Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Endovascular treatment of acute ischemic stroke
McGill Neurology Academic half-day Wednesday, May 8th, 2013 Alexandre Y. Poppe MD CM, FRCPC Stroke neurologist Notre-Dame Hospital, CHUM

2
Disclosures CHUM PI for IMS-3 Honoraria
Conferences: Boehringer-Ingelheim, Sanofi-BMS Advisory boards: Octapharma, Pfizer-BMS

3
Plan Evidence for endovascular stroke therapy CHUM experience
Before 2013 In 2013 CHUM experience The future

4
Time is Brain! During an acute ischemic stroke 1.9 million neurons, 14 billion synapses, 12 km of myelinated fibres Are lost PER MINUTE Stroke. 2006 Jan;37(1):263-6
:")
5
La pénombre ischémique
Occlusion artérielle Baisse de CBF “Coeur” de l’infarcissement: CBF trop bas pour maintenir l’intégrité membranaire des cellules (échec des pompes ioniques) <10ml/100g/min Mort cellulaire en qq minutes Pénombre ischémique: CBF trop bas pour soutenir activite électrique, mais intégrité membranaire intacte 10-20ml/100g/min Tissu pouvant être “sauvé”
 <10ml/100g/min. Mort cellulaire en qq minutes. Pénombre ischémique: CBF trop bas pour soutenir activite électrique, mais intégrité membranaire intacte ml/100g/min. Tissu pouvant être sauvé")
6
Basic principle of acute ischemic stroke therapy: rapid and complete recanalisation of the arterial occlusive lesion!

7
In the subgroup of patients in whom occurrence of recanalization was assessed within 6 hours of onset, good outcome was achieved in 50.9% of recanalized patients versus 11.1% of nonrecanalized patients, (odds ratio, 6.36; 95% CI, 3.32 to 12.17). Courtesy A. Demchuk

8
Neurology. 2009 September 29; 73(13): 1066–1072
IMS 1 et 2 Neurology September 29; 73(13): 1066–1072
: 1066–1072.")
9
Traitement standard: Thrombolyse IV

10
AVC aigu: Thrombolyse 0-6 hrs
Lancet 2012 Jun 23;379(9834):
:")
11
IST-3 RCT ouvert 156 hôpitaux dans 12 pays européens
3035 patients traités avec placebo vs tPA-IV 1515 tPA, 1520 placebo

12
IST-3 OTTT médian: 4.2 heures Issue favorable: 37% vs 35% (p=0.181)
HIC à 7 jours: 3% vs 1% (p<0.0001) Mortalite à 6 mois: 27% vs 27% (p=0.672)
 Mortalite à 6 mois: 27% vs 27% (p=0.672)")
13
Negative study, but supports IV tPA use
In patients >80 years-old Within < 3 heures

14
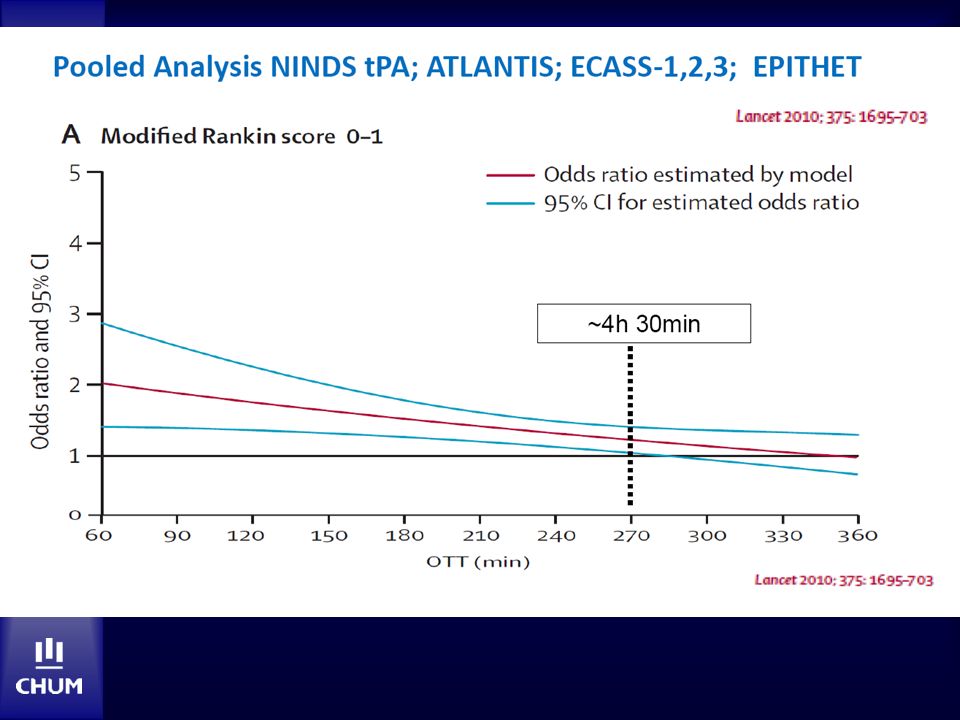
tPA IV: Méta-analyse 2010 NINDS, ATLANTIS, ECASS (1, 2, et 3) et EPITHET (n=3670) “Outcome” favorable (mRS 0-1) Delai de Tx (min) OR (95% CI) NNT 0-90 2.6 ( ) 4.5 91-180 1.6 ( ) 9 1.3 ( ) 14.1 1.2 ( ) 21.4 Ajout IST-3 ne change pas ces conlusions (<3 heures) Lees KR et al. Lancet. 2010;375(9727):1695.
 OR (95% CI) NNT ( ) ( ) ( ) ( ) Ajout IST-3 ne change pas ces conlusions (<3 heures) Lees KR et al. Lancet. 2010;375(9727):1695.")
17
YD Meretoja et al. Neurology 2012; 79:

18
YD Neurol.; 79:

19
Del zoppo Angio Saqqur et Zangerle TCD Courtesy A. Demchuk

20
tPA IV Avantages Disponibilité Acces rapide Facilité d’administration
Bénéfice clinique documenté dans plusieurs études et registres Inconvénients Faible taux de recanalisation (TIMI 2-3)1 CI 10% ACM M1 25% M2-M3 40% Hémorragie intracérébrale Hémorragie systémique 1 Wolpert AJNR 1993, Yamaguchi Cerebrovasc Dis 1993, Mori, Neurology 1992
1. CI 10% ACM M1 25% M2-M3 40% Hémorragie intracérébrale. Hémorragie systémique. 1 Wolpert AJNR 1993, Yamaguchi Cerebrovasc Dis 1993, Mori, Neurology")
21
Endovascular therapy

22
Endovascular therapy (tPA +/- mechanical thrombectomy)
Avantages Meilleurs taux de recanalisation: 40-85% Plus longue fenêtre de Tx ? Visualisation en temps réel de la recanalisation Inconvénients Delai entre AVC et angio Centres spécialisés seulement Complications (dissection, perforation etc.) Embolies distales Anesthésie/intubation?
 Embolies distales. Anesthésie/intubation")
23
Intra-arterial thrombolysis
PROACT II RCT de patients avec occlusion ACM traités en <6 heures NIHSS médian = 17 Pro-urokinase IA + héparine IV (n=121) vs héparine IV (n=59) Recanalisation (par angio): 66 vs 18% (p<0.001) mRS 0-2 a 90 jours: 40% vs 25% (p=0.04) HIC symptomatique: 10% vs 2% (p=0.06) Furlan A et al. JAMA. 1999;282(21):2003.
 vs héparine IV (n=59) Recanalisation (par angio): 66 vs 18% (p<0.001) mRS 0-2 a 90 jours: 40% vs 25% (p=0.04) HIC symptomatique: 10% vs 2% (p=0.06) Furlan A et al. JAMA. 1999;282(21):2003.")
24
Mechanical thrombectomy
3 appareils approuvés par le FDA MERCI Penumbra Solitaire Registres, séries mono-centriques, contrôles historiques

25
Mechanical thrombectomy
MERCI

26
MERCI Study N=151 Contre-indication au tPA-IV <3hrs ou Tx 3-8 hrs
Occlusion CI, ACM, AB, AV NIHSS médian = 19 Comparaison avec groupe témoin de PROACT-II Recanalisation 46% vs 18% sICH 8% vs 2% Mortalité 44% vs 27% mRS 0-2 à 90jrs 27.7% vs 25% Recanalisation associée avec meilleur outcome mRS 0-2: 46% vs 10% Smith WS et al. Stroke. 2005;36(7):1432.
:1432.")
27
Multi MERCI trial N=164 NIHSS médian = 19
Tx IA ad 8 hrs avec CI au tPA-IV ou après «echec» de tPA-IV Recanalisation 57.3% mRS 0-2 à 90jrs 36% sICH 9.8% Mortalité 34% Smith WS et al. Stroke Apr;39(4):
:")
28
Multi MERCI trial Smith WS et al. Stroke Apr;39(4):
:")
29
Mechanical thrombectomy
PENUMBRA

30
Penumbra pivotal stroke trial
Tx IA ad 8 hrs avec CI au tPA-IV ou après «echec» de tPA-IV Recanalisation 81.6% mRS 0-2 à 90jrs 25% sICH 11.2% Mortalité 32.8% Stroke Aug;40(8):
:")
31
Mechanical thrombectomy “Stentrievers”
SOLITAIRE TREVO

32
Lancet Oct 6;380(9849):
:")
33
Lancet 2012 Oct 6;380(9849):
:")
34
Combined therapy or “bridging”

35
IV-IA “bridging”: l’evidence
Emergency Management of Stroke (EMS) tPA IV/IA (n=17) versus placebo IV/tPA IA (n=18) Meilleure recanalisation (TIMI 2-3) pour IV/IA (81% versus 50%) Pour occlusions M1-M2: 100% recanalisation Lewandowksi CA et al. Stroke Dec;30(12):
 tPA IV/IA (n=17) versus placebo IV/tPA IA (n=18) Meilleure recanalisation (TIMI 2-3) pour IV/IA (81% versus 50%) Pour occlusions M1-M2: 100% recanalisation. Lewandowksi CA et al. Stroke Dec;30(12):")
36
IV-IA “bridging”: l’évidence
IMS I Jan-Oct 2001 IV-IA < 3 heures avec NIHSSS ≥ 10 (median 18) “Open-label” sans groupe contrôle n=80 Pour NIHSS ≥ 20 mRS 0-2 a 3 mois: IMS I 42% NINDS tPA 21% Stroke. 2004;35(4):904. Comparaison avec cohort NINDS
 Open-label sans groupe contrôle. n=80. Pour NIHSS ≥ 20. mRS 0-2 a 3 mois: IMS I 42% NINDS tPA 21% Stroke. 2004;35(4):904. Comparaison avec cohort NINDS.")
37
IV-IA “bridging”: l’évidence
IMS II Prolongation de IMS I avec ajout du système EKOS MicroLysus n=73 NIHSSS médian = 19 IMS II versus NINDS tPA mRS 0-2 a 3 mois: 48% versus 36% Stroke. 2007;38(7):2127.
:2127.")
38
Combined IV-IA therapy: the evidence
RECANALISE Registre prospectif “before and after” tPA IV versus tPA IV + endovasculaire IV (n=107) IV-IA (n=53) P value Recanalisation 52% 87% <0.0001 Early neurological improvement 39% 60% 0.07 mRS 0-2 at 90 days 44% 57% 0.13 Death at 90 days 17% 0.98 sICH 11% 9% 0.73 Mazighi M et al. Lancet Neurol Sep;8(9):802-9.
 IV-IA (n=53) P value. Recanalisation. 52% 87% < Early neurological improvement. 39% 60% mRS 0-2 at 90 days. 44% 57% Death at 90 days. 17% sICH. 11% 9% Mazighi M et al. Lancet Neurol Sep;8(9):")
39
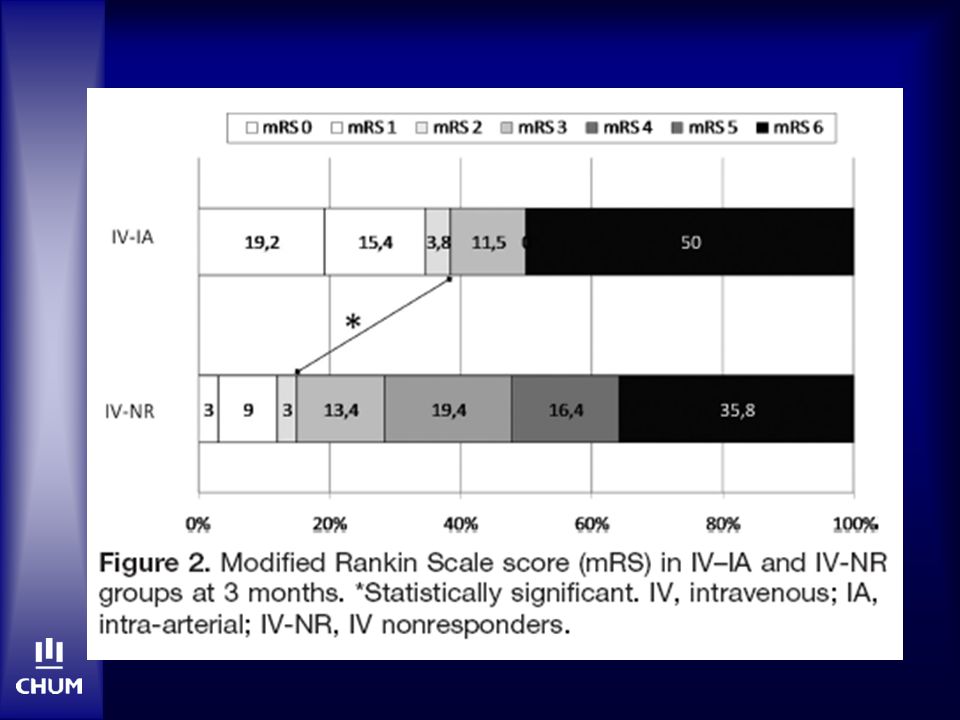
IV-IA “bridging”: l’évidence
Étude retrospective comparant 2 groupes: tPA IV-IA (n=42) vs tPA IV sans amélioration à 1 heure (n=84) Equilibrés pour occlusion, NIHSS et temps de Tx avec tPA-IV NIHSS médian = 20 Occlusion documentée par TCD Rubiera M et al. Stroke. 2011;42:
 vs tPA IV sans amélioration à 1 heure (n=84) Equilibrés pour occlusion, NIHSS et temps de Tx avec tPA-IV. NIHSS médian = 20. Occlusion documentée par TCD. Rubiera M et al. Stroke. 2011;42:")
41
Should we call our INRs?

42
Thrombolyse au CHUM Année Nombre de cas IV-IA Nombre de cas IV
Nombre de cas IA seul 2003 31 3 2004 1 24 7 2005 9 2006 2 32 2007 34 2008 5 36 11 2009 13 48 10 2010 17 43 12 2011 26 60 2012 22 62 29 Données colligées par R. Cournoyer

43
Thrombolyse au CHUM YD 105 IV seul IA seul Combiné Années 2001 à 2012
Données colligées par Y. Deschaintre et R. Cournoyer

44
CHUM experience N=39 (nov 2009 – janv 2011) NIHSS moyen = 18.7
MERCI: 4 (+ Penumbra ou ballon) (10%) Penumbra: 33 (85%) Solitaire: 1 (2%) Recanalisation 66% mRS 0-2 à 90jrs 33% Mortalité 10% Courtesy Dr. F. Bing, unpublished data
 (10%) Penumbra: 33 (85%) Solitaire: 1 (2%) Recanalisation 66% mRS 0-2 à 90jrs 33% Mortalité 10% Courtesy Dr. F. Bing, unpublished data.")
45
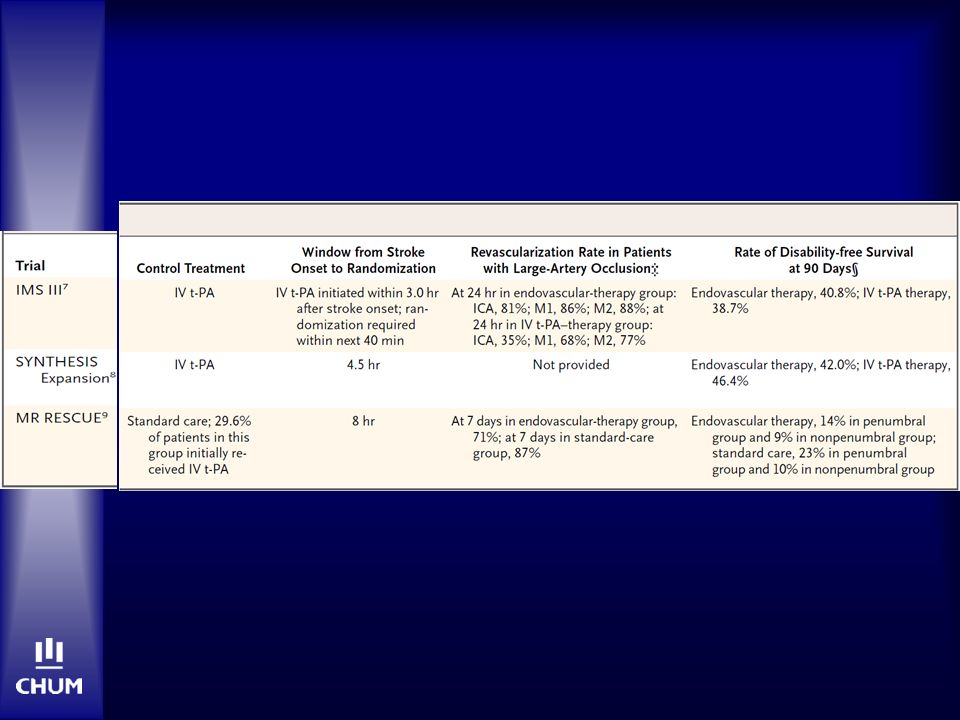
NEJM February 7th 2013

48
Phase 3 RCT, open-label with blinded outcome
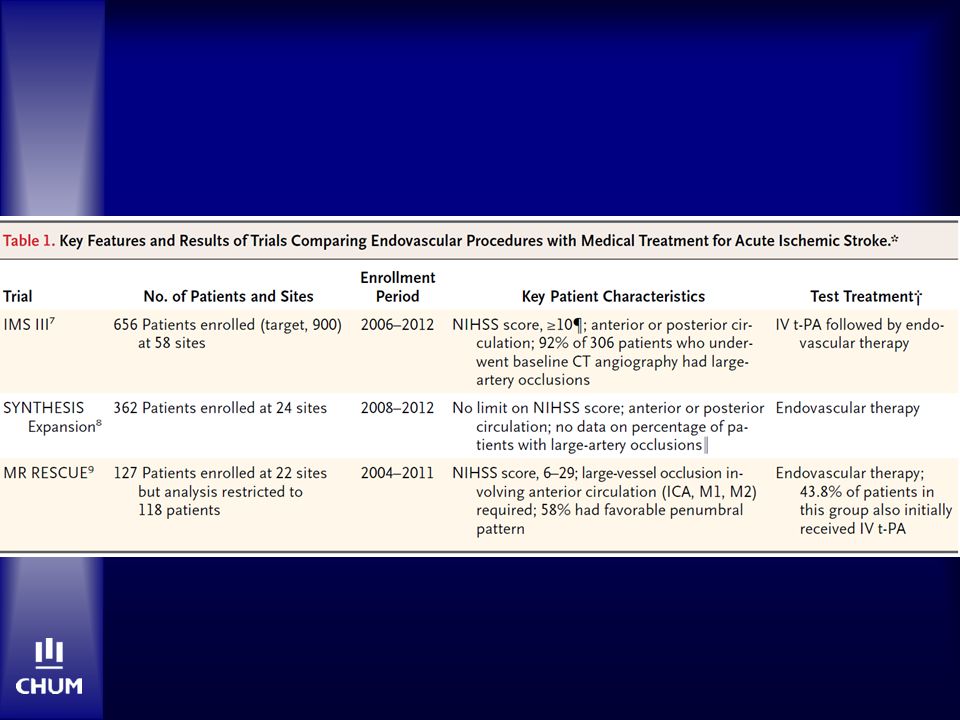
N=656 (IV only=222, IV-IA=434) Tx within 3 hours IA Tx within 5 hours and not beyond 7 hours MERCI, Ekos, Penumbra, Solitaire N Engl J Med 2013;368:
 Tx within 3 hours. IA Tx within 5 hours and not beyond 7 hours. MERCI, Ekos, Penumbra, Solitaire. N Engl J Med 2013;368:")
49
mRS 0-2: 40.8% vs 38.7% (95% CI %) N Engl J Med 2013;368:
 N Engl J Med 2013;368:")
50
IMS-3

51
IMS-3

53
IMS-3: Recanalisation* rates at 24hrs
IV only IV-IA ICA 35% 81% M1 68% 86% M2 77% 88% *Partial or complete on follow-up CTA

54
IMS-3: post-mortem IV tPA better than we assumed?
Patients treated too late? Ischemic changes too extensive? (>40% ASPECTS <8) Less effective first-generation devices? >40% ASPECTS <8
 Less effective first-generation devices >40% ASPECTS <8.")
55
SYNTHESIS Expansion N Engl J Med 2013;368:904-913
Pragmatic open-treatment RCT with blinded endpoint N= 362 (IV=181, IA=181) Median time to treatment (p<0.001) IV: 2.75 hrs IA: 3.75 hrs
 Median time to treatment (p<0.001) IV: 2.75 hrs. IA: 3.75 hrs.")
56
mRS 0-1: 30.4% vs 34.8% (95%CI ) Synthesis N=181 par groupe. IV vs IA
 Synthesis N=181 par groupe. IV vs IA")
57
SYNTHESIS Expansion

58
MR Rescue N Engl J Med 2013;368:914-923
30% mismatch 90cc final infarct volume Mean time to enrollment 5.5hrs 67% reperfusion in IA group

59
IV tPA remains the only proven recanalisation therapy for stroke within 4.5hrs
Patients receiving IV tPA within 2 hours and endovascular Tx within 90 minutes of IV tPA may benefit Extension of the treatment time window using penumbral imaging remains unproven

60
Can guidelines help?

61
Endovasclar therapy Canadian Best Practise Recommendations 2010

62
Endovasclar therapy AHA Guidelines 2013

63
Endovasclar therapy ACCP Guidelines 2012

64
When to consider endovascular therapy...
Clinical Age? Stroke severity (NIHSS >20?) Ultra-rapid door-to-clot time possible Imaging Small core volume Occlusion site “Clot burden/length” (>2cm) Significant mismatch? Good collaterals
 Ultra-rapid door-to-clot time possible. Imaging. Small core volume. Occlusion site. Clot burden/length (>2cm) Significant mismatch Good collaterals.")
65
Stroke 2011 Jan;42(1):93-7 Courtesy A. Demchuk
ASPECTS <5 do not benefit Courtesy A. Demchuk

66
Algorithm for acute recanalisation therapy <4.5hrs

67
Case 1 E/P: SVS Hemiparesie G Hemianesthesie G avec heminegligence G
Dysarthrie NIHSS 15 Labos: OK ID: Homme 71 ans, droitier HMA: Hémiplégie gauche et dysarthrie à 8h00 ATCD: Insuffisance cardiaque (FEVG 25%) FAP Néo vessie 67
 FAP. Néo vessie. 67.")
68
CT C- à 9h47

70
CTA-Source Images Bolus tPA-IV à 10h15

71
Recanalisation TICI 3 à 11h25

72
CT C- à 48 heures Congé jour 5 avec NIHSS 1

73
Case E/P: SVS Hemiplegie B-F D Aphasie globale severe NIHSS 18
ID: Femme 68 ans, droitiere HMA: Plegie hemicorps D avec mutisme a 13h50 ATCD: Anemie severe (rectorragie) Tabagisme E/P: SVS Hemiplegie B-F D Aphasie globale severe NIHSS 18 Labos: Hb 60 ECG: FA
 Tabagisme. E/P: SVS. Hemiplegie B-F D. Aphasie globale severe. NIHSS 18. Labos: Hb 60. ECG: FA.")
74
CT C- 14h00 ASPECTS 4 (insula, lentiform, M1, M2, M4,M5)
")
76
Echec de Tx endovasculaire –
angioplastie, MERCI, tPA-IA

77
Jour 1 NIHSS 20

78
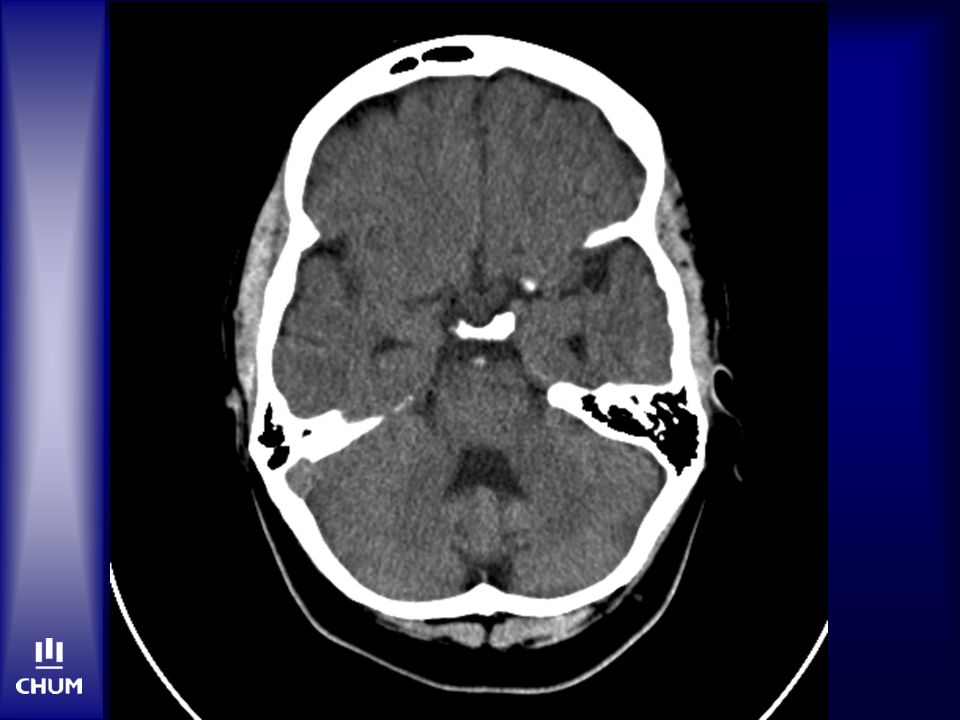
Case 23 year-old woman, no PMH Sudden onset nausea, vomiting
Altered level of consciousness Brought to peripheral hospital Rapidly progressive bilateral facial weakness, tetraparesis, dysarthria and dysconjugate gaze

79
Baseline NCCT (<2hrs after onset)
")
81
CTA 4 hrs post-onset

82
Angio 5 hrs post-onset

83
Recanalization 5h45min post-onset

84
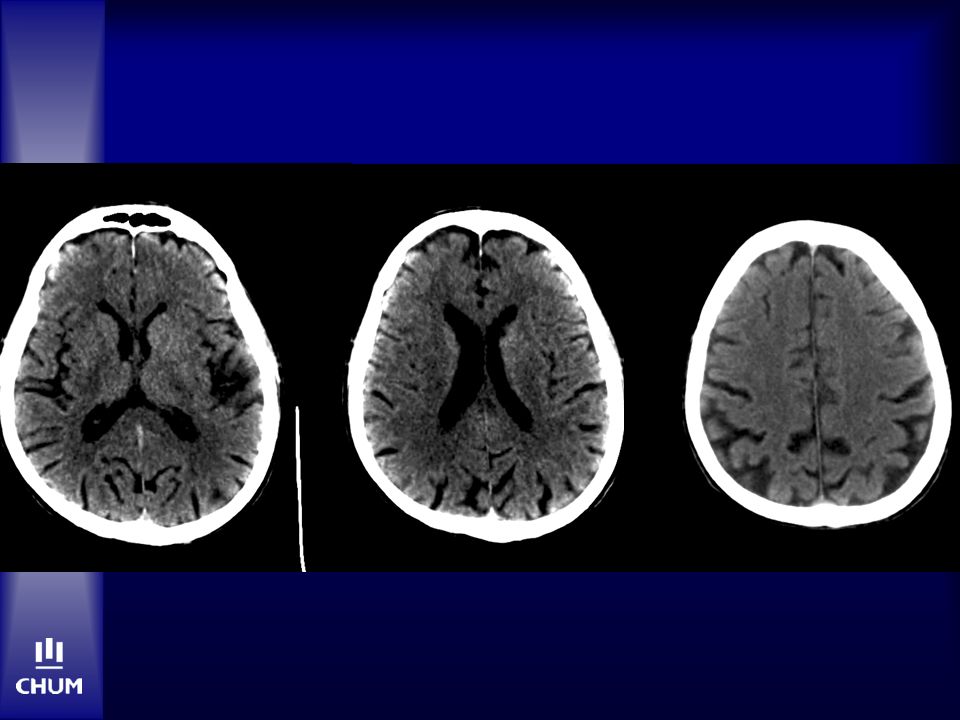
NCCT Day 4 NIHSS 0, mRS 0 at 3 years 84

85
Conclusions Degree of recanalisation and time to recanalisation are associated with better outcomes Recanalisation rates are modest with IV tPA Recanalisation rates are higher with endovascular therapy Newer generation stentrievers are superior to MERCI for opening arteries (and possible improving outcomes)
")
86
Conclusions The discordance between better angiographic results and clinical outcomes despite comparable safety, suggests that patient selection may be the problem Endovascular therapy has a similar safety profile as IV tPA After IMS-3, endovascular therapy remains unproven...

87
Enroll patient in a study

88
Ongoing or planned studies
EASI ESCAPE SWIFT prime REVASCAT BASICS-2 THRACE …

89
Merci

90
Algorithme pour l’approche IV vs IV-IA vs IA

91
Algorithme pour l’approche IV vs IV-IA vs IA

92
Case 2 – Mr. RD 75 year-old RHD male PMH: Meds:
Lives with wife, baseline mRS 0 PMH: HTN Never-smoker Meds: Acebutalol 400 mg qd

93
Case 2 – Mr. RD HPI: 19h17: witnessed sudden onset R hemiplegia, speech arrest and fall. 911 called. 19h27: ambulance arrival on site 20h04: arrival at HND 20h13: NCCT 20h30: stroke team assessment Dysarthria, expressive aphasia, R hemiplegia NIHSS 13

94
NCCT 1 hour

96
Case 2 – Mr. RD NCCT L eye deviation, L HMCA ASPECTS 10 CTA not done…
Obvious HMCA Disabling NIHSS Avoid delays to Angio (NCCT already done)
")
97
Case 2 – Mr. RD 20h55: IV t-PA bolus, 2/3 dose
21h05: Angio suite. No sedation.

98
Angio 2 hours No collateral runs due to time and anatomy
Traverse occlusion with microcatheter, distal injection reveals M1 occlusion Angio 2 hours

99
Penumbra limited by length of microcatheter via occlusion, with access only to proximal face of clot. 10mg IV-tPA injected. 18 mg total Angiplasty carotid occlusion, allowing better access to M1 clot – Thromboaspiration with Penumbra and good recanalization. Sluggish distal flow. Carotid stent (Precise) deployed and angioplastied
 deployed and angioplastied.")
100
Final run: sluggish flow distally, some blushing in the lenticulostriates
22h40: M1 recanalization

101
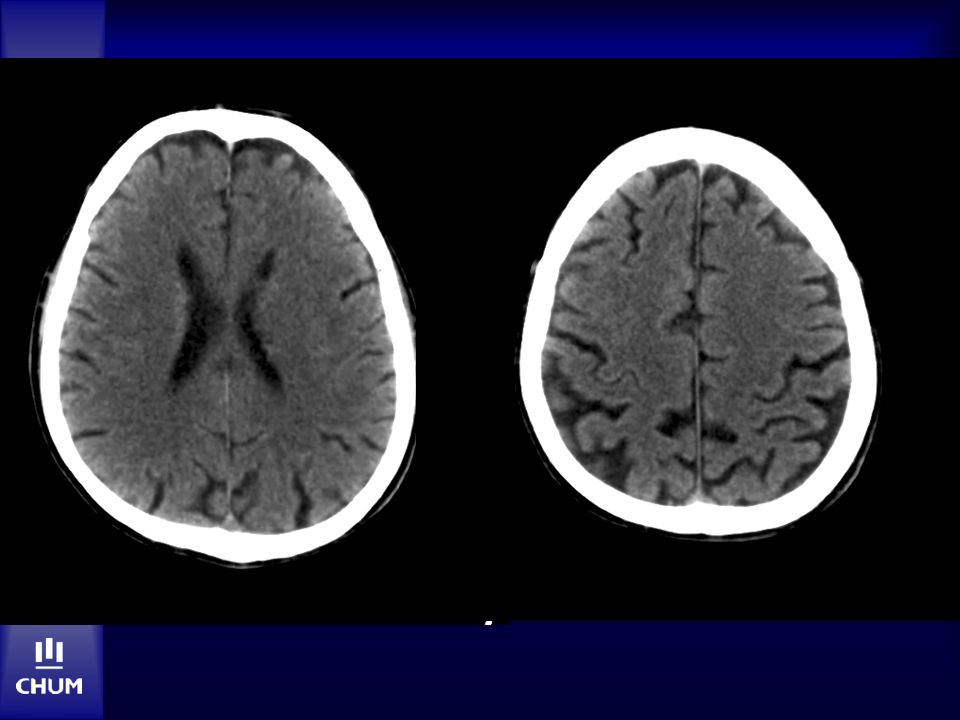
NCCT day 1

103
Case 2 – Mr. RD Favourable in-hospital course
Discharged on ASA + Clopidogrel + atorvastatin NIHSS 1 at discharge At 6 months and 1 year: NIHSS 0 mRS 2 (no longer drives car)
")
104
M. N. Homme de 62 ans, droitier AVC ACM gauche CT… DLP Db2 de novo
Déficit fluctuant; NIHSS 16 10 Famille indécise re. tPA CT…

105
ASPECTS 10

106
M. N. tPA-IV Hyperglycémie malgré insuline IV
OTTT: 3h15 Hyperglycémie malgré insuline IV Aucune amélioration clinique

107
CT: 18 hres

108
CTA: 18 hres

109
CTA: 18 hres Internal cerebral vein sign Bilat ACA via RICA

110
M. N. Jour 3 Plus somnolent, mutique Parésie jambe gauche

111
Angio-IRM: jour 3

112
IRM: jour 3

113
M. N. Jour 5 Comateux Mydriase fixe OS
Consult NeuroChx aucune intervention

114
CT: jour 5

115
M. N. Jour 6: Comateux, tetraplégique Mydriase bilatérale
Soins de confort Décès le même jour

116
CT: jour 6

117
M. A.: un autre exemple... Homme de 50 ans, droitier AVC ACM gauche
Aucuns antecedents AVC ACM gauche NIHSS 9 (aphasie) CT: pas de changements precoces tPA-IV
 CT: pas de changements precoces. tPA-IV.")
118
CT: 18 hres

119
CTA: 18 hres

120
M. A. 24 hres post-tPA Deterioration subite NIHSS 23

121
CTA: 24 hres IA = echec

122
M. A. NIHSS ~ 20 au conge

Présentations similaires

















 Informative Seminar Séminaire informatif Leuven,>")
 you have to do a bit of math. In French, you don’t say « 4: 50».>")



