Télécharger la présentation
1
ARA2 et antagoniste calcique : Une pharmacologie séduisante
Pr M-D DRICI Pharmacologie-Toxicologie Université de Nice-Sophia Antipolis Boards :Boehringer Ingelheim, Novartis Daichii-Sankyo, Lündbeck, Méda-Pharma CNCF Paris le 9 octobre 2009

2
European Society of Hypertension European Society of Cardiology
2007 Guidelines for the Management of Arterial Hypertension BP < 140/90 mmHg European Society of Hypertension European Society of Cardiology Journal of Hypertension 2007;25:

3
Monotherapy versus Combination
Monotherapy : a limited number of patients More than one agent to achieve target BP Numerous effective and well tolerated combinations are available ESH 2007 Journal of Hypertension 2007;25:

4
ESH 2007 Journal of Hypertension 2007;25:1105-1187
high risk hypertensives : BP control achieved promptly, which favours initial combination therapy A combination of two drugs should be preferred as first step treatment :grade 2 or 3 range or total cardiovascular risk high or very high Fixed combination of two drugs can simplify treatment schedule and favour compliance ESH 2007 Journal of Hypertension 2007;25:

5
Tolérance dose-dépendante d’une monothérapie
Max. Efficacité Sécurité Dose Min. D1 D D3 D’1

6
complémentarité additive simple Diurétique thiazidique
Depuis 2007 : > 100 complémentarité additive simple Inh. Syst. RAA B-bloquant ARA II IEC Diurétique thiazidique Inhibiteur calcique

7
Observance du traitement antihypertenseur
initial après un an ( patients) Observants % 61 50 43 38 – Inhibiteur SRAA ICa Diurétiques Adapted from Bloom, Clin. Ther
 Observants % – Inhibiteur. SRAA. ICa. Diurétiques. Adapted from Bloom, Clin. Ther")
8
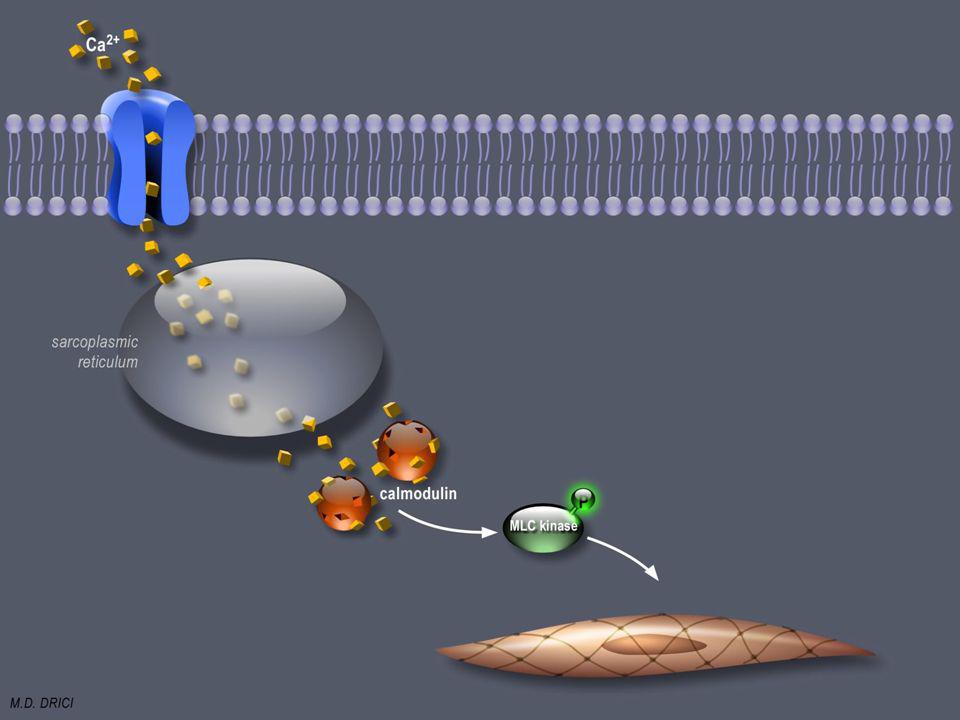
Rôle primordial du calcium dans la contraction des FML
Choix de l’amlodipine ASCOT-BPLA ACCOMPLISH Jamerson K et al. NEJM 2008

9
Complexe Ca++- Calmoduline
Le calcium se fixe à la Calmoduline Calmoduline Complexe Ca++- Calmoduline

12
Amlodipine Mode d’action
Espace extracellulaire Ca++ Membrane d’une cellule musculaire lisse d’un vaisseau Canal calcique Espace intracellulaire

13
Associations fixes antagonistes du SRAA et des canaux calciques
IEC et diurétique ARA2 et diurétique ß-bloquant et diurétique IEC et ICA Association fixe d’un ARAII et d’un ICA There is evidence that multiple-mechanism agents are a highly effective and well-tolerated therapeutic strategy for managing patients with hypertension. Numerous agents offering a dual mode of action are already available for the treatment of hypertension, such as agents combining renin angiotensin system (RAS) blockade with a diuretic (e.g. valsartan plus hydrochlorothiazide [Co-Diovan]) or agents combining angiotensin-converting enzyme (ACE) inhibition with calcium channel blockade (e.g. benazepril plus amlodipine [Lotrel]).1 However, a notable absentee from current multiple-mechanism therapies is an agent that provides dual calcium channel and angiotensin receptor blockade, i.e. a CCBARB. As discussed in the following slides, a CCBARB is a logical and highly effective therapeutic strategy for getting patients to BP goal.2 References Chobanian AV, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. JAMA 2003;289:256072. Andreadis EA, et al. High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension. J Hum Hypertens 2005;19:4916.
 blockade with a diuretic (e.g. valsartan plus hydrochlorothiazide [Co-Diovan]) or agents combining angiotensin-converting enzyme (ACE) inhibition with calcium channel blockade (e.g. benazepril plus amlodipine [Lotrel]).1. However, a notable absentee from current multiple-mechanism therapies is an agent that provides dual calcium channel and angiotensin receptor blockade, i.e. a CCBARB. As discussed in the following slides, a CCBARB is a logical and highly effective therapeutic strategy for getting patients to BP goal.2. References. Chobanian AV, et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. JAMA 2003;289:256072. Andreadis EA, et al. High-dose monotherapy vs low-dose combination therapy of calcium channel blockers and angiotensin receptor blockers in mild to moderate hypertension. J Hum Hypertens 2005;19:4916.")
14
Pourquoi un ARA2 plutôt qu’un IEC ?
Meilleure tolérance du traitement Échappement aux IEC Double complémentarité antihypertensive Garant d’une meilleure vasodilatation?

15
Pourquoi un ARA2 plutôt qu’un IEC ?
Meilleure tolérance du traitement Échappement aux IEC Double complémentarité antihypertensive

16
Poursuite du traitement : les ARA2 sont mieux tolérés
Observants % 64 58 50 43 38 – ARA 2 IEC ICa Diurétiques Adapted from Bloom, Clin. Ther

17
Pourquoi un ARA2 plutôt qu’un IEC ?
Meilleure tolérance du traitement Échappement aux IEC Double complémentarité antihypertensive

18
Comparaison pharmacologique IEC-ARA2
Angiotensinogène Rénine Bradykinine Enzyme de Conversion Angio I IEC IEC Enzymes non spécifiques Produits de dégradation Angio II ARA2 AT1 AT 2 Vasodilatation Vasoconstriction Secrétion d’Aldostérone Libération catécholamines Proliferation FML

19
Plasma ACE (nmol/mL/min) Plasma angio II (pg/mL)
Echappement de l’Angio II lors de l’inhibition au long cours de l’enzyme de conversion 25 50 75 100 Plasma ACE (nmol/mL/min) * 10 20 30 Plasma angio II (pg/mL) Slide 15 Angiotensin-converting enzyme (ACE) inhibition may not completely block the renin-angiotensin-aldosterone system. As shown above, angiotensin II levels are initially suppressed by ACE inhibitor treatment, but soon rise back to pre-treatment levels, despite continued suppression of plasma ACE activity and despite continued antihypertensive activity [Biollaz et al, 1982].The most likely explanation is that angiotensin II can be generated by alternate pathways. Angiotensinogen can be converted to angiotensin II by non-renin enzymes, such as t-PA, cathepsin G, elastase, and chymostatin, and angiotensin I can be converted to angiotensin II by non-ACE enzymes, such as chymostatin-sensitive angiotensin II-generating enzyme (CAGE), chymase, and cathepsin G [Ellis et al, 1996].Angiotensin II receptor blockers block the binding of angiotensin II to the AT, AT, receptor independent of the pathway of angiotensin II production [Ellis et al, 1996]. * Pbo 4 hr 24 hr 1 2 3 4 5 6 Mois *P<0.001 vs. placebo. Biollaz J et al. J Cardiovasc Pharmacol. 1982;4:
 * Plasma angio II (pg/mL) Slide 15. Angiotensin-converting enzyme (ACE) inhibition may not completely block the renin-angiotensin-aldosterone system. As shown above, angiotensin II levels are initially suppressed by ACE inhibitor treatment, but soon rise back to pre-treatment levels, despite continued suppression of plasma ACE activity and despite continued antihypertensive activity [Biollaz et al, 1982].The most likely explanation is that angiotensin II can be generated by alternate pathways. Angiotensinogen can be converted to angiotensin II by non-renin enzymes, such as t-PA, cathepsin G, elastase, and chymostatin, and angiotensin I can be converted to angiotensin II by non-ACE enzymes, such as chymostatin-sensitive angiotensin II-generating enzyme (CAGE), chymase, and cathepsin G [Ellis et al, 1996].Angiotensin II receptor blockers block the binding of angiotensin II to the AT, AT, receptor independent of the pathway of angiotensin II production [Ellis et al, 1996]. * Pbo. 4 hr. 24 hr Mois. *P<0.001 vs. placebo. Biollaz J et al. J Cardiovasc Pharmacol. 1982;4:")
20
Inhibition directe et spécifique des récepteurs AT1
Angiotensinogène rénine Enzyme de Conversion Angiotensine I Enzymes non spécifiques Angiotensine II Olmesartan AT Réc. Type 1 Type 2

21
Grande affinité pour le récepteur de type AT1
8 92 16 12 10 20 30 40 50 60 70 80 90 100 Olmesartan Losartan EXP3174 Candesartan IC (nM) Slide 24 Olmesartan medoxomil has a favourable pharmacokinetic profile [Schwocho et al, 2001; Laeis et al, 2001]. After oral administration, olmesartan medoxomil is rapidly and completely hydrolysed to its active metabolite, olmesartan, by de-esterification in the intestinal wall. Only the active metabolite is detected in plasma. Bioavailability is approximately 25.6%, with little variation for predictable pharmacokinetics.Olmesartan is extensively bound to serum albumin (>99%)After the conversion of olmesartan medoxomil to olmesartan, olmesartan is not metabolised further. Olmesartan is the only compound detected in urine and faeces. Administration of olmesartan medoxomil for 10 days did not result in drug accumulation. Cmax is achieved in approximately 2 hours. t1/2 is between hours. 60% of the absorbed dose is excreted in the faeces, through biliary excretion. Olmesartan is not metabolized by the hepatic cytochrome P450 enzyme system; therefore, the risk of drug interactions is reduced. Administered with or without food. t½ ~10 – 15 h, linéarité parfaite de la cinétique Schwocho LR et al. J Clin Pharmacol. 2001;41: Laeis P et al. J Hypertens. 2001;19(suppl 1):S21-S32. SmPC UK May 2003
 Slide 24. Olmesartan medoxomil has a favourable pharmacokinetic profile [Schwocho et al, 2001; Laeis et al, 2001]. After oral administration, olmesartan medoxomil is rapidly and completely hydrolysed to its active metabolite, olmesartan, by de-esterification in the intestinal wall. Only the active metabolite is detected in plasma. Bioavailability is approximately 25.6%, with little variation for predictable pharmacokinetics.Olmesartan is extensively bound to serum albumin (>99%)After the conversion of olmesartan medoxomil to olmesartan, olmesartan is not metabolised further. Olmesartan is the only compound detected in urine and faeces. Administration of olmesartan medoxomil for 10 days did not result in drug accumulation. Cmax is achieved in approximately 2 hours. t1/2 is between hours. 60% of the absorbed dose is excreted in the faeces, through biliary excretion. Olmesartan is not metabolized by the hepatic cytochrome P450 enzyme system; therefore, the risk of drug interactions is reduced. Administered with or without food. t½ ~10 – 15 h, linéarité parfaite de la cinétique. Schwocho LR et al. J Clin Pharmacol. 2001;41: Laeis P et al. J Hypertens. 2001;19(suppl 1):S21-S32. SmPC UK May")
22
Angiotensin I Challenge Results after 2 hours
Pressure response as percentage of the baseline response % 5 mg 20 mg 10 mg 1 20 mg Placebo Olmesartan medoxomil Enalapril Adapted from Brunner and Nussberger. J. Hypertens 2001; 19 (Suppl 1); S15-20
; S")
23
Pourquoi un ARA2 plutôt qu’un IEC en association avec l’amlodipine?
Meilleure tolérance du traitement Échappement aux IEC Double complémentarité antihypertensive

24
Uehata M et al, Nature 1997 Somlyo AP et al . J Physiol 2000

25
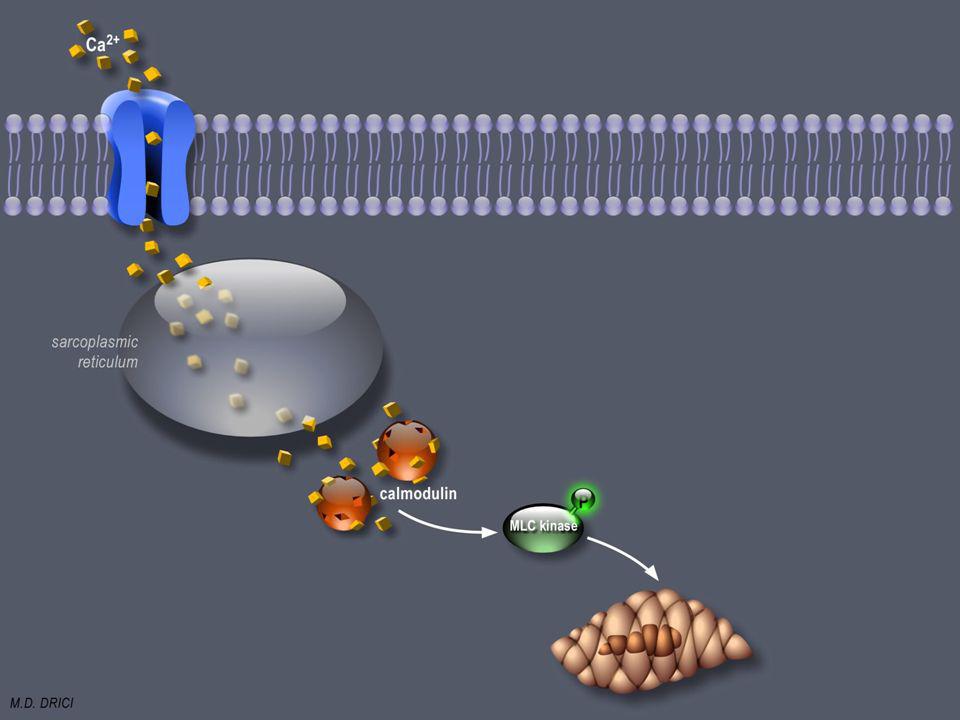
Mécanisme de relaxation des FML
FML contractées

26
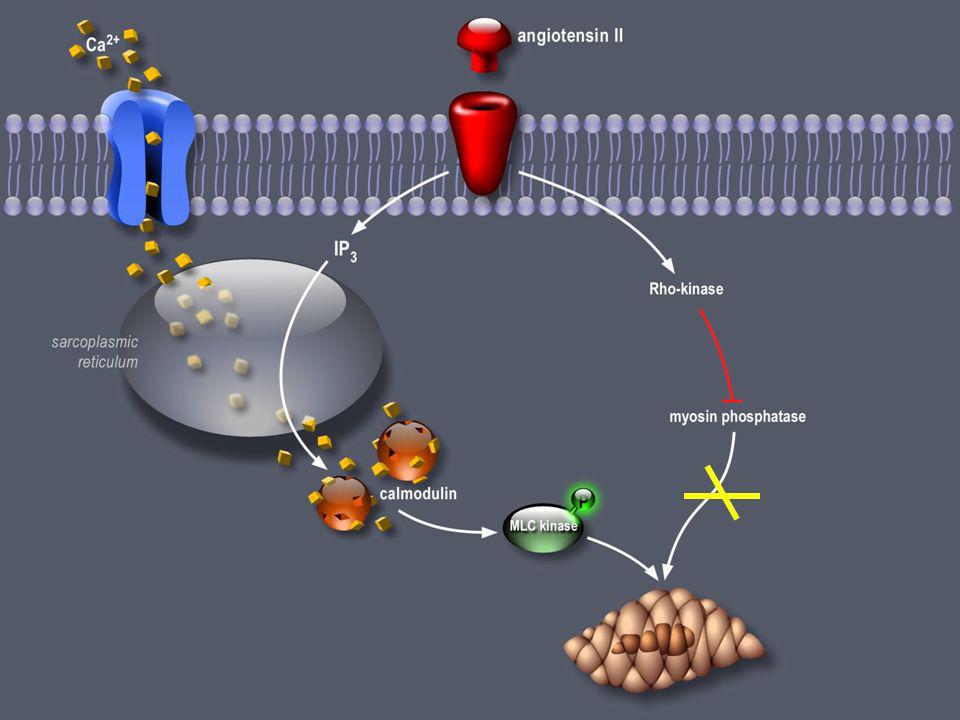
MLC - Phosphatase Activation de la Myosin Light Chain Phosphatase (MLCP)
")
27
Déphosphorylation de la myosine : relaxation
Relaxation de la FML Déphosphorylation de la myosine : relaxation Uehata M et al, Nature 1997 Somlyo AP et al . J Physiol 2000

30
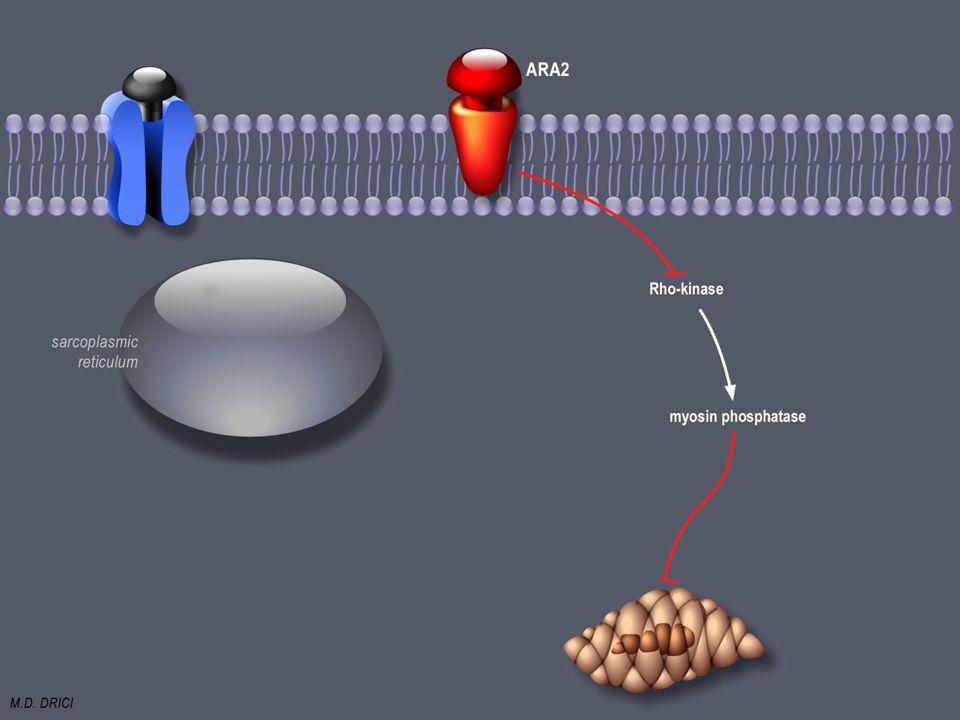
levée de l’inhibition relaxation

31
Amlodipine et ARA 2 : rationnel logique
Antihypertenseurs puissants Efficaces et d’action prolongée double complémentarité antihypertensive Systémique : SRAA et vasculature Cellulaire : fibre musculaire lisse vasculaire Slide 19 Olmesartan medoxomil is a potent and long-lasting angiotensin II receptor antagonist. Olmesartan binds selectively to the AT1 receptor and provides insurmountable inhibition of angiotensin II [Mizuno et al, 1995]. Olmesartan has shown to be a highly potent angiotensin II receptor antagonist that is selective for the AT1 receptor subtype. Olmesartan does not appreciably block the AT2 receptor. In vitro studies using tissues rich in AT1 receptors or AT2 receptors showed that the concentration of Olmesartan needed to inhibit 50% of the angiotension II binding to AT1 (IC50 = nM) was almost 100,000 times less than that needed to inhibit binding to AT2 receptors (IC50 >100,000nM). [Koike et al.2001] AIIA, angiotensin II antagonist. Mizuno M et al. Eur J Pharmacol. 1995;285:
 was almost 100,000 times less than that needed to inhibit binding to AT2 receptors (IC50 >100,000nM). [Koike et al.2001] AIIA, angiotensin II antagonist. Mizuno M et al. Eur J Pharmacol. 1995;285:")
32
MERCI







(4), Jean-Jacques Mourad (2), Jocelyn INAMO(3), Nabila.>")



 A.Compagnucci-A.Faye.>")

>")







