Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

2
Coma et Traumatisme Crânien
Dr. J. Warman Chardon, FRCPC (Neurologie) Fellow, Neurogénétique/Neuromusculaire Université d’Ottawa, McGill University 14 Fevrier 2014
 Fellow, Neurogénétique/Neuromusculaire. Université d’Ottawa, McGill University. 14 Fevrier")
3
Objectifs La “conscience” Le traumatisme cranien
Le coma et ses causes Le traumatisme cranien Ses consequences, et les hematomes craniens La pression intracrânienne Les principes de base L’hypertension intracrânienne Les hernies cérébrales

4
Objectifs de la séance 3437 Définir les termes conscience et coma Discuter de la pression intracrânienne ainsi que des causes et conséquences cliniques de l’hypertension intracrânienne Expliquer les relations entre la pression artérielle systémique, la pression partielle de l’oxygène (pO2), la pression partielle du gaz carbonique (pCO2) et la pression intracrânienne Décrire les syndromes liés à une hernie (uncus de l’hippocampe, amygdale du cervelet) en ce qui concerne les structures anatomiques touchées et les manifestations cliniques Décrire les types suivants de lésion cérébrale acquise: commotion, contusion, hématome extradural, hématome sous‐dural, hémorragie sous‐arachnoïdienne.
, la pression partielle du gaz carbonique (pCO2) et la pression intracrânienne Décrire les syndromes liés à une hernie (uncus de l’hippocampe, amygdale du cervelet) en ce qui concerne les structures anatomiques touchées et les manifestations cliniques Décrire les types suivants de lésion cérébrale acquise: commotion, contusion, hématome extradural, hématome sous‐dural, hémorragie sous‐arachnoïdienne.")
6
La conscience Définition médicale Connaissance de soi-même
Réactivité aux stimulus externes et besoins internes conscience est un concepte qui est difficile a definir parce-que c’est un terme qui n’est pas strictement medical, mais aussi literaire, philosophique et psychologique. Il y a donc beaucoup d’ambiguite quand on parle la conscience. En gros, la conscience est “un etat de connaissance de soi-meme et des environs”, mais cette connaissance de soi-meme peut consister d’emotions, d’attitudes, etc.. D’un point de vue medical, nous preferons une definition plus objective. La conscience consiste de deux parties: la connaissance de soi-meme et la reactivite aux stimulus externes et besoins internes This narrow definition has an advantage in that unconsciousness has the opposite meaning: a state of unawareness of self and environment or a suspension of those mental activities by which people are made aware of themselves and their environment, coupled always with a diminished responsiveness to environmental stimuli Un example: quand on donne un stimulus douloureux a un patient dans un coma, il ne peut Ni sentir la douleur Ni reagir a cette douleur

7
Etat éveille, conscient
Niveaux de conscience Etat éveille, conscient Léthargie Stupeur Coma Lethargie: incapable de soutenir un etat de vigilance sans un stimulus externe. Example - quelqu’un qui est en train de s’endormir, comme des etudiants dans une salle de classe, comme plusieurs parmis vous Stupeur - un etat ou le patient ne peut etre reveille qu’avec un stimulus vigoureux, mais cet etat de reveil ne peut etre soutenu sans stimulus continu. Il faut preciser que ces termes ne sont pas toujours utilises d’une manniere precise. Dans un rapport medical, il vaut mieux de donner une description de ce que le patient peut faire out ne peut pas faire, et aussi comment il reagit a plusieurs stimulus.

8
Lethargie: Stupeur: Ne peut rester eveille sans stimulus externe
Ne peut rester eveille sans stimulus vigoureux et continu Lethargie: incapable de soutenir un etat de vigilance sans un stimulus externe. Example - quelqu’un qui est en train de s’endormir Stupeur - un etat ou le patient ne peut etre reveille qu’avec un stimulus vigoureux, mais cet etat de reveil ne peut etre soutenu sans stimulus continu. Il faut preciser que ces termes ne sont pas toujours utilises d’une manniere precise. Dans un rapport medical, il vaut mieux de donner une description de ce que le patient peut faire out ne peut pas faire, et aussi comment il reagit a plusieurs stimulus.

9
Coma Une abolition complète (+/-) des fonctions de la vie de relation (conscience, motilité, sensibilité) alors que les fonctions de la vie végétative sont relativement conservées Un patient qui a l’air d’etre endormi, et qui ne peut etre reveille par un stimulus externe, our par un besoin interne est dit d’etre dans un etat de coma. Le patient, inconscient, est couché sans bouger et ne sent rien “Une abolition plus ou moins complète des fonctions de la vie de relation (conscience, motilité, sensibilité) alors que les fonctions de la vie végétative sont relativement conservées Il y a plusieurs degres de coma: dans l’etat le plus grave, il n’y a aucun reflex (pupillaire, corneen etc..) Le coma est donc tres semblable au sommeil. Les differences entre le sommeil et le coma peut etre reveille Le niveau d’oxygene cerebral EEG Activite motrice spontanee
 des fonctions de la vie de relation (conscience, motilité, sensibilité) alors que les fonctions de la vie végétative sont relativement conservées. Un patient qui a l’air d’etre endormi, et qui ne peut etre reveille par un stimulus externe, our par un besoin interne est dit d’etre dans un etat de coma. Le patient, inconscient, est couché sans bouger et ne sent rien. Une abolition plus ou moins complète des fonctions de la vie de relation (conscience, motilité, sensibilité) alors que les fonctions de la vie végétative sont relativement conservées. Il y a plusieurs degres de coma: dans l’etat le plus grave, il n’y a aucun reflex (pupillaire, corneen etc..) Le coma est donc tres semblable au sommeil. Les differences entre le sommeil et le coma. peut etre reveille. Le niveau d’oxygene cerebral. EEG. Activite motrice spontanee.")
10
Coma Perte de conscience et de vigilance non reversible par les stimulus Les differences entre le sommeil et le coma peut être réveillé Le niveau d’oxygène cerébral EEG Activite motrice spontanee

11
Les causes? système d'activation réticulaire: thalamus, hypothalamus, tronc cérébral

12
Traumatisme Cranien

13
Traumatisme Cranien Conséquences neurologiques Locaux Diffus
Sensitif, moteur, langue, etc Diffus Perte de memoire et souvenirs Céphalées Crises épileptiques Coma

14
Hématomes Crâniens Epidural (HED) Sous-dural (HSD)
Sous-arachnoïdien (HSA) Contusions cérébrales une lésion axonale diffuse 14
 Contusions cérébrales. une lésion axonale diffuse. 14.")
15
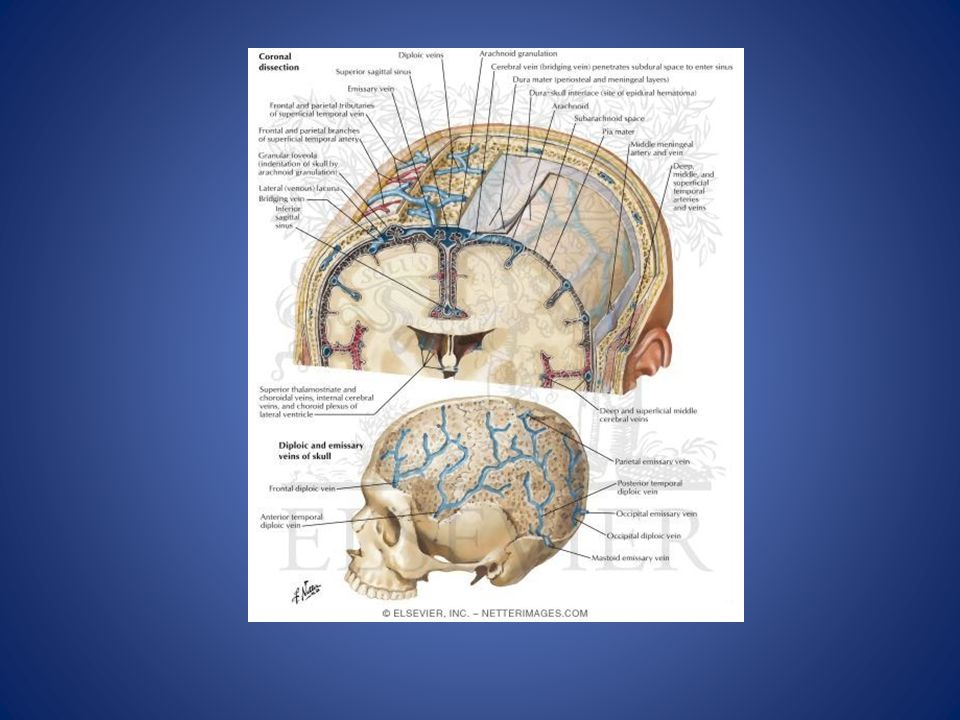
Anatomie Les méninges: Dure-mère Arachnoïde Pie-mère 15

17
Hématome épidural Souvent associées avec les fractures crâniennes
Régions temporales et parietales Croissance limitée par les sutures du crâne Apparence classique: biconvex lenticulaire Moins courant que les HSD (8-10%) Acute Epidural Hemorrhage As a rule, epidural hematoma arises with a temporal or parietal fracture and laceration of the middle meningeal artery or vein. Less often, there is a tear in a dural venous sinus. The injury, even when it fractures the skull, may not have produced coma initially, or it may be part of a devastating craniocerebral injury. A typical example is that of a child who has fallen from a bicycle or swing or has suffered some other hard blow to the head and was unconscious only momentarily. A few hours later (exceptionally, with venous bleeding the interval may be several days or a week), headache of increasing severity develops, with vomiting, drowsiness, confusion, aphasia, seizures (which may be one-sided), hemiparesis with slightly increased tendon reflexes, and a Babinski sign. As coma develops, the hemiparesis may give way to bilateral spasticity of the limbs and Babinski signs. The pulse is often slow (below 60 beats/min) and bounding, with a concomitant rise in systolic blood pressure (Cushing effect). The pupil may dilate on the side of the hematoma. Physicians need not be reminded that lumbar puncture is contraindicated in this setting, particularly now that CT and MRI are available. Death, which is almost invariable if an expanding clot is not removed surgically, comes at the end of a comatose period and is a result of respiratory arrest. The visualization of a fracture line across the groove of the middle meningeal artery and knowledge of which side of the head was struck (the clot is on that side) are of aid in diagnosis and lateralization of the lesion. However, meningeal vessels may occasionally be torn without fracture. The CT scan is definitive and reveals a lens-shaped clot with a smooth inner margin (Fig. 35-8). The surgical procedure consists of placement of burr holes in an emergency situation or, preferably, a craniotomy, drainage of the hematoma, and identification and ligation of the bleeding vessel. The operative results are excellent except in cases with extended fractures and laceration of the dural venous sinuses, in which the epidural hematoma may be bilateral rather than unilateral. If coma, bilateral Babinski signs, spasticity, or decerebrate rigidity supervene before operation, it usually means that displacement of central structures and compression of the midbrain have already occurred; prognosis is then poor, but a few patients do well if surgery is not greatly delayed. Small epidural hemorrhages can be followed by serial CT scanning and will be seen to enlarge gradually for a week or two and then be absorbed. There is controversy about the benefit of removing these smaller clots in a patient who has no symptoms; with careful clinical and imaging surveillance, most can be left alone. Genetics: There is a role for genetics in spontaneous (nontraumatic) epidural hematoma caused by coagulopathies and vascular malformations. Risk factors: Head trauma associated with skull fracture Physical findings & clinical presentation • History of head trauma is present. • Transient loss of consciousness, followed by a “lucid interval” in 47% of cases, where the patient is free of any neurologic signs or symptoms. This is followed by clinical deterioration. • Signs and symptoms vary depending on severity. • Symptoms: headache, vomiting, drowsiness, confusion, aphasia, seizures, paralysis, and even coma are found. • Signs: external signs of skull fracture—lacerations, ecchymoses, cerebrospinal fluid (CSF) rhinorrhea or otorrhea are observed. • Altered mental status, nuchal rigidity, photophobia, focal neurologic deficit—paralysis of one limb, unequal pupils, decerebrate posture, coma—are seen. Etiology • Traumatic: commonly caused by arterial injury (the middle meningeal artery) but may also be injury of the anterior meningeal artery, a dural arteriovenous (AV) fistula at the vertex, or from venous bleeding • Nontraumatic: caused by an infection/eroding abscess, coagulopathy, hemorrhagic tumors, vascular malformations, postsurgical procedures, and in special populations (e.g., pregnant women, patients receiving hemodialysis) 17
 Acute Epidural Hemorrhage. As a rule, epidural hematoma arises with a temporal or parietal fracture and laceration of the middle meningeal artery or vein. Less often, there is a tear in a dural venous sinus. The injury, even when it fractures the skull, may not have produced coma initially, or it may be part of a devastating craniocerebral injury. A typical example is that of a child who has fallen from a bicycle or swing or has suffered some other hard blow to the head and was unconscious only momentarily. A few hours later (exceptionally, with venous bleeding the interval may be several days or a week), headache of increasing severity develops, with vomiting, drowsiness, confusion, aphasia, seizures (which may be one-sided), hemiparesis with slightly increased tendon reflexes, and a Babinski sign. As coma develops, the hemiparesis may give way to bilateral spasticity of the limbs and Babinski signs. The pulse is often slow (below 60 beats/min) and bounding, with a concomitant rise in systolic blood pressure (Cushing effect). The pupil may dilate on the side of the hematoma. Physicians need not be reminded that lumbar puncture is contraindicated in this setting, particularly now that CT and MRI are available. Death, which is almost invariable if an expanding clot is not removed surgically, comes at the end of a comatose period and is a result of respiratory arrest. The visualization of a fracture line across the groove of the middle meningeal artery and knowledge of which side of the head was struck (the clot is on that side) are of aid in diagnosis and lateralization of the lesion. However, meningeal vessels may occasionally be torn without fracture. The CT scan is definitive and reveals a lens-shaped clot with a smooth inner margin (Fig. 35-8). The surgical procedure consists of placement of burr holes in an emergency situation or, preferably, a craniotomy, drainage of the hematoma, and identification and ligation of the bleeding vessel. The operative results are excellent except in cases with extended fractures and laceration of the dural venous sinuses, in which the epidural hematoma may be bilateral rather than unilateral. If coma, bilateral Babinski signs, spasticity, or decerebrate rigidity supervene before operation, it usually means that displacement of central structures and compression of the midbrain have already occurred; prognosis is then poor, but a few patients do well if surgery is not greatly delayed. Small epidural hemorrhages can be followed by serial CT scanning and will be seen to enlarge gradually for a week or two and then be absorbed. There is controversy about the benefit of removing these smaller clots in a patient who has no symptoms; with careful clinical and imaging surveillance, most can be left alone. Genetics: There is a role for genetics in spontaneous (nontraumatic) epidural hematoma caused by coagulopathies and vascular malformations. Risk factors: Head trauma associated with skull fracture. Physical findings & clinical presentation. • History of head trauma is present. • Transient loss of consciousness, followed by a lucid interval in 47% of cases, where the patient is free of any neurologic signs or symptoms. This is followed by clinical deterioration. • Signs and symptoms vary depending on severity. • Symptoms: headache, vomiting, drowsiness, confusion, aphasia, seizures, paralysis, and even coma are found. • Signs: external signs of skull fracture—lacerations, ecchymoses, cerebrospinal fluid (CSF) rhinorrhea or otorrhea are observed. • Altered mental status, nuchal rigidity, photophobia, focal neurologic deficit—paralysis of one limb, unequal pupils, decerebrate posture, coma—are seen. Etiology. • Traumatic: commonly caused by arterial injury (the middle meningeal artery) but may also be injury of the anterior meningeal artery, a dural arteriovenous (AV) fistula at the vertex, or from venous bleeding • Nontraumatic: caused by an infection/eroding abscess, coagulopathy, hemorrhagic tumors, vascular malformations, postsurgical procedures, and in special populations (e.g., pregnant women, patients receiving hemodialysis) 17.")
18
Hématome épidural Pathophysiologie: Déchirure des artères méningées**
Urgence! -> Effet de Cushing 18

19
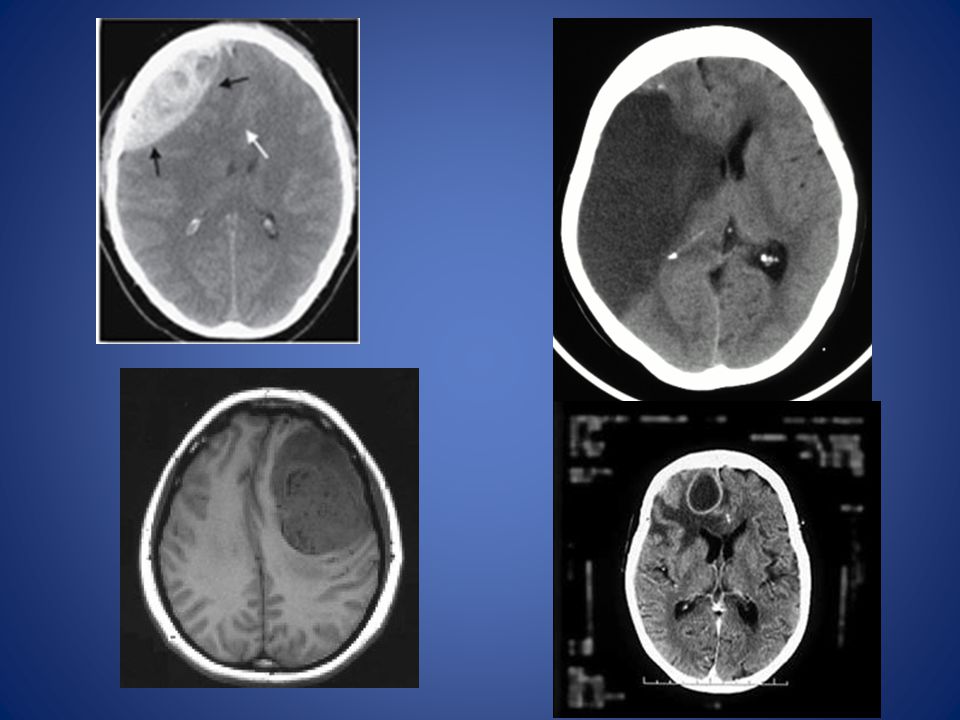
In this case, a predominantly high-density, extra-axial, hemorrhagic collection (black arrows) is producing mass effect on the right frontal lobe on an unenhanced head CT scan (Figure A). Mass effect results in marked distortion of the underlying cortex and leftward subfalcine herniation (white arrow) (Figure A). A linear nondepressed fracture is present along the anterior aspect of the right parietal bone (black arrow) (Figure B). The biconvex appearance of this lesion is typical of an epidural hematoma, which is the acute finding in this case (C is the correct answer to Question 12-12). Intracranial abnormalities in head trauma can be classified as either primary or secondary. Primary lesions occur at the moment of injury and include skull fractures, extracerebral hemorrhage (eg, epidural or subdural hematomas, subarachnoid hemorrhage), and intracerebral hemorrhage (eg, brain contusion, brainstem injury, diffuse axonal injury). The secondary effects of head trauma are actually complications of the primary intracranial injury. Elevated intracranial pressure and cerebral herniation are responsible for most of the secondary effects of head trauma, which in many cases may be more devastating to the patients than the initial injury. Epidural hematoma is usually associated with skull fractures that lacerate the middle meningeal artery or a dural sinus. Up to one-half of patients with epidural hematomas have a lucid interval after the head trauma occurs. On CT, epidural hematomas usually appear as biconvex, high-attenuation, extra-axial masses. Most are located in the temporoparietal area. Underlying skull fractures are common. Intracranial brain herniation may also be a prominent feature in this condition. One important imaging feature in epidural hematomas is that they do not cross skull sutures, but may cross the midline.
, and intracerebral hemorrhage (eg, brain contusion, brainstem injury, diffuse axonal injury). The secondary effects of head trauma are actually complications of the primary intracranial injury. Elevated intracranial pressure and cerebral herniation are responsible for most of the secondary effects of head trauma, which in many cases may be more devastating to the patients than the initial injury. Epidural hematoma is usually associated with skull fractures that lacerate the middle meningeal artery or a dural sinus. Up to one-half of patients with epidural hematomas have a lucid interval after the head trauma occurs. On CT, epidural hematomas usually appear as biconvex, high-attenuation, extra-axial masses. Most are located in the temporoparietal area. Underlying skull fractures are common. Intracranial brain herniation may also be a prominent feature in this condition. One important imaging feature in epidural hematomas is that they do not cross skull sutures, but may cross the midline.")
20
Hématome sous-dural Espace sous-dural L’hématome le plus courrant
Aigu, sous-aigu, chronique Croissance limitée par les pliements duraux Subdural hematoma, on the other hand, is usually a crescent-shaped extra-axial collection that may cross suture lines, but is confined by the dural reflections (Figure 12-31). CT can usually, but not always, distinguish between epidural hematomas and subdural hematomas. Subdural hematomas are a commonly identified abnormality in the abused child (nonaccidental trauma). CT scans are obtained to detect the presence of subdural hematomas (Figure 12-32). A brain MRI, however, can more sensitively delineate small extra-axial hematomas, subdural hematomas of varying ages, and coexisting cortical contusions or shearing injuries. A shearing injury (or diffuse axonal injury) is associated with an overall poor prognosis and is recognized as small petechial hemorrhages at the gray-white junction and in the corpus callosum. Interhemispheric (para- and intrafalcial) subdural hematomas may arise from tearing of bridging veins along the falx cerebri in shaking injuries and are nearly pathognomic for nonaccidental trauma. Retinal hemorrhages may be present and are also suspicious, especially if bilateral. In addition, cerebral ischemia/infarction and multiple, complex, unexplained skull fractures may be associated findings. 20
. CT can usually, but not always, distinguish between epidural hematomas and subdural hematomas. Subdural hematomas are a commonly identified abnormality in the abused child (nonaccidental trauma). CT scans are obtained to detect the presence of subdural hematomas (Figure 12-32). A brain MRI, however, can more sensitively delineate small extra-axial hematomas, subdural hematomas of varying ages, and coexisting cortical contusions or shearing injuries. A shearing injury (or diffuse axonal injury) is associated with an overall poor prognosis and is recognized as small petechial hemorrhages at the gray-white junction and in the corpus callosum. Interhemispheric (para- and intrafalcial) subdural hematomas may arise from tearing of bridging veins along the falx cerebri in shaking injuries and are nearly pathognomic for nonaccidental trauma. Retinal hemorrhages may be present and are also suspicious, especially if bilateral. In addition, cerebral ischemia/infarction and multiple, complex, unexplained skull fractures may be associated findings. 20.")
21
Hématome sous-dural Pathophysiologie: Déchirure des veines en pont 21

22
L’ étiologie? Epidemiology & demographics Incidence:
SDH is a common finding, especially among trauma patients. Prevalence: Unknown Peak incidence: SDH most commonly occurs in the elderly and alcoholic populations as a result of cerebral atrophy and in the infant population (e.g., shaken baby) as a result of the increasing traction on the bridging veins between the brain parenchyma and the dura mater. SDHs are more common than epidural hematomas. Risk factors: Any conditions that predispose patients to hemorrhage (e.g., anticoagulants, antiplatelet therapy); atrophy of the brain (e.g., dementia, alcoholism); or falls and trauma (e.g., movement disorders, previous stroke) Physical findings & clinical presentation Symptoms vary on the basis of acuity, size, and location. Acute traumatic SDHs are often seen in comatose patients. When they are associated with a midline shift (i.e., >5 mm), they can cause signs of cerebral herniation (e.g., ipsilateral pupil dilation, contralateral weakness). Chronic and subacute SDHs present with variable symptoms of headache, mild weakness, slowness of mentation, aphasia, mobility problems, and abulia. Etiology SDH is usually the result of shear and of the tearing of a bridging vein. It can be caused by any source of bleeding into the subdural space (i.e., contusion, extension of parenchymal hemorrhage, rarely other vascular abnormalities [e.g., arteriovenous malformation, aneurysm]). Rapidly evolving subdural hematomas are usually a result of tearing of bridging veins, and symptoms are caused by compression of the adjacent brain and of deep structures. Unlike epidural arterial hemorrhage, which is steadily progressive, the rising intracranial pressure usually arrests venous bleeding. CAUSE/POPULATION AT RISK? Etoh, elderly, anti coag, shaken baby 22
 as a result of the increasing traction on the bridging veins between the brain parenchyma and the dura mater. SDHs are more common than epidural hematomas. Risk factors: Any conditions that predispose patients to hemorrhage (e.g., anticoagulants, antiplatelet therapy); atrophy of the brain (e.g., dementia, alcoholism); or falls and trauma (e.g., movement disorders, previous stroke) Physical findings & clinical presentation. Symptoms vary on the basis of acuity, size, and location. Acute traumatic SDHs are often seen in comatose patients. When they are associated with a midline shift (i.e., >5 mm), they can cause signs of cerebral herniation (e.g., ipsilateral pupil dilation, contralateral weakness). Chronic and subacute SDHs present with variable symptoms of headache, mild weakness, slowness of mentation, aphasia, mobility problems, and abulia. Etiology. SDH is usually the result of shear and of the tearing of a bridging vein. It can be caused by any source of bleeding into the subdural space (i.e., contusion, extension of parenchymal hemorrhage, rarely other vascular abnormalities [e.g., arteriovenous malformation, aneurysm]). Rapidly evolving subdural hematomas are usually a result of tearing of bridging veins, and symptoms are caused by compression of the adjacent brain and of deep structures. Unlike epidural arterial hemorrhage, which is steadily progressive, the rising intracranial pressure usually arrests venous bleeding. CAUSE/POPULATION AT RISK Etoh, elderly, anti coag, shaken baby. 22.")
23
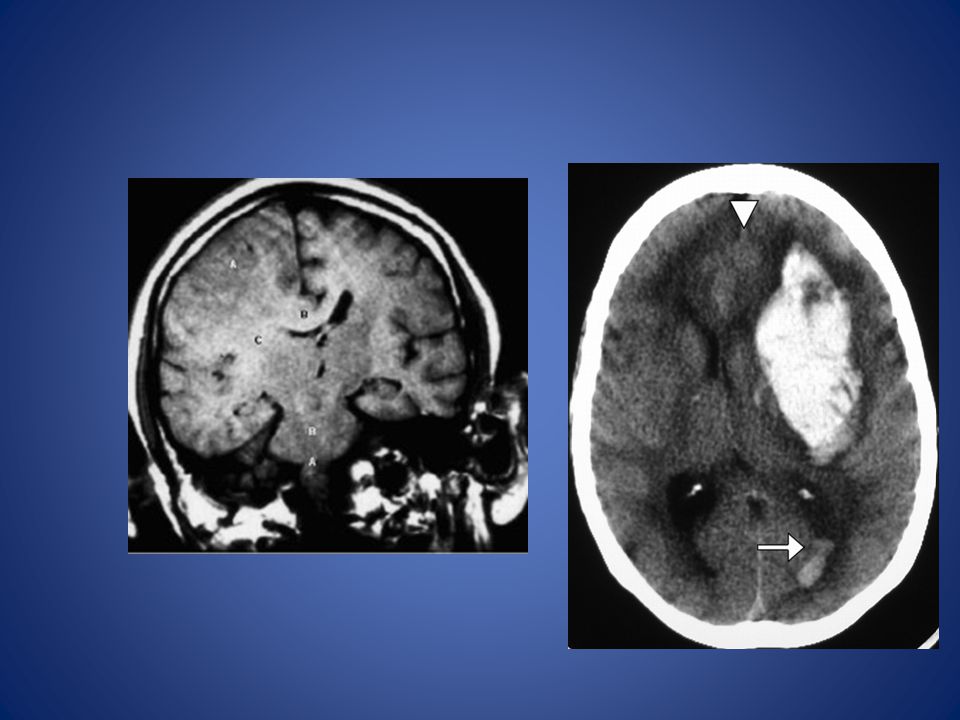
Hématome sous-dural Conséquences cliniques: Effet de masse
+/-Contusions cérébrales, oédème cérébrale Noncontrast axial CT images (A, B) in a 21-day-old male following nonaccidental trauma. Large, bilateral subdural hematomas layer over the tentorium cerebelli in (A) (closed arrows) and within the interhemispheric fissure in (B) (arrow). In addition, a small amount of subarachnoid hemorrhage is seen within the quadrigeminal plate cistern in (A) (open arrows), as well as within the left lateral ventricle (not shown). Loss of the normal cerebral gray-white differentiation is demonstrated. These features are nearly pathognomonic for nonaccidental trauma with diffuse anoxic insult. Cerebral contusions (Case 12-13) are the second most common form of brain parenchymal injury in primary head trauma (diffuse axonal injury is the most common parenchymal injury). Cerebral contusions can be thought of as brain bruises. They result either from the brain striking a bony ridge inside the skull during rapid acceleration/deceleration, as occurs in a motor vehicle accident, or from a depressed skull fracture. These lesions tend to occur in particular anatomic locations, especially the undersurfaces and poles of the frontal and temporal lobes (Figure 12-33). CT scans show areas of low attenuation (edema) and hemorrhage at the site of injury. Delayed hemorrhage, 1 to 2 days after a head injury, is common with contusions. 23
 in a 21-day-old male following nonaccidental trauma. Large, bilateral subdural hematomas layer over the tentorium cerebelli in (A) (closed arrows) and within the interhemispheric fissure in (B) (arrow). In addition, a small amount of subarachnoid hemorrhage is seen within the quadrigeminal plate cistern in (A) (open arrows), as well as within the left lateral ventricle (not shown). Loss of the normal cerebral gray-white differentiation is demonstrated. These features are nearly pathognomonic for nonaccidental trauma with diffuse anoxic insult. Cerebral contusions (Case 12-13) are the second most common form of brain parenchymal injury in primary head trauma (diffuse axonal injury is the most common parenchymal injury). Cerebral contusions can be thought of as brain bruises. They result either from the brain striking a bony ridge inside the skull during rapid acceleration/deceleration, as occurs in a motor vehicle accident, or from a depressed skull fracture. These lesions tend to occur in particular anatomic locations, especially the undersurfaces and poles of the frontal and temporal lobes (Figure 12-33). CT scans show areas of low attenuation (edema) and hemorrhage at the site of injury. Delayed hemorrhage, 1 to 2 days after a head injury, is common with contusions. 23.")
24
Hématome sous-dural Symptômes: Mal de tête/céphalée, assoupissement, trouble neurologique focal…

25
Hématomes sous-arachnoïdiens
Espace sous arachnoidien Courant suivant les ruptures d’anévrisme > les traumatismes crâniens Risque de spasme des vaisseaux sanguins, crises, hydrocéphalie, resaignement Treatment Medical management of the subarachnoid hemorrhage patient in the ED should occur in a monitored critical care area and should target the prevention of complications. The Glasgow Coma Scale (GCS) and pupillary responses should be checked regularly, because a decrease of one GCS point can indicate the onset of complications.1 Intracerebral and extracerebral complications of subarachnoid hemorrhage include vasospasm, rebleeding, cerebral infarction, cerebral edema, hydrocephalus, intracranial hypertension, fluid status and electrolyte abnormalities, respiratory failure, myocardial dysfunction, thromboembolism, and sepsis.23 The risk of rebleeding is greatest in the first 24 hours and can be reduced by adequate blood pressure control. The ideal target blood pressure and antihypertensive agent remain unclear. If known, the patient's prehemorrhage blood pressure should be maintained; otherwise, a mean arterial pressure of <130 mm Hg is a reasonable target. Because blood pressure may fluctuate through the course of the disease, a titratable IV antihypertensive, such as labetalol, is preferred. Pain medications and antiemetics also play an important role in maintaining the alert patient's comfort and blood pressure. Hypotension should be avoided. There is debate regarding the use of antifibrinolytics to prevent rebleeding after subarachnoid hemorrhage, but generally these are not used, because there is a risk of increased cerebral ischemia. Vasospasm is most common 2 days to 3 weeks after subarachnoid hemorrhage. A modest protective benefit is seen with administration of nimodipine, 60 milligrams PO every 4 hours, and this therapy should be initiated within 96 hours of symptom onset unless contraindicated due to allergy, nonfunctioning GI tract, or hepatic disease. IV magnesium and statins may also prove beneficial, although studies are not conclusive at this point. Delayed cerebral ischemia is associated with hypothermia, hyperthermia, and hyperglycemia; these conditions should be prevented with the appropriate use of warming or cooling blankets, antipyretics, or insulin when indicated. Approximately 5% to 20% of patients with subarachnoid hemorrhage have at least one seizure. Seizure prophylaxis is controversial and should be determined in conjunction with the intensivist or neurosurgeon who will manage the patient. 25
 and pupillary responses should be checked regularly, because a decrease of one GCS point can indicate the onset of complications.1 Intracerebral and extracerebral complications of subarachnoid hemorrhage include vasospasm, rebleeding, cerebral infarction, cerebral edema, hydrocephalus, intracranial hypertension, fluid status and electrolyte abnormalities, respiratory failure, myocardial dysfunction, thromboembolism, and sepsis.23. The risk of rebleeding is greatest in the first 24 hours and can be reduced by adequate blood pressure control. The ideal target blood pressure and antihypertensive agent remain unclear. If known, the patient s prehemorrhage blood pressure should be maintained; otherwise, a mean arterial pressure of <130 mm Hg is a reasonable target. Because blood pressure may fluctuate through the course of the disease, a titratable IV antihypertensive, such as labetalol, is preferred. Pain medications and antiemetics also play an important role in maintaining the alert patient s comfort and blood pressure. Hypotension should be avoided. There is debate regarding the use of antifibrinolytics to prevent rebleeding after subarachnoid hemorrhage, but generally these are not used, because there is a risk of increased cerebral ischemia. Vasospasm is most common 2 days to 3 weeks after subarachnoid hemorrhage. A modest protective benefit is seen with administration of nimodipine, 60 milligrams PO every 4 hours, and this therapy should be initiated within 96 hours of symptom onset unless contraindicated due to allergy, nonfunctioning GI tract, or hepatic disease. IV magnesium and statins may also prove beneficial, although studies are not conclusive at this point. Delayed cerebral ischemia is associated with hypothermia, hyperthermia, and hyperglycemia; these conditions should be prevented with the appropriate use of warming or cooling blankets, antipyretics, or insulin when indicated. Approximately 5% to 20% of patients with subarachnoid hemorrhage have at least one seizure. Seizure prophylaxis is controversial and should be determined in conjunction with the intensivist or neurosurgeon who will manage the patient. 25.")
26
Pathophysiology Subarachnoid hemorrhage is the leakage of blood into the subarachnoid space. Seventy-five percent of subarachnoid hemorrhages are caused by a ruptured aneurysm. Approximately 20% of patients with one aneurysm will have an additional aneurysm, which makes identification of the initial aneurysm more important. In 20% of subarachnoid hemorrhage cases, a cause is not identified.1 The remaining 5% are related to a variety of conditions, including arteriovenous malformations, cerebral artery dissection, coagulopathies, moyamoya syndrome, mycotic aneurysm, neoplasm, pituitary apoplexy, vasculopathy, brain tumor, and use of sympathomimetic drugs (particularly amphetamine, cocaine, phenylpropanolamine, and pseudoephedrine). The location of bleeding on CT can help identify the cause of the bleed.1 26
. The location of bleeding on CT can help identify the cause of the bleed")
27
Contusions Cérébrales
Les lésions les plus fréquemment observées Multiples et confluentes Ne causent rarement des troubles de conscience 27

28
Contusions Cérébrales
Substance grise Lobe frontale, à la face inférieure ou sur les faces latérales Coup et contre-coup 28

29
Contusions Cérébrales
Charactéristiques Radiologiques Rarement visibles en phase aiguë en tomographie (CT) Plus visibles des semaines apres l’évènement traumatique grâce a l’oedème et l’effet de masse IRM est plus sensible que la tomographie pour leurs dépistage 29
 Plus visibles des semaines apres l’évènement traumatique grâce a l’oedème et l’effet de masse. IRM est plus sensible que la tomographie pour leurs dépistage. 29.")
30
Pression intracrânienne

31
La loi “Monro-Kellie” La loi de Monro-Kellie stipule que le systême nerveux, sa vascularisation, et les espaces liquidiens céphalorachidiens (ventriculaires et sous-arachnoïens) êtant contenus dans une structure ostéodurale inextensible, toute augmentation de volume de l'un des trois compartiments se fait aux dépens de l'un ou des deux autres. Cerveau ~ 1,200 -1,400 mL Sang ~150 mL LCR ~ 70 to 140 mL
 êtant contenus dans une structure ostéodurale inextensible, toute augmentation de volume de l un des trois compartiments se fait aux dépens de l un ou des deux autres. Cerveau ~ 1,200 -1,400 mL. Sang ~150 mL. LCR ~ 70 to 140 mL.")
32
PRESSION DE PERFUSION CÉRÉBRALE
La pression de perfusion cérébrale résulte de la différence entre la tension artérielle moyenne et la tension intracrânienne : Pour maintenir une pression de perfusion de 70 mmHg, il faut que la tension artérielle moyenne soit de 90mmHg si la TIC est de l’ordre de 20mmHg. Pour ce faire, il faut que la pression systolique soit de l’ordre de 120 à 130 mmHg, ce qui n’est pas toujours le cas chez les patients traumatisés avec une instabilité hémodynamique. => si la tension intracrânienne s’élève, il devient alors nécessaire de maintenir une tension artérielle encore plus élevée

33
Pression intracrânienne
Affectée par La masse du cerveau La circulation Le liquide cérébrospinal (LCS) La rigidité du crâne Pression normale: mm H20
 La rigidité du crâne. Pression normale: mm H20.")
34
Masses intracrâniennes
Tumeurs Hémorragie Oédeme Infection (abscès)
")
36
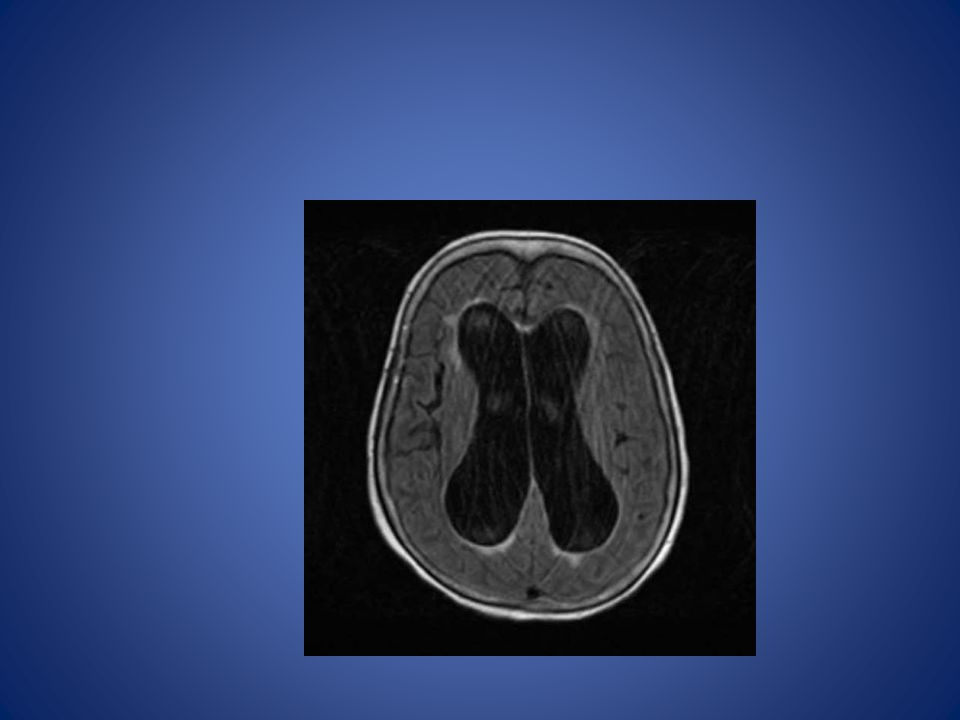
LCS Agrandissement du volume du liquide céphalo-rachidien Hydrocéphalie Méningite Hémorragie sous-arachnoïdien Hydrocephalus due to congenital aqueductal stenosis Acute hydrocephalus secondary to a meningioma

38
Circulation Autoregulation pCO2
Brain edema swelling within the closed cranium will lead to further increases in ICP with even further decreases in CPP in a stage of decompensation. When the capacity for autoregulation is exceeded or damaged so that it can no longer play a role, CBF is linked directly to the CPP. In the management of intracranial pathology, ICP and CPP are easy to measure continuously and thus serve as highly practical surrogates for the more fundamental, but much more difficult to measure, CBF. However, these are not equivalent, and the limitations of these parameters for guiding therapy need to be remembered. Regardless of causation, when concern arises about the possibility of cascading injury, every effort is made to keep the CPP in the realm of 60 mm Hg (range, 50 to 70 mm Hg) and ICP below 20 mm, Hg if possible. Routinely using pressors and volume expansion to maintain CPP higher than 70 mm Hg is not supported based on systemic complications
 and ICP below 20 mm, Hg if possible. Routinely using pressors and volume expansion to maintain CPP higher than 70 mm Hg is not supported based on systemic complications.")
39
Pression de perfusion cérébrale: La circulation cérébrale est autorégulée
Débit (ml/100g/min) Limite inf Définition : Mécanisme assurant un débit constant entre 2 limites de pression de perfusion cérébrale. Au dessous et au dessus de ces limites, le débit n'est plus régulé Limite sup 60 140 mmHg
 Limite inf. Définition : Mécanisme assurant un débit constant. entre 2 limites de pression de perfusion cérébrale. Au dessous et au dessus de ces limites, le débit n est plus régulé. Limite sup mmHg.")
40
Relation entre la pression intracranienne (PIC) et la pression carbonique (pCO2) :
pCO2 = PIC PCO2 pH sanguin Dilatation des vesseaux sanguins Flux sanguin Pression intracrânienne (PIC) Ce principe est la raison pour laquelle la hyperventilation est utilisee comme traitement de la hypertension intracranienne: L’hypertension reduit la pression carbonique sanguine, et donc, cause l’inverse de cette reaction Initial management of ICH includes airway protection and adequate ventilation. A bolus of mannitol up to 1 g/kg causes free water diuresis, increased serum osmolality, and extraction of water from the brain. The effect is delayed by about 20 minutes and has a transient benefit. Driving serum osmolality above 300 mOsm/L is of indeterminate benefit and can have deleterious cardiovascular side effects, such as hypovolemia that leads to hypotension and decreased brain perfusion. Cases of ICH typically require rapid neurosurgical evaluation. Ventriculostomy, craniotomy, or craniectomy may be needed for definitive decompression.
 Ce principe est la raison pour laquelle la hyperventilation est utilisee comme traitement de la hypertension intracranienne: L’hypertension reduit la pression carbonique sanguine, et donc, cause l’inverse de cette reaction. Initial management of ICH includes airway protection and adequate ventilation. A bolus of mannitol up to 1 g/kg causes free water diuresis, increased serum osmolality, and extraction of water from the brain. The effect is delayed by about 20 minutes and has a transient benefit. Driving serum osmolality above 300 mOsm/L is of indeterminate benefit and can have deleterious cardiovascular side effects, such as hypovolemia that leads to hypotension and decreased brain perfusion. Cases of ICH typically require rapid neurosurgical evaluation. Ventriculostomy, craniotomy, or craniectomy may be needed for definitive decompression.")
41
Hypertension Intracrânienne
Symptomes Céphalée Nausée et vomissement Assoupissement Irritabilité, niveau d’attention ou de vigilance réduite Paralysie oculaire (vue double) Édeme papillaire Dilatation de la pupille du côté de la lésion Triade de Cushing: hypertension, bradycardie, respirations irrégulières
 Édeme papillaire. Dilatation de la pupille du côté de la lésion. Triade de Cushing: hypertension, bradycardie, respirations irrégulières.")
42
Hernies intracraniennes
Qu’est-ce-que c’est? Mouvement des structures cérébrales causés par une haute pression intracrânienne

43
Anatomie

44
Méchanismes d’hernies
Brain herniation patterns. Subfalcine herniation. The cingulate gyrus shifts across midline under the falx cerebri. Uncal herniation. The uncus (medial temporal lobe gyrus) shifts medially and compresses the midbrain and cerebral peduncle. Central transtentorial herniation. The diencephalon and midbrain shift caudally through the tentorial incisura. Tonsillar herniation. The cerebellar tonsil shifts caudally through the foramen magnum. The condition that classically illustrates the expanding mass lesion is the acute epidural hematoma, seen after trauma with skull fracture. Regardless of the source, however, the progression can be similar and has been termed rostrocaudal decay to reflect the early and late stages, as listed in order below: • Focal distortion only • Effacement of gyri and sulci • Compression of the lateral (or other) ventricle • Midline shift • Subfalcial herniation • Temporal lobe tentorial herniation • Third nerve compression (unilateral dilated pupil) • Obliteration of basal cisterns • Midbrain compression • Midbrain infarction, Duret's hemorrhages (both pupils dilate, with irreversible damage to midbrain) • Further brainstem compression • Loss of brainstem reflexes: Progression from flexor posturing to extensor posturing; vestibulo-ocular and oculocephalic reflexes; corneal reflexes • Medullary compression syndrome: Respiratory reflexes; vasomotor reflexes, Cushing's reflex with elevation of the systolic blood pressure, widening of the pulse pressure, bradycardia. • Foramen magnum herniation
 shifts medially and compresses the midbrain and cerebral peduncle. Central transtentorial herniation. The diencephalon and midbrain shift caudally through the tentorial incisura. Tonsillar herniation. The cerebellar tonsil shifts caudally through the foramen magnum. The condition that classically illustrates the expanding mass lesion is the acute epidural hematoma, seen after trauma with skull fracture. Regardless of the source, however, the progression can be similar and has been termed rostrocaudal decay to reflect the early and late stages, as listed in order below: • Focal distortion only • Effacement of gyri and sulci • Compression of the lateral (or other) ventricle • Midline shift • Subfalcial herniation • Temporal lobe tentorial herniation • Third nerve compression (unilateral dilated pupil) • Obliteration of basal cisterns • Midbrain compression • Midbrain infarction, Duret s hemorrhages (both pupils dilate, with irreversible damage to midbrain) • Further brainstem compression • Loss of brainstem reflexes: Progression from flexor posturing to extensor posturing; vestibulo-ocular and oculocephalic reflexes; corneal reflexes • Medullary compression syndrome: Respiratory reflexes; vasomotor reflexes, Cushing s reflex with elevation of the systolic blood pressure, widening of the pulse pressure, bradycardia. • Foramen magnum herniation.")
45
Types d’hernies 1) Subfalcine (Cingulaire) 2) Transtentoriale
Unciforme Centrale ↑/↓ 3) Transforaminale Amygdalaire (cervelet)
 Transforaminale. Amygdalaire (cervelet)")
46
Hernie Cingulaire Symptômes: Cephalée
Faiblesse de la jambe contralatérale Mechanisme: Infarctus de la lobe frontale ipislatérale causée par la compression de l’artère cérébrale antérieure

48
Hernie Centrale Méchanisme
Déplacement symétrique des hemispheres vers le bas Compression du tronc cérébral vers le bas a travers le foramen magnum

49
Hernie Centrale - Symptômes
“Détérioration rostro-caudale” progressive Conscience diminuée Respiration Cheyne-Stokes Pupilles symétriques et fixes et nonreactives Posture décortiquée -> posture décérébrée-> flacidité Hémorragies de Duret

50
Hernie unciforme Méchanisme
Deplacement de la partie médiale du lobe temporal a travers le foramen magnum Symptomes Triade: Dilatation de la pupille, Hémiplegie, Coma

52
Hernie amygdalaire du cervelet
Méchanisme Déplacement des amgydales du cervelet vers le bas a travers le foramen magnum Compression de la moelle et de la moelle épinière Symptomes Défaillance rapide des fonctions vitales

54
Glascow Coma Scale

55
Conclusion Coma = état de perte de conscience, de vigilance avec conservation de la vie végétative Pression Perfusion Cérébrale (PPC) = PAM - PIC Retention de pCO2 augmente la pression intracérébrale La loi Monro-Kellie L’hypertension intracrânienne a des causes multiples: masse, enflure, augmentation du volume de LCR Hématome sous-dural est le plus courant, l’apparence d’une couche mince, causée par la déchirure des veines de pont Hématome epi-dural a l’apparence biconvex, lenticulaire Types d’hernie: transfalcine, transtentoriale Triade de l’hernie unciforme: Dilatation de la pupille, hémiplegie, coma 55
 = PAM - PIC. Retention de pCO2 augmente la pression intracérébrale. La loi Monro-Kellie. L’hypertension intracrânienne a des causes multiples: masse, enflure, augmentation du volume de LCR. Hématome sous-dural est le plus courant, l’apparence d’une couche mince, causée par la déchirure des veines de pont. Hématome epi-dural a l’apparence biconvex, lenticulaire. Types d’hernie: transfalcine, transtentoriale. Triade de l’hernie unciforme: Dilatation de la pupille, hémiplegie, coma. 55.")
56
e

57
sa

58
sd

59
sa

60
e

61
S-c

62
e

63
Sd-C+A

64
e

65
sa

66
Same sa - pontine

67
Merci Questions?

Présentations similaires





















>")
