Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Les antiplaquettaires
26/03/2017 Séminaire thromboses et antithrombotiques Les antiplaquettaires Ludovic DROUET (Angio-Hématologie, Hôpital Lariboisière-Paris) 12-13 Mai 2006
 Mai")
2
26/03/2017 Les plaquettes ne peuvent arriver en grand nombre sur les zones lésées que si elles ont une énergie cinétique suffisante. Cette énergie leur est communiquée par la vitesse du sang et les mouvements rotatifs des globules rouges pris dans ce flux. Comme flux rapide = flux artériel, les antiplaquettaires ne sont indiqués que des les pathologies thrombotiques où les plaquettes sont prioritairement impliquées c’est à dire en pathologie artérielle ou valvulaire.

3
26/03/2017 ADP TX Jusqu’à présent n’ont été développés que trois classes d’antiplaquettaires. les inhibiteurs du système des prostaglandines Les inhibiteurs de la voie de l’ADP Les antagonistes des glycoprotéines GP IIb/IIIa On n’a pas développé par exemple d’inhibiteur de l’adhésion plaquettaire en pensant qu’ils seraient trop puissamment pro-hémorragiques

4
ASA AA Cox Thromboxane A2 26/03/2017
L’inhibition de la voie des thromboxanes se fait en pratique essentiellement par l’inhibition de la cyclo-oxygénase (Cox). Les plaquettes sont équipées d’un sous type de Cox: la Cox1. Les anti Cox2 (utilisés comme anti-inflammatoires) n’ont donc pas d’effet antiplaquettaire L’anti Cox (inhibant sans distinction la Cox1 et la Cox 2) de loin la plus utilisée est l’aspirine. Elle agit en acétylant de manière irréversible le site actif de l’enzyme Cox. La dose minimale d’aspirine à utiliser est de 75 mg par jour mais on parle de plus en plus de résistance à l’aspirine ce qui fait utiliser des doses un peu plus fortes (100, 150, 250, ou 320 mg) pour celles commercialisées en France comme antiplaquettaires (les doses plus fortes sont utilisées comme anti-inflammatoires). L’aspirine est rapidement absorbée par voie digestive et donc rapidement active (si la dose est suffisante d’ou la dose de initiale de 500 mg souvent donnée en cardiologie d’urgence) La muqueuse gastrique est aussi équipée d‘une Cox1. Cette l’inhibition explique la toxicité gastrique de l’aspirine. Actuellement de nouvelles molécules en particulier antagonistes des récepteurs à la Thromboxane A2 ( ) sont en développement.
. Les plaquettes sont équipées d’un sous type de Cox: la Cox1. Les anti Cox2 (utilisés comme anti-inflammatoires) n’ont donc pas d’effet antiplaquettaire. L’anti Cox (inhibant sans distinction la Cox1 et la Cox 2) de loin la plus utilisée est l’aspirine. Elle agit en acétylant de manière irréversible le site actif de l’enzyme Cox. La dose minimale d’aspirine à utiliser est de 75 mg par jour mais on parle de plus en plus de résistance à l’aspirine ce qui fait utiliser des doses un peu plus fortes (100, 150, 250, ou 320 mg) pour celles commercialisées en France comme antiplaquettaires (les doses plus fortes sont utilisées comme anti-inflammatoires). L’aspirine est rapidement absorbée par voie digestive et donc rapidement active (si la dose est suffisante d’ou la dose de initiale de 500 mg souvent donnée en cardiologie d’urgence) La muqueuse gastrique est aussi équipée d‘une Cox1. Cette l’inhibition explique la toxicité gastrique de l’aspirine. Actuellement de nouvelles molécules en particulier antagonistes des récepteurs à la Thromboxane A2 ( ) sont en développement.")
5
thienopyridines ADP 26/03/2017
L’autre voie de recrutement plaquettaire physiologiquement très impliquée et utilisée comme cible d’antiplaquettaire est la voie de l’ADP. Les thiénopyridines (ticlopidine (Ticlid®) clopidogrel Plavix ®) sont des prodrogues dont un métabolite hépatique est un antagoniste irréversible des récepteurs (P2Y12). Les thiénopyridines sont des prodrogues elles ont une efficacité thérapeutique largement démontrée mais il faut plusieurs jours pour que cette efficacité s’installe. On essai de contourner ce retard en utilisant de très fortes doses de charge initiale. De nouvelles molécules (d’autres familles moléculaires mais toujours inhibitrices du P2Y12) ( ) sont actuellement en cours de développement.
 clopidogrel Plavix ®) sont des prodrogues dont un métabolite hépatique est un antagoniste irréversible des récepteurs (P2Y12). Les thiénopyridines sont des prodrogues elles ont une efficacité thérapeutique largement démontrée mais il faut plusieurs jours pour que cette efficacité s’installe. On essai de contourner ce retard en utilisant de très fortes doses de charge initiale. De nouvelles molécules (d’autres familles moléculaires mais toujours inhibitrices du P2Y12) ( ) sont actuellement en cours de développement.")
6
thienopyridines ASA AA Cox Thromboxane A2 ADP 26/03/2017
La complémentarité fonctionnelle des voies de la thromboxane A2 et de l’ADP expliquent l’efficacité particulièrement intéressante cliniquement de l’association clopidogrel (Plavix®) + aspirine.
 + aspirine.")
7
Fibrinogène GPIIb GPIIIa 26/03/2017
Les glycoprotéines de membrane GPIIbIIIa sont normalement en configuration non activée ( ). Sous forme activée (après activation plaquettaires ( ) elles lient avec une forte affinité le fibrinogène ( ). La constitution des ponts moléculaires GPIIb/IIIa - fibrinogène - GPIIb/IIIa ( ) réalise le lien physique qui relie les plaquettes dans l’agrégat plaquettaire. L’antagonisme des récepteurs GPIIb/IIIa réalise donc une véritable inhibition de l’agrégation plaquettaire (alors que l’inhibition de la voie des thromboxane ou de l’ADP réalise plutôt une inhibition du recrutement plaquettaire.)
. Sous forme activée (après activation plaquettaires ( ) elles lient avec une forte affinité le fibrinogène ( ). La constitution des ponts moléculaires GPIIb/IIIa - fibrinogène - GPIIb/IIIa ( ) réalise le lien physique qui relie les plaquettes dans l’agrégat plaquettaire. L’antagonisme des récepteurs GPIIb/IIIa réalise donc une véritable inhibition de l’agrégation plaquettaire (alors que l’inhibition de la voie des thromboxane ou de l’ADP réalise plutôt une inhibition du recrutement plaquettaire.)")
8
26/03/2017 PAR Thrombine IIa La thrombine enzyme final de la coagulation est aussi le plus puissant activateur des plaquettes. Elle agit par des récepteurs spécifiques les PAR (Protease Activated Receptor) (r). Les inhibiteurs directes de thrombine en plus d’être des anticoagulants inhibent aussi cette voie. Actuellement des essais se font sur des antagonistes de PAR (ne pas confondre avec les Ppar).
 (r). Les inhibiteurs directes de thrombine en plus d’être des anticoagulants inhibent aussi cette voie. Actuellement des essais se font sur des antagonistes de PAR (ne pas confondre avec les Ppar).")
9
Prévenir les thromboses
26/03/2017 Prévenir les thromboses Artère Athérosclérose HTA, Hyper cholestérolémie, Tabac,… ANTI-AGREGANTS PLAQUETTAIRES A vie Veine Immobilisation +++ ANTICOAGULANTS Tant que le risque persiste Lutter contre les facteurs de risque Agir sur le principal mécanisme en cause

10
Traiter les thromboses
26/03/2017 Traiter les thromboses Artère Angioplastie Veine (Thrombectomie) Désobstruer le vaisseau (si risque vital ou organique majeur) Empêcher l’extension, prévenir la récidive THROMBOLYTIQUES Antiagrégants ANTICOAGULANTS
 Désobstruer le vaisseau (si risque vital ou organique majeur) Empêcher l’extension, prévenir la récidive. THROMBOLYTIQUES. Antiagrégants. ANTICOAGULANTS.")
11
AAP : principales indications
26/03/2017 AAP : principales indications Prévention artérielle ++ prévention au long cours des complications ischémiques (thrombotiques) « l’athérothrombose » prévention primaire, prévention secondaire et prévention primo-secondaire après un premier accident (IDM, angor instable, AVC,etc...) ASPIRINE, (TICLID), PLAVIX : administration orale Phase aiguë des syndromes coronaires Angor instable Angioplasties ASPIRINE, (TICLID) PLAVIX (+ASPIRINE) : administration orale Anti GPIIb IIIa : perfusion IV Post angioplastie + stenting coronaire Autres territoires Durée < 12 mois (Plavix+aspirine)
 « l’athérothrombose » prévention primaire, prévention secondaire et prévention primo-secondaire. après un premier accident (IDM, angor instable, AVC,etc...) ASPIRINE, (TICLID), PLAVIX : administration orale. Phase aiguë des syndromes coronaires. Angor instable. Angioplasties. ASPIRINE, (TICLID) PLAVIX (+ASPIRINE) : administration orale. Anti GPIIb IIIa : perfusion IV. Post angioplastie + stenting. coronaire. Autres territoires. Durée < 12 mois (Plavix+aspirine)")
12
Fbg NO ADP NO NO PGI2 TXA2 IIb IIb pS IIIa IIIa IIb IIIa IIb IIIa vWF
Calcium NO IIb IIIa IIb IIIa vWF FVIIIc ADP Fbg IIb IIIa IIb IIIa TXA2 vWF NO pS COX1 NO Calcium PGI2 FcgRII V Ia IX TM IIa Ib vWF Collagène TISSU CONJONCTIF

13
26/03/2017 ADP TX Jusqu’à présent n’ont été développés que trois classes d’antiplaquettaires. les inhibiteurs du système des prostaglandines Les inhibiteurs de la voie de l’ADP Les antagonistes des glycoprotéines GP IIb/IIIa On n’a pas développé par exemple d’inhibiteur de l’adhésion plaquettaire en pensant qu’ils seraient trop puissamment pro-hémorragiques

14
Catella-Lawson F, Fitzgerald GA & al, NEJM, 2001

15
Antiplatelet Therapy on vascular events (MI, stroke or vascular death)
Antithrombotic Trialists' Collaboration, Meta.analysis of antiplatelet therapy for prevention of death, MI, stroke, BMJ, 2002

16
Antiplatelet therapy on vascular events in 195 trials in high risk patients f(disease) –ATC BMJ 2002-
 –ATC BMJ 2002-")
17
1.00 - 0.99 - 0.98 - 0.97 - 0.96 - 0.95 - 0.94 - 0.93 - 0.92 - 0.91 - 0.90 Aspirin No Diabetes No Aspirin No Diabetes Aspirin Diabetes No Aspirin Diabetes Log-Rank Test No Diabetes x’=4.98 p-value = 0.03 Log-Rank Test Diabetes x’=0.13 p-value = 0.71 Time (years) Primary Prevention of Cardiovascular Events With Low-Dose aspirin and Vitamin E in Type 2 Diabetic Patients, Results of the Primary Prevention Project (PPP) trial M. SACCO,et al Diabetes Care 26:3264–3272, 2003
 Primary Prevention of Cardiovascular Events With Low-Dose aspirin and Vitamin E in Type 2 Diabetic Patients, Results of the Primary Prevention Project (PPP) trial. M. SACCO,et al Diabetes Care 26:3264–3272,")
18
Antiagrégants plaquettaires
L’aspirine a-t-elle une place en prévention de la thrombose veineuse

19
Aspirine & Thrombose veineuse
PEP Study Lancet 2000; 355:1295

20
Anti agrég(e)ant plaquettaire
L’aspirine en pathologie artérielle atherothrombotique: « oui » mais quelle(s) dose(s) ? En phase chronique À la phase aiguë
 dose(s) En phase chronique. À la phase aiguë.")
21
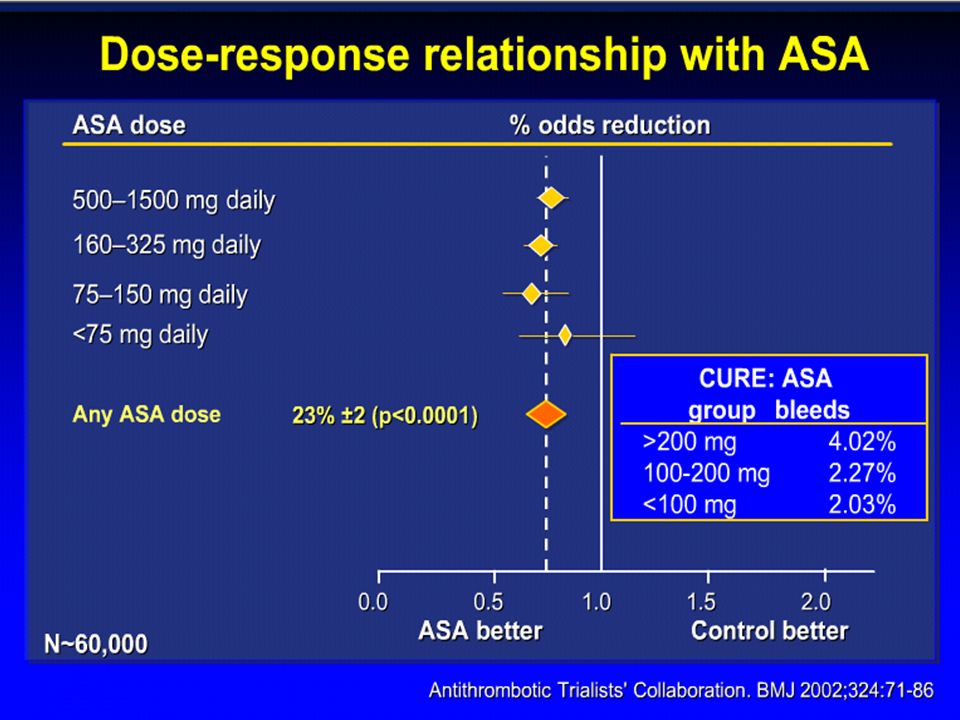
Indirect comparisons of aspirin dosages on vascular events in high risk patients (excluding those with acute stroke) Antithrombotic Trialists' Collaboration, Meta.analysis of antiplatelet therapy for prevention of death, MI, stroke, BMJ, 2002

23
démontré une efficacité
PATHOLOGIE Dose minimale d’aspirine (mg)ayant démontré une efficacité Hommes à haut risque cardiovasculaire 75 Hypertendus Angor stable Angor instable Infarctus aigu du myocarde 160 Accidents vasculaires cérébraux ischémiques (constitués et transitoires) 50 Sténose sévère de la carotide Accidents vasculaires cérébraux ischémiques constitués (période aiguë)
ayant. démontré une efficacité. Hommes à haut risque cardiovasculaire. 75. Hypertendus. Angor stable. Angor instable. Infarctus aigu du myocarde Accidents vasculaires cérébraux ischémiques. (constitués et transitoires) 50. Sténose sévère de la carotide. Accidents vasculaires cérébraux ischémiques constitués (période aiguë)")
24
Aspirine: une notion nouvelle la résistance à l’aspirine
Définition de la résistance : clinique / biologique Observance Interactions médicamenteuses Dose(s)
")
25
Catella-Lawson F, Fitzgerald GA & al, NEJM, 2001

26
Résistance à l’aspirine
Le modèle exemplaire des assistances cardio-circulatoires chroniques Nombre de patients présentant une agrégation plaquettaire - activation par l'AA- Doses d'aspirine par jour 500 Dose de départ : 250 mg 400 3 300 2 2 200 1 1 100 2 4 6 8 10 12 Semaines de suivi post implantation

27
Aspirine: les effets secondaires
Toxicité digestive Gastralgies Hémorragies digestives Allergie

28
CAPRIE : safety events incidence (%) Aspirin Plavix 325 mg/j 75 mg/j P
(n = 9 586) (n = 9 599) Hemorrhages (all bleedings) GI other intra-cranial 9,3 2,7 6,5 0,5 9,3 2,0 7,3 0,4 0,976 0,002 0,024 0,146 GI symptoms (all events) GI ulcers diarrheas severe diarrheas 29,8 1,2 3,4 0,1 27,8 0,7 4,5 0,2 0,001 0,001 0,05 Blood count abnormalities severe Neutropenia(<0,45 x 10 9) severe Thrombopenia (<80 x 10 9) 0,02 0,1 0,04 0,2 0,4 0,255 Other adverse effects headaches, vertigos skin severe rashes severe itching 23,8 13,1 0,07 22,3 15,8 0,13 0,016 0,001 0,05 Eur Heart J 1998
 (n = 9 599) Hemorrhages (all bleedings) GI. other. intra-cranial. 9,3. 2,7. 6,5. 0,5. 9,3. 2,0. 7,3. 0,4. 0,976. 0,002. 0,024. 0,146. GI symptoms (all events) GI ulcers. diarrheas. severe diarrheas. 29,8. 1,2. 3,4. 0,1. 27,8. 0,7. 4,5. 0,2. 0,001. 0,001. 0,05. Blood count abnormalities. severe Neutropenia(<0,45 x 10 9) severe Thrombopenia (<80 x 10 9) 0,02. 0,1. 0,04. 0,2. 0,4. 0,255. Other adverse effects. headaches, vertigos. skin. severe rashes. severe itching. 23,8. 13,1. 0,07. 22,3. 15,8. 0,13. 0,016. 0,001. 0,05. Eur Heart J")
29
Clopidogrel Plavix® prodrogue
active metabolite: Identified , very short half live Acts by irreversible SS bridges with P2Y12 receptor (one the 3 platelet ADP receptors)
")
30
ADP binds to its receptor
Platelet ADP pathway ADP binds to its receptor ADP ADP P2Y12 P2Y1 ADP Adenylate cyclase activity down-regulated G AC PlC P2X1 calcium channel a Dense granule Ca2+ ADP Secretion Ca2+ released from intracellular stores ADP Conformational change activates GPIIb IIIa receptor Fibrinogen binds to its receptor

31
Mean ( SEM) inhibition of platelet aggregation induced by 5µM
Clopidogrel: Kinetics of antiplatelet activity Mean ( SEM) inhibition of platelet aggregation induced by 5µM + - 80 *** ** *** *** *** 60 *** *** ** ** ** * ** 40 * * % Inhibition 20 -20 Placebo 50 mg 75 mg 100 mg Ticlopidine -40 Day 2 Day 3 Day 7 Day 15 * p < 0.05; ** p < 0.01; *** p < 0.001
 inhibition of platelet aggregation induced by 5µM *** ** *** *** *** 60. *** *** ** ** ** * ** 40. * * % Inhibition Placebo. 50 mg. 75 mg. 100 mg. Ticlopidine Day 2 Day 3 Day 7 Day 15. * p < 0.05; ** p < 0.01; *** p <")
32
Inhibition (%) platelet aggregation ADP 5 µM
Kinetics of antiplatelet activity of clopidogrel 75 mg/d for 8d in healthy volunteers (n=12) Inhibition (%) platelet aggregation ADP 5 µM Before daily Clopidogrel intake 3 hours after daily Clopidogrel intake D D D D D8 time
 Inhibition (%) platelet aggregation ADP 5 µM. Before daily Clopidogrel intake. 3 hours after daily Clopidogrel intake. D1 D2 D3 D5 D8. time.")
33
Clopidogrel loading dose
26/03/2017 Draft 3 Clopidogrel loading dose Bleeding time % platelet inhibition 2 * * Bleeding time * * 1 300 mg SLIDE 29 The pharmacodynamic characteristics of a loading dose of clopidogrel were reported by several authors As an example, this study indicated that maximal antiplatelet activity of clopidogrel (similar to those observed at steady state after 3-7 days of 75 mg of clopidogrel once a day), occurs rapidly, within 2 hours of administration when 300 mg to 600 mg are used There is no increase of bleeding time at 300mg as compared to 75 mg. Additional studies have determined that a loading dose of 300 mg to 400 mg is appropriate for initiating antiplatelet therapy with clopidogrel when rapid activity is necessary. Kleffer G et al. Thromb Haemost 1989;62(1):411 (Abstract)
, occurs rapidly, within 2 hours of administration when 300 mg to 600 mg are used. There is no increase of bleeding time at 300mg as compared to 75 mg. Additional studies have determined that a loading dose of 300 mg to 400 mg is appropriate for initiating antiplatelet therapy with clopidogrel when rapid activity is necessary. Kleffer G et al. Thromb Haemost 1989;62(1):411 (Abstract)")
34
Clopidogrel: loading dose
300 mg n=20 75 mg 75 mg n=20 300 mg n=20 Inhibition (%) platelet aggregation ADP 5 µM
 platelet aggregation ADP 5 µM.")
35
CAPRIE : safety events incidence (%) Aspirin Plavix 325 mg/j 75 mg/j P
(n = 9 586) (n = 9 599) Hemorrhages (all bleedings) GI other intra-cranial 9,3 2,7 6,5 0,5 9,3 2,0 7,3 0,4 0,976 0,002 0,024 0,146 GI symptoms (all events) GI ulcers diarrheas severe diarrheas 29,8 1,2 3,4 0,1 27,8 0,7 4,5 0,2 0,001 0,001 0,05 Blood count abnormalities severe Neutropenia(<0,45 x 10 9) severe Thrombopenia (<80 x 10 9) 0,02 0,1 0,04 0,2 0,4 0,255 Other adverse effects headaches, vertigos skin severe rashes severe itching 23,8 13,1 0,07 22,3 15,8 0,13 0,016 0,001 0,05 Eur Heart J 1998
 (n = 9 599) Hemorrhages (all bleedings) GI. other. intra-cranial. 9,3. 2,7. 6,5. 0,5. 9,3. 2,0. 7,3. 0,4. 0,976. 0,002. 0,024. 0,146. GI symptoms (all events) GI ulcers. diarrheas. severe diarrheas. 29,8. 1,2. 3,4. 0,1. 27,8. 0,7. 4,5. 0,2. 0,001. 0,001. 0,05. Blood count abnormalities. severe Neutropenia(<0,45 x 10 9) severe Thrombopenia (<80 x 10 9) 0,02. 0,1. 0,04. 0,2. 0,4. 0,255. Other adverse effects. headaches, vertigos. skin. severe rashes. severe itching. 23,8. 13,1. 0,07. 22,3. 15,8. 0,13. 0,016. 0,001. 0,05. Eur Heart J")
36
TTP : clinical Experience since beginning of commercialization
26/03/2017 TTP : clinical Experience since beginning of commercialization 20 TTP cases reported on more than 4,7 millions patients treated with PLAVIX. Incidence supposée : 1 / Incidence similar to that of general population Causality to be established No need for systematic blood count monitoring D ’ exceptionnels cas de PTT ont été rapportés sous Plavix depuis sa mise sur le marché. A ce jour, sans qu ’une imputabilité certaine ait été prouvée, 20 cas ont été répertoriés sur plus de 4, 7 million de patients traités dans le monde (4,2 cas par million d ’habitants).Cette incidence est très peu différente (si tous les cas sont bien imputables à PLAVIX) de celle des PTT dans la population générale (3, 2 cas par million d ’habitants). (rappeler les mentions légales) Diapositive de backup à n ’utiliser que lors d ’une objection sur la survenue de PTT sous PLAVIX ou de la nécessité de pratiquer une surveillance hématologique.
.Cette incidence est très peu différente (si tous les cas sont bien imputables à PLAVIX) de celle des PTT dans la population générale (3, 2 cas par million d ’habitants). (rappeler les mentions légales) Diapositive de backup à n ’utiliser que lors d ’une objection sur la survenue de PTT sous PLAVIX ou de la nécessité de pratiquer une surveillance hématologique.")
37
Atherothrombose Evolution des traitements antiplaquettaires

38
Aspirin prevents ¼ of ischemic cardio-vascular events
26/03/2017 Aspirin prevents ¼ of ischemic cardio-vascular events 160 Placebo arm extrapolated from APTC meta-analysis. Antiplatelet Trialists’ Collaboration. BMJ 1994;308:81-106, . Placebo 120 Aspirin 80 nb events/1000 patients/year 25% 40 3 6 9 12 15 18 21 24 27 30 33 36 Time since randomisation (mois) Can an antiplatelet agent be more efficacious? Cette diapositive permet de faire le lien entre : La thérapeutique actuellement la plus employée dans la prévention des récidives (aspirine), mais qui ne permet de n’en prévenir qu’un quart (APTC 94). La nécessité de développer d’autres anti-agrégants plus efficaces et aussi bien tolérés.
 Can an antiplatelet agent be more efficacious Cette diapositive permet de faire le lien entre : La thérapeutique actuellement la plus employée dans la prévention des récidives (aspirine), mais qui ne permet de n’en prévenir qu’un quart (APTC 94). La nécessité de développer d’autres anti-agrégants plus efficaces et aussi bien tolérés.")
39
A unique disease with multiple localizations
CAPRIE’s patients n = Cerebrovascular Disease n = 6431 CHD n = 6302 24.7% 7.4% 29.9% 3.3% 3.8% 11.8% Atherothrombosis A unique disease with multiple localizations 19.2% PAD n = 6452 Coccheri. Eur Heart J 1998;19(suppl):P1268.
:P1268.")
40
CAPRIE : Results analysis
As inclusion criteria: As real medical history : 7,3 8,4 Ischemic stroke Ischemic stroke n = 6431 n = 6953 -3,7 7.4 MI MI n = 6302 n = 8446 23,8 22,4 PAD PAD n = 6452 n = 7325 8.7 8.7 All patients All patients n = n = 20 10 10 20 30 20 10 10 20 30 Plavix better Plavix better CAPRIE Steering Committee. Lancet 1996;348: Gent M. Benefit of clopidogrel in patients with coronary disease Circulation 1997, 96(8) supplt Rupprecht HJ. Consistency of the benefit of clopidogrel across a range of vascular related endpoints: results from CAPRIE. European Society of Cardiology, 1998, Vienne (abstract 53116)
 supplt. Rupprecht HJ. Consistency of the benefit of clopidogrel across a range of vascular related endpoints: results from CAPRIE. European Society of Cardiology, 1998, Vienne (abstract 53116)")
41
CAPRIE Study: MI Paradox
26/03/2017 CAPRIE Study: MI Paradox Relative Risk Reduction* by Qualifying Entry Criteria1 Relative Risk Reduction of Individual End Points 7.3 5.2 n=19,185 IS n=6431 MI n=6302 PAD n=6452 Total n=19185 IS (fatal or non-fatal)2 -3.7 19.2 MI (fatal or non-fatal)3 23.8 7.6 Vascular death1 8.7 8.7 IS, MI, vascular death1 20 10 10 20 30 20 10 10 20 30 Slide 15 The relative risk reductions of clopidogrel versus aspirin in the subgroups defined by CAPRIE entry criteria are shown in the left panel of this slide.1 These findings may suggest a disparity of effect between the entry criteria subgroups. However, CAPRIE was not powered to detect treatment differences between subgroups. Because of the apparent lack of consistency among the subgroups, a specific analysis was performed to check the consistency of the benefit of clopidogrel for each component of the outcome cluster: ischemic stroke (IS), myocardial infarction (MI), and vascular death. This analysis showed consistency: for the overall population, clopidogrel reduced the risk of ischemic stroke by 5.2%,2 the risk of MI (fatal or non-fatal) by 19.2%,3 and the risk of vascular death by 7.6%.1 The benefit was consistent for the various components of the primary outcome cluster, the benefit being greatest for myocardial infarction (relative risk reduction = 19.2%; p=0.008).3 1. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996;348: 2. Easton JD. Benefit of clopidogrel in patients with evidence of cerebrovascular disease. Neurology 1998;50(suppl 4):A157. 3. Gent M. Benefit of clopidogrel in patients with coronary disease. Circulation 1997;96(suppl):I-467. clopidogrel better clopidogrel better *Cluster of IS, MI, or vascular death. 1CAPRIE Steering Committee. Lancet 1996;348: 2Easton. Neurology 1998;50(suppl 4):A157. 3Gent. Circulation. 1997;96(suppl):I-467.
 MI (fatal or non-fatal) Vascular death IS, MI, vascular death Slide 15. The relative risk reductions of clopidogrel versus aspirin in the subgroups defined by CAPRIE entry criteria are shown in the left panel of this slide.1 These findings may suggest a disparity of effect between the entry criteria subgroups. However, CAPRIE was not powered to detect treatment differences between subgroups. Because of the apparent lack of consistency among the subgroups, a specific analysis was performed to check the consistency of the benefit of clopidogrel for each component of the outcome cluster: ischemic stroke (IS), myocardial infarction (MI), and vascular death. This analysis showed consistency: for the overall population, clopidogrel reduced the risk of ischemic stroke by 5.2%,2 the risk of MI (fatal or non-fatal) by 19.2%,3 and the risk of vascular death by 7.6%.1 The benefit was consistent for the various components of the primary outcome cluster, the benefit being greatest for myocardial infarction (relative risk reduction = 19.2%; p=0.008) CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet 1996;348: Easton JD. Benefit of clopidogrel in patients with evidence of cerebrovascular disease. Neurology 1998;50(suppl 4):A Gent M. Benefit of clopidogrel in patients with coronary disease. Circulation 1997;96(suppl):I-467. clopidogrel better. clopidogrel better. *Cluster of IS, MI, or vascular death. 1CAPRIE Steering Committee. Lancet 1996;348: Easton. Neurology 1998;50(suppl 4):A157. 3Gent. Circulation. 1997;96(suppl):I-467.")
42
26/03/2017 CAPRIE: Amplified Benefit of Clopidogrel in Patients with Higher Vascular Risk1–3 Incidence of MI, IschemicStroke, or Vascular Death Events Prevented/1000 Patients/Year over ASA 152 200 238 141 172 204 50 100 150 250 300 All CAPRIE patients¹ (n=19,825) Prior history of any ischemic event² (n=8,854) Prior history of major acute event (MI or stroke) (n=4,496) Incidence/1000 patients (average follow-up, 2 years) ASA Clopidogrel 11 28 34 3 In CAPRIE,1 8,854 patients had a prior history of any ischemic event, and of these 4,496 had a history of a major acute event – a myocardial infarction or a stroke.1 The annual incidence per 1,000 patients was reduced in the clopidogrel group vs the ASA group by 34 in patients with a prior history of a major acute event, and by 28 in those with a prior history of any ischemic event, compared with 11 in the overall population.1,2 The benefits of clopidogrel over ASA were amplified in the higher vascular risk group.3 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329– Jarvis B, Simpson K. Drugs 2000; 60: 347– Ringleb PA et al. Eur Heart J 1999; 20: 666. References: 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329–39. 2. Jarvis B, Simpson K. Drugs 2000; 60: 34–77. 3. Ringleb PA. Eur Heart J 1999; 20: 666.
 Prior history of any. ischemic event². (n=8,854) Prior history of major. acute event (MI or stroke) (n=4,496) Incidence/1000 patients (average follow-up, 2 years) ASA. Clopidogrel In CAPRIE,1 8,854 patients had a prior history of any ischemic event, and of these 4,496 had a history of a major acute event – a myocardial infarction or a stroke.1. The annual incidence per 1,000 patients was reduced in the clopidogrel group vs the ASA group by 34 in patients with a prior history of a major acute event, and by 28 in those with a prior history of any ischemic event, compared with 11 in the overall population.1,2. The benefits of clopidogrel over ASA were amplified in the higher vascular risk group CAPRIE Steering Committee. Lancet 1996; 348: 1329– Jarvis B, Simpson K. Drugs 2000; 60: 347– Ringleb PA et al. Eur Heart J 1999; 20: 666. References: 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329– Jarvis B, Simpson K. Drugs 2000; 60: 34– Ringleb PA. Eur Heart J 1999; 20: 666.")
43
Events Prevented/1000 Patients/Year over ASA
CAPRIE: Amplified Benefit of Clopidogrel in Patients with Hypercholesterolemia1 26/03/2017 Incidence of Myocardial Infarction, Stroke, Vascular Death or Hospitalization for Ischemic Events or Bleeding Events Prevented/1000 Patients/Year over ASA Overall benefit: p = 0.026; multivariate analysis 15.1% 14.6% 12.2% 11.9% 2 4 6 8 10 12 14 16 On any lipid-lowering agent On statin * Annual event rate (%) ASA Clopidogrel 29 27 Hypercholesterolemia is a major risk factor for atherothrombotic events. Patients with symptomatic atherothrombosis and hypercholesterolemia represent a high-risk cohort, and lipid-lowering agents (particularly statins) are of proven benefit. In CAPRIE, there were 1,080 hypercholesterolemic patients who received lipid-lowering therapy and were randomized to clopidogrel, and 1,014 patients to ASA. For patients who received any lipid-lowering agent, event rates for the combined endpoint* were ASA, 14.6% and clopidogrel, 11.9%. Patients who received statins, the corresponding event rates were ASA, 15.1% and clopidogrel, 12.2%. These data show that the benefit of clopidogrel vs ASA is consistent with the overall analyses, and this benefit is complementary and additive to the benefit provided by lipid-lowering agents. Thus, the benefit of clopidogrel is amplified, with 27 additional events prevented (per 1,000 patient/year) in patients on any lipid-lowering agent and 29 in those taking statins. *Myocardial infarction, ischemic stroke, vascular death, or rehospitalization for ischemia/ bleeding 1. Bhatt DL et al. J Am Coll Cardiol 2000; 35(suppl A): 326. Reference: 1. Bhatt DL et al. J Am Coll Cardiol 2000; 35(suppl A): 383A.
 ASA. Clopidogrel Hypercholesterolemia is a major risk factor for atherothrombotic events. Patients with symptomatic atherothrombosis and hypercholesterolemia represent a high-risk cohort, and lipid-lowering agents (particularly statins) are of proven benefit. In CAPRIE, there were 1,080 hypercholesterolemic patients who received lipid-lowering therapy and were randomized to clopidogrel, and 1,014 patients to ASA. For patients who received any lipid-lowering agent, event rates for the combined endpoint* were ASA, 14.6% and clopidogrel, 11.9%. Patients who received statins, the corresponding event rates were ASA, 15.1% and clopidogrel, 12.2%. These data show that the benefit of clopidogrel vs ASA is consistent with the overall analyses, and this benefit is complementary and additive to the benefit provided by lipid-lowering agents. Thus, the benefit of clopidogrel is amplified, with 27 additional events prevented (per 1,000 patient/year) in patients on any lipid-lowering agent and 29 in those taking statins. *Myocardial infarction, ischemic stroke, vascular death, or rehospitalization for ischemia/ bleeding. 1. Bhatt DL et al. J Am Coll Cardiol 2000; 35(suppl A): 326. Reference: 1. Bhatt DL et al. J Am Coll Cardiol 2000; 35(suppl A): 383A.")
44
Events Prevented/1000 Patients/Year over ASA
26/03/2017 CAPRIE: Amplified Benefit of Clopidogrel in Patients with Additional Risk Factors1, 2 Incidence of Myocardial Infarction, Stroke, Vascular Death or Hospitalization for Ischemic Events or Bleeding Events Prevented/1000 Patients/Year over ASA 137 177 215 126 156 50 100 150 200 250 All CAPRIE patients¹ Diabetes² Diabetes treated with insulin² Incidence/1000 patients/year ASA Clopidogrel 11 21 38 In CAPRIE, 3,837 patients had co-existing diabetes.1 These patients are at higher risk of myocardial infarction, ischemic stroke, vascular death or hospitalization for ischemic events/bleeding (17.7% diabetic vs 12.7% non-diabetic in the ASA group; 15.6% diabetic vs 11.8% non-diabetic in the clopidogrel group).2,3 The annual event incidence per 1,000 patients was reduced in the clopidogrel group vs the ASA group: by 38 in patients receiving insulin at baseline, 21 in diabetic patients who were not receiving insulin, compared with 11 in the overall CAPRIE population. The benefits of clopidogrel over ASA were amplified in the higher risk, insulin-dependent patients. 1. Bhatt DL et al. Am Heart J 2000; 140: 67– Jarvis B, Simpson K. Drugs 2000; 60: 347–77. References: 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329–39. 2. Jarvis B, Simpson K. Drugs 2000; 60: 347–77. 3. Bhatt DL et al. Am Heart J 2000; 140: 67–73.
.2,3. The annual event incidence per 1,000 patients was reduced in the clopidogrel group vs the ASA group: by 38 in patients receiving insulin at baseline, 21 in diabetic patients who were not receiving insulin, compared with 11 in the overall CAPRIE population. The benefits of clopidogrel over ASA were amplified in the higher risk, insulin-dependent patients. 1. Bhatt DL et al. Am Heart J 2000; 140: 67– Jarvis B, Simpson K. Drugs 2000; 60: 347–77. References: 1. CAPRIE Steering Committee. Lancet 1996; 348: 1329– Jarvis B, Simpson K. Drugs 2000; 60: 347– Bhatt DL et al. Am Heart J 2000; 140: 67–73.")
45
Atherothrombosis is a Generalized Disease
Symptomatic occlusion Acute Syndromes coronaries cerebrovascular peripheral Occlusive thrombus ± permanent PLAQUE RUPTURE / erosion LOCAL Silent occlusion DISTAL Parietal thrombus EVOLUTION Asymptomatic Fatty streak Plaque PLAQUE RUPTURE / erosion Progressive destruction of the downstream capillary bed myocardium brain peripheral tissues

46
Event Rates (% Death, MI, Revasc.)
26/03/2017 Ticlid + aspirin for prevention of subacute thrombosis on coronary stents 12 ASA Coumadin + ASA Ticlopidine + ASA 11 P=0.01 P=0.07 8.3 8 P=0.01 Event Rates (% Death, MI, Revasc.) 6.2 5.7 5.6 P<0.001 4 3.6 2.7 1.6 0.5 ISAR 1 N=517 FANTASTIC 2 N=485 MATTIS 3 N=350 STARS 4 N=1653 Benefit of ticlopidine in coronary stenting Shown here are data on event rates for the composite endpoint of death/MI/revascularization at 30 days’ follow-up for the ISAR,1 FANTASTIC,2 STARS3 and MATTIS4 studies. In ISAR and STARS, only patients with successful stent implantation were randomized, whereas in FANTASTIC and MATTIS, patients with successful implantation or suboptimal results were included. The data clearly demonstrate the clinical benefit of an ADP receptor antagonist plus aspirin, compared with aspirin alone or aspirin plus full anticoagulation following coronary stenting. 1Schomig A et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med 1996;334:1084–1089. 2Bertrand ME et al. Randomized multicenter comparison of conventional anticoagulation versus antiplatelet therapy in unplanned and elective coronary stenting. The full anticoagulation versus aspirin and ticlopidine (FANTASTIC) study. Circulation 1998;98:1597–1603. 3Leon MB et al. A clinical trial comparing three antithrombotic drug regimens after coronary artery stenting. N Engl J Med 1998;339:1665–1671. 4Urban P et al. Randomized evaluation of anticoagulation versus antiplatelet therapy after coronary stent implantation in high-risk patients. The multicenter aspirin and ticlopidine trial after intracoronary stenting (MATTIS). Circulation 1998;98:2126–2132. 1 Schömig et al. (1996), 2 Bertrand et al. (1998), 3 Urban (1998), 4 Leon et al. (1998)
 P< ISAR 1. N=517. FANTASTIC 2. N=485. MATTIS 3. N=350. STARS 4. N=1653. Benefit of ticlopidine in coronary stenting. Shown here are data on event rates for the composite endpoint of death/MI/revascularization at 30 days’ follow-up for the ISAR,1 FANTASTIC,2 STARS3 and MATTIS4 studies. In ISAR and STARS, only patients with successful stent implantation were randomized, whereas in FANTASTIC and MATTIS, patients with successful implantation or suboptimal results were included. The data clearly demonstrate the clinical benefit of an ADP receptor antagonist plus aspirin, compared with aspirin alone or aspirin plus full anticoagulation following coronary stenting. 1Schomig A et al. A randomized comparison of antiplatelet and anticoagulant therapy after the placement of coronary-artery stents. N Engl J Med 1996;334:1084– Bertrand ME et al. Randomized multicenter comparison of conventional anticoagulation versus antiplatelet therapy in unplanned and elective coronary stenting. The full anticoagulation versus aspirin and ticlopidine (FANTASTIC) study. Circulation 1998;98:1597– Leon MB et al. A clinical trial comparing three antithrombotic drug regimens after coronary artery stenting. N Engl J Med 1998;339:1665– Urban P et al. Randomized evaluation of anticoagulation versus antiplatelet therapy after coronary stent implantation in high-risk patients. The multicenter aspirin and ticlopidine trial after intracoronary stenting (MATTIS). Circulation 1998;98:2126– Schömig et al. (1996), 2 Bertrand et al. (1998), 3 Urban (1998), 4 Leon et al. (1998)")
47
Patient Randomization
Clopidogrel 300mg loading dose Clopidogrel 75mg o.d. (6259 patients) Aspirin mg Patients with Acute Coronary Syndrome R 3 months £ double-blind treatment £ 12 months (UA or MI Without ST elevation) Aspirin mg Placebo 1 tab o.d. (6303 patients) Day 1 1 m. Visit 3 m. Visit 6 m. Visit 9 m. Visit 12 m. or Final Visit Placebo loading dose Discharge Visit R=Randomization N Engl J Med. 2001
 Aspirin mg. Patients with. Acute Coronary Syndrome. R. 3 months £ double-blind treatment £ 12 months. (UA or MI Without ST elevation) Aspirin mg. Placebo. 1 tab o.d. (6303 patients) Day 1. 1 m. Visit. 3 m. Visit. 6 m. Visit. 9 m. Visit. 12 m. or Final Visit. Placebo loading dose. Discharge Visit. R=Randomization. N Engl J Med")
48
Cure : Cumulative Hazard Rates for CV Death/MI/Stroke
0.14 11.4% Placebo +ASA 0.12 9.3% 0.10 Clopidogrel + ASA 0.08 Cumulative Hazard Rates Cumulative Hazard Rates 0.06 20% RRR P < 0.001 N = 12,562 0.04 0.02 P < 0.001 0.0 3 6 9 12 3 6 9 12 No of Pts Months of Follow-up Months of Follow-up Plac Clop 6303 6259 5780 5866 4664 4779 3600 3644 2388 2418 N Engl J Med. 2001

49
PCI-CURE: Study Design
26/03/2017 PCI-CURE: Study Design CURE PCI-CURE Pretreatment N=2,658 patients undergoing PCI Open-label thienopyridine PLACEBO + ASA N = 1345 Follow-up (to 12 m after rand.) PCI 30 d. post PCI* R Open-label thienopyridine CLOPIDOGREL + ASA N = 1313 This slide summarizes the PCI-CURE design. A total of 2658 patients with non-ST-elevation MI undergoing PCI were randomized to receive clopidogrel or placebo. The majority of patients received an intracoronary stent (81% placebo 82% clopidogrel). Patients were treated with the blinded study drug for a median of 6 days prior to the procedure. After the procedure the majority (>80%) received clopidogrel open-label for approximately 4 weeks, then the blinded study drug was continued for a average duration of 8 months. The primary endpoint was cardiovascular death, myocardial infarction or urgent vessel revascularization within 30 days of PCI. Pretreatment *1o Outcome: CV Death, MI, Urg Revasc. Mehta SR et al. Lancet 2001:358:527-33
 PCI. 30 d. post PCI* R. Open-label thienopyridine. CLOPIDOGREL. + ASA. N = This slide summarizes the PCI-CURE design. A total of 2658 patients with non-ST-elevation MI undergoing PCI were randomized to receive clopidogrel or placebo. The majority of patients received an intracoronary stent (81% placebo 82% clopidogrel). Patients were treated with the blinded study drug for a median of 6 days prior to the procedure. After the procedure the majority (>80%) received clopidogrel open-label for approximately 4 weeks, then the blinded study drug was continued for a average duration of 8 months. The primary endpoint was cardiovascular death, myocardial infarction or urgent vessel revascularization within 30 days of PCI. Pretreatment. *1o Outcome: CV Death, MI, Urg Revasc. Mehta SR et al. Lancet 2001:358:")
50
PCI-Cure : Overall Results: CV Death or MI
0.0 0.05 0.10 0.15 40 100 200 300 400 10 A B Days following PCI Cumulative Hazard Rate RR 0.69 95% CI P=0.002 Clopidogrel + ASA Placebo A=median time to PCI B=30 days after PCI 12.6% 8.8% Mehta SR et al. Lancet 2001:358:527-33

51
PCI-Cure : CV Death or MI at Various Intervals
12,6 8,8 Overall RRR: 31% * *P=0.002 5,1 3,6 Before PCI 32% 4,4 2,9 PCI to 30 d. 34% 3,9 3,1 30 d. to 1 yr 21% 14 12 Placebo 10 Clopidogrel 8 CV death or MI (%) 6 4 2 Mehta SR et al. Lancet 2001:358:527-33
 Mehta SR et al. Lancet 2001:358:")
52
of atherothrombotic event
CHARISMA - Design Clopidogrel 75mg o.d. (n = 7,600) Patients aged 45 years or older R Double-blind treatment up to 1,040 primary efficacy events* at high-risk of atherothrombotic event Placebo 1 tab o.d. (n = 7,600) 42 month or final visit 1 month visit 3 month visit All patients receiving ASA 75–162 mg o.d. * event driven trial, approximately 15,000 patients R = Randomization
 Patients. aged 45 years or older. R. Double-blind treatment up to 1,040 primary efficacy events* at high-risk. of atherothrombotic event. Placebo. 1 tab o.d. (n = 7,600) 42 month or final visit. 1 month visit. 3 month visit. All patients receiving ASA 75–162 mg o.d. * event driven trial, approximately 15,000 patients. R = Randomization.")
53
Distribution of Responsiveness to Clopidogrel in 544 Individuals
A Normal Distribution: Consistent with a Poly-Genetic and Poly-Environmental Influence 112 96 Who is a Non-Responder? Number of patients 80 64 48 32 16 <= -20 [-10,0] [11,20] [31,40] [51,60] [71,80] [91,100] Change in Aggregation to 5µM ADP Serebruany V. JACC 2004; In press

54
Les antiagrégants plaquettaires dans la fibrillation auriculaire
Inhibiteurs Coagulation FT Plaquette FVIII FVa Fibrinogène Fibrine FVII FVIIa FIX FIXa FVIIIa FV FXa FII FX Thrombine Les antiagrégants plaquettaires dans la fibrillation auriculaire

55
Les antiagrégants plaquettaires dans la fibrillation auriculaire
Inhibiteurs Coagulation FT Plaquette FVIII FVa Fibrinogène Fibrine FVII FVIIa FIX FIXa FVIIIa FV FXa FII FX Thrombine Les antiagrégants plaquettaires dans la fibrillation auriculaire

Présentations similaires