Frequency of lipid abnormalities in male CHD patients Rubins HB et al. Am J Cardiol 1995;75: Occurrence of abnormalities (%) Elevated total-C Elevated LDL-C Elevated triglycerides Low HDL-C
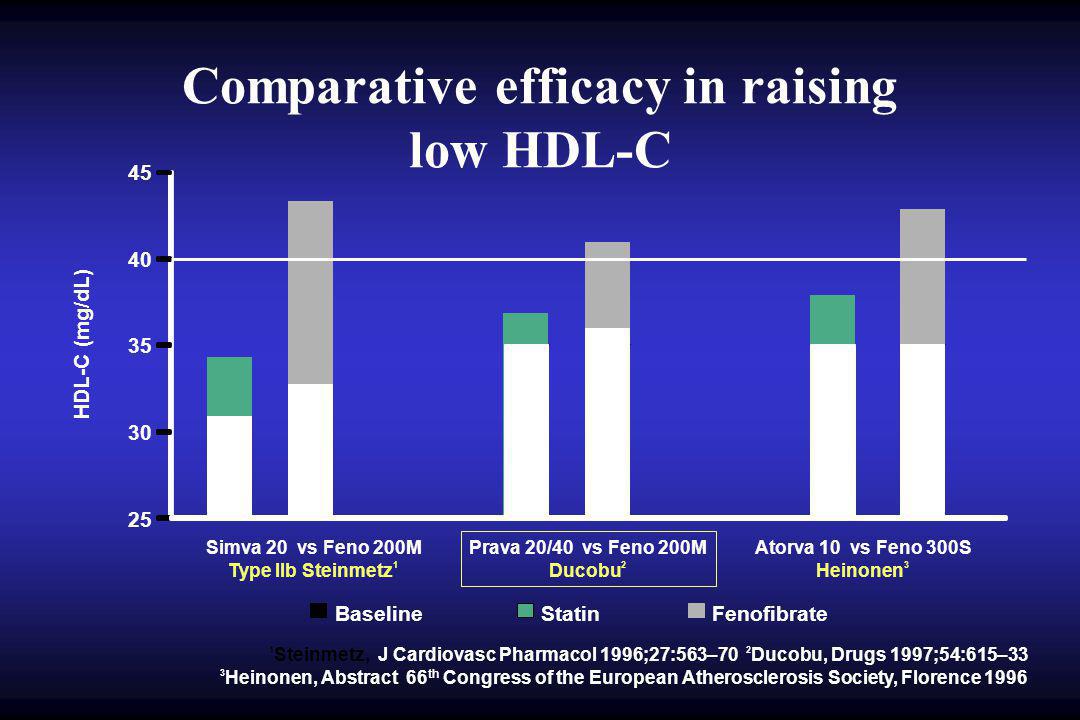
Comparative efficacy in raising low HDL-C HDL-C (mg/dL) Simva 20 vs Feno 200M Type IIb Steinmetz 1 Prava 20/40 vs Feno 200M Ducobu 2 Atorva 10 vs Feno 300S Heinonen BaselineStatinFenofibrate 1 Steinmetz, J Cardiovasc Pharmacol 1996;27:563–70 2 Ducobu, Drugs 1997;54:615–33 3 Heinonen, Abstract 66 th Congress of the European Atherosclerosis Society, Florence 1996
A-I A-I A-II A-II LPL LPL C-III C-III Fibrates PPAR Fibrates: Regulation of lipoprotein metabolism by PPAR metabolism by PPAR HDL particles TG rich particles PPRE PPAR RXR PPRE PPAR RXR PPRE PPAR RXR PPRE PPAR RXR Staels B et al. Circulation 1998;98:2088–93.
ABCA-1 gene expression Apo A-I PPAR activator Activated PPAR Intracellular cholesterol Human macrophages were cholesterol loaded with AcLDL in the presence of PPAR activator and incubated for 24 hours with apo A-I Relative decrease in cellular cholesterol after Apo A-I efflux TCCEFC Cholesterol efflux PPAR activators induce cholesterol efflux from human macrophages
VA-HIT Study: Diabète type 2 & traitement par fibrate (1) (1)Bloomfield Rubins H et al. Arch Intern Med 2002; 162:
Facteurs de risque cardio-vasculaire Sexe Antécédents familiaux Antécédents personnels Lipides et lipoprotéines Hypertension artérielle Diabète Insuffisance rénale chronique Inflammations chroniques Tabagisme Mauvaises habitudes alimentaires Sédentarité et activité physique insuffisante
Lipides plasmatiques Pression artérielle Tendance aux thromboses Résistance à insuline Oxydation Homocystéine Inflammation Fonction endothéliale Irritabilité ventriculaire NUTRITION MCV Nutrition et Pathologies Cardio-vasculaires
Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-Reactive Protein 46 sujets adultes, sains mais hyperlipidémie 25 H; 21 F; 59 1 ans; BMI Intervention : distribution aléatoire A : apports pauvres en graisses sat & riches en céréales ent. B : mêmes apports + Lovastatin 20 mg C : apports riches en phytostérols (1.0 g / 1000 kcal) protéines de soja (21.4 g / 1000 kcal) fibres visqueuses (9.8 g / 1000 kcal) amandes (14 g / 1000 kcal) D.J.A. Jenkins et al, JAMA, 2003
Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-Reactive Protein D.J.A. Jenkins et al, JAMA, 2003
Adherence to a Mediterranean diet and survival in a Greek population Etude prospective sur adultes (20-86 ans) Evaluation des apports alimentaires Classification selon un «score méditerranéen» Suivi sur 44 mois : Adhésion au régime méditerranéen associée à mortalité par maladies cardio-vasculaires et cancer Trichopoulou A et al, N Engl J Med, 2003
Mediterranean Diet, Traditional Risk Factors, and the Rate of Cardiovascular Complications After Myocardial Infarction Final Report of the Lyon Diet Heart Study, de Lorgeril et al, 1999 Survie sans I.M. non mortel Survie sans complication
ALL: 1-week Food Records, Wt, BP & Metabolic Profiles All participants: Step 1 Prudent Diet National Cholesterol Education Program + Regular physical activity + Regular physical activity + Fruits: g per day + Vegetables: g + Nuts: 25-50g walnuts/almonds g/day of whole grains: legumes, rice, maize, wheat servings mustard / soy bean oil Control Group B 501 Intervention A 499 Follow up: weekly, monthly, 3-monthly to 2 years End Points: 1 Myocardial Infarction - fatal /nonfatal 2 Sudden Cardiac Death, 3 Composite total of cardiac events The Indo-Mediterranean diet heart study, R. Singh et al, Lancet, 2002
Change in Risk factors during study: Both groups improved significantly, but more so in Gp A, p<0.001 for all parameters The Indo-Mediterranean diet heart study, R. Singh et al, Lancet, 2002
Numbers & rate ratios for cardiac endpoints, adjusted for age, gender, BMI, cholesterol and BP Group A B B Rate Ratios Non Fatal MI [ ] Fatal MI [ ] Sudden cardiac [ ] death Total Cardiac Endpoints [ ] The Indo-Mediterranean diet heart study, R. Singh et al, Lancet, 2002
Conclusions The Indo-Mediterranean diet heart study, R. Singh et al, Lancet, 2002 The Indo Mediterranean diet is a safe and economical means for improving the health of poorer populationsThe Indo Mediterranean diet is a safe and economical means for improving the health of poorer populations The whole grains, fruits, vegetables and oils used in this study were traditional fare, grown by farmers at the present market cost of about 1 US$ per day Lancet 2002The whole grains, fruits, vegetables and oils used in this study were traditional fare, grown by farmers at the present market cost of about 1 US$ per day Lancet 2002
GISSI-Prevenzione Investigators. Lancet 1999;354: ; Marchioli R et al. Eur Heart J Suppl 2001;3(Suppl D):D85-D97. GISSI-Prevenzione Trial: Design 11,323 patients randomized 4 lost to follow-up 687 discontinued vitamin E 11 received omega-3 PUFAs 3 lost to follow-up 768 discontinued omega-3 PUFAs 4 lost to follow-up 848 discontinued omega-3 PUFAs 808 discontinued vitamin E 2 lost to follow-up 15 received omega-3 PUFAs 2 received vitamin E 2835 given omega-3 PUFAs 2830 given vitamin E 2830 given omega-3 PUFAs & vitamin E 2828 controls 2835 analysed for outcomes 2830 analysed for outcomes 2828 analysed for outcomes
GISSI-Prevenzione Trial: Secondary Endpoint Results ControlOmega-3 Risk P-value PUFAs reduction All-cause mortality 10.6%8.4%21% CV death 7.2%5.1%30%<0.001 Cardiac death 6.1% 4.0%35%<0.001 Coronary death 5.2%3.6%32%<0.01 Sudden death 3.3%1.8%44% Non-fatal CV events 4.9%4.9%2%n.s. Marchioli R et al. Eur Heart J Suppl 2001;3(Suppl D):D85-D97; Marchioli R et al. Circulation 2002;105:
GISSI-Prevenzione Trial: Early Effect of Omega-3 PUFAs on All-Cause Mortality Probability Days (95% CI ) P = Omega-3 PUFAs Control Marchioli R et al. Circulation 2002;105: Calculated adjusting for treatment interaction and major confounding variables
Modifications des recommandations Réduire apports en graisses saturées (animales) Remplacement par graisses mono-insaturées (olive, …) Inclusion et augmentation des acides gras oméga-3 Réduction des sucres simples Remplacement par sucres lents (féculents, pâtes, pain entier, …) Retour aux céréales entières (fibres) notion de mauvaises & bonnes graisses mauvais et bons sucres
Modes de nutrition protecteurs Régime(s) méditerranéen(s) Adaptation possible à goûts/cultures différents graisses saturées sucres simples légumes et/ou fruits (y compris fruits secs) Apports caloriques raisonnables Apports protéiques raisonnables Vin en quantité modérée (sauf si contre-indications) font partie dun mode de vie (« lifestyle »)
Nutrition et Maladies c.v. : les messages Lésions dathéroslérose souvent réversibles Réduction du risque par mode de vie (-50% à –80%) Suppléments alimentaires : NON, sauf si indications: stérols végétaux acides gras oméga-3 acide folique (sélénium)
Modifications du mode de vie Arrêt cigarette Alimentation « santé » sélection aliments / nutriments plaisants & sains activité physique (régulière) risque cardio-vasculaire ( - 80%) Effet additif à celui des médicaments ( lipides, tension artérielle)