Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Traitements médicamenteux du SDRA
Laurent PAPAZIAN Réanimation médicale Unité de Recherche en Maladies Infectieuses et Tropicales Émergentes Hôpital Sainte-Marguerite Université de la Méditerranée Aix-Marseille II Glaxo-Smith-Kline: cisatracurium/placebo + 18,000 €

2
Limites On parlera de On ne parlera pas de Curares Protéine C activée
B2-mimétiques On ne parlera pas de Surfactant NO Almitrine PGI2 KGF Corticoïdes Viagra Albumine Furosemide Oligo-éléments Lipides…

3
NMBAs use in ARDS LOVS ACURASYS LaSRS ExPress

4
" there are no prospective, randomized, controlled trials assigning patients to a neuromuscular blocking agent versus a placebo with a goal of documenting if such patients could be managed by means other than neuromuscular blocking agent therapy " Task force SCCM,ACCP,ACCM

5
Effect of cisatracurium on oxygenation
NMBA/placebo 4 ICUs – 56 patients Gainnier et al. Crit Care Med 2004

6
Effect of cisatracurium on oxygenation
NMBA/placebo p < 0.001 4 ICUs – 56 patients Gainnier et al. Crit Care Med 2004

7
Effect of cisatracurium on oxygenation
NMBA/placebo p < 0.001 4 ICUs – 56 patients Gainnier et al. Crit Care Med 2004

8
Gainnier et al. Crit Care Med 2004

9
Forel et al. CCM 2006

10
Mortality ACURASYS

11
Outcomes Principal: mortality decrease at day 90 Secondary:
mortality: day 28 and ICU VFD and alive day 28 and day 90 Organ-failure free days (day 28) Barotrauma ICU-acquired muscular paresis
 Barotrauma. ICU-acquired muscular paresis.")
12
20 ICUs

13
cisatracurium vs. placebo
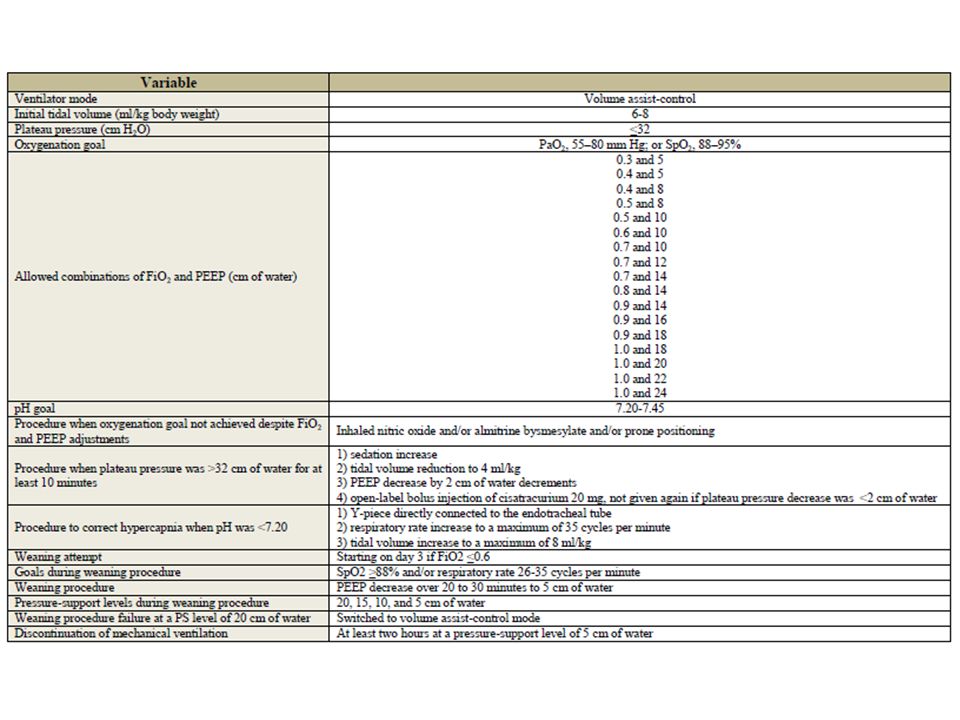
Design Prospective, randomized, double-blind study Open-label cisatracurium allowed according to an algorithm Vt 6-8 ml/kg, Pplat ≤ 32 cmH2O Inclusion criteria: PaO2:FiO2 < 150 (PEEP 5) for < 48 h cisatracurium vs. placebo
 for < 48 h. cisatracurium vs. placebo.")
14
Methods Prior to infusion : Ramsay 6
Cisatracurium: 6 x 150 mg / day for 2 days Volume-assist control mode PEEP and FiO2 according to the ARMA study Goal: SpO % or a PaO mmHg Weaning started on day 3 if FiO2 ≤ 0.6 Pressure support

16
Inclusion NMBA Placebo p Age 58±16 58±15 NS PEEP applied 9.2±3.2
9.2±3.5 Vt 6.55±1.12 6.48±0.92 Plateau pressure 25.0±5.1 24.4±4.7 PaO2/FiO2 106±36 115±41 0.029 SAPS II 50±16 47±14 Direct lung injury 142 (80%) 123 (76%) Inclusion < 48h intubation 152 (86%) 140 (86%) ARDS-inclusion, h 22±23 19±16
 123 (76%) Inclusion < 48h intubation. 152 (86%) 140 (86%) ARDS-inclusion, h. 22±23. 19±16.")
17
Inclusion NMBA Placebo p Age 58±16 58±15 NS PEEP applied 9.2±3.2
9.2±3.5 Vt 6.55±1.12 6.48±0.92 Plateau pressure 25.0±5.1 24.4±4.7 PaO2/FiO2 106±36 115±41 0.029 SAPS II 50±16 47±14 Direct lung injury 142 (80%) 123 (76%) Inclusion < 48h intubation 152 (86%) 140 (86%) ARDS-inclusion, h 22±23 19±16
 123 (76%) Inclusion < 48h intubation. 152 (86%) 140 (86%) ARDS-inclusion, h. 22±23. 19±16.")
18
Mortality Réduction relative de 25%

19
Mortality Réduction relative de 25%

20
Mortality d90 and PaO2/FiO2

21
Survival curve Cox multivariate proportional hazards model - PaO2/FiO2
NMBA placebo Cox multivariate proportional hazards model - PaO2/FiO2 Plateau pressure (predefined) SAPS II without PaO2/FiO2 (predefined) hazard ratio for death at 90 days in the NMBA group versus the control group of 0.68 (CI, 0.48 to 0.98) (P=0.04). NMBA 0.68 ( ), p = 0.04 Plateau pressure p = 0.04 SAPS II without PaO2/FiO2 p = 0.004
 SAPS II without PaO2/FiO2 (predefined) hazard ratio for death at 90 days in the NMBA group versus the control group of 0.68 (CI, 0.48 to 0.98) (P=0.04). NMBA 0.68 ( ), p = Plateau pressure p = SAPS II without PaO2/FiO2 p =")
22
Ventilator-free days and alive
NMBA Placebo p VFD 28 10.6 9.7 8.5 9.4 0.04 VFD 90 53.1 35.8 44.6 37.5 0.03 ICU-free days NMBA Placebo p ICU-FD 28 6.9 8.2 5.7 7.8 0.16 ICU-FD 90 47.7 33.5 39.5 35.6 0.03

23
No. of days without failure of nonpulmonary organs or systems, days 1 to 28
NMBA Placebo p kidney+coag+liver+circul. 15.8 9.9 12.2 11.1 0.002 circulation 18.3 9.4 16.6 10.4 0.12 coagulation 22.6 8.9 20.5 9.9 0.05 liver 21.3 9.6 19.1 10.6 kidney 20.5 10.1 18.1 11.6

24
Pneumothorax

25
Time from inclusion to pneumothorax

26
Open-label cisatracurium

27
ICU-acquired muscular paresis by ICU discharge
MRC score < 48

28
Pourquoi ? Homogénéisation ventilation régionale ?
Effet « protecteur » ? Effet propre de la molécule ?

29
* BAL IL1b IL6 IL8 * Forel et al. CCM 2006

30
Blood * IL1b IL6 * IL8 Forel et al. CCM 2006

31
d11: 240 mg/24h… decrease over several weeks
Critical Care Medicine: Volume 26(7) July 1998 pp Prolonged weakness after cisatracurium infusion: A case report Davis, Neil A. PharmD; Rodgers, Jo E. PharmD; Gonzalez, Edgar R. PharmD; Fowler, Alpha A. III, MD 45 yrs, aspiration, ARDS d2: cisatracurium d6-J11: solumedrol 500 mg/24h d11: 240 mg/24h… decrease over several weeks d13: stop cisatracurium d30: extubation d33: ICU discharge
 July 1998 pp Prolonged weakness after cisatracurium infusion: A case report. Davis, Neil A. PharmD; Rodgers, Jo E. PharmD; Gonzalez, Edgar R. PharmD; Fowler, Alpha A. III, MD. 45 yrs, aspiration, ARDS. d2: cisatracurium. d6-J11: solumedrol 500 mg/24h. d11: 240 mg/24h… decrease over several weeks. d13: stop cisatracurium. d30: extubation. d33: ICU discharge.")
32
Hansen-Flaschen et al. ARRD 93
Muscular paresis NMBAs > 48 h Hansen-Flaschen et al. ARRD 93 De Jonghe et al. JAMA 2002 Independent risk factors Women 4.66 More than one organ dysfunction 1.28 Duration of MV 1.1 Corticosteroids 14.9

33
NMBA + corticosteroids
Muscular atrophy (rat) surgical denervation + corticosteroids > corticosteroids or surgical denervation " several critically ill patients have developed myonecrosis after administration of very high doses of NMBAs alone "(61). Rouleau et al. Muscle Nerve 87 Hund CCM 99
 surgical denervation + corticosteroids > corticosteroids or surgical denervation. several critically ill patients have developed myonecrosis after administration of very high doses of NMBAs alone (61). Rouleau et al. Muscle Nerve 87. Hund CCM 99.")
34
Curares Systématique: oui mais « Curatifs » ???????
PaO2/FiO2 < 150 (120 ?) Tôt (48 premières h) Court: 2 jours « Curatifs » ???????
 Tôt (48 premières h) Court: 2 jours. « Curatifs »")
35
Protéine C activée Activation coagulation + suppression fibrinolyse
Dépôts de fibrine intra- et extravasculaires Thromboses vasculaires APC participe à la fibrinolyse a une activité anti-thrombotique a une activité anti-inflammatoire

36
Ware et al. AJP 2003 Boxplot summary of plasma protein C levels in 2 groups, 10 normal healthy controls and 45 patients with acute lung injury (ALI) or acute respiratory distress syndrome (ARDS)
 or acute respiratory distress syndrome (ARDS)")
37
Ware et al. AJP 2003 Plasma protein C levels in 45 patients with ALI or ARDS

38
Pré-traitement APC: PaO2/FiO2
Richard et al. Intensive Care Med 2007 C1, before onset of APC or placebo; C2, 110 min after onset of oleic acid injection; C3, 180 min after C2

39
Richard et al. Intensive Care Med 2007
Lung perfusion nonsignificantly tended to redistribute towards dorsal lung regions with APC Ac oléique Average ventral-to-dorsal distribution of the fractional pulmonary blood flow (PBF) afetr 180 min of injury stabilization Richard et al. Intensive Care Med 2007
 afetr 180 min of injury stabilization. Richard et al. Intensive Care Med")
40
Richard et al. Intensive Care Med 2007
Cytokines sériques Richard et al. Intensive Care Med 2007

41
Protéine C activée et ALI
24 mg/kg/h for 96 h et placebo Liu et al. AJRCCM 2008

42
Diminution de la perméabilité vasculaire
Souris VM 4h APC à 30 et 150 min 7 vs 20 ml/kg Vt FR = 160/min APC posttreatment attenuates MV-mediated increases in pulmonary vascular permeability. Mice were exposed to 4-h MV and treated with 100 g/kg APC or vehicle 30 and 150 min after initiation of ventilation. Vascular integrity was assessed using BAL protein (A) and EBD leakage (B). APC given after initiation of MV significantly attenuated increases in MV-induced vascular leak. *P HVT vs. control, LVT, and HVT APC; **P 0.05 control vs. LVT and HVT APC; n 4–6 for each group. LVT has no effect on EBD extravasation. Finigan et al. AJP 2009
 and EBD leakage (B). APC given after initiation of MV significantly attenuated increases in MV-induced vascular leak. *P 0.05 HVT vs. control, LVT, and HVT APC; **P control vs. LVT and HVT APC; n 4–6 for each group. LVT has no effect. on EBD extravasation. Finigan et al. AJP")
43
APC inhalée: meilleure aération
Waerhaug et al. Crit Care 2009 Mechanically ventilated Sheep Sham = sham-operated group (n = 8); LPS = lipopolysaccharide group (n = 8); LPS+inhAPC = LPS group treated with inhaled recombinant human activated protein C (n = 8) at FRC, the gas/tissue ratio was also higher in the LPS+inhAPC group as compared with sheep exposed to LPS alone (Figure 4; P = 0.03), but the intergroup difference was not present at end inspiration (P = 0.09).
; LPS = lipopolysaccharide group. (n = 8); LPS+inhAPC = LPS group treated with inhaled recombinant. human activated protein C (n = 8) at FRC, the gas/tissue ratio was also higher in the. LPS+inhAPC group as compared with sheep exposed to LPS. alone (Figure 4; P = 0.03), but the intergroup difference was. not present at end inspiration (P = 0.09).")
44
ALI/ARDS: altered alveolar clearance
Mortalité hospitalière en fonction de la clairance alvéolaire Ware L, Matthay M AJRCCM 2001

45
b2-mimétiques clairance alvéolaire perméabilité endothéliale
lésions épithéliales inflammation β2-adrenergic agonists have been shown to accelerate the airspace fluid clearance by increasing transepithelial sodium and chloride transport

46
b2-mimétiques HCl chez rat ventilé 4h McAuley et al. CCM 2004
Alveolar fluid clearance (AFC) following acid aspiration-induced lung injury. a, at 2 hrs after acid injury, salmeterol (n 4) did not increase AFC compared with saline-treated rats (n 4). At 4 hrs, AFC in the salmeterol group (n 3) was 2.4-fold higher than in the saline-treated rats (n 3). Excess lung water at 2 hrs after acid injury was similar in saline- (n 3) and salmeterol- tress syndrome. treated rats (n 3). By 4 hrs after acid injury, excess extravascular lung water was significantly higher in saline-treated rats (n 6) compared with salmeterol treatment (n 6).
 following acid aspiration-induced lung injury. a, at 2 hrs after acid injury, salmeterol (n 4) did not increase AFC compared with saline-treated rats (n 4). At 4 hrs, AFC in the salmeterol group (n 3) was 2.4-fold higher than in the saline-treated rats (n 3). Excess lung water at 2 hrs after acid injury was similar in saline- (n 3) and salmeterol- tress syndrome. treated rats (n 3). By 4 hrs after acid injury, excess extravascular lung water was significantly higher. in saline-treated rats (n 6) compared with salmeterol treatment (n 6).")
47
Rétrospective: 86 ALI Salbutamol inhalé 'high dose' ≥ 2.2 mg/day
'low dose' < 2.2 mg/day Manocha et al. Crit Care 2006 Days alive and free of PaO2/FiO2 < 300 Days alive and free of ALI

49
b2-mimétiques IV Etude BALTI Salbutamol IV (n=19) vs. Placebo (n=21)
Atteinte directe, 16 vs. 52% Perkins et al. AJRCCM 2005

50
Perkins et al. AJRCCM 2005

51
* Perkins et al. AJRCCM 2005 J7 Pas de variation du SOFA

53
Conclusion Traitement(s) médicamenteux du SDRA Des conséquences
Adjuvants de la ventilation mécanique Ont des effets secondaires

54
Conclusion: NMBA and ARDS
Systematic NMBA use ? Yes, but For severe ARDS (PaO2:FiO2 < 150… 120???) Early in the course of ARDS For a short duration (2 days) It is not a plea for the long-term use of NMBA It is not the plea for the delayed use of NMBA
 Early in the course of ARDS. For a short duration (2 days) It is not a plea for the long-term use of NMBA. It is not the plea for the delayed use of NMBA.")
56
Adjunctive therapies NMBA Placebo p Prone position 50 (28%) 47 (29%)
0.88 NOi 53 (33%) 0.37 Almitrine 6 (3%) 10 (6%) 0.23 At least one 75 (42%) 77 (48%) 0.34
 Almitrine. 6 (3%) 10 (6%) At least one. 75 (42%) 77 (48%)")
57
Other treatments NMBA Placebo p Vasopressors 162 (92%) 144 (89%) 0.41
Dobutamine 35 (20%) 40 (25%) 0.28 RRT 59 (33%) 59 (36%) 0.55
 40 (25%) RRT. 59 (33%) 59 (36%)")
59
NMBA use LaSRS LOVS ACURASYS ExPress

60
PaO2/FiO2 inclusion T/P PEEP inclusion T/P Mortality T/P
ARMA 2000 138±64 / 134±58 ?/? 31 / 39.8 ALVEOLI 2004 165±77 / 151±67 27.5 / 24.9 ExPress 2008 143±57 / 144±58 7.9±3.3/8.2±3.7 35.4 / 39 LOV 2008 145±48 / 145±49 11.5±3.5/11.2±3.3 30.5 / 35 ACURASYS 2009 106±36 / 115±41 9.2±3.2/9.2±3.5 31.6 / 40.7 Express SAPS II score, mean (SD) 49 (16) 50 (16)
 49 (16) 50 (16)")
61
PaO2/FiO2 inclusion T/P PEEP inclusion T/P BarotarumaT/P
ARMA 2000 138±64 / 134±58 ?/? 10 / 11 ALVEOLI 2004 165±77 / 151±67 ExPress 2008 143±57 / 144±58 7.9±3.3/8.2±3.7 7 / 6* LOV 2008 145±48 / 145±49 11.5±3.5/11.2±3.3 11.2 / 9.1 ACURASYS 2009 106±36 / 115±41 9.2±3.2/9.2±3.5 5.1 / 11.7 Express SAPS II score, mean (SD) 49 (16) 50 (16) * Only pneumothoraces
 49 (16) 50 (16) * Only pneumothoraces.")
62
PaO2/FiO2 inclusion T/P PEEP inclusion T/P VFD28 T/P
ARMA 2000 138±64 / 134±58 ?/? 12±11/10±11 ALVEOLI 2004 165±77 / 151±67 14.5±10.4/13.8±10.6 ExPress 2008 143±57 / 144±58 8±3/8±4 3 (0-17)/7 (0-19) LOV 2008 145±48 / 145±49 11±4/11±3 - ACURASYS 2009 106±36 / 115±41 9.2±3.2/9.2±3.5 10.69.7/8.59.4 Express SAPS II score, mean (SD) 49 (16) 50 (16)
/7 (0-19) LOV ±48 / 145±49. 11±4/11±3. - ACURASYS ±36 / 115± ±3.2/9.2± 9.7/8.59.4. Express SAPS II score, mean (SD) 49 (16) 50 (16)")
63
1326 Patients were assessed for eligibility
986 Were excluded 121 (12.3%) Could not contact next of kin 118 (12.0%) Did not get commitment from physician for aggressive care 97 (9.8%) Had received bone marrow transplant or chemotherapy-induced neutropenia 97 (9.8%) Organizational failure 85 (8.6%) Had chronic respiratory disease 82 (8.3%) Had chronic liver disease 57 (5.8%) Were enrolled in another trial within 30 days 54 (5.5%) Next of kin declined to give consent 50 (5.1%) Had a terminal illness 48 (4.9%) Exceeded time window 42 (4.3%) Received open-label NMBA 18 (1.8%) Had a pneumothorax prior inclusion 15 (1.5%) Had intracranial hypertension 9 (0.9%) Were pregnant 9 (0.9%) < 18 years 83 (8.4%) Had other reasons 340 Underwent randomization 178 were assigned to receive cisatracurium 1 Did not undergo infusion (withdrew consent) 162 were assigned to receive placebo 177 Were assessed 162 Were assessed
 Could not contact next of kin. 118 (12.0%) Did not get commitment from. physician for aggressive care. 97 (9.8%) Had received bone marrow transplant. or chemotherapy-induced neutropenia. 97 (9.8%) Organizational failure. 85 (8.6%) Had chronic respiratory disease. 82 (8.3%) Had chronic liver disease. 57 (5.8%) Were enrolled in another trial within 30 days. 54 (5.5%) Next of kin declined to give consent. 50 (5.1%) Had a terminal illness. 48 (4.9%) Exceeded time window. 42 (4.3%) Received open-label NMBA. 18 (1.8%) Had a pneumothorax prior inclusion. 15 (1.5%) Had intracranial hypertension. 9 (0.9%) Were pregnant. 9 (0.9%) < 18 years. 83 (8.4%) Had other reasons. 340 Underwent randomization. 178 were assigned to receive cisatracurium. 1 Did not undergo infusion (withdrew consent) 162 were assigned to receive placebo. 177 Were assessed. 162 Were assessed.")
64
Mortality d90 and plateau pressure on inclusion
< 24 ≥ 24

67
Oxygenation

68
Putensen et al. AJRCCM 2001

69
Putensen et al. AJRCCM 2001

Présentations similaires