmacokenetics of Dipeptidyl peptidase-4 inhibitors
European label advise physicians the need for dose adjustment with saxagliptin for patients use drug metabolized by CYT 450 3A4/5 Hocher/Reichetzeder/Alter: Renal & Cardiac effects o DDP4 Ref: KidneyBlood Press Res 2012:36:65-84

14
Dipeptidyl peptidase-4 inhibitors and cardiovascular risk: a meta-analysis of randomized clinical trials Aims: Preliminary data from randomized 70 trials including with metabolic outcomes have shown that treatment with DPP4i could be associated with a reduced incidence of major cardiovascular events (MACE). The present meta-analysis is aimed at verifying this protective effect, collecting all available data from randomized trials. patients with a mean follow-up of 44.1 weeks. Ref: Diabetes, Obesity and Metabolism 15: 112–120, 2013. original article © 2012 Blackwell Publishing Ltd
. The present meta-analysis is aimed at verifying this protective effect, collecting all available data from randomized trials patients with a mean follow-up of 44.1 weeks. Ref: Diabetes, Obesity and Metabolism 15: 112–120, original article © 2012 Blackwell Publishing Ltd.")
15
Dipeptidyl peptidase-4 inhibitors and cardiovascular risk: a meta-analysis of randomized clinical trials Results: TheMH–OR (95% Confidence Interval) was 0.71[0.59;0.86], 0.64[0.44;0.94], 0.77[0.48;1.24] and 0.60[0.41;0.88] for MACE, myocardial infarction, stroke and mortality, respectively. Conclusions: Treatment with DPP4i reduces the risk of cardiovascular events (particularly myocardial infarction) and all-cause mortality in patients with type 2 diabetes. The reduction in the incidence of myocardial infarction is greater than what predicted on the basis of conventional risk factors, suggesting a role for other mechanisms. Ref: Diabetes, Obesity and Metabolism 15: 112–120, 2013. original article © 2012 Blackwell Publishing Ltd
 was 0.71[0.59;0.86], 0.64[0.44;0.94], 0.77[0.48;1.24] and 0.60[0.41;0.88] for MACE, myocardial infarction, stroke and mortality, respectively. Conclusions: Treatment with DPP4i reduces the risk of cardiovascular events (particularly myocardial infarction) and all-cause mortality in patients with type 2 diabetes. The reduction in the incidence of myocardial infarction is greater than what predicted on the basis of conventional risk factors, suggesting a role for other mechanisms. Ref: Diabetes, Obesity and Metabolism 15: 112–120, original article © 2012 Blackwell Publishing Ltd.")
16
Est-ce qu’il des risques cardiovasculaire avec DPPP4?
Méta-analyse patients, 53 études Sitagliptine, saxagliptine, linagliptine, alogliptine, dutogliptine et vildagliptine 257 avec évènement CV RR 0.69 (0.006) Réduction 31% favorable au DPP4 Dr Lamana EASD,Lisbonne sept 2011 Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated.
 Réduction 31% favorable au DPP4. Dr Lamana EASD,Lisbonne sept Summary: Combination Therapy With Sitagliptin Plus Metformin. Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated.")
17
THE BEGAMI STUDY Primary End-point
The aim of this study was to test the hypothesis that treatment with a DPP-4 initiated soon after a coronary event improves beta-cell function. Conclusion Sitagliptin improved beta-cell function and normalised glucose perturbations in patients with ACS and newly discovered glucose disturbances. Based on the present results, it is proposed that this DPP IV inhibitor, by targeting a core deficit in ACS patients with newly detected glucose perturbations, may prevent future development of T2DM as well as the accompanying cardiovascular complications. An important finding is that the drug could be safely introduced shortly after the acute coronary event. Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated. Ref: Camilla Hage & all. 1doi: /joim.12032 © 2013 The Association for the Publication of the Journal of Internal Medicine

18
THE BEGAMI STUDY Figure 2. Patient allocation according to glucose tolerance at randomisation and after 12 weeks of treatment. Numbers on the lines represent the number of patients transferred between glucose categories. ■ Normal glucose tolerance ■ Impaired glucose tolerance ■ Type 2 diabetes. Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated. Ref: Camilla Hage & all. 1doi: /joim.12032 © 2013 The Association for the Publication of the Journal of Internal Medicine

19
Sitagliptine vs sulfonylurés
Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated.

20
Incretine Based Therapies Ongoing Cardiovascular Outcome Trials
Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated.

21
Coadministration de la sitagliptine et de la metformine chez des adultes en santé : augmentation plus grande du GLP-1 actif, comparativement à l’un ou l’autre agent en monothérapie Sitagliptine 100 mg Metformine mg Placebo Sitagliptine 100 mg + metformine mg 50 Rapports des ASC moyennes : Cette étude avait pour but d’examiner l’effet de la sitagliptine, de la metformine et de la combinaison de ces deux agents sur les concentrations postprandiales des hormones incrétines, plus précisément du GLP-1 et du GIP, chez des sujets en santé, non atteints de diabète de type 21. Les sujets ont été répartis de manière aléatoire pour recevoir la sitagliptine, la metformine, la combinaison de ces deux agents, ou le placebo. Au jour 2 de chaque période de traitement, on a prélevé des échantillons de sang pour mesurer les concentrations du GLP-1 actif et du GLP-1 total ainsi que celles du GIP actif et du GIP total, avant le repas ainsi qu’à intervalles prédéterminés après le repas durant lequel le patient avait pris son médicament1. On constate qu’après l’administration du placebo (ligne bleue), les concentration du GLP-1 actif ont légèrement augmenté, comme c’est le cas en général après un repas. Après l’administration de la sitagliptine (ligne jaune), les concentrations du GLP-1 actif ont augmenté davantage, comme on pouvait s’y attendre vu le mode d’action de la sitagliptine comme inhibiteur de la DPP-4. Ce qu’on n’avait peut-être pas prévu, toutefois, est que la metformine a également élevé les concentrations du GLP-1 actif après le repas et qu’après la coadministration de la sitagliptine et de la metformine, on a observé une élévation beaucoup plus marquée des concentrations du GLP-1 actif – même un peu plus marquée que l’élévation attribuable à l’effet additif des deux agents. Nous savons que la metformine n’inhibe pas la DPP-4 et on croit qu’elle accroît les concentrations du GLP-1 actif en stimulant la sécrétion de GLP-1. Ce que l’on constate, toutefois, c’est que la coadministration de la sitagliptine et de la metformine est un moyen très efficace d’accroître les concentrations du GLP-1 actif, ce qui est une très bonne justification raisonnée de l’association de la sitagliptine et de la metformine. Il importe de souligner cependant que cette étude était menée auprès de sujets en santé et que ces résultats n’ont pas encore été reproduits chez des sujets atteints de diabète de type 2. Référence : Données en dossier, MSD 40 Sita + Met : 4,12 Concentrations de GLP-1 actif (pM) 30 20 Sita : 1,95 Met : 1,6 10 –2 –1 1 2 3 4 Dose matinale, jour 2 Repas Temps (nombre d’heures avant et après le repas) Valeurs exprimées comme la moyenne géométrique ± l’écart type. N = 16 sujets en santé. ASC : aire sous la courbe des concentrations sanguines. Données en dossier, MSD.
, les concentration du GLP-1 actif ont légèrement augmenté, comme c’est le cas en général après un repas. Après l’administration de la sitagliptine (ligne jaune), les concentrations du GLP-1 actif ont augmenté davantage, comme on pouvait s’y attendre vu le mode d’action de la sitagliptine comme inhibiteur de la DPP-4. Ce qu’on n’avait peut-être pas prévu, toutefois, est que la metformine a également élevé les concentrations du GLP-1 actif après le repas et qu’après la coadministration de la sitagliptine et de la metformine, on a observé une élévation beaucoup plus marquée des concentrations du GLP-1 actif – même un peu plus marquée que l’élévation attribuable à l’effet additif des deux agents. Nous savons que la metformine n’inhibe pas la DPP-4 et on croit qu’elle accroît les concentrations du GLP-1 actif en stimulant la sécrétion de GLP-1. Ce que l’on constate, toutefois, c’est que la coadministration de la sitagliptine et de la metformine est un moyen très efficace d’accroître les concentrations du GLP-1 actif, ce qui est une très bonne justification raisonnée de l’association de la sitagliptine et de la metformine. Il importe de souligner cependant que cette étude était menée auprès de sujets en santé et que ces résultats n’ont pas encore été reproduits chez des sujets atteints de diabète de type 2. Référence : Données en dossier, MSD. 40. Sita + Met : 4,12. Concentrations de GLP-1 actif (pM) Sita : 1,95. Met : 1, –2. – Dose matinale, jour 2. Repas. Temps (nombre d’heures avant et après le repas) Valeurs exprimées comme la moyenne géométrique ± l’écart type. N = 16 sujets en santé. ASC : aire sous la courbe des concentrations sanguines. Données en dossier, MSD.")
23
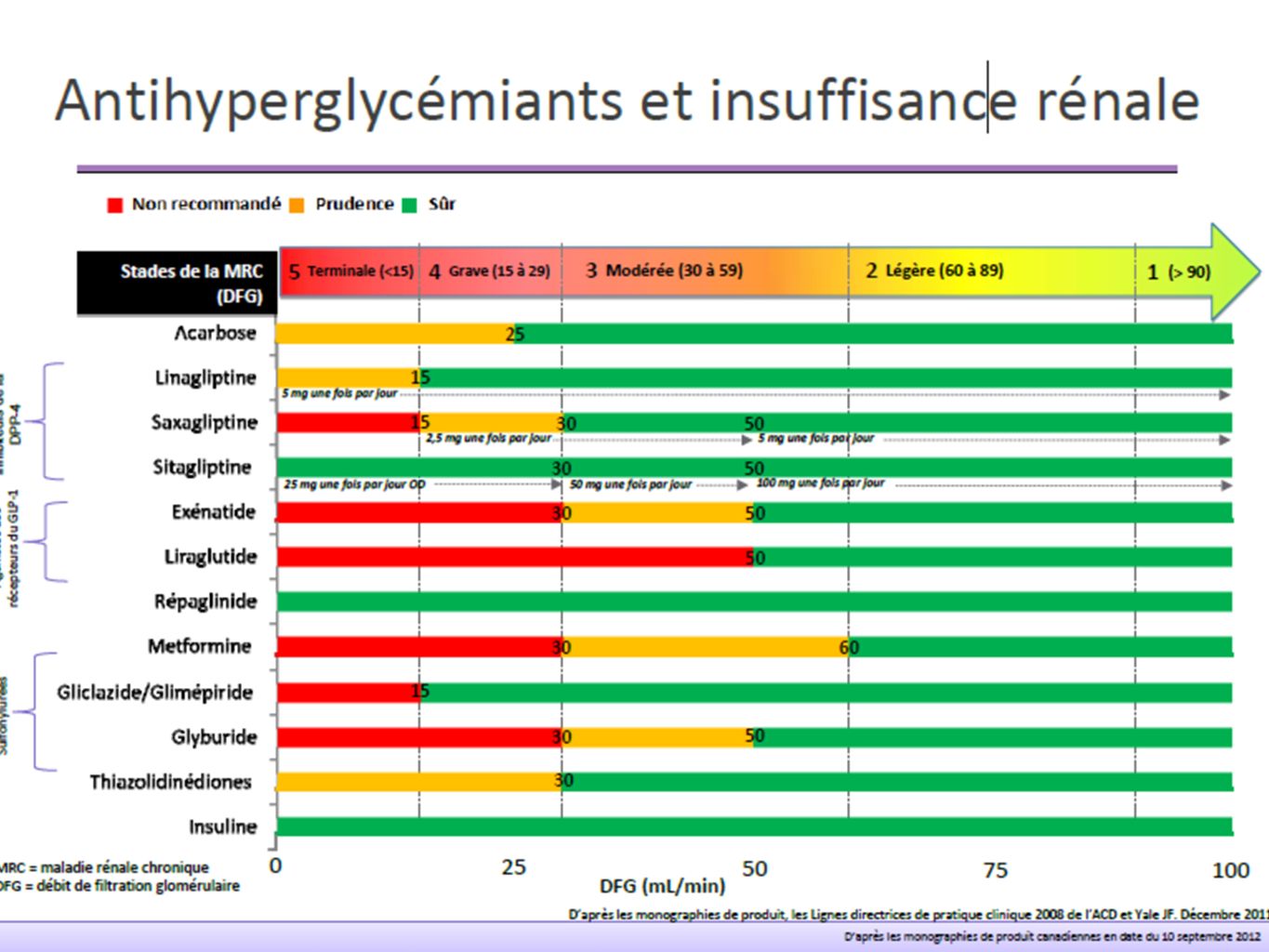
Incretin-based therapies in renal insufficiency Canadian Monographs
Sitagliptin Januvia®1 Linagliptin Trajenta®2 Saxagliptin Onglyza®3 Exenatide Byetta®4 Liraglutide Victoza®5 Stage of renal insufficiency Mild CrCl >50mlL/min Yes Limited clinical experience Moderate CrCl :50 to 30mL/min Dose reduction 50mg Dose reduction 2.5 mg QD Caution Not recommended Severe CrCl <30ml/min 25mg (Dose reduction 2.5 mg QD) No ESRD/Dialysis CrCl <15ml/min Yes* Not Recommended * Clinical study experience with TRAJENTA in patients with End Stage Renal Disease (ESRD) and those on dialyis is limited. TRAJENTATM should be used with caution in these patients 1 Product Monograph Canada Januvia Aug 2012 Product Monograph Canada Trajenta Aug 2012 Product Monograph Onglyza Nov 8, 2011 4. Product Monograph Canada Byetta July 2012 5. Product Monograph Canada Victoza Nov 15, 2011
 No. ESRD/Dialysis. CrCl <15ml/min. Yes* Not Recommended. * Clinical study experience with TRAJENTA in patients with End Stage Renal Disease. (ESRD) and those on dialyis is limited. TRAJENTATM should be used with caution in these patients. 1 Product Monograph Canada Januvia Aug Product Monograph Canada Trajenta Aug Product Monograph Onglyza Nov 8, Product Monograph Canada Byetta July Product Monograph Canada Victoza Nov 15,")
25
OU De 6 à 2 comprimés ! Janumet 2 fois par jour Matin Soir
Summary: Combination Therapy With Sitagliptin Plus Metformin Evidence suggests that earlier combination therapy for appropriate patients may be a viable strategy for patients with type 2 diabetes. Sitagliptin and metformin have complementary mechanisms of action. Initial combination therapy with sitagliptin and metformin for the treatment of type 2 diabetes substantially improves glycemic control and is generally well tolerated. OU Janumet 2 fois par jour

Présentations similaires