Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Jean-François Gautier,
Foetal programming of the cardiovascular risk: Effect of maternal diabetes Jean-François Gautier, Department of Diabetes and Endocrinology, Saint-Louis Hospital, INSERM UMRS 872, team 8, Paris, France 12th meeting of the MGSD, Casablanca, Morocco, 2011

2
What is fœtal programming ?
Definition Alteration of intrauterine environment that predisposes to the development of disorders and diseases later in life First evidences Caloric restriction during pregnancy has been associated with a higher metabolic and cardiovascular risk at adult age (review in Hales Diabetologia 2003)
")
3
Outline Epidemiological evidences of maternal transmission of diabetes Metabolic defects associated with foetal exposure to maternal diabetes Potential mechanisms: what did we learn from animal studies? Multi organ defects as a consequences of maternal diabetes in human offspring Late consequences

4
Diabetes Pathophysiology of type 2 diabetes IGT Genetic Factors
Environmental factors Insulin resistance IGT Cell dysfunction Diabetes

5
Difference between the ratio of diabetic mothers and diabetic fathers within selected populations of diabetic patients (with 95% confidence interval)
")
6
Maternal influence in the development of T2D
Reference Population Ratio mother/father with T2D Alcolado J.C.et al.1992 Mitchell B.D.et al.1993 Thomas F.et al.1994 Lin R.S.et al. 1994 Young C.A.et al.1995 Viswanathan M.et al.1995 McCarthy M.et al.1996 Klein B.E.K.et al.1996 Riley M.D.et al.1996 Karter A.J.et al.1999 Meigs J.B.et al.2000 Bo S.et al.2000 Bjornholt J.V.et al.2000 UK Mexican/Caucasian Americans France Taiwan Europeans/ Caraïbes Indians Wisconsin,USA Tasmania California Framingham Italy Norway 2.1 NS 2.6 2.1/ 1.9 2.0 2.7 1.2 4.0 1.5 Review in Alcolado 2002

7
The Framingham Offspring Study
2527 offspring from 1303 Caucasian families All offspring and parents were formally tested for diabetes The risk of developing diabetes was similar among offspring of diabetic mothers and of diabetic fathers However, offspring of mothers who had diabetes before the age of 50 years had a marked increased risk for developing : Impaired glucose tolerance OR 9.0 ( ) Type 2 diabetes OR 9.7 (4.3-22) → Possible role of foetal environment ? Meigs Diabetes 2000
 Type 2 diabetes OR 9.7 (4.3-22) → Possible role of foetal environment Meigs Diabetes")
8
In Utero Exposure to Hyperglycemia Increases Risk of Diabetes in Pima Indians
Prevalence of T2DM among year olds 50 40 30 % with T2DM 20 10 No DM DM Maternal Status During Pregnancy Pettitt Diabetes 1988

9
Is there a threshold of blood glucose level during pregnancy ?
Franks Diabetes 2006

10
What are the mechanisms that explain the higher risk for type 2 diabetes in offspring of diabetic mothers in Pima Indians? Body composition ? Insulin action ? Insulin secretion ? We conducted 2 experiments to determine the mechanisms that increase the risk for diabetes in the adult offspring of Pima Indians with early onset diabetes in the parents

11
Reduced acute insulin response in adult NGT offspring of diabetic women
Insulin secretion Insulin action 1600 P = 0.018 P = 0.6 20 1200 15 AIR (pmol/l) M720 (mmol/kg MBS.min) 10 800 5 400 DM No DM DM No DM Maternal DM status during pregnancy Gautier J.F. Diabetes, 2001
 M720 (mmol/kg MBS.min) DM. No DM. DM. No DM. Maternal DM status during pregnancy. Gautier J.F. Diabetes,")
12
Conclusion Intra uterine exposure to maternal diabetes in Pima Indians : Increases the risk for type 2 diabetes in offspring Is associated with a decreased acute insulin response to IV glucose in adult offspring with normal glucose tolerance Does not worsen insulin resistance and body fat accumulation usually observed in Pima Indians “In utero diabetes” acquired defect in insulin secretion

13
The effects of intrauterine exposure to diabetes may be confounded by genetic factors :
Women who develop diabetes at earlier age might carry more diabetes-susceptibility genes than those who develop diabetes later and therefore might transmit greater genetic susceptibility to their offspring

14
Relationship Between Insulin Secretion and Parental Age of Diabetes Onset
P=0.03; r=0.23 1500 P =0.02 3 DMO > 49y 1000 2.5 Log AIR (U/ml) Insulin Secretion Rate (pmol/min) DMO < 35y 2 500 Acute insulin secretion in response to IV glucose was correlated with the age of onset of diabetes of the mother. These are adjusted values for age, sex, % body fat and insulin action. In contrast, AIR was not correlated with the age of diabetes onset of the father. 1.5 20 40 60 80 50 100 150 200 250 300 Age of Diabetes Onset of the Mother (years) Plasma Glucose (mg/dl) Adjusted for age, sex, % body fat, and insulin action Gautier J.F. Diabetes, 2001
 Insulin Secretion Rate. (pmol/min) DMO < 35y Acute insulin secretion in response to IV glucose was correlated with the age of onset of diabetes of the mother. These are adjusted values for age, sex, % body fat and insulin action. In contrast, AIR was not correlated with the age of diabetes onset of the father Age of Diabetes Onset of the Mother. (years) Plasma Glucose (mg/dl) Adjusted for age, sex, % body fat, and insulin action. Gautier J.F. Diabetes,")
15
Conclusion Offspring of mothers with early onset diabetes have lower insulin secretion rates with no aggravation of insulin resistance Inherited factors Insulin secretion

16
How to solve the problem
How to solve the problem ? To determine the role of intrauterine exposure per se To compare the prevalence of diabetes in Pima nuclear families in which at least 1 sibling was born before and after the mother was diagnosed with T2D To study the effect of intrauterine exposure to type 1 diabetes (to circumvent the confounding effect of genetic factors related to T2D)
")
17
Dabelea D, Diabetes, 2000, 49: 58 siblings from 19 families In 15 of the sibships : diabetes more frequent after mother ’s diagnosis of diabetes In 4 of the sibships : diabetes occured only before mother ’s diagnosis of diabetes Odds ratio : 3.7 (CI: ) ; p = 0.024
 ; p =")
18
Dabelea D, 2000

19
Inclusion Criteria We proposed to adult offspring of confirmed type 1 diabetic patients attending our department to participate in the study if : They were non diabetic They were born after the diagnosis of parental diabetes They had no family history of type 2 diabetes (first-degree relative) They had no type 1 diabetes-associated autoantibodies (ICA, anti-GAD, anti-IA2)
 They had no type 1 diabetes-associated autoantibodies (ICA, anti-GAD, anti-IA2)")
20
Subjects 31 subjects fulfilled the inclusion criteria, they were offspring of: Type 1 diabetic mother (diabetes diagnosed before the index pregnancy) n = 15 Type 1 diabetic father (diabetes diagnosed before the birth of the offspring) n = 16
 n = 15. Type 1 diabetic father (diabetes diagnosed before the birth of the offspring) n = 16.")
21
INVESTIGATIONS Measurement of body composition by dual-energy X ray absorptiometry (DEXA) 75g Oral Glucose Tolerance Test: Glucose tolerance status (WHO 1985 criteria) Early insulin secretion (I30 – I0 / G30 – G0) Insulin action: Euglycemic Hyperinsulinemic Clamp at 80 mU/m2/min Insulin secretion: Graded glucose infusion (5 x 40 min steps) at 2, 4, 8, 12 et 16 mg/kg/min with measurement of glucose and C-peptide Calculation of Insulin Secretion Rate by C-peptide deconvolution analysis All subjects had a measurement of body composition, an OGTT, a 2-step hyperinsulinemic glucose clamp to measure insulin action at low and high insulin infusion doses and an IVGTT to estimate the acute insulin response to IV glucose.
 Early insulin secretion (I30 – I0 / G30 – G0) Insulin action: Euglycemic Hyperinsulinemic Clamp. at 80 mU/m2/min. Insulin secretion: Graded glucose infusion (5 x 40 min steps) at 2, 4, 8, 12 et 16 mg/kg/min with measurement of glucose and C-peptide. Calculation of Insulin Secretion Rate by C-peptide deconvolution analysis. All subjects had a measurement of body composition, an OGTT, a 2-step hyperinsulinemic glucose clamp to measure insulin action at low and high insulin infusion doses and an IVGTT to estimate the acute insulin response to IV glucose.")
22
Characteristics of the Volunteers
Offspring of diabetic mother (Subjects) Offspring of diabetic father (Controls) Mean difference [95% CI] N 15 16 M:F (n) 6:9 6:10 Age (yr)¤ 23.9 5.9 22.7 4.1 -1.2 [-4.8 ; 2.6] Birth weight (g)¤ 3306 400 3322 319 16 [-302 ; 333] SBP (mmHg)¤ 118 13 119 9 2 [-6 ; 9] BMI (kg.m-²)¤ 22.5 3.6 23.1 5.6 0.7 [-2.8 ; 4.1] Percent body fat (%)¤ M F 13.9 5.1 27.0 5.9 12.4 6.1 31.0 12.2 -1.5 [-9.3 ; 6.3] 4.0 [-6.2 ; 14.3] Mean SD
 Offspring of diabetic father. (Controls) Mean difference. [95% CI] N M:F (n) 6:9. 6:10. Age (yr)¤ 23.9 [-4.8 ; 2.6] Birth weight (g)¤ 3306 [-302 ; 333] SBP (mmHg)¤ 118 9. 2 [-6 ; 9] BMI (kg.m-²)¤ 22.5 [-2.8 ; 4.1] Percent body fat (%)¤ M. F [-9.3 ; 6.3] 4.0 [-6.2 ; 14.3] Mean SD.")
23
Oral Glucose Tolerance
Offspring of Type 1 diabetic mothers (n = 15) Impaired glucose tolerance: 33% (5/15) Normal glucose tolerance: 67% (10/15) Offspring of Type 1 diabetic fathers (n = 16) All had normal glucose tolerance (100%)
 Impaired glucose tolerance: 33% (5/15) Normal glucose tolerance: 67% (10/15) Offspring of Type 1 diabetic fathers (n = 16) All had normal glucose tolerance (100%)")
24
Insulin action and secretion in offspring of T1DM mothers
Early insulin secretion N=10 N=5 25 p = 0.035 16 20 p = 0.037 14 in mg.min-1.kg-1 of fat-free mass Adjusted M-value 12 15 10 (I30-I0)/(G30-G0) 8 10 6 4 5 2 NGT offspring of type 1 father NGT offspring of type 1 mother IGT offspring of type 1 mother Off father NGT Off mother IGT Off mother Sobngwi E. Lancet 2003
/(G30-G0) NGT offspring of type 1 father. NGT offspring of type 1 mother. IGT offspring of type 1 mother. Off father. NGT Off mother. IGT Off mother. Sobngwi E. Lancet")
25
ISR Sobngwi Lancet 2003

26
Summary This study suggests that in utero exposure to a type 1 diabetic environment : Is associated with impaired glucose tolerance in 1/3 adult offspring in the study population Is associated with a defective insulin secretory response (kinetics and magnitude) to oral and intravenous glucose Is not associated with altered insulin sensitivity Is not associated with fat mass accumulation
 to oral and intravenous glucose. Is not associated with altered insulin sensitivity. Is not associated with fat mass accumulation.")
27
Prevalence of impaired glucose tolerance in offspring of diabetic mothers
198 offspring of mothers with T1D or gestational diabetes Range of yr T1D Gestational diabetes yr 10.8% ( 14 / 129 ) 13% ( 9 / 69 ) yr 9.4% ( 10 / 106 ) 11.1% ( 6 / 54 ) yr 17.4% (4 / 23 ) 20.0% ( 3 / 15 ) Plagemann Diabetologia 1997
 13% ( 9 / 69 ) yr. 9.4% ( 10 / 106 ) 11.1% ( 6 / 54 ) yr. 17.4% (4 / 23 ) 20.0% ( 3 / 15 ) Plagemann Diabetologia")
28
Silverman Diabetes Care 1995
Prevalence of impaired glucose tolerance in offspring of diabetic mothers 367 offspring of mothers with T1D or gestational diabetes Range of age N IGT < 5 yr 168 1.2% 5 – 9 yr 111 5.4% 10 – 16 yr 88 19.3% (p<0.005) Control group (10-16 yr) 80 2.5% Silverman Diabetes Care 1995
 Control group (10-16 yr) % Silverman Diabetes Care")
29
FSIGTT : Bergman's minimal model
Insulin sensitivity/secretion in prebubertal offspring exposed to a diabetic intrauterine environment Groups of offspring : 17 offspring of type 1 diabetic women 10 offspring of type 2 diabetic women 50 control children Aged between 5 and 10 years FSIGTT : Bergman's minimal model insulin sensitivity and acute insulin response were not statistically different in the 3 groups Hunter Diabetes Care 2004

30
Early insulin secretion in adult offspring of mothers with young-onset of T2D
Singh Diabetologia 2006

31
Outline Epidemiological evidences of maternal transmission of diabetes Metabolic defects associated with foetal exposure to maternal diabetes Potential mechanisms: what did we learn from animal studies? Multi organ defects as a consequences of maternal diabetes in human offspring Late consequences

32
What are the cellular and molecular mechanisms ?
Oxidative stress due to hyperglycaemia (apoptosis, disturbed organogenesis) Foetal hyperinsulinism (abnormal hypothalamic development) Altered angiognenesis Exposure to glucocorticoid excess Epigenetic modifications (imprinted genes or not) Reduced organ mass Multi organ defect
 Foetal hyperinsulinism (abnormal hypothalamic development) Altered angiognenesis. Exposure to glucocorticoid excess. Epigenetic modifications (imprinted genes or not) Reduced organ mass. Multi organ defect.")
33
Animal studies 1st generation Mild diabetes Severe diabetes
6.5 and 9.8 mmol/l glycaemia > 20 mmol/l 2nd generation Foetus Mild Hyperglyc. Severe Hyperglyc. Hypersinsulinaemia Hypoinsulinaemia Macrosomia Microsomia Adult Decreased -cell Increased -cell response response Insulin resistance Pregnant Gestational diabetes Gestational diabetes Aerts 1997 ; Holemans 1991 ; Gauguier 1990 ; Bihoreau 1986 …..

34
Animal studies 1st generation Mild diabetes Severe diabetes
3rd generation Foetus: Mild Hyperglyc. Mild Hyperglyc. Hypersinsulinaemia Hyperinsulinaemia Adult Impaired glucose Impaired glucose tolerance tolerance Aerts 1990 ; Gauguier 1990 ; Aerts, 1990

35
Goto Kakizaki (GK) rats
Rodent model of non obese type 2 diabetes Produced by selective breeding of individuals with mild glucose intolerance from a non diabetic Wistar rat colony (Portha 1991) Foetuses have a reduced beta cell mass (Serradas 1998) Adults display : Mild hyperglycaemia, glucose intolerance Impaired glucose-induced insulin secretion Decreased beta cell mass Hepatic glucose overproduction Moderate peripheral insulin resistant (muscle and adipose) tissues (Portha 1991 , Bisbis Movassat 1995)
 Foetuses have a reduced beta cell mass (Serradas 1998) Adults display : Mild hyperglycaemia, glucose intolerance. Impaired glucose-induced insulin secretion. Decreased beta cell mass. Hepatic glucose overproduction. Moderate peripheral insulin resistant (muscle and adipose) tissues. (Portha 1991 , Bisbis Movassat 1995)")
36
R. Gill-Randall et al Diabetologia (2004) 47:1354–1359
Adult offspring from Wistar gametes reared in hyperglycaemic GK mothers were significantly more hyperglycaemic at adulthood than offspring from Wistar gametes transferred back into euglycaemic Wistar mothers At 6 months

37
Endothelial cell Proliferation
Diabetes 53:752–761, 2004 Control CAM Hyperglycaemic glucose-injected CAM Endothelial cell Proliferation

39
L’exposition in utero au diabète maternel chez le rat entraîne une réduction du capital néphronique

40
Outline Epidemiological evidences of maternal transmission of diabetes Metabolic defects associated with foetal exposure to maternal diabetes Potential mechanisms: what did we learn from animal studies? Multi organ defects as a consequences of maternal diabetes in human offspring Late consequences

41
(mg/kg fat free mass /min)
% Insulin sensitivity Fat mass (DXA) p = 0.44 p = 0.75 glucose utilisation (mg/kg fat free mass /min) N=29 N=29 (±sd) N=29 N=29
 p = p = glucose utilisation. (mg/kg fat free mass /min) N=29. N=29. (±sd) N=29. N=29.")
42
Early insulin secretion in response to OGTT
Off T1D F OFF T1D M (médiane)
")
43
Insulin secretion in response to IV glucose
Significant interaction between group and offspring gender was found for the slope of ISR ( p= 0.03)
")
44
Arginine test Insulin Glucagon p = 0.10 Off T1D F Off T1D M p = 0.6
(médiane)
")
45
Pancreatic exocrine dysfunction
Off of DT1 Fathers (n=29) Off of T1D Mothers p Stool weight, moy (sd) , g/24h 124 (56) 112 (66) 0.57 Faecal fat output, 4.9 (2.7) 3.7 (2.3) 0.13 Chymotrypsin activity, moy (sd), U/g 22.8 (13.0) 14.5 (7.2) 0.016 Elastase concentration, moy (sd) µg/g 451 (100) 487 (30) 0.12
 Off of T1D Mothers. p. Stool weight, moy (sd) , g/24h. 124 (56) 112 (66) Faecal fat output, 4.9 (2.7) 3.7 (2.3) Chymotrypsin activity, moy (sd), U/g (13.0) 14.5 (7.2) Elastase concentration, moy (sd) µg/g. 451 (100) 487 (30)")
46
Inter-group changes p= 0.009
GFR changes Relative changes: +8(13), p= Relative changes: +19(17), p= 0.002 Inter-group changes p= 0.009 Diabetes 2010
, p= Relative changes: +19(17), p= Inter-group changes p= Diabetes")
47
Outline Epidemiological evidences of maternal transmission of diabetes Metabolic defects associated with foetal exposure to maternal diabetes Potential mechanisms: what did we learn from animal studies? Multi organ defects as a consequences of maternal diabetes in human offspring Late consequences

52
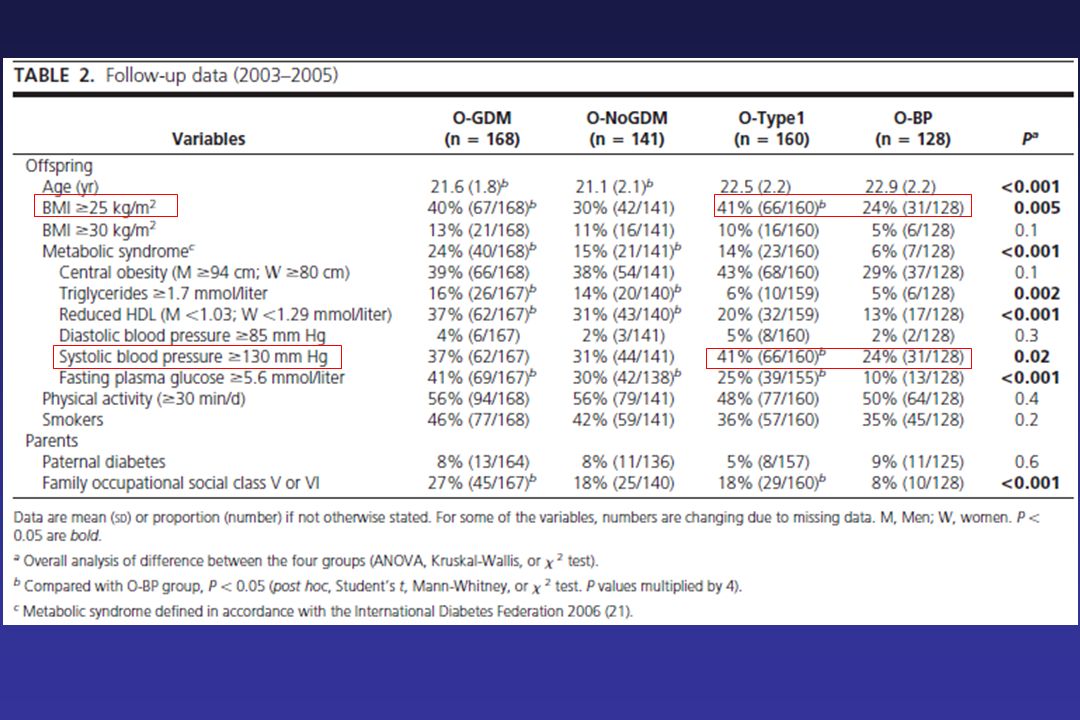
In Utero Exposure to Maternal Type 1 Diabetes
Risk of Diabetes Prevalence of prediabetes among 22 year olds 50 40 30 % with T2DM 20 3 % (4/128) 9 % (14/160) 10 No DM DM Maternal Status During Pregnancy Clausen Diabetes Care 2008
 9 % (14/160) 10. No DM. DM. Maternal Status During Pregnancy. Clausen Diabetes Care")
53
Nelson 1998

54
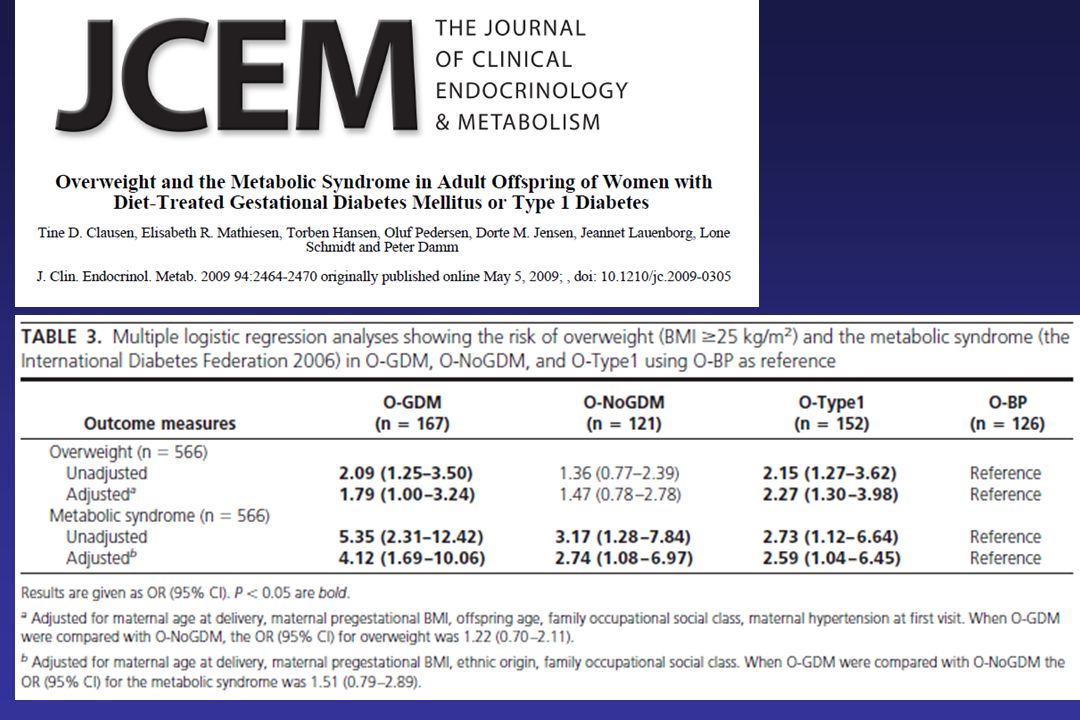
Conclusions (1) Intrauterine exposure to maternal diabetes is associated in adult offspring with multi organ dysfunction: an insulin secretion dysfunction (female offspring) a defect of the exocrine pancreas a decrease in renal functional reserve Late consequences of exposure in utero to maternal type 1 diabetes are IGT, type 2 diabetes, high blood pressure, microalbuminuria, metabolic syndrome and possibly CVD This need to be confirmed in larger longitudinal studies with adequate control groups
 a defect of the exocrine pancreas. a decrease in renal functional reserve. Late consequences of exposure in utero to maternal type 1 diabetes are IGT, type 2 diabetes, high blood pressure, microalbuminuria, metabolic syndrome and possibly CVD. This need to be confirmed in larger longitudinal studies with adequate control groups.")
55
Conclusions (2) Underlying mechanisms need to be unraveled :
epigenetic studies capillary density studies ….. Intensive glucose control maintained throughout pregnancy may contribute to a decrease in the prevalence of T2D and renal dysfunction in later life

56
Diabetes Parents Offspring CV disease
Pathophysiologic vicious circle model for development of type 2 diabetes Insulin resistance Genetic Factors Environmental factors IGT Cell dysfunction Diabetes Parents Diabetes during pregnancy Offspring Genetic Factors Environmental factors Renal dysfunction CV disease

58
Contact Dr LS Fetita Tel : 01 42 49 48 57 / 96 96
Cell : Fax :

59
PROJET

60
ETUDE EPIDEMIOLOGIQUE
Objectif : montrer une augmentation de la prévalence du diabète de type 2 chez les descendants adultes de mères ayant un diabète de type 1 comparativement aux descendants de pères diabétiques de type 1 Nombre de sujets nécessaire: Hypothèse : prévalence à 4 ans du diabète de type 2 respectivement 10.8% vs 1% 110 par groupe de descendants âgés de plus de 30 ans Méthodes : Questionnaire aux parents DT1 : Descendants diabétiques et non diabétiques (T1 et T2) Aux descendants non diabétiques : HGPO, Ac, HLA
 Aux descendants non diabétiques : HGPO, Ac, HLA.")
61
ETUDE PHYSIOLOGIQUE Evaluer si l’exposition au diabète in utero est associée à : Une altération globale de la fonction pancréatique Des anomalies rénales

62
ETUDE PHYSIOLOGIQUE Explorations de la fonction endocrine Sécrétions d’insuline et de glucagon : en réponse au glucose et à l’arginine Action de l’insuline : clamp euglycémique hyperinsulinique et Exploration de la fonction exocrine du pancréas Dosage des graisses totales, de l’élastase et de l’activité chymotrypsique fécales

63
ETUDE PHYSIOLOGIQUE Exploration de la fonction rénale
Dosage de l’excrétion urinaire d’albumine au repos et à l’effort Holter tensionnel des 24h Réserve fonctionnelle rénale: Débit de filtration glomérulaire isotopique en réponse à une perfusion d’acides aminés Composition corporelle (DEXA)
")
64
Mécanismes 1. Défaut d’angiogénèse pendant la vie fœtale Atteinte multiviscérale ? 2. Phénomène d’empreinte maternelle ?

65
Diabète in utero et anomalies rénales ( Nelson R. G. et al
Diabète in utero et anomalies rénales ( Nelson R.G. et al. Diabetes 1998) Population : 503 Indiens Pimas diabétiques de type 2 207 descendants de mères non diabétiques 246 descendants de mères diabétiques postérieurement à la grossesse 50 descendants de mères diabétiques pendant la grossesse Prévalence de l’élévation de l’excrétion urinaire de l’albumine Descendants de mères non diabétiques 40 % Descendants de mères diabétiques postérieurement à la grossesse 43 % Descendants de mères diabétiques 58 % Odd Ratio d’une excrétion urinaire d’albumine élevée 3.8 (95% CI ) chez les descendants de mères diabétiques par rapport aux descendants de mères diabétiques postérieurement à la grossesse (ajustement pour l’âge, le sexe, la durée du diabète, HbA1C et la pression artérielle)
 Population : 503 Indiens Pimas diabétiques de type descendants de mères non diabétiques. 246 descendants de mères diabétiques postérieurement à la grossesse. 50 descendants de mères diabétiques pendant la grossesse. Prévalence de l’élévation de l’excrétion urinaire de l’albumine. Descendants de mères non diabétiques 40 % Descendants de mères diabétiques postérieurement à la grossesse 43 % Descendants de mères diabétiques 58 % Odd Ratio d’une excrétion urinaire d’albumine élevée 3.8 (95% CI ) chez les descendants de mères diabétiques. par rapport aux descendants de mères diabétiques postérieurement à la grossesse. (ajustement pour l’âge, le sexe, la durée du diabète, HbA1C et la pression artérielle)")
66
Diabète de type 2 Trait familial :
Obésité, insulino-sensibilité, et insulino-sécrétion Lillioja 1987, Knowler 1991, Janssen 1994, Sakul 1997 Analyses de Ségrégation : Un gène majeur influence l ’âge de survenue du diabète Hanson R et al, Am J Hum Genet, 1995, 57 : Porte-t-il sur la composition corporelle, l’action de l’insuline ou la sécrétion de l’insuline ?

67
Plasma Glucose (mg/dl)
Study 2: Changes in Plasma Glucose and Insulin Concentrations During the Stepped Glucose Infusion Test DMO > 49 y DMO < 35 y Plasma Glucose (mg/dl) Plasma Insulin (mU/l) The stepped glucose infusion test consisted of infusing glucose at 2, 3, 4, 6, 8 mg per kg and per min, each step lasting 40 min. This slide shows you the average glucose values during each step in the left and the average insulin values in the right panel. Subject whose mother had early diabetes onset are shown in yellow. Subjects whose mother had late diabetes onset are shown in white. Changes in glucose and insulin concentrations were similar in the two groups. GINF (mg.kg-1.min-1) GINF (mg.kg-1.min-1)
 Plasma Insulin (mU/l) The stepped glucose infusion test consisted of infusing glucose at 2, 3, 4, 6, 8 mg per kg and per min, each step lasting 40 min. This slide shows you the average glucose values during each step in the left and the average insulin values in the right panel. Subject whose mother had early diabetes onset are shown in yellow. Subjects whose mother had late diabetes onset are shown in white. Changes in glucose and insulin concentrations were similar in the two groups. GINF (mg.kg-1.min-1) GINF (mg.kg-1.min-1)")
68
Pettitt DJ et al, Diabetes, 1988, 37 : 622-628
Effet du Diabète Pendant la Grossesse sur la Prévalence du Diabète de Type 2 dans la Descendance Prévalence du diabète de type 2 chez les indiens Pimas âgés de 20 à 24 ans : ~ 45 % lorsque la mère était diabétique pendant la grossesse ~ 9 % lorsque la mère a développé un diabète postérieurement à la grossesse Pettitt DJ et al, Diabetes, 1988, 37 :

69
But de l’Etude Evaluer les mécanismes possibles responsables de l’augmentation du risque de diabète de type 2 chez les descendants de mère diabétique pendant la grossesse Composition corporelle ? Action de l’insuline ? Sécrétion de l’insuline ? We conducted 2 experiments to determine the mechanisms that increase the risk for diabetes in the adult offspring of Pima Indians with early onset diabetes in the parents

70
Masse grasse et action de l’insuline
Oui Non M720 (mmol/kg MBS.min) P = 0,6 15.5 14.9 Oui Non Masse Grasse (%) 34 33 P = 0,8 Diabète Pendant la Grossesse de la Mère
 P = 0, Oui. Non. Masse Grasse (%) P = 0,8. Diabète Pendant la Grossesse de la Mère.")
71
Phase Précoce de l’Insulino-sécrétion
Moyenne Géométrique (IC 95%) P = 0,018 Oui Non * Insulino-sécrétion (pmol/l) 1255 740 Diabète Pendant la Grossesse de la Mère Ajustée pour l’âge, le sexe, la masse grasse et l’action de l’insuline Gautier J.F., Diabetes, 2001
 P = 0,018. Oui. Non. * Insulino-sécrétion. (pmol/l) Diabète Pendant la Grossesse de la Mère. Ajustée pour l’âge, le sexe, la masse grasse et l’action de l’insuline. Gautier J.F., Diabetes,")
72
Résumé Le « diabète in utero » déficit acquis de l’insulino-sécrétion
Cette étude suggère que le diabète in utero chez les indiens Pimas : Entraîne une diminution de la phase précoce de l’insulino-sécrétion en réponse au glucose chez les descendants adultes ayant une tolérance au glucose normale N’aggrave pas l’insulino-résistance habituellement observée dans cette population Ne contribue pas à une accumulation de masse grasse supplémentaire Le « diabète in utero » déficit acquis de l’insulino-sécrétion

73
Solution 2 Evaluer les effets du diabète in-utero sur les facteurs métaboliques prédisposant au diabète de type 2 chez les descendants de patients présentant un diabète de type 1 Composition corporelle ? Action de l’insuline ? Sécrétion de l’insuline ? We conducted 2 experiments to determine the mechanisms that increase the risk for diabetes in the adult offspring of Pima Indians with early onset diabetes in the parents

74
Méthodes Descendants majeurs de patients diabétiques de type 1 suivis à l’hôpital Saint-Louis : Nés après le diagnostic du diabète chez leur parent Non diabétiques Sans stigmates d’autoimmunité du diabète de type 1 (ICA, anti-GAD, anti-IA2) Sans antécédents familiaux connus de diabète de type 2 Descendants de mères Descendants de pères (groupe contrôle)
 Sans antécédents familiaux connus de diabète de type 2. Descendants de mères. Descendants de pères (groupe contrôle)")
75
Composition corporelle: DEXA HGPO: Tolérance au glucose (critère OMS)
Méthode (2) Composition corporelle: DEXA HGPO: Tolérance au glucose (critère OMS) Action de l’insuline: Clamp hyperinsulinémique euglycémique 80 mU/m2/min Sécrétion de l’insuline: Perfusion de glucose par palier de 40 min 2, 4, 8, 12 et 16 mg/kg/min All subjects had a measurement of body composition, an OGTT, a 2-step hyperinsulinemic glucose clamp to measure insulin action at low and high insulin infusion doses and an IVGTT to estimate the acute insulin response to IV glucose.
 Composition corporelle: DEXA. HGPO: Tolérance au glucose (critère OMS) Action de l’insuline: Clamp hyperinsulinémique euglycémique. 80 mU/m2/min. Sécrétion de l’insuline: Perfusion de glucose par palier de 40 min. 2, 4, 8, 12 et 16 mg/kg/min. All subjects had a measurement of body composition, an OGTT, a 2-step hyperinsulinemic glucose clamp to measure insulin action at low and high insulin infusion doses and an IVGTT to estimate the acute insulin response to IV glucose.")
76
31 sujets répondaient aux critères d ’inclusion :
Mère diabétique avant la grossesse n = 15 Père diabétique avant la naissance du descendant n = 16

77
Characteristics of volunteers
Offspring of diabetic mother (Subjects) Offspring of diabetic father (Controls) Mean difference [95% CI] N 15 16 M:F (n) 6:9 6:10 Age (yr)¤ 23.9 5.9 22.7 4.1 -1.2 [-4.8 ; 2.6] Birth weight (g)¤ 3306 400 3322 319 16 [-302 ; 333] SBP (mmHg)¤ 118 13 119 9 2 [-6 ; 9] DBP (mmHg)¤ 65 8 70 14 6 [-3 ; 14] Serum creatinine (mol.l-1)¤ 82 10 79 10 -3 [-11 ; 4] BMI (kg.m-²)¤ 22.5 3.6 23.1 5.6 0.7 [-2.8 ; 4.1] Percent body fat (%)¤ M F 13.9 5.1 27.0 5.9 12.4 6.1 31.0 12.2 -1.5 [-9.3 ; 6.3] 4.0 [-6.2 ; 14.3] Mean SD
 Offspring of diabetic father. (Controls) Mean difference. [95% CI] N M:F (n) 6:9. 6:10. Age (yr)¤ 23.9 [-4.8 ; 2.6] Birth weight (g)¤ 3306 [-302 ; 333] SBP (mmHg)¤ 118 9. 2 [-6 ; 9] DBP (mmHg)¤ 65 [-3 ; 14] Serum creatinine (mol.l-1)¤ 82 [-11 ; 4] BMI (kg.m-²)¤ 22.5 [-2.8 ; 4.1] Percent body fat (%)¤ M. F [-9.3 ; 6.3] 4.0 [-6.2 ; 14.3] Mean SD.")
78
OGTT NGT Controls NGT Subjects IGT Subjects N 16 10 5 G0 4.6 0.5
NGT Controls NGT Subjects IGT Subjects N 16 10 5 G0 4.6 0.5 4.5 0.7 5.0 0.4 G30 6.6 1.5 7.0 1.3 7.3 2.2 G120 5.3 1.2 6.0 1.0 8.6 0.7 I0 4.7 2.4 5.6 5.1 3.8 2.1 I30 37.8 19.4 42.4 27.6 25.4 16.2 I120 25.5 16.6 34.4 23.2 33.3 19.4

79
MLM

80
Early Insulin Secretion

81
EVOLUTION DE LA GLYCEMIE AU COURS DE LA PERFUSION DE GLUCOSE PAR PALIER
mg.kg-1.min-1 16 12 8 4 2 Glycemie (mmol/l) moy+/-SD 30 25 20 15 10 5 Desc. de Pere Mere
 moy+/-SD Desc. de. Pere. Mere.")
82
C-Peptide

83
Résumé Cette étude suggère que le diabète de type 1 in utero :
Est associé à une intolérance au glucose chez plus de 30 % des descendants majeurs Entraîne une diminution de l’insulino-sécrétion en réponse au glucose oral et intraveineux N’entraîne pas une insulino-résistance Ne contribue pas à une accumulation de masse grasse

84
Conclusion Le diabète de type 1 in utero:
Entraîne un déficit acquis de l’insulino-sécrétion en réponse au glucose chez les descendants adultes Confère aux descendants adultes une fréquence élevée d’intolérance au glucose Augmente le risque de développer un diabète de type 2 ? Mécanismes ?

85
Study 2: Characteristics of the Subjects
8 subjects whose mother had early diabetes onset and 15 subjects whose mother had late diabetes onset were included in this study. Sex ratio, age, and %body fat were similar in the 2 groups. Fasting and 2 hour glucose and insulin action were also similar.

86
Study 2: Relationship Between Insulin Secretion Rates and Plasma Glucose Levels
Average ISR 65080 P =0.02 DMO > 49 y Insulin Secretion Rate (pmol/min) DMO < 35 y 43986 P=0.007 This slide depicts the relationship between ISR and plasma glucose levels. The curve is significantly lower in subjects whose mother developed diabetes before age 35. Also, the average ISR over the total period was significantly reduced in this group. Plasma Glucose (mg/dl) Gautier J.F., Diabetes, 2001
 DMO < 35 y. 43986. P= This slide depicts the relationship between ISR and plasma glucose levels. The curve is significantly lower in subjects whose mother developed diabetes before age 35. Also, the average ISR over the total period was significantly reduced in this group. Plasma Glucose (mg/dl) Gautier J.F., Diabetes,")
87
PP

88
Résumé Le « diabète in utero » déficit acquis de l’insulino-sécrétion
Cette étude suggère que le diabète in utero chez les indiens Pimas : Entraîne une diminution de la phase précoce de l’insulino-sécrétion en réponse au glucose chez les descendants adultes ayant une tolérance au glucose normale N’aggrave pas l’insulino-résistance habituellement observée dans cette population Ne contribue pas à une accumulation de masse grasse supplémentaire Le « diabète in utero » déficit acquis de l’insulino-sécrétion

89
Groupe contrôle (10-16ans) 80 2.5%
Prévalence de l’intolérance au glucose chez les descendants de mères diabétiques 367 descendants de mères DT1 ou ayant présenté un diabète gestationnel Tranche d’âge N IGT < 5 ans 168 1.2% 5 – 9 ans 111 5.4% 10 – 16 ans 88 19.3% (p<0.005) Groupe contrôle (10-16ans) 80 2.5% Silverman Diabetes Care 1995
 Groupe contrôle (10-16ans) % Silverman Diabetes Care")
91
Metabolic Defects in Type 2 Diabetes
Peripheral insulin resistance in muscle and fat Decreased pancreatic insulin secretion Increased hepatic glucose output Haffner Diabetes Care 1999

92
Physiopathologie du diabète de type 2
Facteurs environnementaux Facteurs génétiques Etudes des descendants de parents diabétiques

93
} } Diabète de type 2 Poids corporel Insulino-sensibilité
Obésité Diminution de l’action de l’insuline Altération de la sécrétion de l’insuline Poids corporel Insulino-sensibilité Insulino-sécrétion } Anomalies prédictives } Trait familial

94
Rôle de la mère dans la transmission du diabète de type 2
Référence Population Ratio mères/pères atteints Alcolado J.C.et al.1992 Mitchell B.D.et al.1993 Thomas F.et al.1994 Lin R.S.et al. 1994 Young C.A.et al.1995 Viswanathan M.et al.1995 McCarthy M.et al.1996 Klein B.E.K.et al.1996 Riley M.D.et al.1996 Karter A.J.et al.1999 Meigs J.B.et al.2000 Bo S.et al.2000 Bjornholt J.V.et al.2000 Britannique Mexicains/Caucasiens américains Française Taiwanaise Européens/Caraïbes Indiens Wisconsin,USA Tasmanie Californie du Nord Framingham Italiens Norvégienne 2.1 NS 2.6 2.1/ 1.9 2.0 2.7 1.2 4.0 1.5 Review in Alcolado 2002

95
Anomalies génétiques : facteur de confusion des effets de l’exposition du diabète in utero
Les femmes présentant un diabète pendant la grossesse, ont un diabète à révélation précoce et peuvent donc porter plus de gènes de susceptibilité, qu’elles peuvent transmettre à leurs descendants

96
Option 2 Descendants majeurs de patients diabétiques de type 1 :
Nés après le diagnostic du diabète chez leur parent Non diabétiques Sans stigmates d’autoimmunité du diabète de type 1 (ICA, anti-GAD, anti-IA2) Sans antécédents familiaux connus de diabète de type 2 Descendants de mères Descendants de pères (groupe contrôle)
 Sans antécédents familiaux connus de diabète de type 2. Descendants de mères. Descendants de pères (groupe contrôle)")
97
Conclusion Le diabète de type 1 in utero:
Entraîne un déficit acquis de l’insulino-sécrétion en réponse au glucose chez les descendants adultes Confère aux descendants adultes une fréquence élevée d’intolérance au glucose

98
Quels mécanismes cellulaires ?
1. Phénomène d’empreinte parentale ? 2. Défaut d’angiogénèse pendant la vie fœtale Atteinte multiviscérale ?

99
Conclusion Il existe un excès de transmission maternelle du diabète de type 2 Cet excès est en partie expliqué par l’exposition au diabète in utero L’exposition au diabète in utero est associé à un déficit de l’insulinosécrétion chez le descendant Les mécanismes impliqués restent à définir

100
The Framingham Offspring Study
Population 2527 descendants issus de 1303 familles caucasiennes Moyenne d’âge: 54 ans , femmes: 53% Diabétiques: 8.6% ; intolérance au glucose: 11.4% Diagnostic du diabète Descendants: Glycémie à jeun >7.8 mmol/l à 2 reprises ou HGPO Ou sous ADO Parents: sous ADO ou glycémie > 11.1 mmol/l Antécédents familiaux de diabète mère diabétique: 10.5% père diabétique: 11.5% 2 parents diabétiques: 1.7% parents non diabétiques: 76.3% Meigs Diabetes 2000

101
The Framingham Offspring Study
Population 2527 descendants issus de 1303 familles caucasiennes Moyenne d’âge: 54 ans , femmes: 53% Diabétiques: 8.6% ; intolérance au glucose: 11.4% Diagnostic du diabète Descendants: Glycémie à jeun >7.8 mmol/l à 2 reprises ou HGPO Ou sous ADO Parents: sous ADO ou glycémie > 11.1 mmol/l Antécédents familiaux de diabète mère diabétique: 10.5% père diabétique: 11.5% 2 parents diabétiques: 1.7% parents non diabétiques: 76.3% Meigs Diabetes 2000

Présentations similaires

















 Nombres (1-100).>")


 Please Translate the Following: 1. I love the math course. (Adorer.>")

