Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

2
The Complement System Le Systeme du Complement Patricia C. Giclas
Department of Pediatric Allergy and Immunology National Jewish Medical and Research Center, Denver, Colorado, USA Marie-Agnès Dragon-Durey, MD Department of Biological Immunology, European Hospital of Georges Pompidou, Paris, France. Kheir Eddine Kerboua, PharmD, DEMS, Central Laboratory of Clinical Biology, Unit of Immunology Military Hospital of Oran, Algeria. Corresponding:

3
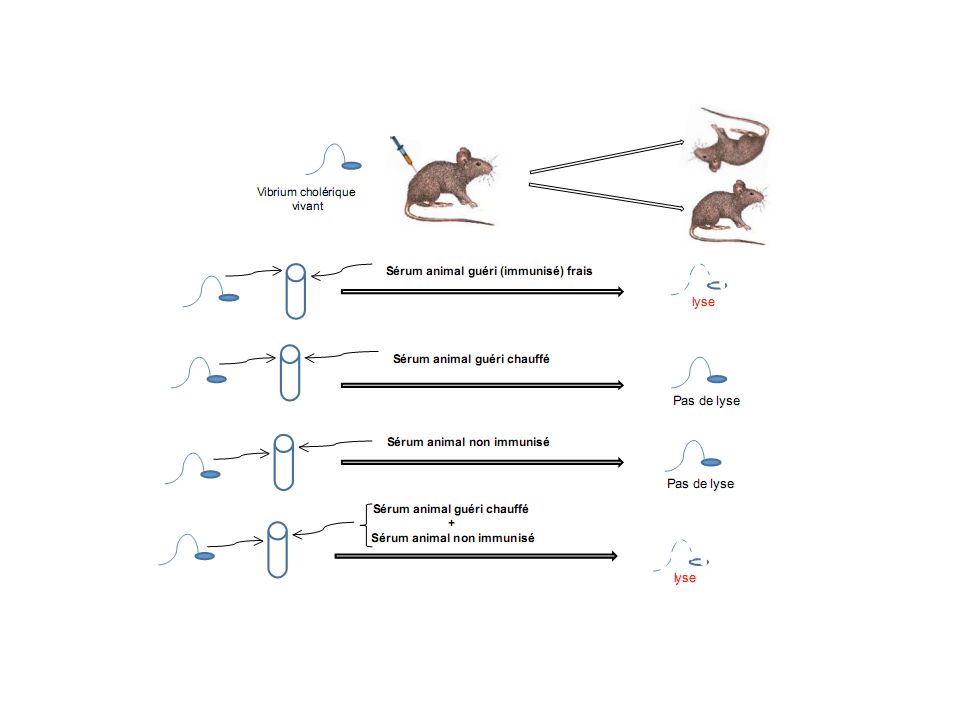
Jules Bordet Pris Nobel 1919

5
INTRODUCTION The innate immune system operates in the absence of the specific adaptive immune system but is tied to adaptive immunity in many ways. The innate immune system is characterized by a rapid response to an invading pathogen or foreign or effete cells. rapid nonspecific and usually of a short duration. lacks immunological memory and there is no clonal expansion of lymphocytes as seen in the adaptive immune response. The innate immune response is also important in directing the specific, long-lived adaptive immune response. The host defense mechanisms associated with innate immunity consist of a num- ber of physical barriers (intact skin), secretions accompanied by a number of serum factors such as complement, certain cytokines, and natural immunoglobulins The cellular components of innate immunity include a number of cell types: natural killer (NK) cells, polymorphonuclear neutrophils (PMNs), macrophages, and dendritic cells (DCs).
, secretions accompanied by a number of serum factors such as complement, certain cytokines, and natural immunoglobulins. The cellular components of innate immunity include a number of cell types: natural killer (NK) cells, polymorphonuclear neutrophils (PMNs), macrophages, and dendritic cells (DCs).")
6
The intact skin and mucosal tissues provide considerable protection against invading infectious agents. However, once the agents pass through the skin a number of important events take place. A number of antimicrobial peptides are produced at epithelial cell surfaces. These antimicrobial peptides play an important role in local defense mechanisms, disrupt bacterial cell membranes, and probably play a role in preventing skin infections. This includes activation of the complement cascade that triggers the development of a number of substances to attract phagocytes to the area.

7
The system consists of 30 proteins found in serum or on the surface of certain cells .
Activation of the complement system results in a cascade of biochemical reactions that ultimately ends in lysis and disruption of foreign or effete cells. Without activation, the components of the complement system exist as proenzymes in body fluids. As a by-product of the activation of the cascade, a number of biologically reactive complement fragments are generated. The complement fragments can modulate other parts of the immune system by binding directly to T lymphocytes and bone marrow–derived lymphocytes (B lymphocytes) of the adaptive immune system and also stimulate the synthesis and release of cytokines.
 of the adaptive immune system and also stimulate the synthesis and release of cytokines.")
8
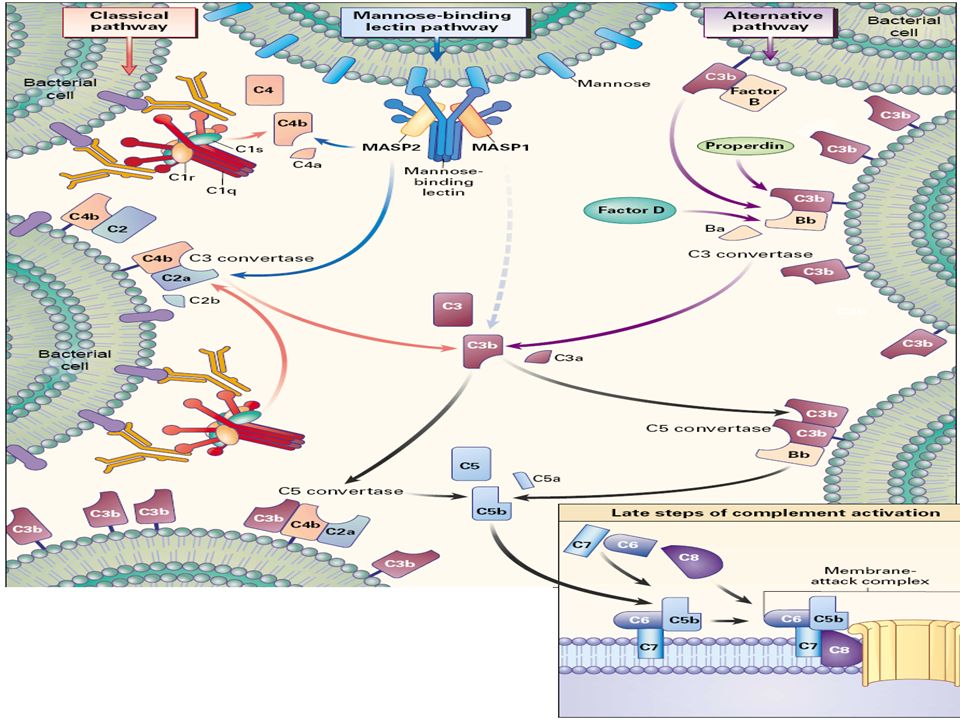
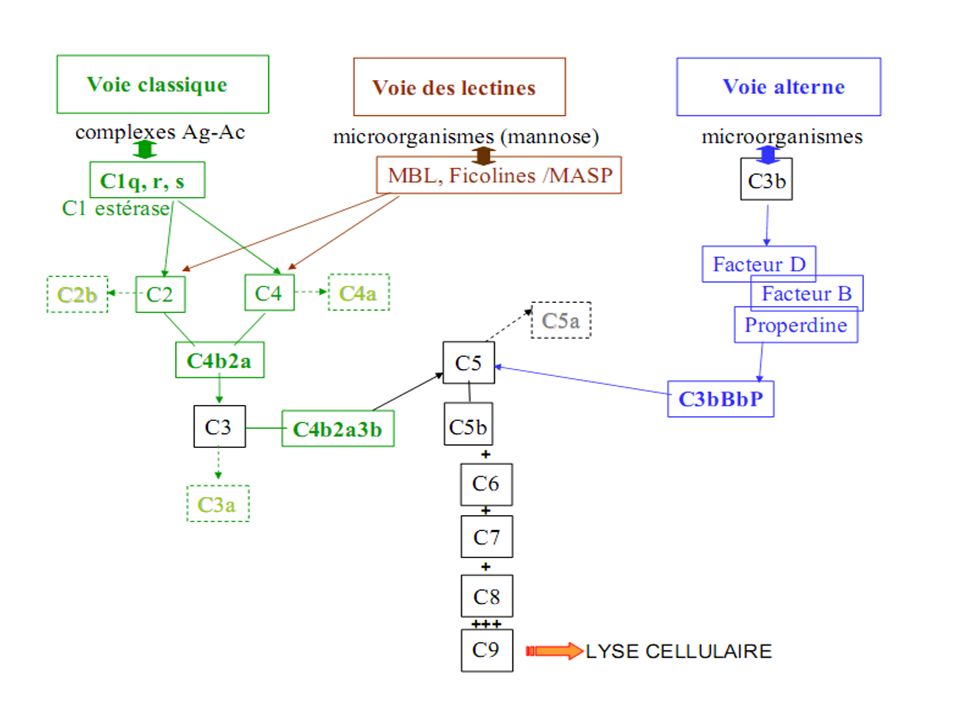
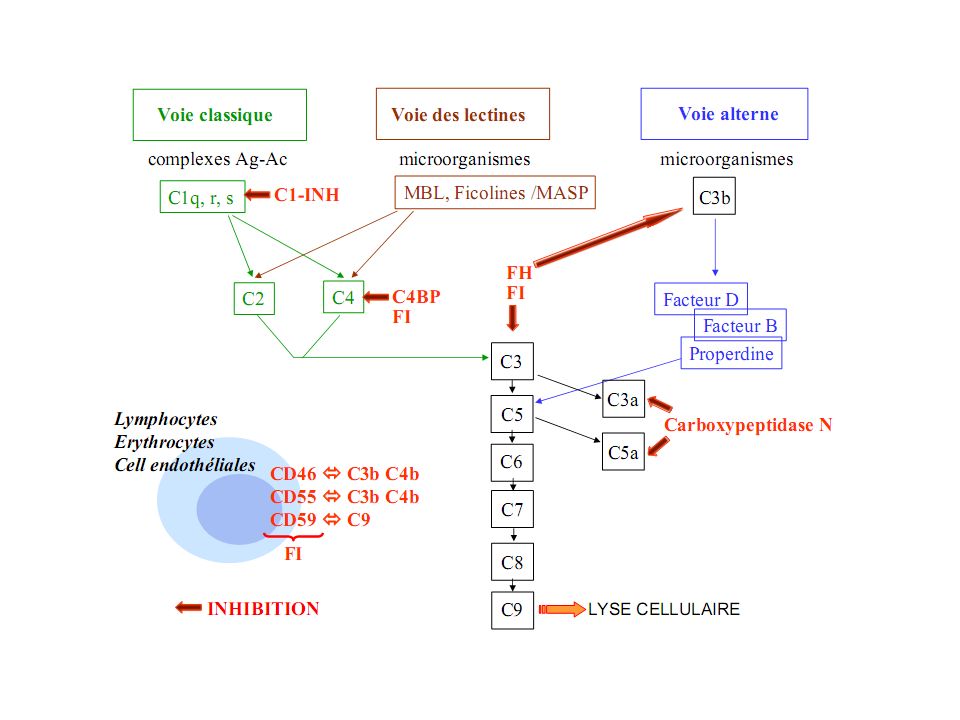
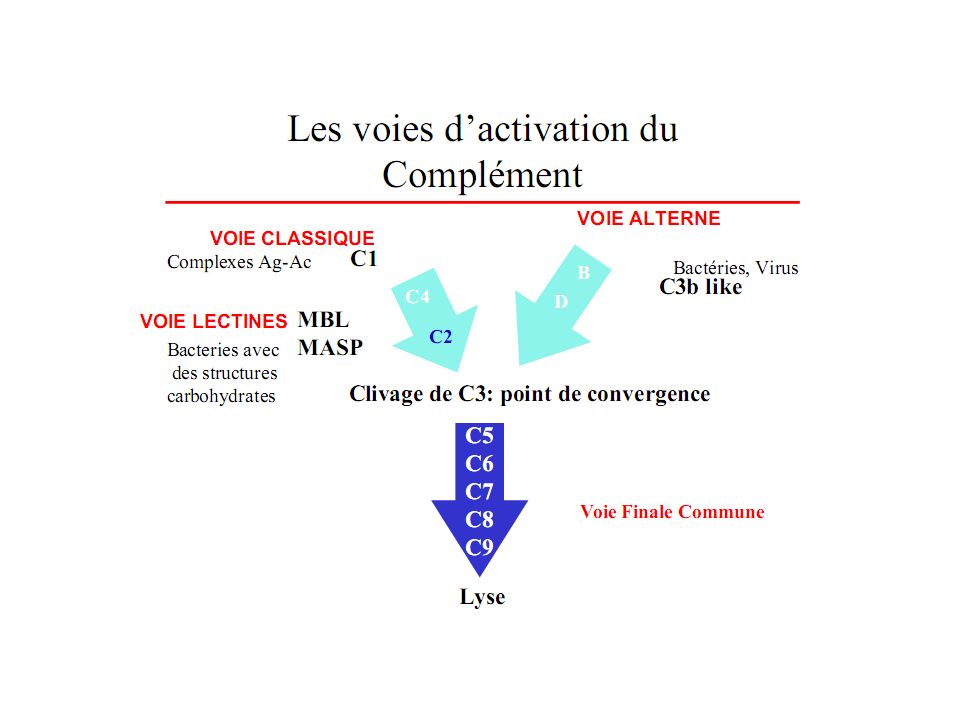
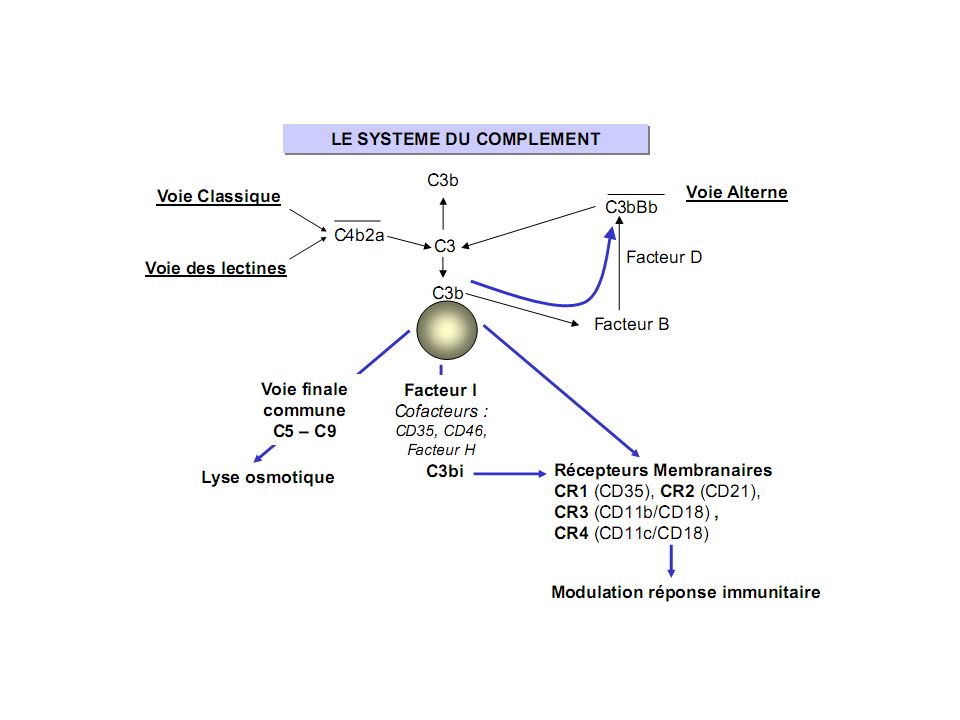
ACTIVATION There are three activation pathways for the complement system. The three pathways are the CLASSICAL, mannan-binding LECTIN (MBL), and the ALTERNATIVE. Each of the pathways has its own recognition mechanism and is activated through different mechanisms, but all result in the formation of a membrane attack complex (MAC) and lysis of a target cell.
, and the ALTERNATIVE. Each of the pathways has its own recognition mechanism and is activated through different mechanisms, but all result in the formation of a membrane attack complex (MAC) and lysis of a target cell.")
10
Although the activation pathways are different, they all act at the microbial surface to assemble an enzyme convertase that cleaves C3 to form C3b that binds to a microbial surface where it activates C5 and the other components of the cascade.

11
The classical pathway Is ACTIVATED by either 1 IgM or 2 IgG attached to a microbial surface antigen. THE RECOGNITION MOLECULE for the classical pathway is complement component C1q. A CONFORMATIONAL CHANGE occurs in C1q, which results in activation of C1r and C1s, which, in turn, ACTIVATES C4 and C2, which leads to the formation of the C4b2a complex (C3 convertase). The C3 COVERTASE acts on C3, which ultimately leads to the formation of the MAC.
. The C3 COVERTASE acts on C3, which ultimately leads to the formation of the MAC.")
12
Activation of the MBL pathway
begins after the recognition of mannose-binding lectin on various carbohydrate ligands. MBLs and Ficolins Are found in serum and are structurally similar to C1q. Bind to mannose-containing carbohydrates on the surface of microbes are considered to be typical pattern recognition molecules and as such attach to the MBL-associated serine proteases. On activation, the MBL-associated serine proteases cleave C4 and C2 to generate the C3 convertase C4bC2a and activate the remainder of the cascade.

13
The alternative pathway
Is important in innate immunity because it does not require specific antibodies for activation of C3. There are low levels of C3 present in body fluids at all times. C3 undergoes HYDROLYSIS to produce C3(H2O), which is an activated form. C3(H2O) can BIND to factor B that is then CLEAVED by the factor D to form the fluid-phase C3 convertase C3(H2O)Bb. Small amounts of C3b are needed to activate the alternative pathway at microbial surfaces. C3b on the microbial surface binds to factor B, which is cleaved by factor D to form C3bBb, the C3 convertase. Properdin serves to STABILIZE the convertase whose role is to CLEAVE C5, which activates the remainder of the cascade. There are several agents that can activate the alternative pathway: bacterial cells, tumor cells, enveloped viruses, and damaged mast cells.
, which is an activated form. C3(H2O) can BIND to factor B that is then CLEAVED by the factor D to form the fluid-phase C3 convertase C3(H2O)Bb. Small amounts of C3b are needed to activate the alternative pathway at microbial surfaces. C3b on the microbial surface binds to factor B, which is cleaved by factor D to form C3bBb, the C3 convertase. Properdin serves to STABILIZE the convertase whose role is to CLEAVE C5, which activates the remainder of the cascade. There are several agents that can activate the alternative pathway: bacterial cells, tumor cells, enveloped viruses, and damaged mast cells.")
14
Amplification Loop This makes the AP more eficient at producing large amounts of C3b that deposit on cell or antigen surfaces. Each new C3 that is cleaved provides another C3b to feed back into the amplification loop or deposit on the surface of the activating particle or other nearby residue.

17
FUNCTION The complement system and its by-products serve to facilitate OPSONIZATION and may ultimately remove or destroy invading microorganisms. Tissue and circulating PMNs and MACROPHAGES are the cells that are most often involved in the ingestion of intracellular pathogens and killing of the invading microbes. Surface-bound C3b and iC3b (on the microbes) facilitate the attachment of the microbes to phagocyte COMPLEMENT RECEPTORS, which activates the ingestion and intracellular killing by the phagocytes.
 facilitate the attachment of the microbes to phagocyte COMPLEMENT RECEPTORS, which activates the ingestion and intracellular killing by the phagocytes.")
18
In addition to enhancing opsonization in the presence or absence of antibodies, complement components have other IMPORTANT BIOLOGICAL FUNCTIONS. For example, free cleavage fragments of C3 and C5 are known to promote host inflammatory responses. C3a and C5a stimulate the bone marrow to release additional PMNs (C3b) and to serve as strong chemoattractants (C3a) for PMNs, monocytes, and eosinophils. Complement components C4a and C5a behave as anaphylotoxins to induce histamine release, which, in turn, causes increased vascular dilatation and permeability. As mentioned earlier, the complement system helps modulate the adaptive immune response by enhancing antigen recognition and by stimulating the synthesis and release of cytokines.
 and to serve as strong chemoattractants (C3a) for PMNs, monocytes, and eosinophils. Complement components C4a and C5a behave as anaphylotoxins to induce histamine release, which, in turn, causes increased vascular dilatation and permeability. As mentioned earlier, the complement system helps modulate the adaptive immune response by enhancing antigen recognition and by stimulating the synthesis and release of cytokines.")
19
CONTROL OF COMPLEMENT ACTIVATION
Because activation of complement is potentially harmful to host cells and disrupts homeostasis, complement activation must be very tightly controlled. Passive control of complement activation occurs because the half-life of the thioester sites on C4b and C3b is very short and limits the distance that the molecules can diffuse away from the activation site before becoming inactive (C4bi, C3bi). the cofactor parts (C4b, C3b) remain bound to the activator surface and can accept another C2 or B to repeat the enzyme formation. Active control occurs through specific complement fluid-phase and cell-bound inhibitors and inactivators whose functions include blocking the initiation of the cascade, preventing formation and stabilization of the C3 and C5 convertases, and preventing the formation of the biologically active split products such as the anaphylatoxins and the MAC.
. the cofactor parts (C4b, C3b) remain bound to the activator surface and can accept another C2 or B to repeat the enzyme formation. Active control. occurs through specific complement fluid-phase and cell-bound inhibitors and inactivators whose functions include blocking the initiation of the cascade, preventing formation and stabilization of the C3 and C5 convertases, and preventing the formation of the biologically active split products such as the anaphylatoxins and the MAC.")
20
CONTROL OF THE CLASSICAL PATHWAY
The net result of all of the controls for the CP is that unless the AP-amplification loop is triggered by the C3b generated in the early stages of CP activation, the reac- tion generally burns out before it reaches the TP, and C3 depletion by this pathway alone is rare.

21
CONTROL OF THE ALTERNATIVE PATHWAY
The AP differs from the other pathways in that it contains both positive and negative regulators.

22
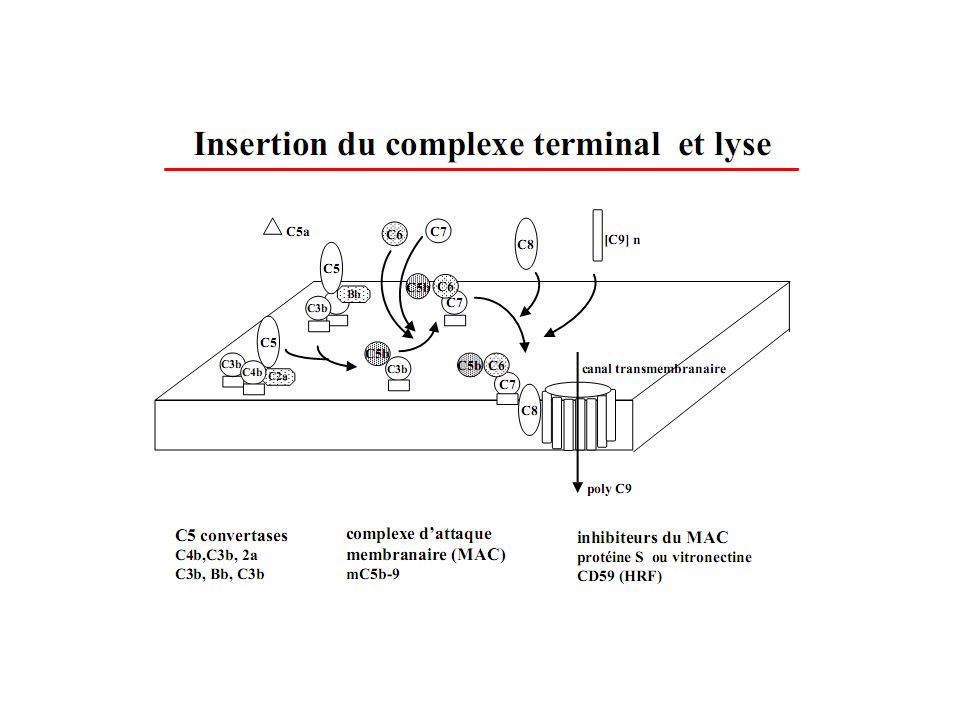
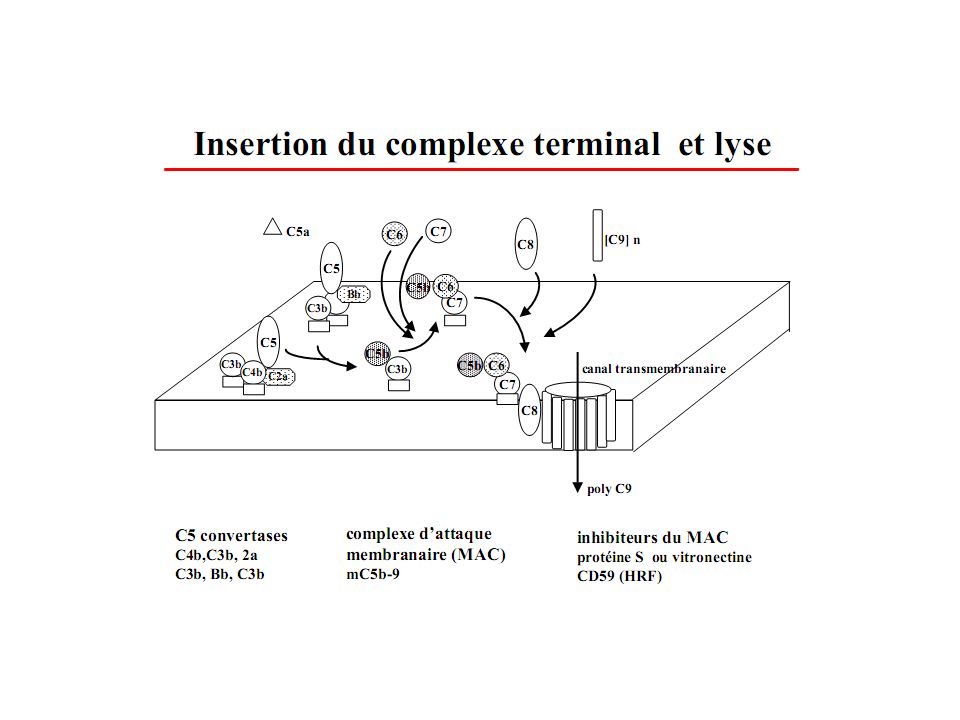
CONTROL OF THE TERMINAL PATHWAY
The C5 convertases are under the same controls as the C3 convertase of the AP The MAC is controlled through two mechanisms Cell surface receptor CD59 binding to C8 Clusterin (SP40,40) and S Protein (vitronectin) can bind to the C5b-7 complexes
 and S Protein (vitronectin) can bind to the C5b-7 complexes.")
24
COMPLEMENT DEFICIENCIES AND THEIR DIAGNOSIS
Deficiencies or mutations in complement components, whether inherited or acquired, predispose the individual to infections, autoimmune diseases, impaired immune responses, and an increasingly long list of diverse conditions including fetal loss, renal disease, vasculitis, angioedema, and macular degeneration. It is important to know as much as possible about the reason(s) for low or absent complement so that decisions regarding appropriate treatment can be made, including when to use antibiotics and immunizations as well as genetic counseling for inherited deficiencies. A family history of members having the same presentation should increase the suspicion about a complement deficiency.
 for low or absent. complement so that decisions regarding appropriate treatment can be made, including when to use antibiotics and immunizations as well as genetic counseling for inherited deficiencies. A family history of members having the same presentation should increase the suspicion about a complement deficiency.")
25
DEFICIENCIES OF CLASSICAL PATHWAY COMPONENTS
C1q, C1r, C1s, C2, C4 are associated with immune complex diseases such as systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA) as well as recurrent infections. C1-Inhibitor low C4 levels (or elevated C4a) and absent or dysfunctional C1-Ihn protein confirms the diagnosis of hereditary angioedema (HAE). DEFICIENCIES OF THE LECTIN PATHWAY L P ativation of complement is antibody -independent so it is thought to play an important role in innate immunity during infancy at the time that maternal antibodies are clearing but before the infant’s immune responses are mature frequency of pyogenic infections and sepsis, particularly in neonates and young children
 and rheumatoid arthritis (RA) as well as recurrent infections. C1-Inhibitor. low C4 levels (or elevated C4a) and absent or dysfunctional C1-Ihn protein confirms the diagnosis of hereditary angioedema (HAE). DEFICIENCIES OF THE LECTIN PATHWAY. L P ativation of complement is antibody -independent so it is thought to play an important role in innate immunity during infancy at the time that maternal antibodies are clearing but before the infant’s immune responses are mature. frequency of pyogenic infections and sepsis, particularly in neonates and young children.")
26
DEFICIENCIES OF THE ALTERNATIVE PATHWAY
Factors D, B, and Properdin P is the only complement protein that is X-linked, increases the susceptibility to bacterial infections including Neisseria. AP Control Proteins Complete deficiency of H leads to uncontrolled activation of AP, and depletion of C3 occurs In addition to pyogenic infections, deficiency or dysfunction of factor H is associated with type II membranoproliferative glomerulonephritis (MPGN-II),atypical hemolytic uremic syndrome (aHUS),and age-related macular degeneration (AMD).
,atypical hemolytic uremic syndrome (aHUS),and age-related macular degeneration (AMD).")
27
DEFICIENCIES OF THE TERMINAL PATHWAY
C3, C4, C5, C6, C7, C8, C9 C3 deficiency is rare and generally associated with recurrent fulminant infections. Deficiency of C3, the major opsonin, results in severe, recurrent pyogenic infections that begin shortly after birth, a clinical presentation and course similar to that observed in hypogammaglobulinemia. Acquired C3 deficiency that occurs with factor H deficiency, factor I defi iency, or in the presence of C3 nephritic factor (C3NeF) predisposes the patient to the same risks as congenital C3 deficiency. Dei ciencies of C3, C5, C6, C7, and C8 are strongly linked with susceptibility to pyogenic infec- tions, particularly with Neisseria. Deficiency of C9 is not strongly linked with infections.
 predisposes the patient to the same risks as congenital C3 deficiency. Dei ciencies of C3, C5, C6, C7, and C8 are strongly linked with susceptibility to pyogenic infec- tions, particularly with Neisseria. Deficiency of C9 is not strongly linked with infections.")
28
LABORATORY EVALUATION OF COMPLEMENT
SPECIMEN PREPARATION AND HANDLING the tube containing the serum should be kept on ice once it has been separated, and transferred to a −70°C freezer or placed on dry ice as quickly as possible. TESTS FOR FUNCTIONAL ACTIVITY Quantitative Tests for Component Concentrations Like most other circulating proteins, complement components can be measured by immunochemical methods common in most laboratories. Tests for Complement Autoantibodies

29
TESTS FOR CLASSICAL PATHWAY FUNCTIONAL ACTIVITY

30
TESTS FOR ALTERNATIVE PATHWAY FUNCTIONAL ACTIVITY

31
Préparation aux Concours d’Acces au Résidanat

32
Cas clinique N°1 : Vous recevez aux urgences Walid, 15 ans: • Examen clinique : – syndrome fébrile – céphalées intenses, vomissements – photophobie. – Raideur méningée • Antécédents personnels : – Une méningite à l’âge de 10 ans non documentée microbiologiquement • Antécédents familiaux : – Origine centrafricaine – Un grand frère décédé d’une infection Quel diagnostic suspectez-vous? Quels examens bactériologiques vous permettront de confirmer ce diagnostic? Vous faites les prélèvements bactériologiques nécessaires et instituez un traitement. L’évolution est rapidement favorable.Deux semaines plus tard vous recevez les résultats du typage de méningocoque : W135 Comment expliquez-vous ce résultat? Quelles sont les conséquences sur votre attitude thérapeutique? Quel bilan devez-vous réaliser?

33
W135 : sérogroupe rare de méningocoque : se trouve de façon endémique ou épidémique dans certaines régions (pèlerinage à la Mecque) • En dehors de ce contexte : suspicion d’une immunodéficience, principalement déficit homozygote en l’une des protéines de la voie finale commune ou en properdine • Indication d’une étude familiale pour proposer une vaccination préventive aux membres de la famille déficitaires homozygotes • Indication d’une vaccination anti-méningocoque comprenant les sérogroupes rares

34
la voie finale commune • Dépistage : Dosage du CH50 : dosage fonctionnel explorant la cascade d’activation impliquant les protéines de la voie classique et de la voie finale commune : détermine la quantité de plasma permettant de lyser 50% de globules rouges de mouton sensibilisés (anticorps de lapin anti-globules de mouton : modèle de surface activatrice) : comparaison avec un pool de plasma normal Ici CH50 = 0% • Identification de la protéine manquante : dosage antigénique (ELISA) +/- fonctionnel • Etude génétique possible DEFICIT EN PROPERDINE 5% DES INDIVIDUS DEFICITAIRES : MENINGITES FULMINANTES A NEISSERIA
 : comparaison avec un pool de plasma normal Ici CH50 = 0% • Identification de la protéine manquante : dosage antigénique (ELISA) +/- fonctionnel. • Etude génétique possible. DEFICIT EN PROPERDINE. 5% DES INDIVIDUS DEFICITAIRES : MENINGITES FULMINANTES A NEISSERIA.")
35
DIAGNOSTIC : – AP50 <10% – Dosages CH50, de C3 et Facteur B normaux – DOSAGE PONDERAL DE P – ETUDE FAMILIALE +++

36
Cas clinique N°2 Vous voyez en consultation Madame R Ahlem, 45 ans, qui vous est adressée par son psychiatre qu’elle consulte pour des douleurs abdominales répétées sans étiologie retrouvée depuis plusieurs mois. Son thérapeute a noté un épisode d’œdème labial et souhaite éliminer toute pathologie organique. Comment orientez-vous votre interrogatoire? L’examen clinique est sans particularité Quel type de bilan biologique demandez-vous? Deux semaines plus tard la patiente vous téléphone pour vous signaler une nouvelle crise. Vous lui demandez de venir immédiatement : la patiente présente un œdème facial important, non inflammatoire

37
Que devez-vous craindre?
Quelle attitude thérapeutique adoptez-vous dans l’urgence? Quel bilan étiologique demandez-vous? Les résultats de l’exploration des protéines du Complément sont : -CH50 : <10 % (70-130) -C3 : 890 mg/L ( ) -C4 : <14 mg/L (93-210) Le médecin Biologiste a effectué les examens complémentaires suivants : -C1-Inh (Ag) : 180 mg/L ( ) -C1-Inh (fonction) : < 30% (70-130) Recherche d’anticorps anti-C1-Inh : Positive, Isotype IgG
 -C3 : 890 mg/L ( ) -C4 : <14 mg/L (93-210) Le médecin Biologiste a effectué les examens complémentaires suivants : -C1-Inh (Ag) : 180 mg/L ( ) -C1-Inh (fonction) : < 30% (70-130) Recherche d’anticorps anti-C1-Inh : Positive, Isotype IgG.")
38
Cas clinique N°3 • Vous voyez en consultation une jeune femme de 25 ans qui se plaint de douleurs articulaires d’horaire inflammatoire • Dans ses antécédents : – Méningite à pneumocoque à l’âge de 5 ans – Photosensibilité cutanée – Une sœur de 40 ans qui a eu une embolie pulmonaire • A l’examen : rash malaire évident, raideur articulaire •Quel diagnostic suspectez-vous? •Quels examens complémentaires prescrivez-vous?

39
Cas clinique N° 4 On vous adresse en consultation ALI l H. âgé de 7 ans pour oedèmes avec protéinurie. Il n’a pas d’ATCD particulier, les parents ont noté des oedèmes des MI le soir depuis une dizaine de jour. Le médecin traitant a détecté une protéinurie à la bandelette et a prescrit des examens complémentaires. Vous notez dans celui-ci : Créatininémie : 150 µmol/L Protéinurie : 1.50 g/24h Hématurie + + Devant l’insuffisance rénale, une PBR est réalisée : Glomérulonéphrite Membrano proliférative avec dépôts de C3

40
Une exploration des protéines du Complément est réalisée :
CH50 : 80% (N : ) C3 : 430 mg/L (N : ) C4 : 210 mg/L (N : ) Le médecin biologiste a effectué des dosages complémentaires : Facteur B : 50 mg/L (N : ) Facteur H : 90% (N : ) Facteur I : 115 % (N : ) C3Nef : Positive Auto-Anticorps anti-C3 convertase alterneC3 nephritic Factor ou C3 Nef •Auto-Anticorps d’isotype IgG (autres sous-classes ?) ayant la capacité de stabiliser la C3 convertase alterne Clivage de C3 Diminution du C3 +/- Facteur B •Détecté dans le plasma de patients atteints de : - GNA avec C3 bas (activité faible et transitoire, surveiller sa disparition) - Glomérulonéphrite Membrano-Proliférative - Syndrome de Barraquer-Simons (lipodystrophie partielle)
 C3 : 430 mg/L (N : ) C4 : 210 mg/L (N : ) Le médecin biologiste a effectué des dosages complémentaires : Facteur B : 50 mg/L (N : ) Facteur H : 90% (N : ) Facteur I : 115 % (N : ) C3Nef : Positive. Auto-Anticorps anti-C3 convertase alterneC3 nephritic Factor ou C3 Nef. •Auto-Anticorps d’isotype IgG (autres sous-classes ) ayant la capacité de stabiliser la C3 convertase alterne. Clivage de C3 Diminution du C3 +/- Facteur B. •Détecté dans le plasma de patients atteints de : - GNA avec C3 bas (activité faible et transitoire, surveiller sa. disparition) - Glomérulonéphrite Membrano-Proliférative. - Syndrome de Barraquer-Simons (lipodystrophie partielle)")
41
Voie Alterne et Pathologies Rénales

48
CONCLUDING REMARKS Pharmaceutical companies are studying complement to discover how activation can be blocked by specific compounds including monoclonal antibodies and new inhibitors. Complement is a powerful tool for the destruction of target cells and, if controlled activation could be accomplished, could be directed against tumors.

Présentations similaires



 - Jean Rauscher>")

















