Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Urgences cardiovasculaires
DCEM 4

2
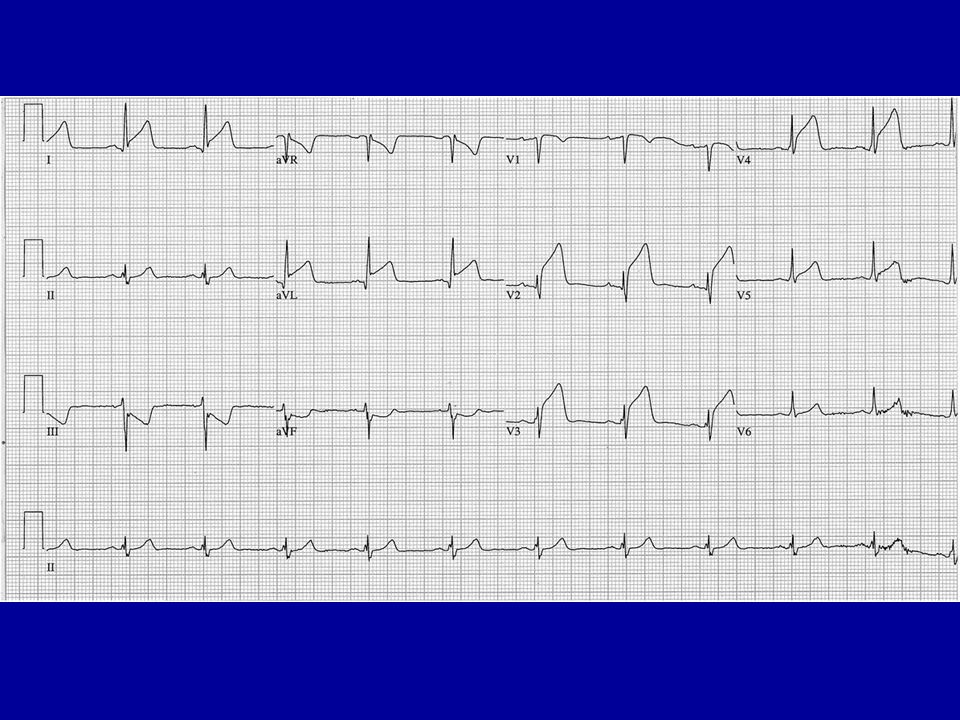
Cas clinique 1 Homme de 53 ans, tabagique (35 PA), dyslipidémique.
Douleur précordiale constrictive évoluant depuis 3 heures. Auscultation normale, pas de SPIC, artères perçues symétriques. TA : 120 / 70, FC : 70 , Sat O2 : 96%,

4
Quel est votre diagnostic ?
Comment traitez vous la douleur de ce patient ? Quelle va être votre conduite thérapeutique ?

5
Rupture de plaque

6
L ’infarctus du myocarde avec sus décalage ST
- La thrombose coronaire est occlusive (> 20 minutes) - Le thrombus est fibrino-cruorique
 - Le thrombus est fibrino-cruorique.")
7
Prévalence de l’occlusion coronaire dans l’infarctus du myocarde
De Wood. NEJM. 1980;303: 897

8
Etape diagnostique Douleur thoracique.
Sus décalage de ST ou BBG d’apparition récente. Savoir répéter les tracés. Augmentation des enzymes cardiaques ( CPK MB, Troponine I ou T), mais ne pas attendre les résultats. Echocardiogramme (ou scintigraphie myocardique) utile pour éliminer le diagnostic en cas de doute.
, mais ne pas attendre les résultats. Echocardiogramme (ou scintigraphie myocardique) utile pour éliminer le diagnostic en cas de doute.")
9
Marqueurs biologiques

10
Marqueurs biologiques

11
Traitement de l’ IdM Lutte contre la douleur.
Antiagrégants plaquettaires. Reperfusion coronaire

12
Traitement de la douleur
La douleur de l’infarctus du myocarde résiste aux dérivés nitrés. Opiacés: chlorhydrate de morphine Ampoules de 1 cg à diluer dans 10 cc de G5 Administration iv de 1cc/mn soit 1mg/mn Cédation ou franche diminution en 10 à 20 mn

13
Thrombolyse et aspirine
Etude ISIS 2. 17187 pts suspects d’ IdM vus dans les 24 heures. Double randomisation: SK vs placebo et ASA vs placebo Lancet. 1988; ii: 349

14
Clarity / TIMI 28 : IDM thrombolysé < 12 h Critère jugement principal : artère occluse
Odds Ratio 0.64 (95% CI ) 36% Odds Reduction P= 0.4 0.6 0.8 1.0 1.2 1.6 n=1752 n=1739 Clopidogrel better Placebo better Clopidogrel 300 mg Placebo
 36% Odds Reduction. P= n=1752. n=1739. Clopidogrel. better. Placebo. better. Clopidogrel. 300 mg. Placebo.")
15
Percentage with endpoint (%)
Clarity / TIMI 28 : décès CV, IDM, récurrence ischémique Revasc. urgente 15 Placebo 20% 10 Clopidogrel Percentage with endpoint (%) Odds Ratio 0.80 (95% CI ) P=0.026 5 5 10 15 20 25 30 days
 Odds Ratio (95% CI ) P= days.")
16
Autres mesures en préhospitalier : classe I (ACC/AHA)
Β-bloquants voie orale en absence de contre-indication, quelle que soit la méthode de reperfusion. (Niveau de preuve: A) Oxygène si SaO2 < 90% (Niveau de preuve : B) Sulfate de morphine : 2 à 4 mg IV (Niveau preuve : C) Nitrés Per os (3 doses TNT sublinguale) Puis IV si douleurs ischémiques, HTA, OAP Sauf si contre-indications (TA < 90 mm Hg, π < 50 bpm ou > 100 bpm, suspiçion d’infarctus VD) Niveau de preuve C Antman et al. JACC 2004;44:680.
 Oxygène si SaO2 < 90% (Niveau de preuve : B) Sulfate de morphine : 2 à 4 mg IV (Niveau preuve : C) Nitrés. Per os (3 doses TNT sublinguale) Puis IV si douleurs ischémiques, HTA, OAP. Sauf si contre-indications (TA < 90 mm Hg, π < 50 bpm ou > 100 bpm, suspiçion d’infarctus VD) Niveau de preuve C. Antman et al. JACC 2004;44:680.")
17
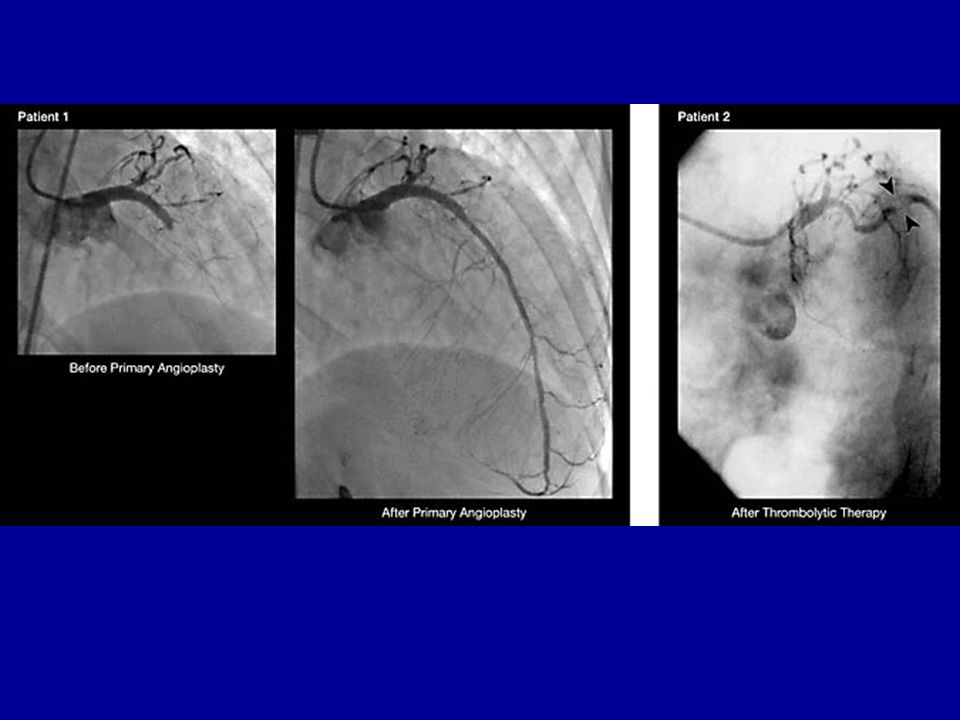
Méthodes de reperfusion

18
Deux éléments conditionnent cette réduction de mortalité
1/ Obtenir un flux normal à la fin de la thrombolyse 2/ Administrer le thrombolytique le plus tôt possible 80 9,9 10 % 9,2 60 7 ,9 Réduction absolue Mortalité 40 de mortalité pour à 1 mois 1000 patients traités 4,3 5 % 20 3 6 9 12 15 18 21 24 TIMI-0 TIMI-1 TIMI-2 TIMI-3 Flux dans la coronaire responsable de l’IDM au décours immédiat de la thrombolyse Délai entre la thrombolyse et le début de la douleur thoracique (heures) GUSTO-I angiographic substudy; Circulation 1995 Boersma, Lancet 1996
 GUSTO-I angiographic substudy; Circulation Boersma, Lancet")
19
Reperfusion coronaire

20
Thrombolytiques dans l’IdM
Streptokinase (SK) 1.5 Million U dans 100 cc G5 ou physio en 30 à 60 minutes. Alteplase (tPA) 15 mg iv bolus puis 0.75 mg/kg en 30 mn et 0.5 mg/kg en 60 mn sans dépasser 100 mg Reteplase (rPA) 2 bolus 10 U en 30 mn Tenecteplase (TNK-tPA) Bolus fonction du poids 30 à 50 mg
 1.5 Million U dans 100 cc G5 ou physio en 30 à 60 minutes. Alteplase (tPA) 15 mg iv bolus puis 0.75 mg/kg en 30 mn et 0.5 mg/kg en 60 mn sans dépasser 100 mg. Reteplase (rPA) 2 bolus 10 U en 30 mn. Tenecteplase (TNK-tPA) Bolus fonction du poids 30 à 50 mg.")
21
TPA et ses dérivés

22
Comparaison des thrombolytiques
Etude GUSTO patients NEJM. 1993; 329: 673

23
Etude GUSTO 1 N Engl J Med. 1993; 329: 673

24
Comparaison de thrombolytiques
Assent 2 Gusto 3

25
Importance de la précocité
Boersma. Lancet. 1994; 343: 311

26
La réduction de mortalité est très importante dans les 3 premières heures. Elle est beaucoup plus faible au delà. Délai de traitement / début des symptomes (H) >80 60 40 20 3 6 9 12 réduction absolue de la mortalité pour 1000 patients traités < 3 heures 3-12 heures Boersma, Lancet 1996
 > réduction absolue de la mortalité pour 1000 patients traités. < 3 heures heures. Boersma, Lancet")
27
Méta-analyse des essais randomisés
En faveur de la thrombolyse préhospitalière En faveur de la thrombolyse hospitalière EMIP MITI Odds Ratio and 95% CI GREAT Schofer Castaigne RR 17%; p=0,03 0,0 0,5 1,0 1 ,5 2 ,0 Leizorovicz N Engl J Med 1993

28
Age et thrombolyse

29
Angioplastie dans l’infarctus
Angioplastie primaire Angioplastie associée à la fibrinolyse Angioplastie de sauvetage.

30
NRMI 2: Primary PCI Door-to-Balloon Time vs. Mortality
MV Adjusted Odds of Death The guidelines discuss in detail the decision to take the time from first medical contact or first door to balloon number to < 90 minutes. For the last decade the importance of time to treatment in PPCI has been debated. The next few studies support the argument “time does matter in PPCI”. n = 2,230 5,734 6,616 4,461 2,627 5,412 Door-to-Balloon Time (minutes)
")
31
Délai entre début symptômes et traitement prédit mortalité à 1 an après ACT primaire
A recent publication from the Zwolle group in the Netherlands looked at the relationship between ischemic time and 1-year mortality assessed as a continuous function and plotted with a quadratic regression model. The dotted lines represent 95% CIs of predicted mortality. Circulation. 2004;109: About the study: “The study population consisted of 1791 patients with STEMI treated by primary angioplasty. The relationship between ischemic time and 1-year mortality was assessed as a continuous function and plotted with a quadratic regression model. The Cox proportional hazards regression model was used to calculate relative risks (for each 30 minutes of delay), adjusted for baseline characteristics related to ischemic time. Variables related to time to treatment were age 70 years (P ), female gender (P-0.004), presence of diabetes mellitus (P-0.002), and previous revascularization (P-0.035). Patients with successful reperfusion had a significantly shorter ischemic time (P-0.006). A total of 103 patients (5.8%) had died at 1-year follow-up. After adjustment for age, gender, diabetes, and previous revascularization, each 30 minutes of delay was associated with a relative risk for 1-year mortality of (95% CI to 1.15; P_0.041). Conclusions—These results suggest that every minute of delay in primary angioplasty for STEMI affects 1-year mortality, even after adjustment for baseline characteristics. Therefore, all efforts should be made to shorten the total ischemic time, not only for thrombolytic therapy but also for primary angioplasty”. Actual abstract, pg 1123 Le risque relatif de la mortalité à 1 an augmente de 7,5% pour chaque 30 mn de délai De Luca. Circulation 2004;109:1223
, adjusted for baseline characteristics related to ischemic time. Variables related to time to treatment were age 70 years (P ), female gender (P-0.004), presence of diabetes mellitus (P-0.002), and previous revascularization (P-0.035). Patients with successful reperfusion had a significantly shorter ischemic time (P-0.006). A total of 103 patients (5.8%) had died at 1-year follow-up. After adjustment for age, gender, diabetes, and previous revascularization, each 30 minutes of delay was associated with a relative risk for 1-year mortality of (95% CI to 1.15; P_0.041). Conclusions—These results suggest that every minute of delay in primary angioplasty for STEMI affects 1-year mortality, even after adjustment for baseline characteristics. Therefore, all efforts should be made to shorten the total ischemic time, not only for thrombolytic therapy but also for primary angioplasty . Actual abstract, pg Le risque relatif de la mortalité à 1 an augmente de 7,5% pour chaque 30 mn de délai. De Luca. Circulation 2004;109:1223.")
32
Importance du stenting dans l’IdM
Etude CADILLAC 2082 patients traités par angioplastie ou Angioplastie plus endoprothèse. Critère de jugement composite NEJM. 2002;346: 957.

33
Anti GIIb/IIIa dans l’angioplastie
Etude ADMIRAL 300 pts dilatés et stentés au stade aigu. Randomisation Réopro vs placebo Critères de jugement composite : décès, réinfarctus, revscularisation Montalescot. NEJM.2001; 344 : 1895

35
Angioplastie vs thrombolyse
Métaanalyse de 23 études randomisées Keeley. Lancet. 2003; 361: 13

36
Angioplastie vs thrombolyse
Métaanalyse de 23 études randomisées Keeley. Lancet. 2003; 361: 13

37
Tous les patients pris en charge en préhospitalier à la phase aiguë d’un infarctus du myocarde devraient être tranférés directement vers un centre de cardiologie interventionnelle. Thrombolyse préhospitalière puis transfert et rescue Transfert et angioplastie primaire 8 p=0.06 p=0.47 5.9 6 5.7 MORTALITE % à 30 jours 3.7 2.2 2 < 2 heures / début de la douleur thoracique > 2 heures / début de la douleur thoracique Steg CAPTIM, Circulation 2003

38
CAPTIM : ATC I vs thrombolyse préhosp
CAPTIM : ATC I vs thrombolyse préhosp. (IDM < 6 h) 1Year Results; Sx to Treatment Analysis Sx 2 h Sx 2 h 7.5 10.0 Death Death Death P=0.057 P=0.47 5.7 7.5 5.0 5.9 Percent 5.0 3.7 2.5 2.2 A recent subanalysis of CAPTIMindicates indicates that prehospital fibrinolysis may be preferable to PPCI for those patients treated within the first 2 hours. Steg PG, et al. Circulation.2003;108(23): As noted on the slide: Other data from CAPTIM suggested a trend toward a decrease in 1-year mortality among fibrinolytic patients presenting within 2 hours of symptom onset. 2.5 0.0 0.0 Pre-hospital Lysis Primary PCI Pre-hospital Lysis Primary PCI Touboul P. Presented at: The 18th International Symposium on Thrombolysis and Interventional Therapy in Acute Myocardial Infarction - George Washington University Symposium; November 16, 2002; Chicago, Ill.
 1Year Results; Sx to Treatment Analysis. Sx 2 h. Sx 2 h Death. Death. Death. P= P= Percent A recent subanalysis of CAPTIMindicates indicates that prehospital fibrinolysis may be preferable to PPCI for those patients treated within the first 2 hours. Steg PG, et al. Circulation.2003;108(23): As noted on the slide: Other data from CAPTIM suggested a trend toward a decrease in 1-year mortality among fibrinolytic patients presenting within 2 hours of symptom onset Pre-hospital Lysis. Primary PCI. Pre-hospital Lysis. Primary PCI. Touboul P. Presented at: The 18th International Symposium on Thrombolysis and Interventional Therapy in Acute Myocardial Infarction - George Washington University Symposium; November 16, 2002; Chicago, Ill.")
39
Choix des stratégies de reperfusion
Décision multifactorielle et individualisée Espérance de vie sans reperfusion. Risque d’hémorragie intracérébrale. Possibilités locales (disponibilité, qualité) pour l’angioplastie. Bon jugement clinique
 pour l’angioplastie. Bon jugement clinique.")
40
Recommandations ESC. 2005

41
Prise en charge initiale (1)
Age Antécédents Examen clinique ECG Examens de laboratoire + enzymes cardiaques Premières mesures de routine Appréciation des délais et des risques Délai début symptômes Délai vers centre angioplastie + disponibilité Risque de l’IDM Risque hémorragique “Regardless of the approach used, all patients presenting to the ED with chest discomfort or other symptoms suggestive of STEMI or UA should be considered high priority triage cases and should be evaluated and treated based on predetermined, institution-specific chest pain protocol. The goal should be to achieve a door-to-needle time within 30 minutes and a door-to-balloon time within 90 minutes” (p.677, Exec Summary, 2004). Optimal Strategies for Emergency Department Triage Class I B Hospitals should establish multidisciplinary teams to develop guideline-based institution-specific written protocols for triaging and managing pts who present to the ED with symptoms suggestive of STEMI. Initial Patient Evaluation -covered in previous slides History Class I C Targeted HX of STEMI pt. taken in the ED to include: prior episodes of MI, CABG, or PCI; chest discomfort, associated symptoms, sex & age related differences in presentation, HTN, DM, possibility of aortic dissection, risk of bleeding, and clinical cerebrovascular disease (amaurosis fugax, face/limb weakness or clumsiness or numbness, or sensory loss, ataxia, or vertigo) Physical Exam Class IC A physical exam should be performed to aid in the DX and assessment of the extent, location, and presence of complications. A brief, focused, and limited neurological exam to look for prio stroke or cognitive deficits should be performed before administering fibrinolytics ECG Class I 1. 12-Lead ECG completed and shown to an experienced ED physician within 10 minutes of arrival to ED for chest discomfort (or anginal equivalents) or other symptoms suggestive of STEMI (Level C). 2. Non-DX initial ECG- patients remain symptomatic, perform serial ECGs at 5 to 10 minute intervals or continuous 12-Lead ST-segment monitoring should performed to detect potential development of STEMI (Level C). In pts with inferior STEMI, right-sided ECG leads should be obtained to detect the potential development of ST elevation and RV infarct (Level B). Laboratory Exams Lab exams should be performed as part of the management of STEMI but SHOULD NOT delay the implementation of reperfusion therapy (Level C). Biomarkers of cardiac damage Cardiac specific troponins should be used as the optimum biomarkers for the evaluation of patients with STEMI who have coexistent skeletal muscle injury (Level C). Patients with ST elevation on their ECG and symptoms of STEMI, reperfusion therapy should be initiated as soon as possible and is not contingent on a biomarker assay (Level C). -may choose to review IIa and III recommendations or move ahead Imaging Patients with STEMI should have a portable chest X-ray, but this should not delay implementation of a reperfusion therapy (unless a potential contraindication, such as aortic dissection, is suspected)-Review symptomology of aortic dissection (Level C). Other imaging studies may help differentiate DX……….t-echo, MRI…etc. Routine Measures The routine measures of Oxygen, NTG, Analgesia, ASA,& Beta-Blockers will be covered briefly at the end of the program. These routine measures should be done in conjunction with screening the patient and facilitating for rapid reperfusion once the diagnosis of STEMI is made. Antman et al. JACC 2004;44:677.
. Optimal Strategies for Emergency Department Triage. Class I B Hospitals should establish multidisciplinary teams to develop guideline-based institution-specific written protocols for triaging and managing pts who present to the ED with symptoms suggestive of STEMI. Initial Patient Evaluation. -covered in previous slides. History. Class I C Targeted HX of STEMI pt. taken in the ED to include: prior episodes of MI, CABG, or PCI; chest discomfort, associated symptoms, sex & age related differences in presentation, HTN, DM, possibility of aortic dissection, risk of bleeding, and clinical cerebrovascular disease (amaurosis fugax, face/limb weakness or clumsiness or numbness, or sensory loss, ataxia, or vertigo) Physical Exam. Class IC. A physical exam should be performed to aid in the DX and assessment of the extent, location, and presence of complications. A brief, focused, and limited neurological exam to look for prio stroke or cognitive deficits should be performed before administering fibrinolytics. ECG. Class I Lead ECG completed and shown to an experienced ED physician within 10 minutes of arrival to ED for chest discomfort (or anginal equivalents) or other symptoms suggestive of STEMI (Level C). 2. Non-DX initial ECG- patients remain symptomatic, perform serial ECGs at 5 to 10 minute intervals or continuous 12-Lead ST-segment monitoring should performed to detect potential development of STEMI (Level C). In pts with inferior STEMI, right-sided ECG leads should be obtained to detect the potential development of ST elevation and RV infarct (Level B). Laboratory Exams. Lab exams should be performed as part of the management of STEMI but SHOULD NOT delay the implementation of reperfusion therapy (Level C). Biomarkers of cardiac damage. Cardiac specific troponins should be used as the optimum biomarkers for the evaluation of patients with STEMI who have coexistent skeletal muscle injury (Level C). Patients with ST elevation on their ECG and symptoms of STEMI, reperfusion therapy should be initiated as soon as possible and is not contingent on a biomarker assay (Level C). -may choose to review IIa and III recommendations or move ahead. Imaging. Patients with STEMI should have a portable chest X-ray, but this should not delay implementation of a reperfusion therapy (unless a potential contraindication, such as aortic dissection, is suspected)-Review symptomology of aortic dissection (Level C). Other imaging studies may help differentiate DX……….t-echo, MRI…etc. Routine Measures. The routine measures of Oxygen, NTG, Analgesia, ASA,& Beta-Blockers will be covered briefly at the end of the program. These routine measures should be done in conjunction with screening the patient and facilitating for rapid reperfusion once the diagnosis of STEMI is made. Antman et al. JACC 2004;44:677.")
42
Prise en charge initiale (2)
. ATCD hgie intracrânienne . Lésion vasc. ou néopl. cérébrale . AVC dans les 3 mois . Diathèses hémorragiques . Hémorragie active . HTA sévère . Suspiçion dissection aortique . Trauma crânien < 3 mois Douleur thoracique < 12 h Contre-indication thrombolyse “Regardless of the approach used, all patients presenting to the ED with chest discomfort or other symptoms suggestive of STEMI or UA should be considered high priority triage cases and should be evaluated and treated based on predetermined, institution-specific chest pain protocol. The goal should be to achieve a door-to-needle time within 30 minutes and a door-to-balloon time within 90 minutes” (p.677, Exec Summary, 2004). Optimal Strategies for Emergency Department Triage Class I B Hospitals should establish multidisciplinary teams to develop guideline-based institution-specific written protocols for triaging and managing pts who present to the ED with symptoms suggestive of STEMI. Initial Patient Evaluation -covered in previous slides History Class I C Targeted HX of STEMI pt. taken in the ED to include: prior episodes of MI, CABG, or PCI; chest discomfort, associated symptoms, sex & age related differences in presentation, HTN, DM, possibility of aortic dissection, risk of bleeding, and clinical cerebrovascular disease (amaurosis fugax, face/limb weakness or clumsiness or numbness, or sensory loss, ataxia, or vertigo) Physical Exam Class IC A physical exam should be performed to aid in the DX and assessment of the extent, location, and presence of complications. A brief, focused, and limited neurological exam to look for prio stroke or cognitive deficits should be performed before administering fibrinolytics ECG Class I 1. 12-Lead ECG completed and shown to an experienced ED physician within 10 minutes of arrival to ED for chest discomfort (or anginal equivalents) or other symptoms suggestive of STEMI (Level C). 2. Non-DX initial ECG- patients remain symptomatic, perform serial ECGs at 5 to 10 minute intervals or continuous 12-Lead ST-segment monitoring should performed to detect potential development of STEMI (Level C). In pts with inferior STEMI, right-sided ECG leads should be obtained to detect the potential development of ST elevation and RV infarct (Level B). Laboratory Exams Lab exams should be performed as part of the management of STEMI but SHOULD NOT delay the implementation of reperfusion therapy (Level C). Biomarkers of cardiac damage Cardiac specific troponins should be used as the optimum biomarkers for the evaluation of patients with STEMI who have coexistent skeletal muscle injury (Level C). Patients with ST elevation on their ECG and symptoms of STEMI, reperfusion therapy should be initiated as soon as possible and is not contingent on a biomarker assay (Level C). -may choose to review IIa and III recommendations or move ahead Imaging Patients with STEMI should have a portable chest X-ray, but this should not delay implementation of a reperfusion therapy (unless a potential contraindication, such as aortic dissection, is suspected)-Review symptomology of aortic dissection (Level C). Other imaging studies may help differentiate DX……….t-echo, MRI…etc. Routine Measures The routine measures of Oxygen, NTG, Analgesia, ASA,& Beta-Blockers will be covered briefly at the end of the program. These routine measures should be done in conjunction with screening the patient and facilitating for rapid reperfusion once the diagnosis of STEMI is made. Angioplastie primaire
. Optimal Strategies for Emergency Department Triage. Class I B Hospitals should establish multidisciplinary teams to develop guideline-based institution-specific written protocols for triaging and managing pts who present to the ED with symptoms suggestive of STEMI. Initial Patient Evaluation. -covered in previous slides. History. Class I C Targeted HX of STEMI pt. taken in the ED to include: prior episodes of MI, CABG, or PCI; chest discomfort, associated symptoms, sex & age related differences in presentation, HTN, DM, possibility of aortic dissection, risk of bleeding, and clinical cerebrovascular disease (amaurosis fugax, face/limb weakness or clumsiness or numbness, or sensory loss, ataxia, or vertigo) Physical Exam. Class IC. A physical exam should be performed to aid in the DX and assessment of the extent, location, and presence of complications. A brief, focused, and limited neurological exam to look for prio stroke or cognitive deficits should be performed before administering fibrinolytics. ECG. Class I Lead ECG completed and shown to an experienced ED physician within 10 minutes of arrival to ED for chest discomfort (or anginal equivalents) or other symptoms suggestive of STEMI (Level C). 2. Non-DX initial ECG- patients remain symptomatic, perform serial ECGs at 5 to 10 minute intervals or continuous 12-Lead ST-segment monitoring should performed to detect potential development of STEMI (Level C). In pts with inferior STEMI, right-sided ECG leads should be obtained to detect the potential development of ST elevation and RV infarct (Level B). Laboratory Exams. Lab exams should be performed as part of the management of STEMI but SHOULD NOT delay the implementation of reperfusion therapy (Level C). Biomarkers of cardiac damage. Cardiac specific troponins should be used as the optimum biomarkers for the evaluation of patients with STEMI who have coexistent skeletal muscle injury (Level C). Patients with ST elevation on their ECG and symptoms of STEMI, reperfusion therapy should be initiated as soon as possible and is not contingent on a biomarker assay (Level C). -may choose to review IIa and III recommendations or move ahead. Imaging. Patients with STEMI should have a portable chest X-ray, but this should not delay implementation of a reperfusion therapy (unless a potential contraindication, such as aortic dissection, is suspected)-Review symptomology of aortic dissection (Level C). Other imaging studies may help differentiate DX……….t-echo, MRI…etc. Routine Measures. The routine measures of Oxygen, NTG, Analgesia, ASA,& Beta-Blockers will be covered briefly at the end of the program. These routine measures should be done in conjunction with screening the patient and facilitating for rapid reperfusion once the diagnosis of STEMI is made. Angioplastie primaire.")
43
Stratégie thrombolyse Aspirine 500 mg IV HNF
< 3 heures 3-12 heures Stratégie thrombolyse Aspirine 500 mg IV HNF Clopidogrel 300 mg (<75 ans) Stratégie angioplastie primaire Aspirine 500 mg IV HNF 5000 ui clopidogrel 600 mg RESCUE ’ Délai de ponction << 1 heure Pas de transfert possible vers un centre PCI
 Stratégie angioplastie primaire. Aspirine 500 mg IV. HNF 5000 ui. clopidogrel 600 mg. RESCUE 45-60’ Délai de ponction << 1 heure. Pas de transfert possible vers un centre PCI.")
44
Prise en charge initiale (3)
Douleur < 3 h Douleur 3 à 12 h ATC Pas centre ATC impossible ATC possible < 90 mn disponible < 90 mn sauf si délai ATC > 90 mn Absence contre-indications Douleur < 3 h Douleur 3 à 12 h “Regardless of the approach used, all patients presenting to the ED with chest discomfort or other symptoms suggestive of STEMI or UA should be considered high priority triage cases and should be evaluated and treated based on predetermined, institution-specific chest pain protocol. The goal should be to achieve a door-to-needle time within 30 minutes and a door-to-balloon time within 90 minutes” (p.677, Exec Summary, 2004). Optimal Strategies for Emergency Department Triage Class I B Hospitals should establish multidisciplinary teams to develop guideline-based institution-specific written protocols for triaging and managing pts who present to the ED with symptoms suggestive of STEMI. Initial Patient Evaluation -covered in previous slides History Class I C Targeted HX of STEMI pt. taken in the ED to include: prior episodes of MI, CABG, or PCI; chest discomfort, associated symptoms, sex & age related differences in presentation, HTN, DM, possibility of aortic dissection, risk of bleeding, and clinical cerebrovascular disease (amaurosis fugax, face/limb weakness or clumsiness or numbness, or sensory loss, ataxia, or vertigo) Physical Exam Class IC A physical exam should be performed to aid in the DX and assessment of the extent, location, and presence of complications. A brief, focused, and limited neurological exam to look for prio stroke or cognitive deficits should be performed before administering fibrinolytics ECG Class I 1. 12-Lead ECG completed and shown to an experienced ED physician within 10 minutes of arrival to ED for chest discomfort (or anginal equivalents) or other symptoms suggestive of STEMI (Level C). 2. Non-DX initial ECG- patients remain symptomatic, perform serial ECGs at 5 to 10 minute intervals or continuous 12-Lead ST-segment monitoring should performed to detect potential development of STEMI (Level C). In pts with inferior STEMI, right-sided ECG leads should be obtained to detect the potential development of ST elevation and RV infarct (Level B). Laboratory Exams Lab exams should be performed as part of the management of STEMI but SHOULD NOT delay the implementation of reperfusion therapy (Level C). Biomarkers of cardiac damage Cardiac specific troponins should be used as the optimum biomarkers for the evaluation of patients with STEMI who have coexistent skeletal muscle injury (Level C). Patients with ST elevation on their ECG and symptoms of STEMI, reperfusion therapy should be initiated as soon as possible and is not contingent on a biomarker assay (Level C). -may choose to review IIa and III recommendations or move ahead Imaging Patients with STEMI should have a portable chest X-ray, but this should not delay implementation of a reperfusion therapy (unless a potential contraindication, such as aortic dissection, is suspected)-Review symptomology of aortic dissection (Level C). Other imaging studies may help differentiate DX……….t-echo, MRI…etc. Routine Measures The routine measures of Oxygen, NTG, Analgesia, ASA,& Beta-Blockers will be covered briefly at the end of the program. These routine measures should be done in conjunction with screening the patient and facilitating for rapid reperfusion once the diagnosis of STEMI is made. Thrombolyse Angioplastie primaire
. Optimal Strategies for Emergency Department Triage. Class I B Hospitals should establish multidisciplinary teams to develop guideline-based institution-specific written protocols for triaging and managing pts who present to the ED with symptoms suggestive of STEMI. Initial Patient Evaluation. -covered in previous slides. History. Class I C Targeted HX of STEMI pt. taken in the ED to include: prior episodes of MI, CABG, or PCI; chest discomfort, associated symptoms, sex & age related differences in presentation, HTN, DM, possibility of aortic dissection, risk of bleeding, and clinical cerebrovascular disease (amaurosis fugax, face/limb weakness or clumsiness or numbness, or sensory loss, ataxia, or vertigo) Physical Exam. Class IC. A physical exam should be performed to aid in the DX and assessment of the extent, location, and presence of complications. A brief, focused, and limited neurological exam to look for prio stroke or cognitive deficits should be performed before administering fibrinolytics. ECG. Class I Lead ECG completed and shown to an experienced ED physician within 10 minutes of arrival to ED for chest discomfort (or anginal equivalents) or other symptoms suggestive of STEMI (Level C). 2. Non-DX initial ECG- patients remain symptomatic, perform serial ECGs at 5 to 10 minute intervals or continuous 12-Lead ST-segment monitoring should performed to detect potential development of STEMI (Level C). In pts with inferior STEMI, right-sided ECG leads should be obtained to detect the potential development of ST elevation and RV infarct (Level B). Laboratory Exams. Lab exams should be performed as part of the management of STEMI but SHOULD NOT delay the implementation of reperfusion therapy (Level C). Biomarkers of cardiac damage. Cardiac specific troponins should be used as the optimum biomarkers for the evaluation of patients with STEMI who have coexistent skeletal muscle injury (Level C). Patients with ST elevation on their ECG and symptoms of STEMI, reperfusion therapy should be initiated as soon as possible and is not contingent on a biomarker assay (Level C). -may choose to review IIa and III recommendations or move ahead. Imaging. Patients with STEMI should have a portable chest X-ray, but this should not delay implementation of a reperfusion therapy (unless a potential contraindication, such as aortic dissection, is suspected)-Review symptomology of aortic dissection (Level C). Other imaging studies may help differentiate DX……….t-echo, MRI…etc. Routine Measures. The routine measures of Oxygen, NTG, Analgesia, ASA,& Beta-Blockers will be covered briefly at the end of the program. These routine measures should be done in conjunction with screening the patient and facilitating for rapid reperfusion once the diagnosis of STEMI is made. Thrombolyse. Angioplastie primaire.")
45
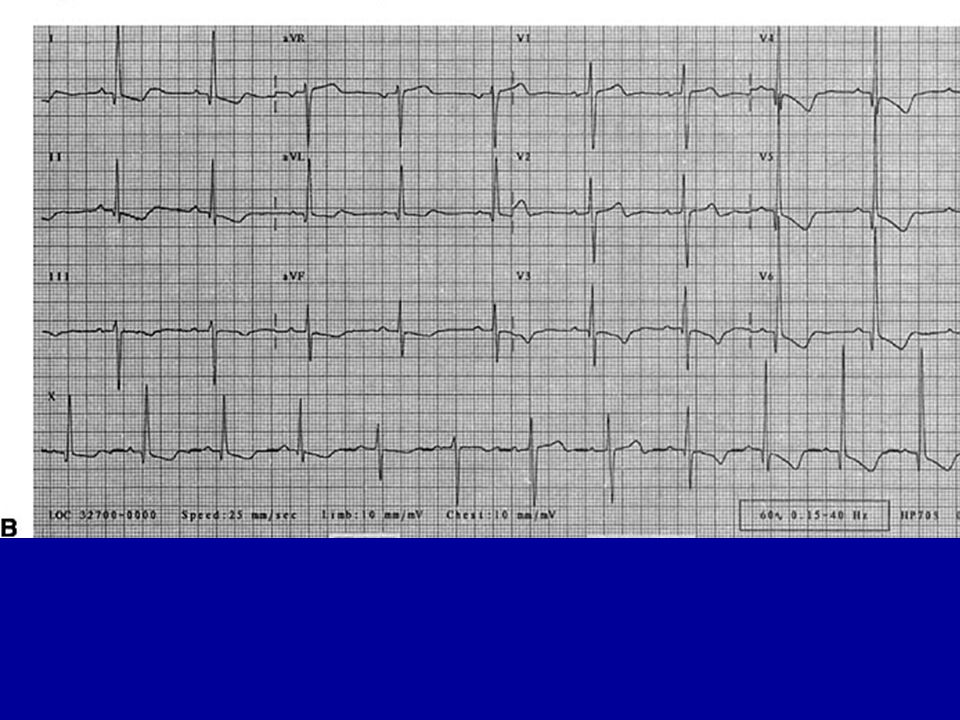
Cas clinique 2 Homme de 64 ans, diabétique traité par du glucophage, tabagique. Apparition depuis 3 jours de douleur thoracique rétrosternale à l’effort, cédant à l’arrêt. Survenue d’une douleur identique spontanée, ayant motivée la consultation. Examen clinique normal. TA : 145 / 75, Sat O2 : 96 % en AA

47
Quel est votre diagnostic ?
Quels examens complémentaires demandez – vous ? Quels sont les éléments de sévérité ? Quelle va être votre conduite thérapeutique ?

48
Syndromes Coronariens Aigus sans sus-déclage de ST: angor instable et infarctus sans onde Q
- la thrombose coronaire reste incomplète et brève, uniquement plaquettaire- Les embolies distales de plaquettes sont habituelles mais ± importantes

49
Thrombus et SCA

50
Microembolisations dans les syndromes coronariens aigus

51
Syndrome coronarien aigu

52
Troponine

53
Valeur pronostique de la troponine
Syndrome coronarien aigu (TIMI 3B) Antman. NEJM. 1996; 335: 1342
 Antman. NEJM. 1996; 335:")
54
Activation des plaquettes

55
Antiagrégants et coronaropathie
L’aspirine. Les thiénopyriridines Ticlopidine (Ticlid ®) Clopidogrel ( Plavix ®) Les Antagonistes des récepteurs IIb/IIIa. L’abciximab (Réopro ®) L’eptifibatide (Integrilin ®) Le tirofiban (Agrastat ®)
 Clopidogrel ( Plavix ®) Les Antagonistes des récepteurs IIb/IIIa. L’abciximab (Réopro ®) L’eptifibatide (Integrilin ®) Le tirofiban (Agrastat ®)")
56
Clopidogrel et aspirine dans les syndromes coronariens aigus
patients hospitalisés pour un SCA sans sus décalage de ST. Randomisation entre Clopidogrel (300 mg en dose de charge puis 75 mg/j pendant 3 à 12 mois) et placebo en association avec l’aspirine (75 à 325 mg/j). Critère de jugement composite: Décès CV et IdM ou AVC non mortels. CURE. NEJM. 2001; 345: 494
 et placebo en association avec l’aspirine (75 à 325 mg/j). Critère de jugement composite: Décès CV et IdM ou AVC non mortels. CURE. NEJM. 2001; 345: 494.")
57
CURE. Résultats (1) Clopidogrel Placebo RR Citèrre Principal 9.3 11.4
Décès CV 5.1 5.5 IdM 5.2 6.7 AVC 1.2 1.4 Angor réfractaire 8.7 Critère principal: 7.9 vs 9.9% chez les non diabétiques et 14.2 vs 16.7% chez les diabétiques.

58
CURE. Résultats (2)
")
59
CURE. Complications hémorragiques
Clopidogrel Placebo RR H. majeures 3.7% 2.7% 1.38 (1.13 – 1.67) AVC hémorragique 0.1% H. mineures 5.1% 2.4% 2.12 ( ) Hémorragies 8.5% 5.0% 1.69 (1.48 – 1.94)
 AVC hémorragique. 0.1% H. mineures. 5.1% 2.4% 2.12 ( ) Hémorragies. 8.5% 5.0% 1.69 (1.48 – 1.94)")
60
Influence de la dose d’aspirine
Analyse rétrospective des patients de l’étude CURE Critère principal Hémorragies majeures Peters et al. Circulation. 2003; 108: 1682

61
Anti-GPIIb/IIIa

62
Héparine et SCA Métaanalyse du risque de décès et d’Idm dans Essence et Timi 11 B. NEJM.1997; 337:447 et Circulation. 1999;100: 1593

63
Intérêt d’une stratégie invasive
2220 pts avec SCA sans sus-décalage ST mais Tropo + Asa, Hép, tirofiban Stratégie invasive vs conservatrice Critère de jugement: décès, Idm , nouveau SCA Cannon. NEJM. 2001; 344:1879

64
Facteurs de risque élevé
Récidive douloureuse. Angor post infarctus. Augmentation de la troponine. Instabilité hémodynamique ou rythmique. Diabétiques. Variations du segment ST Impossibilité de surveiller le ST.

65
Prise en charge d’un SCA
Suspicion clinique de sca. Clinique, ECG, Biologie Dg incertain Sus décalage de ST Pas de sus décalage ASA, HBPM, clopidogrel Bêta -, Nitrés, statine Aspirine Thrombolyse Angioplastie Haut risque Bas risque 2éme tropo Anti G 2b3a Coronaro Négative Positive Recherche d’ischémie

66
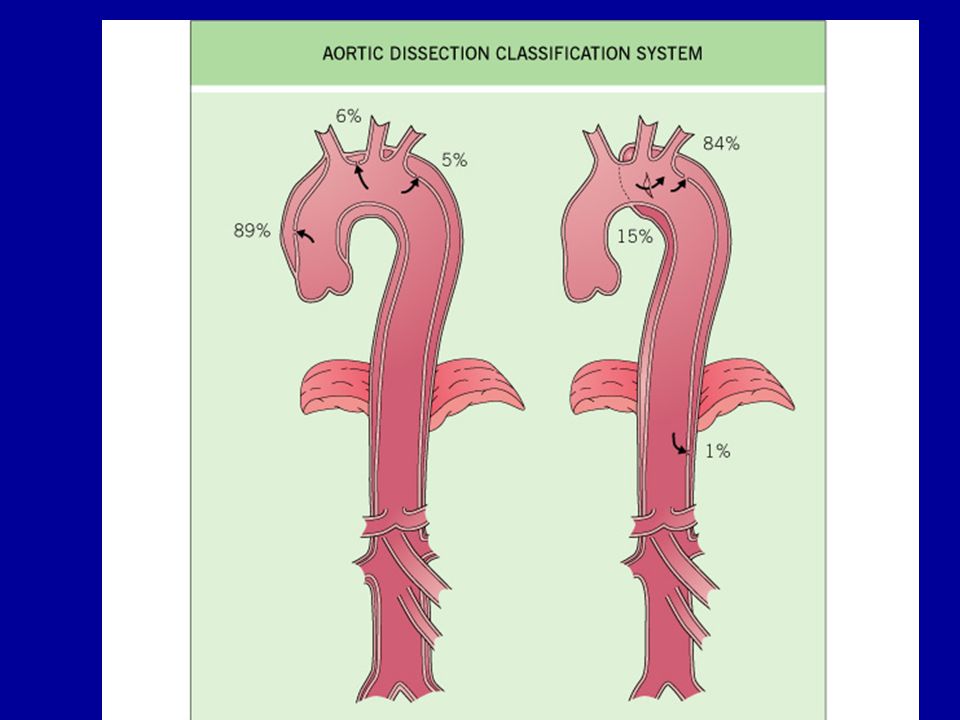
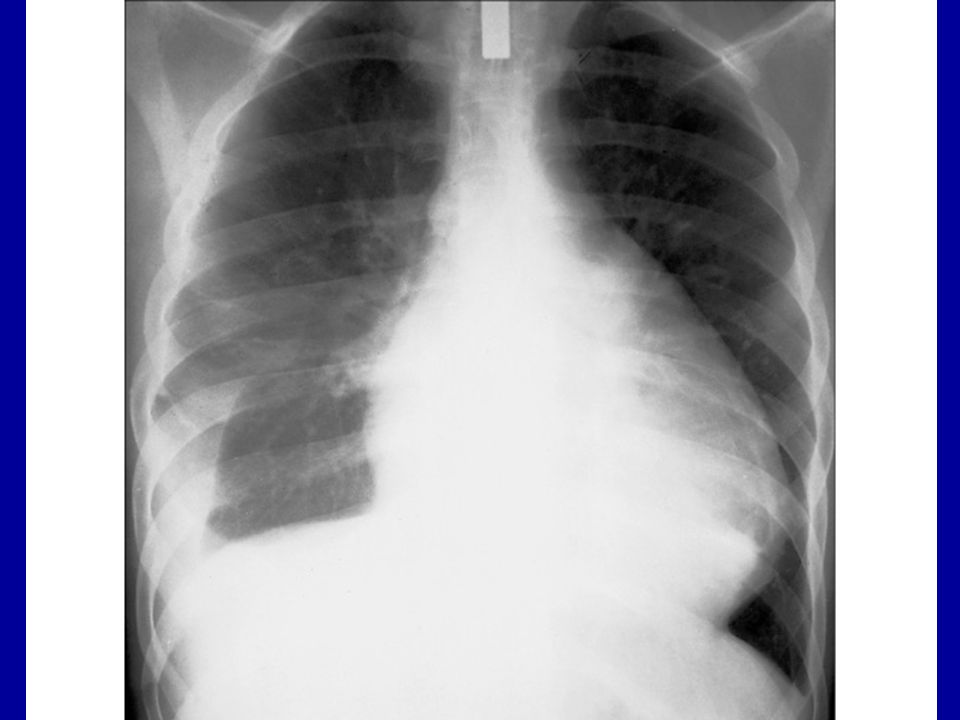
Cas clinique 3 Homme de 65 ans ayant des antécédents d ‘ HTA sévère, négligée. Douleur thoracique intense ayant débutée il y a 6 heures avec une perte de connaissance brève initiale. La douleur initialement rétrosternale est devenue dorsale haute. Cliniquement: TA 19 / 11, SPIC = 0, Sat 94 %, SD latérosternal gauche 2/6.

68
Quel est votre diagnostic ?
Quel(s) examen(s) complémentaires demandez- vous ? Quel est le pronostic de la maladie? Quelle va être votre conduite thérapeutique?
 examen(s) complémentaires demandez- vous Quel est le pronostic de la maladie Quelle va être votre conduite thérapeutique")
72
Cas clinique 4 Femme de 45 ans sans antécédent contributif.
Douleur précordiale évoluant depuis 36 heures avec gêne respiratoire. TA 125 / 70, FC 100 /mn, Température: 38.8°, Sat O2 95 %. Auscultation cardiaque normale.

74
Quel est votre diagnostic ?
Quels examens complémentaires demandez- vous ? Quel traitement instaurez – vous? Quels sont les éléments de la surveillance?

75
Temps du frottement

77
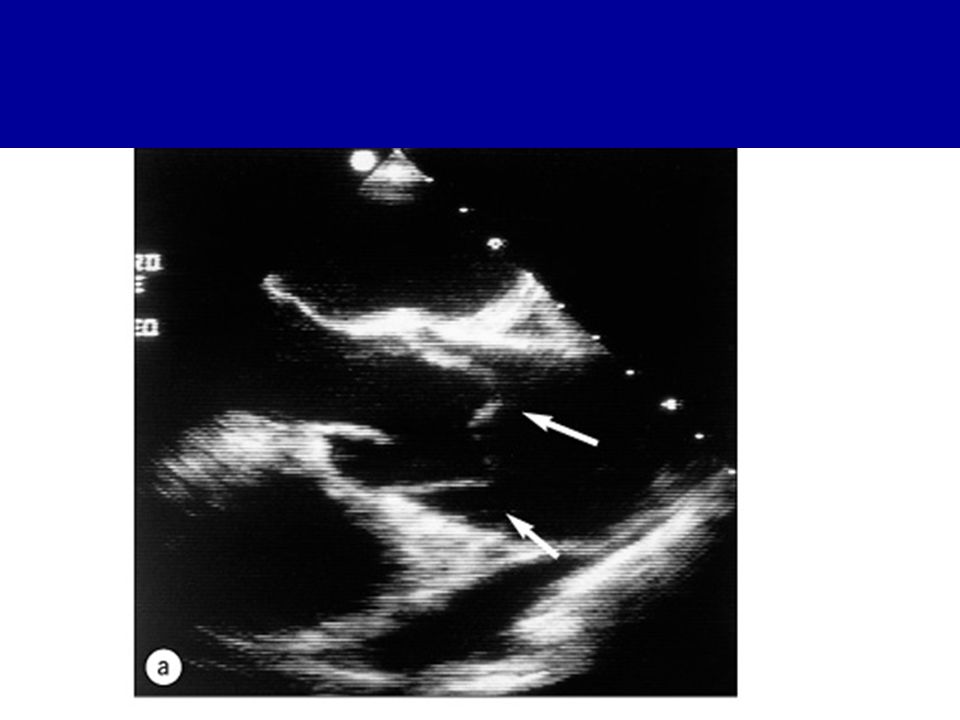
Signes échographiques
Confirme le diagnostic en cas d épanchement important Est normal dans les formes avec peu de liquide ou sèches

78
Tamponnade Responsable d’une adiastolie aigue;
La vitesse de constitution est plus importante que le volume

79
Tamponnade Diagnostic clinique: Ecg :variation de l’axe
Hypotension voire choc avec tachycardie Pouls paradoxal Signes droits: turgescence jugulaire, foie cardiaque Ecg :variation de l’axe Echo Volume, signes de mauvaise tolérance, « swinging heart »

80
Physiopathologie du pouls paradoxal

81
Alternance électrique

82
Doppler et tamponnade

83
Diagnostic étiologique
Péricardites autonomes Idiopathique Virale (coxsackie, grippe, adénovirus, entérovirus,mononucléose, HIV ) Rhumatismale Septique Tuberculeuse Collagénose Péricardites secondaires Cancer (habituellement secondaire) ou hémopathie Radiothérapie Insuffisance rénale, hypothyroïdie Infarctus du myocarde Chirurgie cardiaque
 Rhumatismale. Septique. Tuberculeuse. Collagénose. Péricardites secondaires. Cancer (habituellement secondaire) ou hémopathie. Radiothérapie. Insuffisance rénale, hypothyroïdie. Infarctus du myocarde. Chirurgie cardiaque.")
84
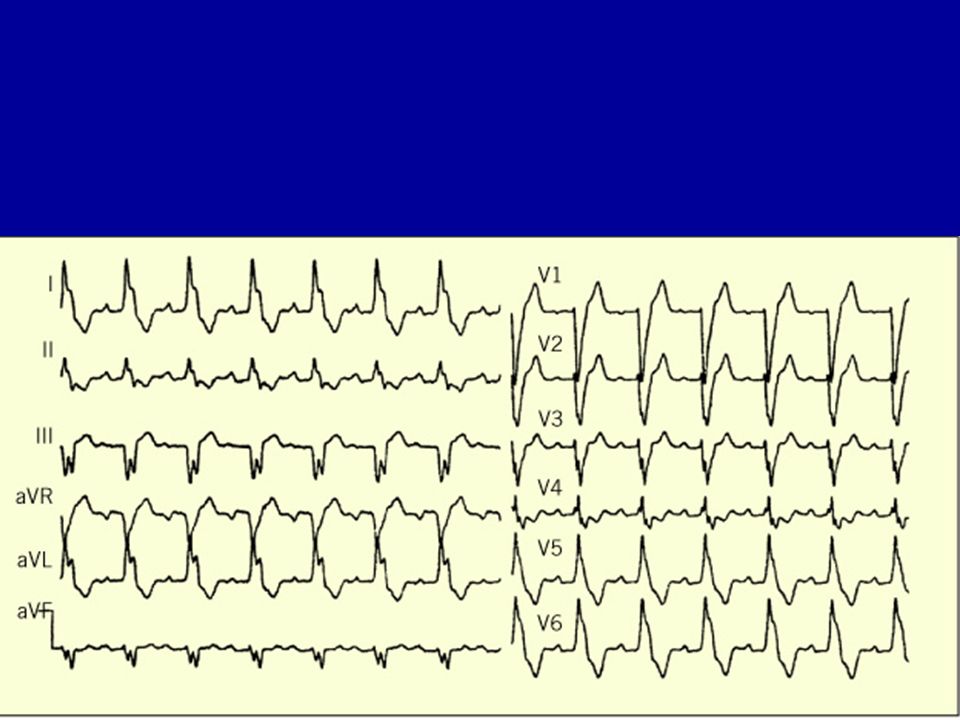
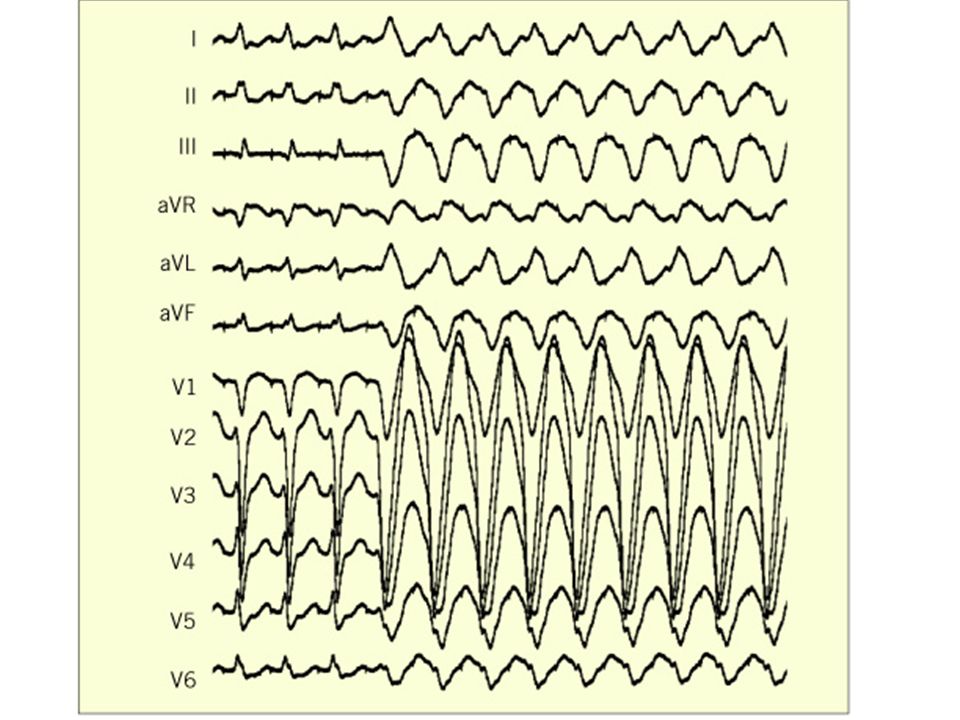
Cas clinique 5 Femme de 54 ans , tabagique, sans antécédents contributifs. Survenue brutale d’un malaise lipothymique avec dyspnée et palpitations. FC : 150 / mn, TA 105 / 70 . Auscultation normale, pas d’insuffisance cardiaque.

86
Comment analysez – vous le tracé ?
Quel est votre diagnostic ? Quelle va être votre conduite thérapeutique ?

87
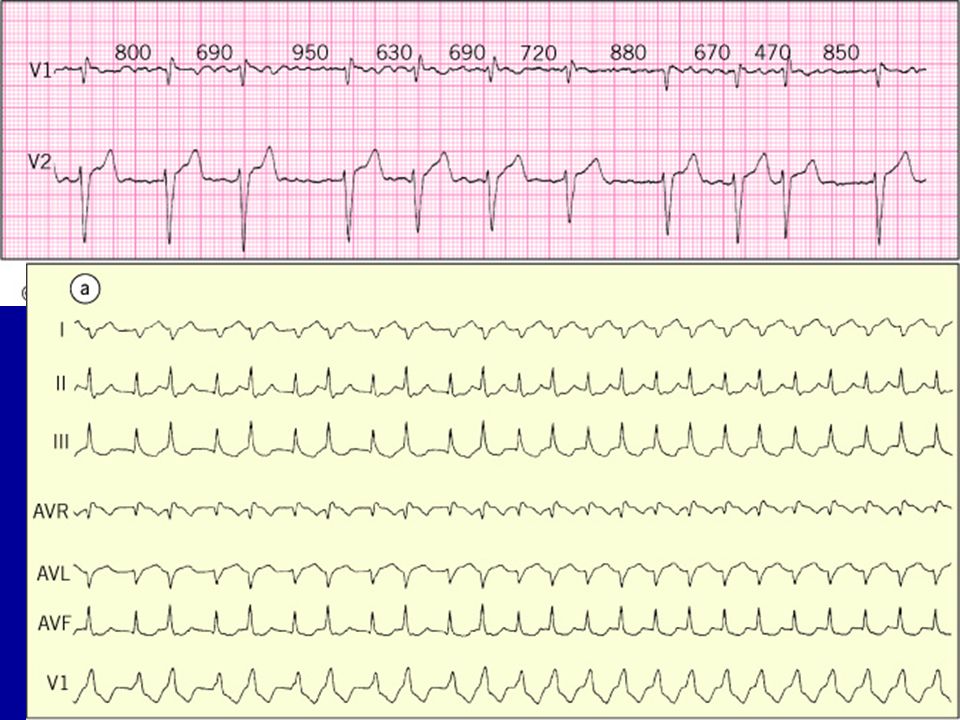
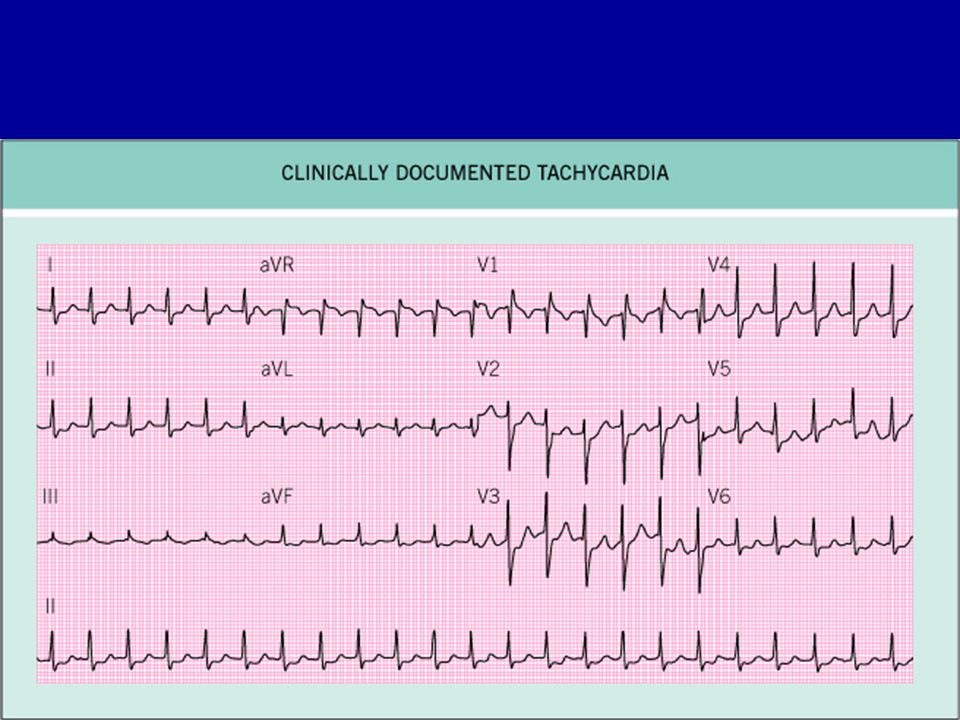
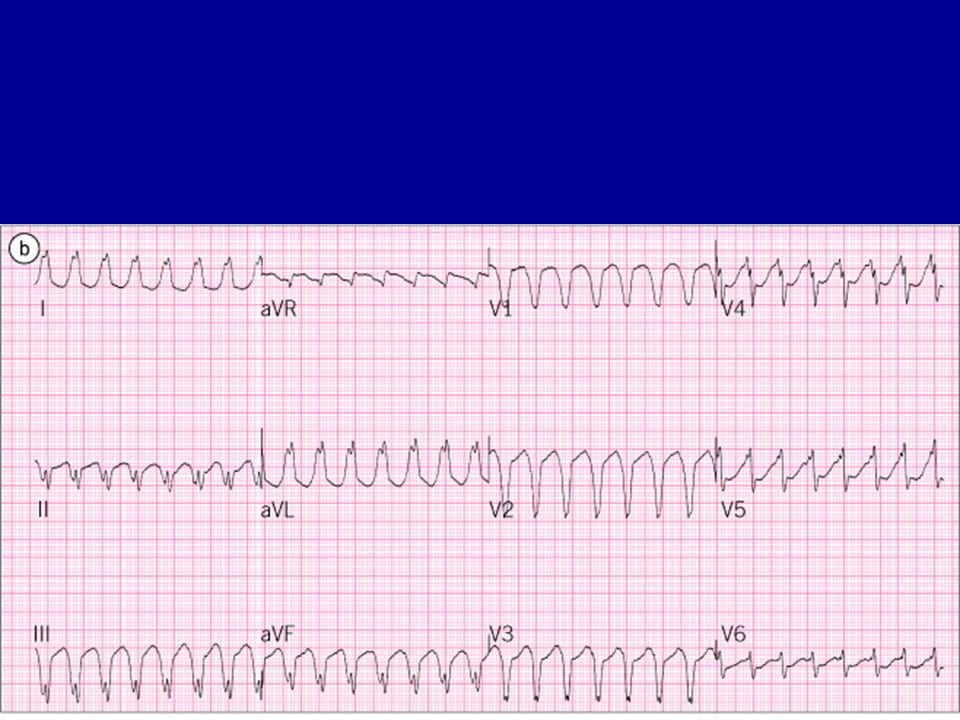
Analyse ECG d’une tachycardie
Rythme régulier ou irrégulier. Si irrégulier : probable TAC / FA. QRS fins ou larges. QRS fins ( < 0.12s ): TSV QRS larges (≥ 0.12s): TV ou TSV avec BB organique ou fonctionnel Analyse de l’activité auriculaire.
: TSV. QRS larges (≥ 0.12s): TV ou TSV avec BB organique ou fonctionnel. Analyse de l’activité auriculaire.")
89
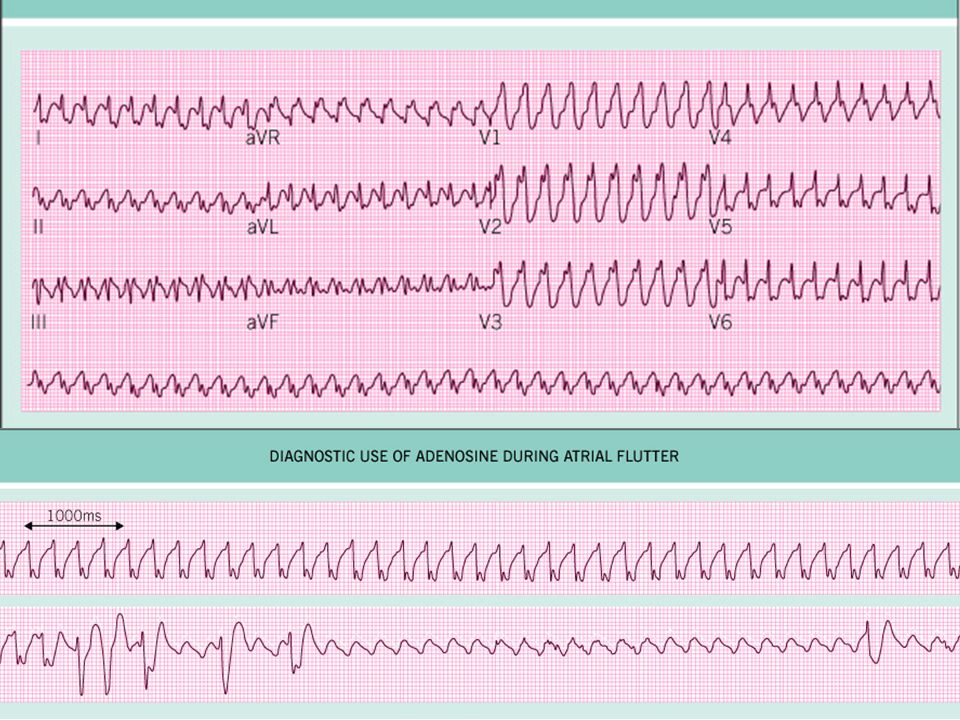
Analyse de l’activité auriculaire
Surtout en D2, D3, Vf et V1. Tracé long. Oesophagienne. 3 cas de figure. A > V : Tachycardie auriculaire. :V > A: TV A = V: Manœuvres vagales: compression des globes, Massage SC, Valsalva, Striadyne

90
Influence des manœuvres vagales
Tachycardie SV: Ralentissement de la cadence ventriculaire avec meilleure visualisation de l’activité auriculaire. TJ : Réduction de la crise. TV : aucune influence

Présentations similaires