Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Correct treatment Safer sexual behavior promotion Condom promotion Tt completed Cured

2
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Correct treatment Partner treatment Education to recognize symptoms Screening at FP, ANC… Tt completed Cured

3
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Staff behavior Health seeking behavior promotion Correct treatment Tt completed Cured

4
Possible impact of certain interventions
Population with STI Aware and worried Seeking care Correct diagnosis Syndromic approach Include STD drug in essential list Correct treatment Prescribe single dose Counsel for compliance Tt completed Cured

7
Iconographie atlas

8
Iconographie atlas

15
Iconographie atlas

16
Iconographie atlas

17
Iconographie atlas

19
(Czelusta A. J Am Acad Dermatol 2000;43:409-32.)
Fig 5. HIV-positive patient. Chancroid with typical “kissing” ulcers. (Czelusta A. J Am Acad Dermatol 2000;43: )
")
20
Iconographie atlas

24
Chancre mou- une ou plusieurs ulcérations anales, purulentes- adénopathie inguinale inflammatoire évoluant vers la suppuration

25
CHANCRE MOU (chancroid)
Azithromycin 1 g orally in a single dose, OR Ceftriaxone 250 mg intramuscularly (IM) in a single dose, Ciprofloxacin 500 mg orally twice a day for 3 days, Erythromycin base 500 mg orally three times a day for 7 days. (CDC,2006)
 in a single dose, Ciprofloxacin 500 mg orally twice a day for 3 days, Erythromycin base 500 mg orally three times a day for 7 days. (CDC,2006)")
26
CHANCRE MOU (chancroid)
Ciprofloxacin 500 mg orally X 2 j X 3 j, OU Erythromycine base 500 mg p os X 3 x j X 7 j, Azithromycine 1 g p os X 1 Alternative: Ceftriaxone 250 mg intramuscularly (IM) X 1, (OMS, 2004)
 X 1, (OMS, 2004)")
41
Ulcérations herpétiques chez co-infecté VHC/HIV>Fe…Emmanuel

42
Herpes simulant un Chancre ulcéreux, Martinique

43
Ulcérations herpétiques chez co-infecté VHC/HIV>Fe…Emmanuel

44
Herpès atypique chez HIV +: reconstitution Bo….Gérard

45
Herpès atypique chez HIV +: reconstitution Ful Rch

46
Herpès atypique chez HIV +: reconstitution Ful Rch

47
Herpès atypique chez HIV +: reconstitution Ul Brune…

51
First Clinical Episode
HERPES GENITAL First Clinical Episode Acyclovir 400 mg orally three times a day for days, OR Acyclovir 200 mg orally five times a day for days, Famciclovir 250 mg orally three times a day for days, Valacyclovir 1 g orally twice a day for days. (CDC, 2006,WHO, 2004)
")
52
Episodic Therapy for Recurrent Herpes
HERPES GENITAL Episodic Therapy for Recurrent Herpes Acyclovir 400 mg orally three times a day for 5 days*, OR Acyclovir 200 mg orally five times a day for 5 days*, Acyclovir 800 mg orally twice a day for 5 days*, Famciclovir 125 mg orally twice a day for 5 days*, Valacyclovir 500 mg orally twice a day for 3--5 days*, Valacyclovir 1.0 g orally once a day for 5 days*. (CDC, 2006,WHO, 2004) (5-10 days if HIV+, CDC)
 (5-10 days if HIV+, CDC)")
53
Suppressive Therapy for Recurrent Herpes
HERPES GENITAL Suppressive Therapy for Recurrent Herpes Acyclovir 400 mg orally twice a day, OR Famciclovir 250 mg orally twice a day, Valacyclovir 500 mg orally once a day, Valacyclovir 1.0 gram orally once a day. (CDC, 2006,WHO, 2004)
")
54
Suppressive Therapy for Recurrent Herpes if HIV+
HERPES GENITAL Suppressive Therapy for Recurrent Herpes if HIV+ Acyclovir mg orally twice to three times a day, OR Famciclovir 500 mg orally twice a day, Valacyclovir 500 mg orally twice a day. (CDC, 2006)
")
68
Hart G. Clinical Infectious Diseases 1997;25:24–32
Figure 3. Extensive granulomatous lesions of the buccal mucosa in a 30-year-old Australian Aboriginal woman. The affected gums were tender and bled on gentle contact, some teeth were loose, and a radiograph showed erosion of the underlying maxilla. The patient had been treated for genital donovanosis 2 years previously and had residual scarring (but no active lesions) at the primary site. Reprinted with permission from Australian Dental Journal [37]. Hart G. Clinical Infectious Diseases 1997;25:24–32
 at the primary site. Reprinted with permission from Australian Dental Journal [37]. Hart G. Clinical Infectious Diseases 1997;25:24–32.")
69
Hart G. Clinical Infectious Diseases 1997;25:24–32
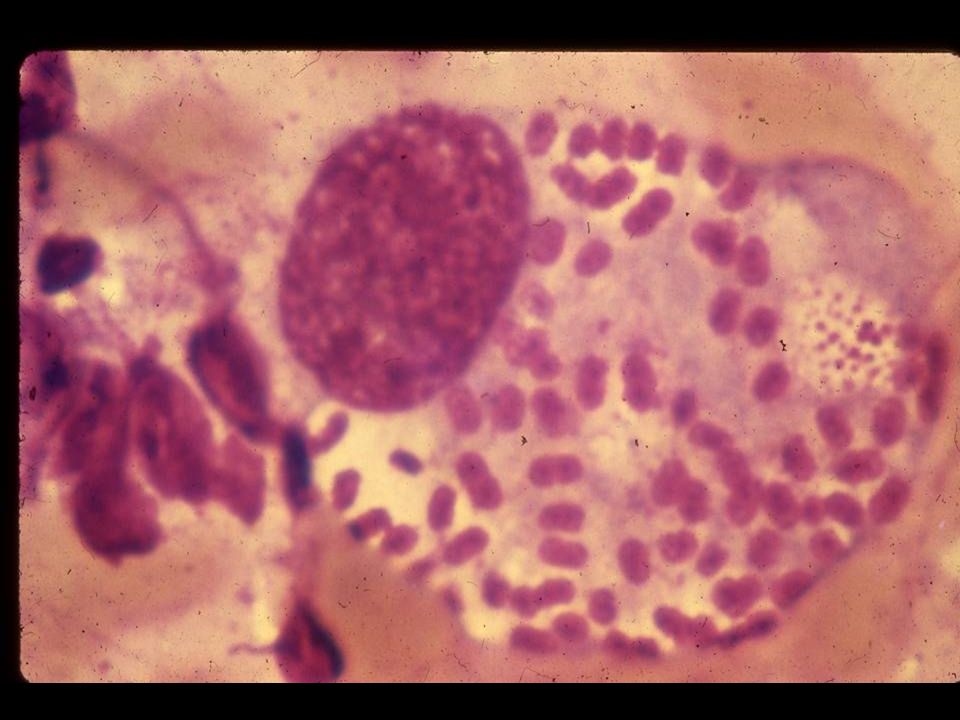
Figure 4. Typical bipolar black-staining Donovan bodies are seen in a mononuclear cell in the center of this slide. Several cells on the periphery show characteristic palisading or clustering of organisms lining the cytoplasmic vacuoles. (Stain, Warthin-Starry silver stain; original magnification, 1400.) Reproduced with permission fromCurrent Medcine [27]. Hart G. Clinical Infectious Diseases 1997;25:24–32
 Reproduced with permission fromCurrent Medcine [27]. Hart G. Clinical Infectious Diseases 1997;25:24–32.")
71
GRANULOMA INGUINALE Co-trimoxazole: 160/800 mg p os x 2 x 14j
(DONOVANOSE) Co-trimoxazole: /800 mg p os x 2 x 14j Alternatives: Doxycycline mg p os x 2 x 14 j Tetracycline 500 mg p os x 4 x 14 j + Streptomycine 1g IM x 1 x 14j (WHO, 1992)
 Co-trimoxazole: 160/800 mg p os x 2 x 14j. Alternatives: Doxycycline 100 mg p os x 2 x 14 j Tetracycline 500 mg p os x 4 x 14 j + Streptomycine 1g IM x 1 x 14j. (WHO, 1992)")
72
GRANULOMA INGUINALE Azithromycine:1g p os x 1/j
(DONOVANOSE) Azithromycine:1g p os x 1/j + 500mg p os x 1/j * Ou Doxycycline: 100 mg p os x 2/j * Alternatives: Erythromycine: 500 mg p os x 4 x/j * Tetracycline 500 mg p os x 4/j x 14 j * Cotrimoxazole 80mg/400 mg x 2 x 2/j x 14 j* (WHO, 2004)
 Azithromycine:1g p os x 1/j mg p os x 1/j * Ou. Doxycycline: 100 mg p os x 2/j * Alternatives: Erythromycine: 500 mg p os x 4 x/j * Tetracycline 500 mg p os x 4/j x 14 j * Cotrimoxazole 80mg/400 mg x 2 x 2/j x 14 j* (WHO, 2004)")
73
GRANULOMA INGUINALE Doxycycline: 100 mg p os x 2/d x ≥3 weeks*
(DONOVANOSE) Doxycycline: 100 mg p os x 2/d x ≥3 weeks* Alternatives: Azithromycine: 1g p os x 1 j ≥3 weeks* OR Ciprofloxacine: 750 mg p os x 2/d x ≥3 weeks* Cotrimoxazole DS (800mg/160mg) p os x2/d x ≥3 weeks* * Up to complete healing (CDC,2006)
 Doxycycline: 100 mg p os x 2/d x ≥3 weeks* Alternatives: Azithromycine: 1g p os x 1 j ≥3 weeks* OR. Ciprofloxacine: 750 mg p os x 2/d x ≥3 weeks* Cotrimoxazole DS (800mg/160mg) p os x2/d x ≥3 weeks* * Up to complete healing. (CDC,2006)")
74
Hart G. Clinical Infectious Diseases 1997;25:24–32

82
Iconographie atlas

84
Fig. 1. Increases in risky behavior and the usage of antiretroviral therapy. (a) Relationship between antiretroviral usage, increases in risky behavior (in both infected and uninfected individuals) and HIV incidence rates after 5 years of antiretroviral usage. HIV incidence rates (where incidence = incidence of drug-susceptible strains plus incidence of drug resistance strains) are plotted, the data points show the area in which the HIV incidence rates are stable. The green, pink and blue data show prevalence one, 5 and 10 years, respectively, after the introduction of antiretroviral treatment Marie Laga, The synergy between Prevention and Care in Africa. IAS, Rio de Janeiro, 2005

87
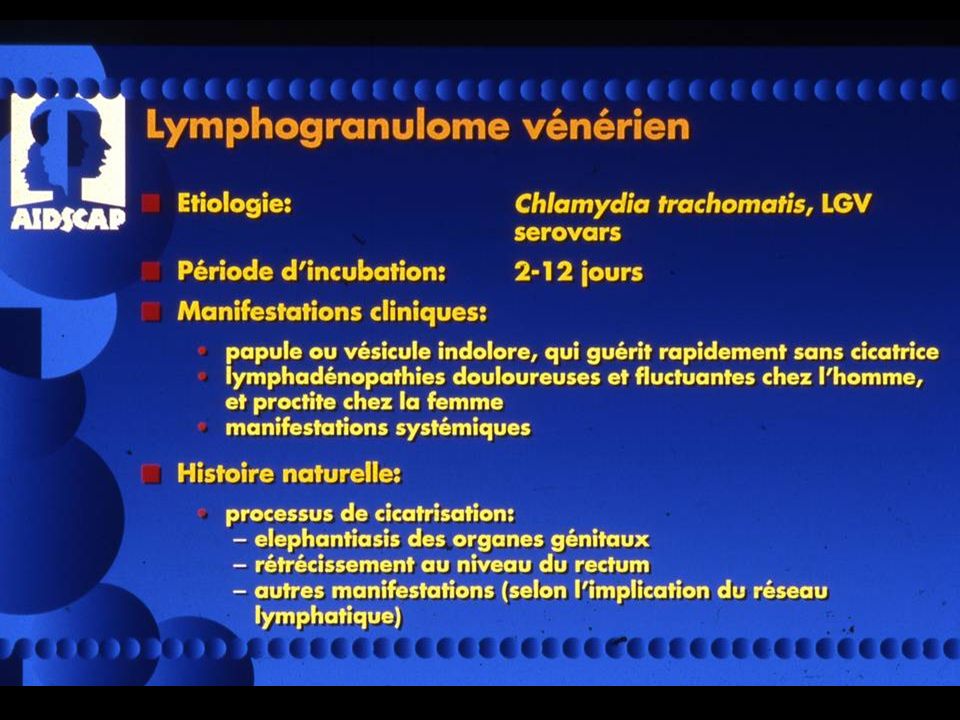
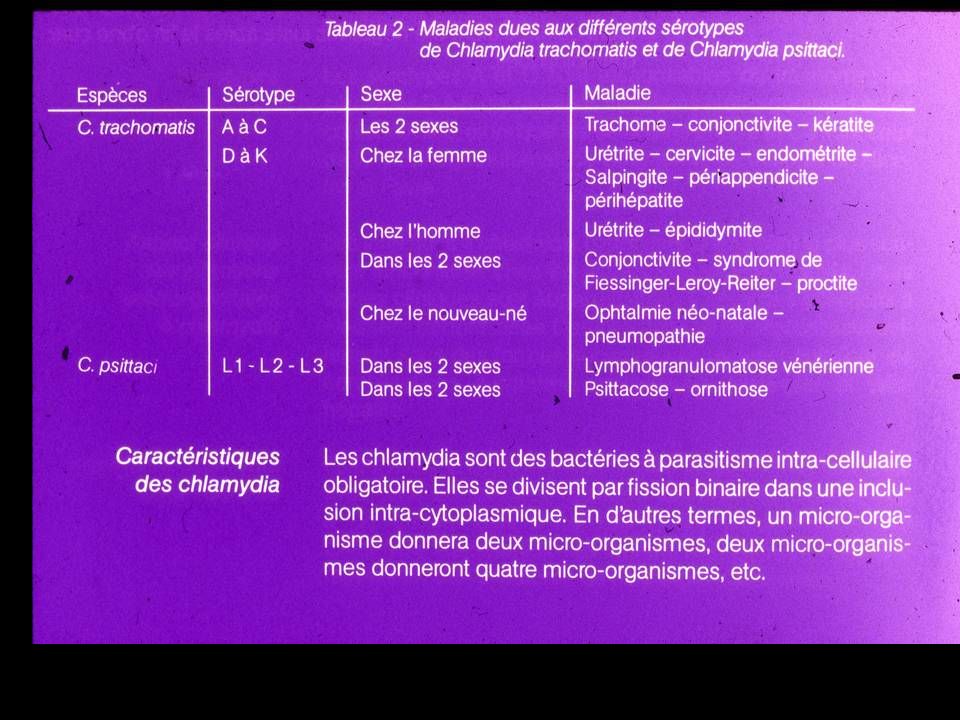
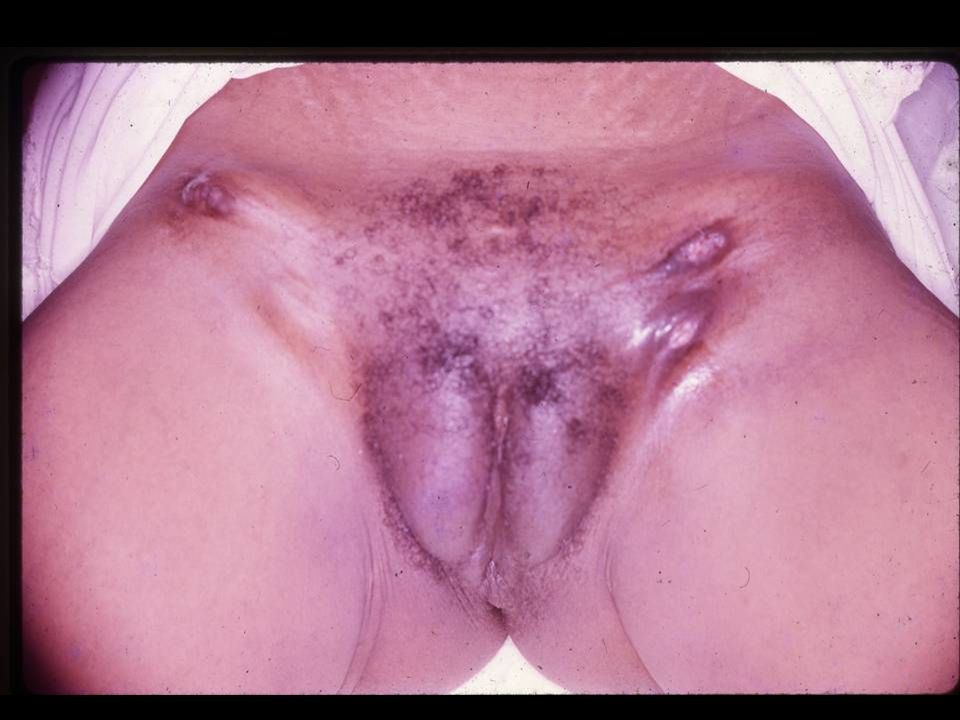
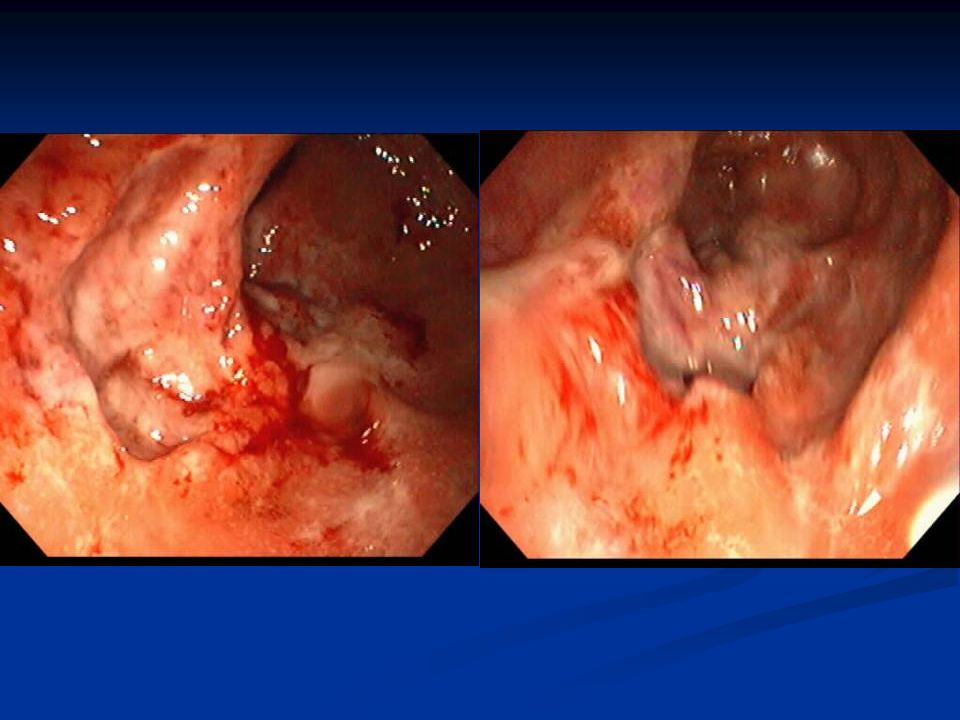
Lymphogranulomatose vénérienne
- fièvre - ténesme - écoulement purulent - adénopathie inguinale le plus souvent unilatérale, unique ou multiple, très inflammatoire avec risque de fistulisation - douleur ano-rectale sévère avec émission sanglante et muco-purulente, ténesme - proctite ou colo-proctite en rapport avec l'évolution de l'inflammation des ganglions lymphatiques péri-rectaux ou périanaux- muqueuse nodulaire et friable, ulcérations diffuses et superficielles

90
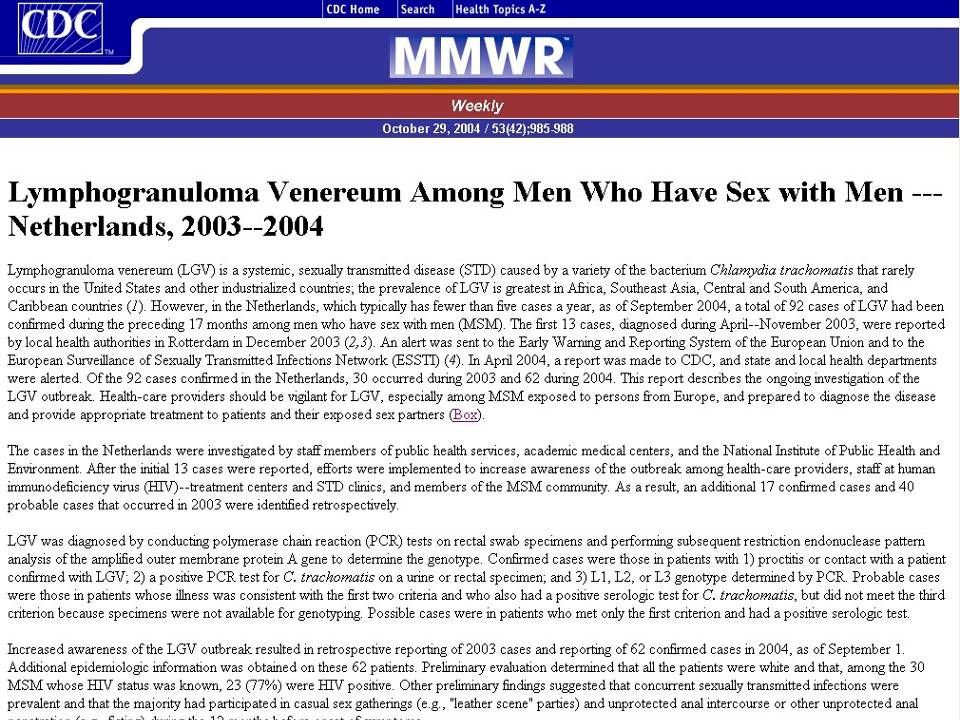
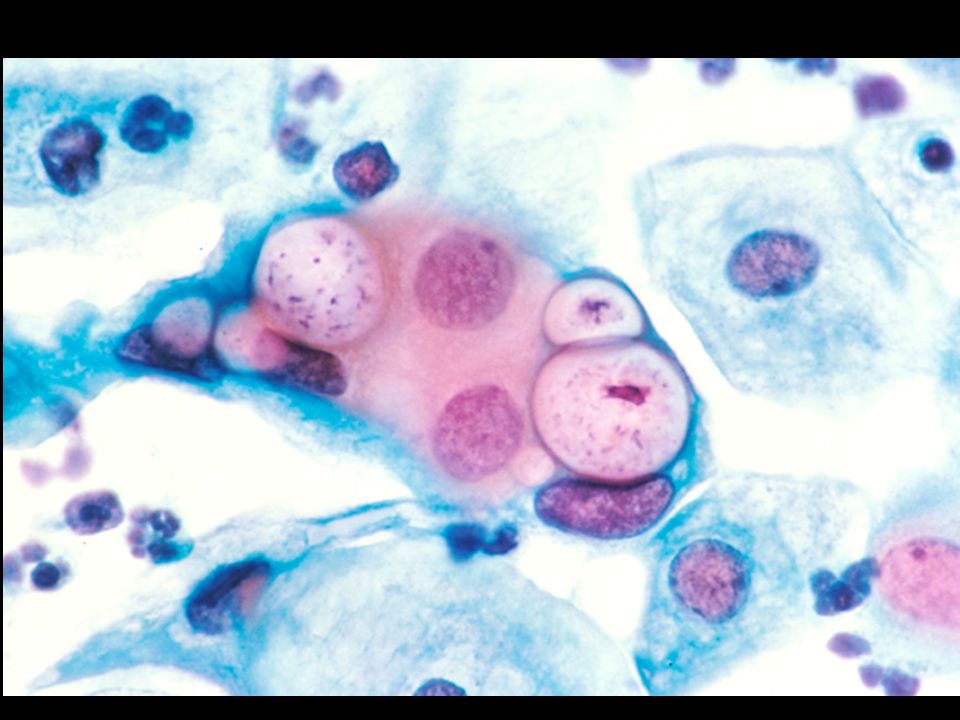
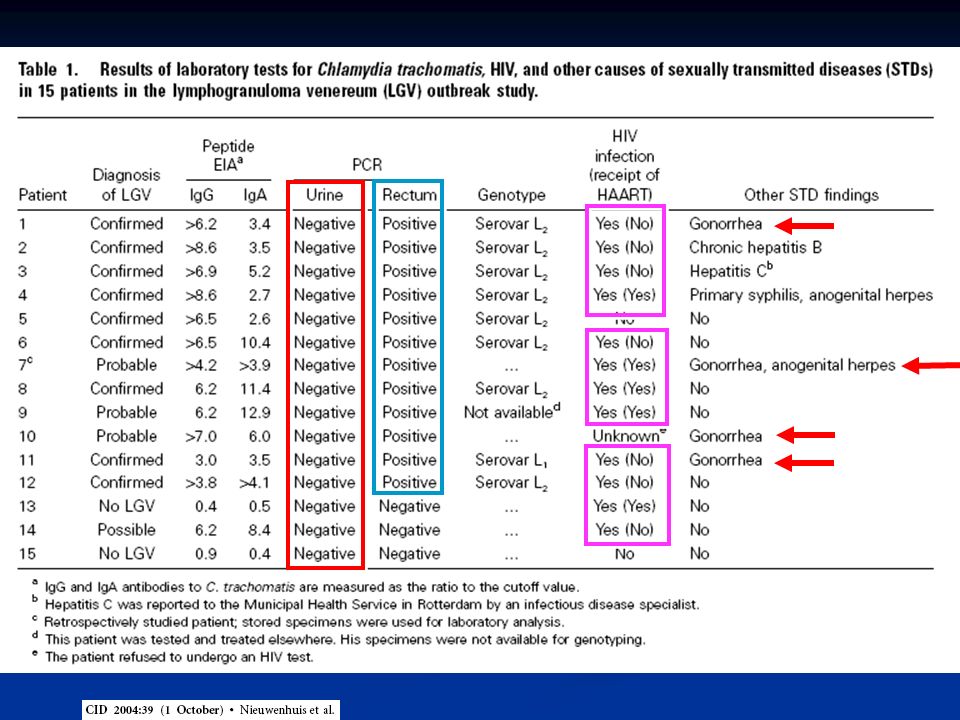
148 patients homo et bisexuels masculins
ayant consulté pour une ano-rectite sur une période de 29 mois (décembre mai 2005) Prélèvement ano-rectal +sérologie Chlamydia par micro-immunofluorescence 1er groupe:(n=26) LGAR (sérotype L2) 2ème groupe: (n=12) Chlamydioses anorectales (sérotype D à K ) 3 ème groupe:(n=110) Anorectites autres origines <256 512 1 1024 2 2048 4096 7 >8192 14 5 2 1 77 7 4 8 Titre des IgG anti-C. trachomatis chez LGAR >2048 chez 88,4% (23/26) Versus 25% (3/12) Chlamydiose anorectales Versus 20% (22/110) Ano-rectites autres origines
 Prélèvement ano-rectal +sérologie Chlamydia par micro-immunofluorescence. 1er groupe:(n=26) LGAR. (sérotype L2) 2ème groupe: (n=12) Chlamydioses anorectales. (sérotype D à K ) 3 ème groupe:(n=110) Anorectites autres origines. < > Titre des IgG anti-C. trachomatis chez LGAR >2048 chez 88,4% (23/26) Versus 25% (3/12) Chlamydiose anorectales. Versus 20% (22/110) Ano-rectites autres origines.")
91
LYMPHOGRANULOMA VENEREUM
(LGV) For 21 days Doxycycline mg p os x 2/d Alternative: Erythromycine 500mg p os x 4/d (CDC,2006)
 For 21 days. Doxycycline 100mg p os x 2/d. Alternative: Erythromycine 500mg p os x 4/d. (CDC,2006)")
92
LYMPHOGRANULOME VENERIEN
(Nicolas et Favre) Pendant 14 jours Doxycycline mg p os x 2 Ou Erythromycine 500mg p os x 4 Alternatives: Tetracycline mg p os x 4 (WHO, 2004)
 Pendant 14 jours. Doxycycline 100mg p os x 2. Ou. Erythromycine 500mg p os x 4. Alternatives: Tetracycline 500mg p os x 4. (WHO, 2004)")
95
Iconographie atlas

Présentations similaires













































>")



>")








 A.Compagnucci-A.Faye.>")




