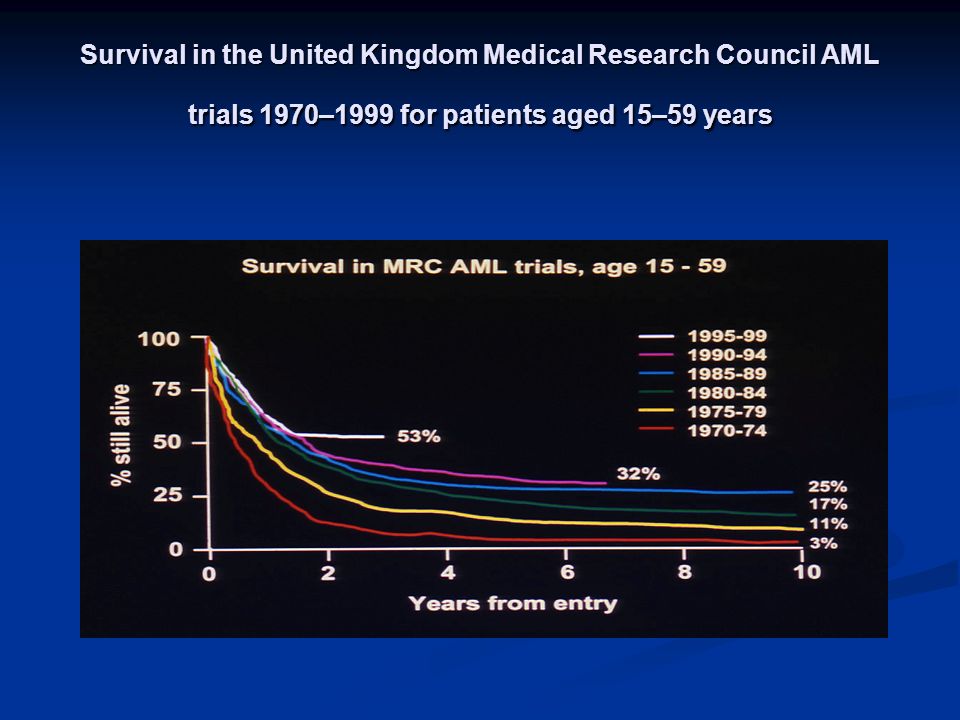
Survival in the United Kingdom Medical Research Council AML trials 1970–1999 for patients aged 15–59 years
FACTEURS PRONOSTIQUES - liés au malade performance status âge liés à histoire de la maladie (de novo/secondaire) - liés à la présentation clinique / biologique tumeurs taux GB LDH - liés au type LAM cytologie M3, M2-M4 / M6-M7 phénotype (CD34, Pgp) cytogénétique biologie moléculaire - liés à la réponse au traitement RC en 2 cures (MRC) blastose a J15 (German AMLCG)
GOELAM2 TRIAL PROGNOSTIC FACTORS CR achievement (multivariate analysis) - karyotype (0.0004) - WBC count (0.002) - PS (0.002) DFS (multivariate analysis) - karyotype (0.0004) - allo BMT (0.005)
t(15;17) t(8;21) inv(16)/t(16;16) CR (%) ID (%) RD (%) 11** 88 2** 98** 2** 0** 92* 8 0* 6 71** 23** t(9;22) t(6;9) t(11q23) inv(3)/t(3;3) t(3;5) ** 19 47** ** 36** t(12p13) abn(11p13~5) t(8p11) Outcome according to hierarchical cytogenetic classification n *p<0.01, **p<0.001, Chi-squared test or Fisher exact test (CR/ID/RD), log rank test (RR & OS) RR (%,5yrs) OS (5yrs) 23** 69** 22** 70** 35* 61* 92** 5** 84** ** 6** ** normal
abn(16q22~24) -5/5q/-7/7q 7q, no adverse CR (%) ID (%) RD (%) ** 9 27** ** 426** del(9q) * * 1419 del(11)(q23) abn(3q) 12* 78** 11Other Outcome according to hierarchical cytogenetic classification n RR (%,5yrs) OS (5yrs) ** 16** * 70 20* 53 37** ** 26 89** 8** 48 37* normal *p<0.01, **p<0.001, Chi-squared test or Fisher exact test (CR/ID/RD), log rank test (RR & OS)
Outcome in AML patients with 11q23 abnormalities ID (%) CR (%) RD (%) Median age RR (%,5yrs) OS (5yrs) t(11q23) total (n=212) t(6;11)(q27;q23) (n=21) t(9;11)(p21~2;q23) (n=73) t(10;11)(p11~4;q13~23) (n=46) t(11;19)(q23;p13) (n=18) Other t(11q23) (n=54) p value for heterogeneity <0.01 NS
Impact of additional cytogenetic abnormalities: Survival of patients entered into AML 10 & 12 (n=3453) Years from entry % still alive Favourable only (n=478) Favourable + intermediate (n=331) Favourable + adverse (n=22) Intermediate only (n=2235) Adverse + intermediate (n=297) Adverse only (n=478) 71% 65% 59% 42% 17% 14%
PROGNOSTIC IMPACT OF KARYOTYPE PtsFavorableIntermediateunfavorable MRCEBMTSWOG/ECOG t(8;21)t(15;17)inv(16)t(8;21) Abnormaliti es of 16 t(8;21) All others Including 11q23 Abnormalitiest(15;17) Pseudidiploid hyperdiploid or diploid Normal +8, -y, +6, del (12p) Complex -5, (del 5q) -7 abnormalities of 3q Abnormalities of 5 and/or 7 Abnormalities of 11q hypodiploid -5, del (5q) -7, del (7a) Inv 3 Complex abnormalities of 11q, 20q, 21q Del (9q) t(6;9), t(9;22) Abn 17p
TRAITEMENT DINDUCTION « Gold standard » : DNR +ARA-C 3 (45-50 mg/m2) + 7 (200 mg/m2) Variantes (100mg/m2) -Doses plus élevées de DNR (60-90 mg/m2) -IDR (12-13 mg/m2 x 3 ou 8mg/m2 x 5 ) -3eme drogue (6TG Etoposide)
TRAITEMENT DINDUCTION - Facteurs de croissance hématopoiétique - Modulateurs mdr -Hautes doses dARA-C (1 à 3 g/m2, seule ou associée à anthracyclines ou Fludarabine ) - Date dadministration de la deuxième cure
G-CSF DANS LES LAM G-CSFR EXPRIME A LA SURFACE DES BLASTES DE LAM Après traitement dinduction - nombreuses études randomisées avec G ou GM-CSF (surtout chez le sujet âgé) - diminution de la durée neutropénie de 2 à 6 J - augmentation du taux de RC seulement dans 2/9 - pas dimpact sur la survie ou EFS - généralement diminution de la durée dhospitalisation et de lutilisation dATB - réduction du cout dhospitalisation dans 2 études - pas daugmentation du risque de progression ou de rechute Après consolidation - 2 études (Heil Blood 1997, Harousseau JCO 2000) Réduction de la durée neutropénie et dhospitalisation
PRIMING DANS LES LAM Neuf études randomisées avec G ou GM-CSF Nombre de patients et modalités dadministration du FCH variables pas daugmentation significative du taux de RC quelques arguments en faveur du priming - Witz (Blood 1998) : augmentation de la DFS à 2 A surtout entre 55 et 65 A (57% vs 20%) p=0.002) - Lowenberg (NEJM 2003) : augmentation de la DFS à 4 A (42% vs 33%) et de la SV dans les LAM à risque standard (45% vs 35%)
MODULATEURS MDR - Gène code pour protéine pgp (réduit concentration intracellulaire des anthracyclines et de VP16 ) - Expression de pgp - corrélée à pronostic défavorable (Marie 91,Pirker 91,Campos 92) -associée à dautres facteurs de mauvais pc (CD34,Cytogénétique,LAM réfractaires ou en rechute) -rare au Dg chez sujets jeunes mais fréquente chez sujets agés (Leith 97) *
MODULATEURS MDR - Cyclosporine - 1 essai >0 ds LAM à haut risque (List,Blood 2001 ) - 1 essai <0 (Liu,BJH 2001) - PSC essais interrompus précocément ou négatifs (Baer Blood 2002, Greenberg JCO 2004, Chauncey) -Cyclo et PSC modifient la pharmacocinétique des drogues dont il faut réduire les doses (Kolitz JCO 2004)
Modulateurs MDR (GOELAM 2 ) pts A Quinine 30 mg/kq pdt ind et 2 conso 81% RC,à 3A DFS 43%,SV 42% Globalement pas de différence entre les deux bras - Pas de valeur pronostique de mdr et pgp - Mais sous-groupe de 54 pts avec efflux de rhodamine +) : 83% RC vs 48% avec quinine
HAUTES DOSES ARA-C BD100mg/m²/PCx7HD 3g/m² (J1,3,5,7 ) SD200mg/m²/PCx7HP 2g/m²x2 J1-6 % RC Durée med RC DFS (%) SV (%) m 24*25*71 45 m 49*31*58 < 50A < 50A * À 5 ans BISHOP Blood pts A denovo Weick Blood pts < 65 A De novo ou secondaire
DATE ADMINISTRATION 2ème CURE - A sortie daplasie après 1ère (ou à J30) - En fonction des résultats du myélogramme intermédiaire (J15) - Systématiquement (quel que soit le résultat dun éventuel myélogramme intermédiaire) - timed-sequential - double induction
TRAITEMENT INDUCTION 2ème CURE - Timed sequential « Intensive timing » vs standard timing (Woods Blood 1996) pas de différence en taux de RC mais EFS à 3A 42% vs 27% - Double induction (Buchner Blood 1999) soit reprise traitement induction standard (TAD/TAD) soit 2ème cure + intense (TAD/HAM) : TAD/HAM supérieur dans formes de mauvais pronostic - Comparaison 3 modalités (Castaigne Blood 2004) * pas de différence en taux RC (76%) ou en taux de décès toxique * timed-sequential retarde la rechute < 50A
TRAITEMENT INDUCTION - Avec les progrès de la réanimation hématolo- gique : taux de décès toxique < 5% et taux de RC élevés dans les LAM de novo < 60A - Difficile de démontrer la supériorité dun régime par rapport à un autre pour le taux de RC - « qualité » de RC peut expliquer certaines différences en DFS - Taux de RC dépend des facteurs pronostiques initiaux (cytogénétique +++)
POST-REMISSION THERAPY IN AML Allogeneic BMT - Most effective antileukemic treatment Myeloablative preparative regimen GVL effect - High incidence of severe procedure-related toxicity High transplant-related mortality Indicated only in patients < 55 yo - Only patients with an HLA-identical sibling
POST-REMISSION THERAPY IN AML AUTOLOGOUS SCT - Toxic death rate much lower than after allo BMT - High relapse rate Contamination by malignant cells Absence of GVL - Age limit 60 y - Uncontrolled studies have shown DFS rates of 30% to 60% In AML CR1 Selection bias ?
POST-REMISSION THERAPY ICC - Non myeloablative - Age limit : 60y - High relapse rate - DFS 30-50% in pilot uncontrolled studies
RANDOMIZED TRIALS COMPARING ASCT AND ICC DFS PtsAutoChemop Adult studies Zittoun 95 Harousseau 97 Burnett* 98 Cassileth 98 Pediatric studies Ravindranath 96 Woods** (128) 44 (86) 53 (190) 35 (116) 38 (89) 42 (177) 30 (126) 40 (78) 40 (191) 35 (117) 36 (115) 47 (179) *Autologous BMT was compared to no further treatment after 4 courses of intensive chemo ** Bone marrow was purged with 4 HC in the autologous transplantation arm. Number of patients is shown in parenthses
RANDOMIZED TRIALS COMPARING ASCT AND ICC OS PtsAutoChemop Adult studies Zittoun 95 Harousseau 97 Burnett* 98 Cassileth 98 Pediatric studies Ravindranath 96 Woods** *Autologous BMT was compared to no further treatment after 4 courses of intensive chemo ** Bone marrow was purged with 4 HC in the autologous transplantation arm. Number of patients is shown in parenthses
COMPARISON AMBT / ICC RELAPSE RATE AND TOXIC-DEATH ABMTICCABMTICC Adult studies Zittoun 95 Harousseau 97 Burnett* 98 Cassileth 98 Pediatric studies Ravindranath 96 Woods** *Autologous BMT was compared to no further treatment after 4 courses of intensive chemo ** Bone marrow was purged with 4 HC in the autologous transplantation arm. Relapse (%)Toxic death (%)
ABMT / ICC No convincing evidence that unpurged ABMT is superior to the best available CT Lower relapse rate but higher toxic death rate with ABMT Strategies to reduce TRM are needed
ALLO versus AUTO AML in CR1 RETROSPECTIVE COMPARISONALLON=516AUTON=598 p value TRMRelapseLFS p< EBMT (Gorin 1996)
Comparison of allogeneic BMT autologous BMT and ICC Number of patients in shown in parentheses DFS intention to treat Age limit (years) AUTOALLOCHEMO ZittounCassilethWoods (n=128) 35 (n=116) 42 (n=179) 55 (n=168) 43 (n=113) 55 (n=177) 30 (n=126) 35 (n=117) 47 (n=179)
THE ROLE OF ALLOGENEIC BMT DONOR / NO DONOR ANALYSIS Age limit Pts with HLA id sibl Donor No donor Donor No donnor EORTCBGMTGOELAMMRC %66%44%54% 33% (p=0.01) 42% (p=0.05) 38% (p=0.6) 42% (p=0.006) 48%65%53%57% 40% p=NS 51% p=NS 53% p=NS 50% p=NS DFS Overall survival
DFS ALLO COMPARISON GOELAM1 / GOELAM GOELAM 2 56% GOELAM 1 42% p = 0.05
GOELAM 2 COMPARISON CHEMO / ALLO DFS (Intent to treat) Allo 56% Chemo 41% p = 0.017
PROGNOSTIC VALUE OF KARYOTYPE (ALLO BMT) FerrantGrimwadeFerrantFerrantGrimwade GoodStandardPoor Relapse LFS SV
DONOR VS NO DONOR ROLE OF CYTOGENETICS Donor No donor Donor Donor NoRelapseDFSSV Good risk Standard risk Poor risk MRC 10 (A. Burnett) donor vs no donor
AML10 and AML12 Recruits <45 years n = CR 729 Donor1231 No Donor 427 Transplant (60%)
AML 10 & 12: Overall Survival Donor vs No Donor
AML 10 & 12 Donor vs no donor comparisons Overall survival stratified by risk group
AML 10 & 12 Donor vs no donor comparisons Overall survival stratified by age
EORTC AML 10 Comparison ALLO / AUTO 1198 Pts < CR 734 IC 293 DONOR 441 NO DONOR ALLO 69% AUTO 56% 4 year DFS 52% 42%
ALLO vs AUTO EORTC-GIMEMA (AML10) Suciu Blood pst in CR1 < 46 yo 293* sibling 441** no donor donor p value 4yr DFS 4 yr SV* RR Death in CR 52%58%30%17%42%51%52%5% <0.0001< Intent to treat analysis * Allo performed in 69% cases ** auto performed in 56% cases
EORTC AML 10 COMPARISON ALLO / AUTO ACCORDING TO CYTOGENETICS (4 yr DFS) Definition t(8;21) inv 16 NN, -y all others Donor 68% 53% 50% No Donor 74% 54% 29.5% GOOD INTERMEDIATE BAD / VERY BAD
ALLO VS AUTO INFLUENCE OF AGE Donor No donor p-value (67) 55% (88) 55% (138) 49% (114) 41% (88) 38% (185) 46% EORTC-GIMEMA (AML 10) Suciu Blood – yr DFS Intent to treat Analyis
ROLE OF ALLO BMT IN AML - Good risk cytogenetics not indicated in CR1 not indicated in CR1 - Intermediate risk indicated in CR1 (MRC) indicated in CR1 (MRC) different definitions (MRC / EORTC) different definitions (MRC / EORTC) novel prognostic parameters novel prognostic parameters - Poor risk poor prognosis even with allo poor prognosis even with allo
RISK ADAPTED TREATMENT IN YOUNGER PATIENTS WITH DE NOVO AML Risk classification based upon cytogenetic profiles Define Tx strategy according to risk Specific molecularly defined entities New strategies (targeted to molecular abnormalities Flt-3)
LAM CBF Anomalie cytog Gène fusion FAB Fréquence t(8;21) AML 1 /ETO M % Rares après 60 ans Inv(16) t(16;16) CFB /MYH 11 M 4 eo 4 %
PRONOSTIC t(8;21) MRC* Bloomfield NGuyen N CR (%) 92** SV 5 ans (%) * protocoles AML 10 et AML 12 (3453 pts) ** 2% décès en induction
PRONOSTIC inv(16)/t(16;16) MRC* Delaunay N CR (%) 92** 93 PR (%) * protocoles AML 10 et AML 12 (3453 pts) ** 8% décès en induction SV (%) 61 58
TRANSLOCATION t(8;21) ROLE DE LALLOGREFFE Burnett (BJH 2002) Essai MRC AML10 : 1063 patients Etude donor / no donor Bénéfice de lallogreffe en DFS et en SV seulement dans le groupe de pronostic intermédiaire Réduction du risque rechute dans tous les groupes sauf CBF Pas dallogreffe en 1ère ligne pour ces malades dans AML12
TRANSLOCATION t(8;21) COMPARISON ALLO / AUTO At 3 y N Relapse Relapse EFS EFS SV SV AlloAuto NS NS Ferrant (EBMT)
TRANSLOCATION t(8;21) COMPARISON ALLO / CHEMO At 3 y N DFS DFS SV SV AlloChemo NS NS NGuyen (Blood 2002)
CHIMIOTHERAPIE DE CONSOLIDATION C. Bloomfield (Cancer Research 1998) Impact de ARA-C HD dans le groupe des LAM CBF [ t(8;21) inv(16) del(16) t(16;16) ] 3gN=18400mg/m²N=20100mg/m² N = 19 DFS à 5 A 78%57%16%
CHIMIOTHERAPIE CONSOLIDATION Byrd (JCO 1999) Les études CALGB successives Rôle du nombre de cycles ARAC-HD à 5 ans 1 cycle > 3 cycles N Rechute 62 0, DFS 38 0,03 71 SV 44 0,04 76
CONCLUSION Pronostic global favorable - taux très élevé RC - survie à 5 A 60% Allogreffe en 1ère ligne actuellement non recommandée Allogreffe pour certains malades ? - index GB élevé - maladie résiduelle après intensification
TRANSLOCATION t(8;21) DETECTION MALADIE RESIDUELLE Tobal Blood 2000 RRT-PCR quantitative 221 malades Iinductionréduction 2-3 logs Cconsolidationréduction 2-3 logs suppl. TTaux< / g RNA dans moelle < / g RNA dans sang compatible avec RC prolongée Définition de malades à haut risque de rechute
Constitutively activated receptor Internal tandem duplication of the FLT3 gene Agarose gel electrophoresis Ladder WT AML patients DDW PCR Transmembrane Ig-like domain Kinase insert Kinase 1 Kinase 2 C-terminus Juxtamembrane Internal tandem duplication WT Mutant
FLT-3 TANDEM DUPLICATIONS N of cases % with FLT-3 TD CR%* Inferior OS* Inferior EFS* Kiyoi 99 Kottaridis 01 Schnittger 02 Thiede 02 Frohling ** vs vs vs vs NSNS NS0.007 * Compared to AML without FLT-3 TD ** with normal cytogenetics
NEW GENETIC PROGNOSTIC FACTORS Frequency 4.5% 8% (normal karyotype) 36% 10% 11% (NK) Prognosis UNF FAV Author Nakano 2000 Döhner 2002 Karakas 2002 Van Waalwijk 2003 Baldus 2003 Preudhomme 2002 P53 mutation MLL PTD Bcl2 and WT1 EVI 1 BAALC CEBP mutation
HOW TO IMPROVE THE RESULTS OF ABMT 1) Purged marrow 2) PBSC 3) Double transplantations 4) Maintenance therapy
IN VITRO PURGING Retrospective analysis of the EBMT database suggested that purged marrow is superior in selected cases (Gorin) - After TBI - Slow responding to induction CT - Transplanted early Kinetics of engraftment slower No randomised study
Retrospective comparison of bone marrow and peripheral blood as the source of stem cells for autolgous transplantation in AML Authors Source of stem cell Granulocyte recovery (D) <0.5x10 9 /l Platelet recovery (D) Outcome VisaniVellengaReiffers Marrow n=21 PB n=23 Marro n=41 PB n=28 Unpurged marrow PurgedMarrowPB36 p<0.01 p< p<0.001 p< p< p<0.3 p< p<0.001 p< p< Identical relapse rate and DFS - Purged marrow better
PBSC vs BM AUTOLOGOUS TRANSPLANTATION NbRelapseLFS Non purged BM Purged BM PBSC EBMT retrospective analysis 1393 pts (Reiffers 2000) Hematopoietic recovery significantly quicker after PBSC Selection bias ?
CAN WE IMPROVE THE RESULTS OF ALLOGENEIC BMT 1)Reduce toxicity Better control of GVH and infectious complications Cord blood PBSC Reduced intensity conditioning 2)Reduce relapse Use matched unrelated donors
RANDOMIZED TRIALS COMPARING ALLOGENEIC PERIPHERAL BLOOD TO BONE MARROW Study Vigorito-1998 Blaise-2000 Powles-2000 Heldal-2000 Schmitz-1998 Couban-2002 Bensinger-2001 n PB BM ANC a PLT b TRM Agvhd Cgvhd OS PB BM PB,% ND BM,% ND PB,% BM,% PB,% BM,% PB,% ND BM,% ND 55 54
RIC for AML in 1st CR - 36 pts (26-60 y, med 52) - with comorbidity (12) or adverse prognostic factors (23) - Flu,Bu,ATG (2.5 to 10 mg/kg) - 20 conso with HDARA-C - 11 with double conso (2nd with ASCT) - 2 toxic deaths,11 relapses - Med F-up 16 m :65% DFS at 18 m - Prognostic factor :GVHD DFS (multivariate analysis) - karyotype (0.0004) - allo BMT (0.005)
LAM 2001 INDUCTION R IDA 8mg/m 2 x5 DNR 60mg/m 2 x3 + ARA-C 200mg/m 2 D 15 < 5% blasts > 5% blasts IDA or DNR x 2 + ARA-C 1g/m 2
LAM 2001 POST REMISSION THERAPY No HLA id sibling R2R2 Mini conso SC collection 1 ASCT Bu-Mel 2 ASCT Mel 200 Bu-Mel ICC ARA-C 3j x 8 IDA or DNR x 2
LAM 2001 POST REMISSION THERAPY HLA id sibling Good risk< WBC/L favorable cytogenetics No Allo CR in one course All others standard Allo < 50 yo ICC and Miniallo > 50 yo
ALLO versus AUTO RELAPSE RATEALLOAUTO Lowenberg (90) Ferrant (91) Mitus (95) Reiffers (96) Sierra (96) 34 (23) 25 (20) 20 (31) 24 (36) 23 (47) 60 (32) 48 (33) 50 (52) 56 (60)* 37 (68) * Auto transplantation or intensive chemotherapy
ALLO versus AUTO LEUKEMIA FREE SURVIVAL ALLOAUTO Lowenberg (90) Ferrant (91) Mitus (95) Reiffers (96) Sierra (96) 51 (23) 71 (20) 56 (31) 66 (36) 31 (47) 35 (32) 31 (33) 45 (52) 42 (60)* 50 (68) * Auto transplantation or intensive chemotherapy
SURVIVAL ACCORDING TO CYTOGENETIC STATUS AND POST REMISSION THERAPY CytogeneticSubgroupAlloAutoChemoDonorNodonorAlloAutoChemo FavorableIntermediateUnfavorable 62 (50) 65 (148) 13 (13) 78 (50) 56 (131) 46 (18) 76 (242) 48 (626) 25 (69) 61 (129) 66 (100) 28 (46) 56 (155) 38 (130) 22 (69) 63 (19) 52 (37) 44 (18) 71 (26) 36 (37) 13 (20) 35 (22) 55 (44) 15 (20) MRC* EORTC** SWOG/ECOG*** Number of patients is shown in parentheses * at 3 years ** at 6 years *** at 5 years
PROGNOSTIC IMPACT OF KARYOTYPE PtsFavorableIntermediateunfavorable MRCEBMTSWOG/ECOG t(8;21)t(15;17)inv(16)t(8;21) Abnormaliti es of 16 t(8;21) All others Including 11q23 Abnormalitiest(15;17) Pseudidiploid hyperdiploid or diploid Normal +8, -y, +6, del (12p) Complex -5, (del 5q) -7 abnormalities of 3q Abnormalities of 5 and/or 7 Abnormalities of 11q hypodiploid -5, del (5q) -7, del (7a) Inv 39 Complex abnormalities of 11q, 20q, 21q Del (9q) t(6;9), t(9;22) Abn 17p
GOELAM 2 INDUCTION TREATMENT R1 Quinine 30mg/kg CI Control INDUCTION IDR 8x5 ARA-C 200x7 D2O EVALUATION >20% blasts MTZ 12x2 ARA-C 6gx4
Impact of additional cytogenetic abnormalities: Survival of patients entered into AML 10 & 12 (n=3453) Years from entry % still alive Favourable only (n=478) Favourable + intermediate (n=331) Favourable + adverse (n=22) Intermediate only (n=2235) Adverse + intermediate (n=297) Adverse only (n=478) 71% 65% 59% 42% 17% 14%
Outcome of those with done and no transplant Donor – Allo (195) Donor – No allo (110)
DONOR vs NO DONOR ROLE OF CYTOGENETICS Donor No donor Donor Donor NoRelapseDFSSV Good risk Standard risk Poor risk MRC 10 (A. Burnett) donor vs no donor
ALLO vs AUTO INFLUENCE OF CYTOGENETICS EORTC-GIMEMA (AML10) Suciu Blood yr DFS Intent to treat analysis Donor No donor P value Good risk Interm Bad risk Unknown (50) 62% (61) 45% (64) 43% (118) 58% (73) 66% (104) 48.5% (94) 18% (170) 41%
GOELAM 2 CONSOLIDATION < 45 yo HLA identical sibling Allo BMT yo or no identical sibling ICC1ICC2 ARA-C 6gx4Amsa 150x5 MTZ 12x2VP16 100x5 + QUININE
Peripheral blood vs bone marrow allogeneic transplantation Results of randomized studies Author N° pts BloodMarrowBloodMarrowBloodMarrowBloodMarrow SchmitzVigoritoPowlesBlaiseHeldalBensinger %27%NS44%6%64%48%19%NS42%3%57%NA71%NS50%15%46%NA53%NS28%8%35%NSNS 2y sv 70% vs 63% NSNS *2y DFS 65% vs 45% P=0.03 Duration of Duration of a GVHD c GVHD Outcome neutropenia thrombocytopen grade 2-4 (days) No significant difference for early stage malignancies NS = not significant NA = not available
Survival in the United Kingdom Medical Research Council AML trials 1970–1999 for patients aged 15–59 years
THE ROLE OF TRANSPLANTATION IN AML Jean-Luc HAROUSSEAU Nantes - FRANCE
TRAITEMENT DINDUCTION NS NS
GOELAM2 TRIAL PROGNOSTIC FACTORS CR achievement (multivariate analysis) - karyotype (0.0004) - WBC count (0.002) - PS (0.002) DFS (multivariate analysis) - karyotype (0.0004) - allo BMT (0.005)