Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Qualité des Soins Gestion des Risques Iatrogènes et Système dInformation Clinique Pascal Staccini LabSTICs, Faculté de Médecine de Nice DIIM, Centre Hospitalier Universitaire de Nice pascal.staccini@unice.fr pascal.staccini@unice.fr Séminaire de Formation aux Internes de Santé Publique - 19 Novembre 2009 - NICE

2
Plan de la présentation Source : http://qualitydigest.comhttp://qualitydigest.com 1.Problèmes et concepts 2.Professionnels et SI 3.Risk managers et SI 4.Dispositifs 5.Perspectives 6.Conclusion Problèmes

3
Evidence Based Management Faits prouvés mesurant limpact dun système dinformation clinique 1) sur lamélioration continue de la qualité des soins 2) sur la réduction de la survenue des événements indésirables Source : http://blogs.onisep.fr/http://blogs.onisep.fr Problèmes
 sur lamélioration continue de la qualité des soins 2) sur la réduction de la survenue des événements indésirables Source : Problèmes")
4
Plan de la présentation Source : http://qualitydigest.comhttp://qualitydigest.com 1.Problèmes et concepts 2.Professionnels et SI 3.Risk managers et SI 4.Dispositifs 5.Perspectives 6.Conclusion Problèmes

5
Problématiques P. Degoulet, M. Fieschi. Informatique médicale. 3ème édition, Eds Masson, 1998 Problèmes

6
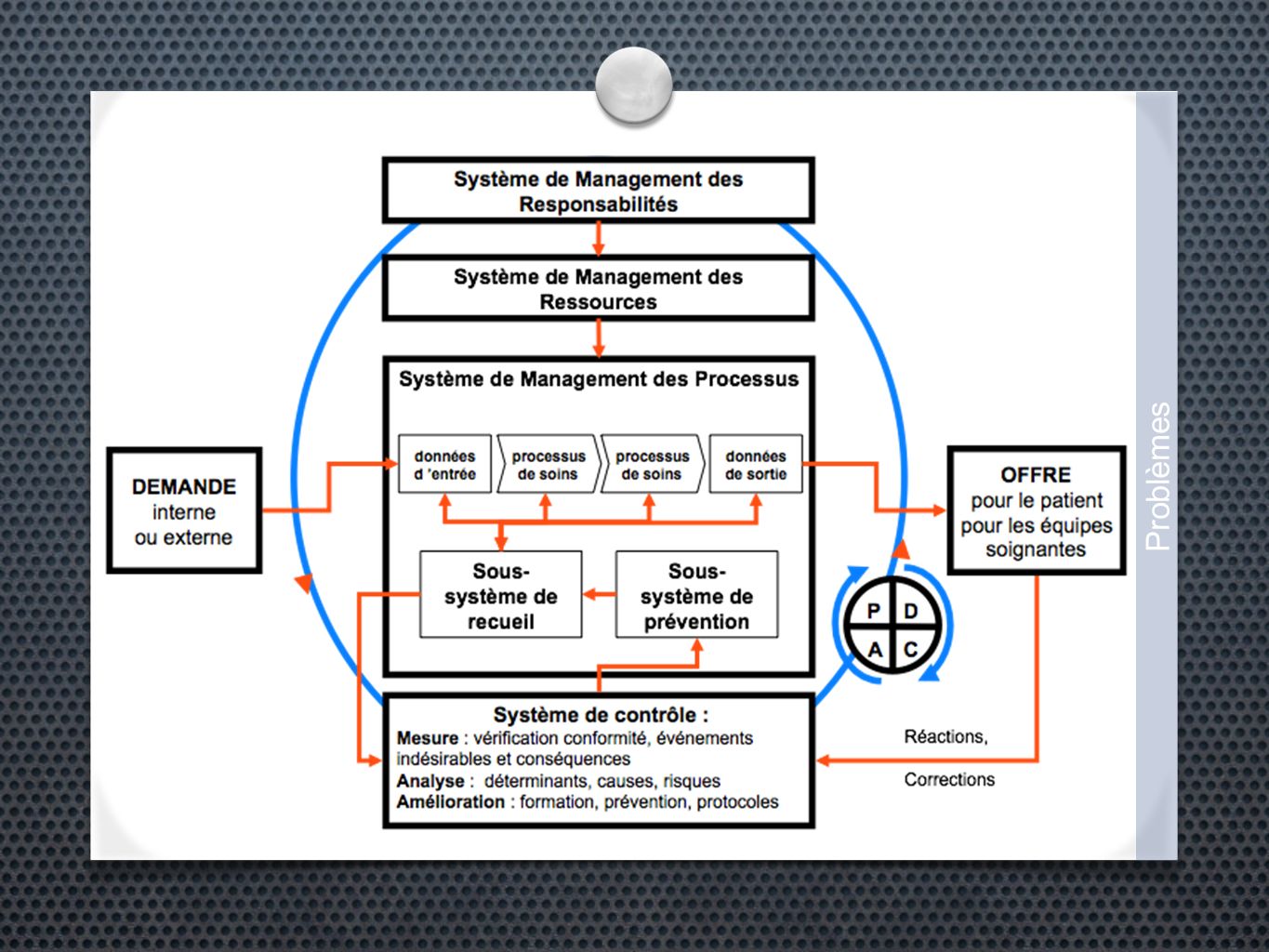
Problématiques Connaître pour mieux Soigner Gérer Risques Qualité Coût Sécurité Conformité Efficience Efficacité Effectivité Problèmes Trace Indicateur Modèle Processus

7
Problématiques Connaître pour mieux Soigner Gérer Risques Qualité Coût Sécurité Conformité Efficience Efficacité Effectivité Problèmes Trace Indicateur Processus Modèle

8
Qualité et SI Démarches amélioration continue de la qualité structurantes sur le plan stratégique, puisquelles - précisent les objectifs dévaluation - définissent les objets de la mesure structurantes sur le plan organisationnel puisquelles précisent les méthodes de travail et les actions de prévention Système dinformation support de la preuve (trace) et outil de communication et de travail collaboratif entre les acteurs support de la mesure (source de données) et des traitements Problèmes
 et outil de communication et de travail collaboratif entre les acteurs support de la mesure (source de données) et des traitements Problèmes")
9
Problématiques Impliquer les soignants Comprendre, recueillir, analyser, interpréter les besoins des utilisateurs Impliquer les «organisations» Quel lien construire entre information et activité réalisée et à réaliser ? Expression des besoins : - 1) Implicites / explicites - 2) Individuels / collectifs Problèmes
 Implicites / explicites - 2) Individuels / collectifs Problèmes.")
10
Les soignants Considérations comportementales Connaissance des bénéfices potentiels Ne pas craindre le partage et le changement de pratique Considérations méthodologiques Savoir faire correspondre modèles de travail et processus cliniques Considérations organisationnelles Prendre en compte lorganisation du travail (rôles, responsabilités) Problèmes
 Problèmes")
11
Les établissements Conformité réglementaire - Traçabilité, Sécurité - Connaissance des pratiques - Manuel de certification Capacités du système dinformation à répondre Sollicitations en temps réel - Prise en charge du patient - Adaptation au contexte Sollicitations en temps différé - Évaluation des pratiques professionnelles Problèmes

12
Qualité... à lhôpital La norme ISO 9004:2000 (SMQ et performance) définit les principes fondateurs constituant des règles et conseils destinés aux organisations (hôpital, pôles, services, PMT, logistique...) : - pour améliorer de façon continue leur performance (conformité, délais) - en se focalisant sur la satisfaction de leurs clients (bénéficiaires au sens large) (patients, familles, professionnels, tutelles) - tout en prenant en compte les besoins des différentes parties prenantes (contrats inter-pôles, EPRD, stratégie du recrutement) Problèmes
 définit les principes fondateurs constituant des règles et conseils destinés aux organisations (hôpital, pôles, services, PMT, logistique...) : - pour améliorer de façon continue leur performance (conformité, délais) - en se focalisant sur la satisfaction de leurs clients (bénéficiaires au sens large) (patients, familles, professionnels, tutelles) - tout en prenant en compte les besoins des différentes parties prenantes (contrats inter-pôles, EPRD, stratégie du recrutement) Problèmes.")
13
Point de convergence Sensibiliser les acteurs de soins Les aider à identifier, prioriser et formaliser leurs besoins en termes de données, dutilité, daccessibilité et de traitements Décrire les activités Comprendre les organisations Evaluer leur performance Problèmes Approche par processus

14
2 démarches Problèmes

15
Au final Un processus correctement réorganisé doit présenter : un temps de cycle réduit de moitié ; un traitement des tâches en parallèle chaque fois que cest possible ; des procédures distinctes en fonction de la complexité des opérations ; moins de boucles de retour dinformation ; plus aucune tâche inutile. Problèmes

16
Effets du BPR Healthcare continues to face many significant challenges in its quest to provide optimal patient care. Many hospitals have instituted various process improvement methodologies to address these challenges. The outcome of these efforts still produces a large volume of manual tasks that must be addressed by the caregiver. The Chester County Hospital employed a Business Process Management (BPM) engine to automate and manage several of these processes. A BPM engine can perform key tasks and interact with the clinician to decrease the manual requirements of a process. The result is reduced workloads and improved outcomes. The Chester County Hospital has been able to demonstrate significant decreases in hospital acquired MRSA infections and compliance with several CMS core measures. There are multiple items to evaluate before attempting to use a BPM engine. This paper reviews the work at Chester County, its outcomes and the considerations that were important for achieving success. Hess R. The missing link to success: using a business process management system to automate and manage process improvement. J Healthc Inf Manag 2009; 23(1):27-33. Problèmes
 engine to automate and manage several of these processes. A BPM engine can perform key tasks and interact with the clinician to decrease the manual requirements of a process. The result is reduced workloads and improved outcomes. The Chester County Hospital has been able to demonstrate significant decreases in hospital acquired MRSA infections and compliance with several CMS core measures. There are multiple items to evaluate before attempting to use a BPM engine. This paper reviews the work at Chester County, its outcomes and the considerations that were important for achieving success. Hess R. The missing link to success: using a business process management system to automate and manage process improvement. J Healthc Inf Manag 2009; 23(1): Problèmes.")
17
from EHR to BPR BACKGROUND: Implementation of health information technology (HIT) has encountered many difficulties and produced mixed outcomes. Yet Trinity Health, a major integrated delivery system, successfully leveraged implementation of a systemwide electronic health record (EHR) to promote process redesign and continuous quality improvement. IMPLEMENTING A SYSTEMWIDE EHR: After several years of planning, two waves of EHR implementation were launched, in 2001 and 2003. One system HIT team collaborated with each hospital team for 18 months before its 24- hour transition to the EHR. During EHR planning, the system HIT team used five principles of redesign of care processes: (1) identify and address safety problems, (2) promote evidence-based practices, (3) reduce practice variations and standardize terminologies and care processes, (4) improve communication and relationships among clinician roles, and (5) augment multiple uses of data in HIT-supported care processes. Patient-centered work flows were developed to design improved patient care processes for different types of patients, such as medical inpatients and emergency outpatients. These admission-to-discharge work flows addressed gaps in quality, safety, and efficiency and helped ensure that the EHR and decision supports reflected crucial interactions among clinicians and with the patient. By the end of 2008, 13 of Trinity Health's 17 major health care organizations ("ministries") made the transformation to using EHRs. DISCUSSION: EHR-supported care redesign requires development of substantial system capacities in clinical informatics, customization and standardization of vendor's products, collaboration and coordination between system and hospital implementation teams, quality training for clinicians and change agents, and significant clinician participation in local preparations. Brokel JMBrokel JM, Harrison MI. Redesigning care processes using an electronic health record: a system's experience. Jt Comm J Qual Patient Saf. 2009 Feb;35(2):82-92.MI. Redesig Brokel JMBrokel JM, Harrison MI. Redesigning care processes using an electronic health record: a system's experience. Jt Comm J Qual Patient Saf. 2009 Feb;35(2):82-92.MI. Redesig Problèmes
 to promote process redesign and continuous quality improvement. IMPLEMENTING A SYSTEMWIDE EHR: After several years of planning, two waves of EHR implementation were launched, in 2001 and One system HIT team collaborated with each hospital team for 18 months before its 24- hour transition to the EHR. During EHR planning, the system HIT team used five principles of redesign of care processes: (1) identify and address safety problems, (2) promote evidence-based practices, (3) reduce practice variations and standardize terminologies and care processes, (4) improve communication and relationships among clinician roles, and (5) augment multiple uses of data in HIT-supported care processes. Patient-centered work flows were developed to design improved patient care processes for different types of patients, such as medical inpatients and emergency outpatients. These admission-to-discharge work flows addressed gaps in quality, safety, and efficiency and helped ensure that the EHR and decision supports reflected crucial interactions among clinicians and with the patient. By the end of 2008, 13 of Trinity Health s 17 major health care organizations ( ministries ) made the transformation to using EHRs. DISCUSSION: EHR-supported care redesign requires development of substantial system capacities in clinical informatics, customization and standardization of vendor s products, collaboration and coordination between system and hospital implementation teams, quality training for clinicians and change agents, and significant clinician participation in local preparations. Brokel JMBrokel JM, Harrison MI. Redesigning care processes using an electronic health record: a system s experience. Jt Comm J Qual Patient Saf Feb;35(2):82-92.MI. Redesig Brokel JMBrokel JM, Harrison MI. Redesigning care processes using an electronic health record: a system s experience. Jt Comm J Qual Patient Saf Feb;35(2):82-92.MI. Redesig Problèmes.")
19
De lerreur au risque « Lerreur est de toute façon inéluctable … il faut tirer les bonnes leçons des accidents du passé » (Reason, 1990) « Maîtriser le risque, cest éviter laccident et quand laccident survient, en minimiser les conséquences » (JJ Duby, 1996) Conséquences pratiques en termes de recueil et de traitement dinformations : concept de «médicovigilance» - comment prévenir et éviter la survenue derreurs ? - comment identifier et récupérer les erreurs ? - comment rechercher les défaillances latentes ? Reason J. The contribution of latent human failures to the breakdown of complex systems. Philos Trans R Soc Lond B Biol Sci. 1990 Apr 12;327(1241):475-84. The contribution of latent human failures to the breakdown of complex systems. Duby JJ. Cindynique de la vache folle. Institut Européen de Cindyniques, Lettre n°19, Juin 1996. Reason J. The contribution of latent human failures to the breakdown of complex systems. Philos Trans R Soc Lond B Biol Sci. 1990 Apr 12;327(1241):475-84. The contribution of latent human failures to the breakdown of complex systems. Duby JJ. Cindynique de la vache folle. Institut Européen de Cindyniques, Lettre n°19, Juin 1996. Problèmes
: The contribution of latent human failures to the breakdown of complex systems. Duby JJ. Cindynique de la vache folle. Institut Européen de Cindyniques, Lettre n°19, Juin Reason J. The contribution of latent human failures to the breakdown of complex systems. Philos Trans R Soc Lond B Biol Sci Apr 12;327(1241): The contribution of latent human failures to the breakdown of complex systems. Duby JJ. Cindynique de la vache folle. Institut Européen de Cindyniques, Lettre n°19, Juin Problèmes.")
20
Prévenir les erreurs réduction du recours à la mémoire de court terme : aides-mémoire, listes de contrôle, informatisation des tâches répétitives utilisation de détrompeurs : « watch-dogs » qui guident les opérateurs et ne leur permettent pas d effectuer une action sans que les conditions de sécurité de base soient effectives amélioration de laccès à linformation pour optimiser la prise de décision Problèmes

21
Prévenir les erreurs standardisation de lactivité sur la base de processus évalués comme les plus fiables : lexistence de règles claires et connues des opérateurs est de première importance dans un contexte de surcharge de travail pédagogie de la sécurité : expliquer le pourquoi de la rationalité des procédures et analyser les facteurs facilitant la compliance aux procédures et à la déclaration dincident Problèmes

22
Identifier et décrire sorganiser pour identifier/détecter les erreurs, les décrire - pour les corriger et ainsi éviter les accidents ou en réduire limpact organiser le feed-back vers les déclarants - immédiat, contextualisé - différé, spécifique, agrégé Problèmes

23
Défaillances latentes Recherche des défaillances latentes par la constitution dune base dincidents (base de connaissance) décrivant : - domaine dactivité, processus clinique en cause... - identification et description de lévénement, - contexte de survenue, - gravité, conséquences, - analyse de la causalité, - actions mises en place, - impact des actions Recherche de profils par la fouille de données et/ou lapplication dalgorithmes de proximité Problèmes

24
Situation duale Le Système dInformation Contribution : actions de correction ou damélioration intégré aux processus de soins : prévention, aide à la décision Support dun dispositif de gestion des risques identification, analyse, traitement, évaluation (modèle HAS*) (*)Principes méthodologiques pour la gestion des risques en établissement de santé. ANAES 2003 Problèmes

25
Plan de la présentation 1. Problèmes et concepts 2. Professionnels et SI 3. Risk managers et SI 4. Dispositifs 5. Perspectives 6. Conclusion Source : http://trustedadvisor.comhttp://trustedadvisor.com Professionnels

26
Health Evaluation through Logical Processing Professionnels

27
HELP DATA wich comes from measurements, becoming INFORMATION by transformation, becoming INTEGRATION by combining and finally DECISION SUPPORT by adding inference. Alertes cliniques si valeurs biologiques anormales Evaluations des interactions : - médicament/médicament ; - médicament/biologie ; - médicament/allergies Professionnels

28
Aide à la décision Lepage EF, Gardner RM, Laub RM, Jacobson JT. Assessing the effectiveness of a computerized blood order "consultation" system. Proc Annu Symp Comput Appl Med Care. 1991:33-7. Professionnels

29
Aide à la décision Gardner RM, Golubjatnikov OK, Laub RM, Jacobson JT, Evans RS. Computer-critiqued blood ordering using the HELP system. Comput Biomed Res. 1990 Dec;23(6):514-28. Each order is justified at the time it is entered by selecting from a menu of physician-approved criteria. The criteria are linked to supportive data in the data base, i.e., laboratory results and clinical data. The computer verified that 82% of these orders met criteria. Quality Assurance nurses verified the remaining 18%. Of these 18% only one in eight required manual chart review. After computer and Quality Assurance review, only eight (0.24%) of the orders were found to be true exceptions to established criteria. Physicians and nurses have accepted the computerized critiquing system. Professionnels
: Each order is justified at the time it is entered by selecting from a menu of physician-approved criteria. The criteria are linked to supportive data in the data base, i.e., laboratory results and clinical data. The computer verified that 82% of these orders met criteria. Quality Assurance nurses verified the remaining 18%. Of these 18% only one in eight required manual chart review. After computer and Quality Assurance review, only eight (0.24%) of the orders were found to be true exceptions to established criteria. Physicians and nurses have accepted the computerized critiquing system. Professionnels.")
30
Aide à la décision Fernández Pérez ER, Winters JL, Gajic O. The addition of decision support into computerized physician order entry reduces red blood cell transfusion resource utilization in the intensive care unit. Am J Hematol. 2007 Jul;82(7):631-3. From the institutional APACHE III database we identified 2,200 patients with anemia, but no active bleeding on admission: 1,100 during a year before and 1,100 during a year after the intervention. The mean number of RBC transfusions per patient decreased from 1.5 +/- 1.9 units to 1.3 +/- 1.8 units after the intervention (P = 0.045). RBC transfusion cost decreased from $616,442 to $556,226 after the intervention. Hospital length of stay and adjusted hospital mortality did not differ before and after protocol implementation. Conclusion: the implementation of an evidenced-based decision support system through a CPOE can decrease RBC transfusion resource utilization in critically ill patients. Professionnels
: From the institutional APACHE III database we identified 2,200 patients with anemia, but no active bleeding on admission: 1,100 during a year before and 1,100 during a year after the intervention. The mean number of RBC transfusions per patient decreased from 1.5 +/- 1.9 units to 1.3 +/- 1.8 units after the intervention (P = 0.045). RBC transfusion cost decreased from $616,442 to $556,226 after the intervention. Hospital length of stay and adjusted hospital mortality did not differ before and after protocol implementation. Conclusion: the implementation of an evidenced-based decision support system through a CPOE can decrease RBC transfusion resource utilization in critically ill patients. Professionnels.")
31
Adverse Drug Events Leape LL, Bates DW, Culien DJ, et al. Systems Analysis of Adverse Drug Events. JAMA 1995;274(1):35-43 Professionnels
:35-43 Professionnels.")
32
Adverse Drug Events REEM : Réseau Epidémiologique de lErreur Médicamenteuse Berhneim C, Schmitt E, Dufay E. Iatrogénie médicamenteuse nosocomiale et gestion des risques derreur médicamenteuse : à propos de lanalyse des notifications du réseau REEM. Oncologie 2005;7:104-119 Professionnels

33
Adverse Drug Events Agrawal A. Medication Errors: Prevention Using Information Technology Systems. Br J Clin Pharmacol 2009;67(6):681- 6 Professionnels
: Professionnels.")
34
Limites Koppel R, Metlay JP, Cohen A. Role of Computerized Order Entry System in Facilitating Medication Errors. JAMA 2005;293(10):1197-1203 Professionnels
: Professionnels.")
35
Limites Henneman PL, Fisher DL, Henneman EA, Pham TA, Mei YY, Talati R, Nathanson BH, Roche J. Providers do not verify patient identity during computer order entry. Acad Emerg Med. 2008 Jul;15(7):641-8 This was a prospective study using simulated scenarios with an eye-tracking device. Medical providers were asked to review 10 charts (scenarios), select the patient from a computer alphabetical list, and order tests. Two scenarios had embedded ID errors compared to the computer (incorrect DOB or misspelled last name), and a third had a potential error (second patient on alphabetical list with same last name). Providers were not aware the focus was patient ID. (...) Two of 25 (8%; 95% CI = 1% to 26%) noted the DOB error; the remaining 23 ordered tests on an incorrect patient. One of 25 (4%, 95% CI = 0% to 20%) noted the last name error; 12 ordered tests on an incorrect patient. Professionnels
:641-8 This was a prospective study using simulated scenarios with an eye-tracking device. Medical providers were asked to review 10 charts (scenarios), select the patient from a computer alphabetical list, and order tests. Two scenarios had embedded ID errors compared to the computer (incorrect DOB or misspelled last name), and a third had a potential error (second patient on alphabetical list with same last name). Providers were not aware the focus was patient ID. (...) Two of 25 (8%; 95% CI = 1% to 26%) noted the DOB error; the remaining 23 ordered tests on an incorrect patient. One of 25 (4%, 95% CI = 0% to 20%) noted the last name error; 12 ordered tests on an incorrect patient. Professionnels.")
36
Limites Bedouch P, Allenet B, Grass A, Labarère J, Brudieu E, Bosson JL, Calop J. Drug-related problems in medical wards with a computerized physician order entry system. J Clin Pharm Ther. 2009 Apr;34(2):187-95. Bedouch PAllenet BGrass ALabarère JBrudieu EBosson JLCalop Results: A total of 29 016 medication orders relating to 8152 patients were analysed, and 2669 DRPs, involving 1564 patients (56% female; mean age 72±6 years), were identified representing 33 DRPs per 100 admissions. The most commonly identified DRPs were non-conformity to guidelines or contra- indication (29.5%), improper administration (19.6%), drug interaction (16.7%) and overdosage (12.8%). Conclusions: Drug-related problems are common even after implementation of CPOE. In this context, routine participation of clinical pharmacists in clinical medical rounds may facilitate identification of DRPs. Pharmacists should be able to enhance patient safety through such involvement. Professionnels
: Bedouch PAllenet BGrass ALabarère JBrudieu EBosson JLCalop Results: A total of medication orders relating to 8152 patients were analysed, and 2669 DRPs, involving 1564 patients (56% female; mean age 72±6 years), were identified representing 33 DRPs per 100 admissions. The most commonly identified DRPs were non-conformity to guidelines or contra- indication (29.5%), improper administration (19.6%), drug interaction (16.7%) and overdosage (12.8%). Conclusions: Drug-related problems are common even after implementation of CPOE. In this context, routine participation of clinical pharmacists in clinical medical rounds may facilitate identification of DRPs. Pharmacists should be able to enhance patient safety through such involvement. Professionnels.")
37
Singh H, Mani S, Espadas D, Petersen N, Franklin V, Petersen LA. Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Arch Intern Med. 2009 May 25;169(10):982-9.Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Singh H, Mani S, Espadas D, Petersen N, Franklin V, Petersen LA. Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Arch Intern Med. 2009 May 25;169(10):982-9.Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Professionnels
:982-9.Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Singh H, Mani S, Espadas D, Petersen N, Franklin V, Petersen LA. Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Arch Intern Med May 25;169(10):982-9.Prescription errors and outcomes related to inconsistent information transmitted through computerized order entry: a prospective study. Professionnels.")
38
Limites Garg AX, Adhikari NK, McDonald H et al. Effets on Computerized Clinical Decision Support Systems on Practitioner Performance and Patient Outcomes: A Systematic Review. JAMA 2005;293(10):1223-1238 Professionnels
: Professionnels.")
39
Limites Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007 Feb 28;297(8):831-41. Review.Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. Professionnels
: Review.Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. Professionnels.")
40
Education and CPOE Rothschild JM, McGurk S, Honour M, Lu L, McClendon AA, Srivastava P, Churchill WH, Kaufman RM, Avorn J, Cook EF, Bates DW. Assessment of education and computerized decision support interventions for improving transfusion practice. Transfusion. 2007 Feb;47(2):228-39. Education and computerized DS both decreased the percentage of inappropriate transfusions, although the residual amount of inappropriate transfusions remained high. Professionnels
: Education and computerized DS both decreased the percentage of inappropriate transfusions, although the residual amount of inappropriate transfusions remained high. Professionnels.")
41
Failure analysis and CPOE Kim GR, Chen AR, Arceci RJ, Mitchell SH, Kokoszka KM, Daniel D, Lehmann CU. Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Arch Pediatr Adolesc Med. 2006 May;160(5):495-8.Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Kim GR, Chen AR, Arceci RJ, Mitchell SH, Kokoszka KM, Daniel D, Lehmann CU. Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Arch Pediatr Adolesc Med. 2006 May;160(5):495-8.Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Professionnels
:495-8.Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Kim GR, Chen AR, Arceci RJ, Mitchell SH, Kokoszka KM, Daniel D, Lehmann CU. Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Arch Pediatr Adolesc Med May;160(5):495-8.Error reduction in pediatric chemotherapy: computerized order entry and failure modes and effects analysis. Professionnels.")
42
Process redesign and CPOE Schnipper JLSchnipper JL, Hamann C, Ndumele CD, Liang CL, Carty MG, Karson AS, Bhan I, Coley CM, Poon E, Turchin A, Labonville SA, Diedrichsen EK, Lipsitz S, Broverman CA, McCarthy P, Gandhi TK. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009 Apr 27;169(8):771-80.umele CD, Carty MG Bhan I, Poon E,, Labonvidrichsipsitz Sn CA, P, Gandht of an electn reconciliatind proceson potentialevents: a omized tr Schnipper JLSchnipper JL, Hamann C, Ndumele CD, Liang CL, Carty MG, Karson AS, Bhan I, Coley CM, Poon E, Turchin A, Labonville SA, Diedrichsen EK, Lipsitz S, Broverman CA, McCarthy P, Gandhi TK. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med. 2009 Apr 27;169(8):771-80.umele CD, Carty MG Bhan I, Poon E,, Labonvidrichsipsitz Sn CA, P, Gandht of an electn reconciliatind proceson potentialevents: a omized tr Professionnels
: umele CD, Carty MG Bhan I, Poon E,, Labonvidrichsipsitz Sn CA, P, Gandht of an electn reconciliatind proceson potentialevents: a omized tr Schnipper JLSchnipper JL, Hamann C, Ndumele CD, Liang CL, Carty MG, Karson AS, Bhan I, Coley CM, Poon E, Turchin A, Labonville SA, Diedrichsen EK, Lipsitz S, Broverman CA, McCarthy P, Gandhi TK. Effect of an electronic medication reconciliation application and process redesign on potential adverse drug events: a cluster-randomized trial. Arch Intern Med Apr 27;169(8): umele CD, Carty MG Bhan I, Poon E,, Labonvidrichsipsitz Sn CA, P, Gandht of an electn reconciliatind proceson potentialevents: a omized tr Professionnels.")
43
Plan de la présentation 1. Problèmes et concepts 2. Professionnels et SI 3. Risk managers et SI 4. Dispositifs 5. Perspectives 6. Conclusion Source : http://carpefactum.typepad.comhttp://carpefactum.typepad.com Risks manager

44
Identification Evans RS, Pestotnik SL, Classen DC, Bass SB, Menlove RL, Gardner RM, Burke JP. Development of a computerized adverse drug event monitor. Proc Annu Symp Comput Appl Med Care. 1991:23-7. The computerized system identified 401 ADEs during the first year of use compared to 9 by voluntary reporting methods during the previous year (p less than 0.001) Risks manager
 Risks manager.")
45
Identification Evans RS, Burke JP, Classen DC, Gardner RM, Menlove RL, Goodrich KM, Stevens LE, Pestotnik SL. Computerized identification of patients at high risk for hospital- acquired infection. Am J Infect Control. 1992 Feb;20(1):4-10. Recently, we used the HELP system to employ statistical methods to automatically identify high-risk patients. Patient data from more than 6000 patients were used to develop a high-risk equation. Stepwise logistic regression identified 10 risk factors for nosocomial infection. The HELP system now uses this logistic-regression equation to monitor and determine the risk status for all hospitalized patients each day. The computer notifies infection control practitioners each morning of patients who are newly classified as being at high risk. Of 605 hospital-acquired infections during a 6-month period, 472 (78%) occurred in high-risk patients, and 380 (63%) were predicted before the onset of infection. Computerized regression equations to identify patients at risk of having hospital-acquired infections can help focus prevention efforts. Risks manager
:4-10. Recently, we used the HELP system to employ statistical methods to automatically identify high-risk patients. Patient data from more than 6000 patients were used to develop a high-risk equation. Stepwise logistic regression identified 10 risk factors for nosocomial infection. The HELP system now uses this logistic-regression equation to monitor and determine the risk status for all hospitalized patients each day. The computer notifies infection control practitioners each morning of patients who are newly classified as being at high risk. Of 605 hospital-acquired infections during a 6-month period, 472 (78%) occurred in high-risk patients, and 380 (63%) were predicted before the onset of infection. Computerized regression equations to identify patients at risk of having hospital-acquired infections can help focus prevention efforts. Risks manager.")
46
Identification Classen DC, Pestotnik SL, Evans RS, Burke JP, Battles JB. Computerized surveillance of adverse drug events in hospital patients. Qual. Saf. Health Care 2005;14:221-6. Results: Over 18 months we monitored 36 653 hospitalized patients. There were 731 verified ADEs identified in 648 patients, 701 ADEs were characterized as moderate or severe, and 664 were classified as type A reactions. During this same period only nine ADEs were identified using traditional detection methods. Physicians, pharmacists, and nurses voluntarily reported 92 of the 731 ADEs detected using this automated system. (...) The most common drug classes involved were analgesics, anti-infectives, and cardiovascular agents. Conclusion: We believe that screening for ADEs with a computerized hospital information system offers a potential method for improving the detection and characterization of these events in hospital patients. Risks manager
 The most common drug classes involved were analgesics, anti-infectives, and cardiovascular agents. Conclusion: We believe that screening for ADEs with a computerized hospital information system offers a potential method for improving the detection and characterization of these events in hospital patients. Risks manager.")
47
Identification Bedouch P, Allenet B, Grass A, Labarère J, Brudieu E, Bosson JL, Calop J. Drug-related problems in medical wards with a computerized physician order entry system. J Clin Pharm Ther. 2009 Apr;34(2):187-95. Bedouch PAllenet BGrass ALabarère JBrudieu EBosson JLCalop Results: A total of 29 016 medication orders relating to 8152 patients were analysed, and 2669 DRPs, involving 1564 patients (56% female; mean age 72±6 years), were identified representing 33 DRPs per 100 admissions. The most commonly identified DRPs were non-conformity to guidelines or contra- indication (29.5%), improper administration (19.6%), drug interaction (16.7%) and overdosage (12.8%). Conclusions: Drug-related problems are common even after implementation of CPOE. In this context, routine participation of clinical pharmacists in clinical medical rounds may facilitate identification of DRPs. Pharmacists should be able to enhance patient safety through such involvement. Risks manager
: Bedouch PAllenet BGrass ALabarère JBrudieu EBosson JLCalop Results: A total of medication orders relating to 8152 patients were analysed, and 2669 DRPs, involving 1564 patients (56% female; mean age 72±6 years), were identified representing 33 DRPs per 100 admissions. The most commonly identified DRPs were non-conformity to guidelines or contra- indication (29.5%), improper administration (19.6%), drug interaction (16.7%) and overdosage (12.8%). Conclusions: Drug-related problems are common even after implementation of CPOE. In this context, routine participation of clinical pharmacists in clinical medical rounds may facilitate identification of DRPs. Pharmacists should be able to enhance patient safety through such involvement. Risks manager.")
48
Identification Bilimoria KY, Kmiecik TE, DaRosa DA, Halverson A, Eskandari MK, Bell RH Jr, Soper NJ, Wayne JD. Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Arch Surg. 2009 Apr;144(4):305-11Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Bilimoria KY, Kmiecik TE, DaRosa DA, Halverson A, Eskandari MK, Bell RH Jr, Soper NJ, Wayne JD. Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Arch Surg. 2009 Apr;144(4):305-11Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Risks manager
:305-11Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Bilimoria KY, Kmiecik TE, DaRosa DA, Halverson A, Eskandari MK, Bell RH Jr, Soper NJ, Wayne JD. Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Arch Surg Apr;144(4):305-11Development of an online morbidity, mortality, and near-miss reporting system to identify patterns of adverse events in surgical patients. Risks manager.")
49
Feedback Evans SM, Berry JG, Smith BJ, Esterman A, Selin P, OShaughnessy J, DeWit M. Attitudes and barriers to incident reporting: a collaborative hospital study. Qual. Saf. Health Care 2006;15:39-43 Risks manager

50
Feedback Benn J, Koutantji M, Wallace L, Spurgeon P, Rejman M, Healey A, Vincent C. Feedback from incident reporting: information and action to improve patient safety. Qual Saf Health Care. 2009 Feb;18(1):11-21Feedback from incident reporting: information and action to improve patient safety. Benn J, Koutantji M, Wallace L, Spurgeon P, Rejman M, Healey A, Vincent C. Feedback from incident reporting: information and action to improve patient safety. Qual Saf Health Care. 2009 Feb;18(1):11-21Feedback from incident reporting: information and action to improve patient safety. Risks manager
:11-21Feedback from incident reporting: information and action to improve patient safety. Benn J, Koutantji M, Wallace L, Spurgeon P, Rejman M, Healey A, Vincent C. Feedback from incident reporting: information and action to improve patient safety. Qual Saf Health Care Feb;18(1):11-21Feedback from incident reporting: information and action to improve patient safety. Risks manager.")
51
Plan de la présentation 1. Problèmes et concepts 2. Professionnels et SI 3. Risk managers et SI 4. Dispositifs 5. Perspectives 6. Conclusion Source : http://traitportrait.blogspot.com/2008/11/carte-didentit-prime.htmlhttp://traitportrait.blogspot.com/2008/11/carte-didentit-prime.html Dispositifs

52
Haug PJ, Rocha BH, Evans RS. Decision support in medicine: lessons from the HELP system. Int J Med Inform. 2003 Mar;69(2-3):273-84. Dispositifs
: Dispositifs.")
53
Runciman WB, Williamson JAH, Deakin A, Benveniste KA, Bannon K, Hibbert PD. An integrated framework for safety, quality and risk management: an information and incident management system based on a universal patient safety classification. Qual. Saf. Health Care 2005;15:i82-i90 Dispositifs

54
Permettre le signalement de tout type dévénement indésirable Améliorer la mise en œuvre de mesures correctives immédiates Optimiser la circulation de linformation dalerte Effectuer lanalyse de événements indésirables Permettre une interrogation décentralisée de la base de données Optimiser la communication entre acteurs de soins Optimiser la gestion documentaire Optimiser lauto-évaluation des professionnels Mettre à disposition en externe les protocoles de pratique Donner une information « grand public »

55
Dispositifs

56
Identitovigilance Annuaire identités Algorithmes de détection Workflow des suspicions Correction documentée en temps différé Correction en temps réel Base de connaissance Actions ciblées Dispositifs

57
Fusion des dossiers Dispositifs

58
Pharmacovigilance Constitution dune base de connaissance locale non seulement sur lévénement mais surtout sur la réponse fournie, généralement basée sur lhistorique local (réponse quasi-immédiate) sur une recherche bibliographique (nouvelle ou dactualisation) sur les conclusions du staff de réponse Dispositifs
 sur une recherche bibliographique (nouvelle ou dactualisation) sur les conclusions du staff de réponse Dispositifs")
59
Marquage a minima sous forme de codes diagnostics au sein des RUM du PMSI imprécision des codes, certes, MAIS lidée est didentifier des types de séjours à risque pour les surveiller en leur appliquant les principes de la MSP Dispositifs

60
Plan de la présentation 1. Problèmes et concepts 2. Professionnels et SI 3. Risk managers et SI 4. Dispositifs 5. Perspectives 6. Conclusion Source : http://noticebored.comhttp://noticebored.com Perspectives

61
CPOE with DS Evans RS, Pestotnik SL, Classen DC, Clemmer TP, Weaver LK, Orme JF Jr, Lloyd JF, Burke JP. A Computer-assisted Management Program for Antibiotics and Other Antiinfective Agents. N Engl J Med. 1998 Jan 22;338(4):232-8 Perspectives
:232-8 Perspectives.")
62
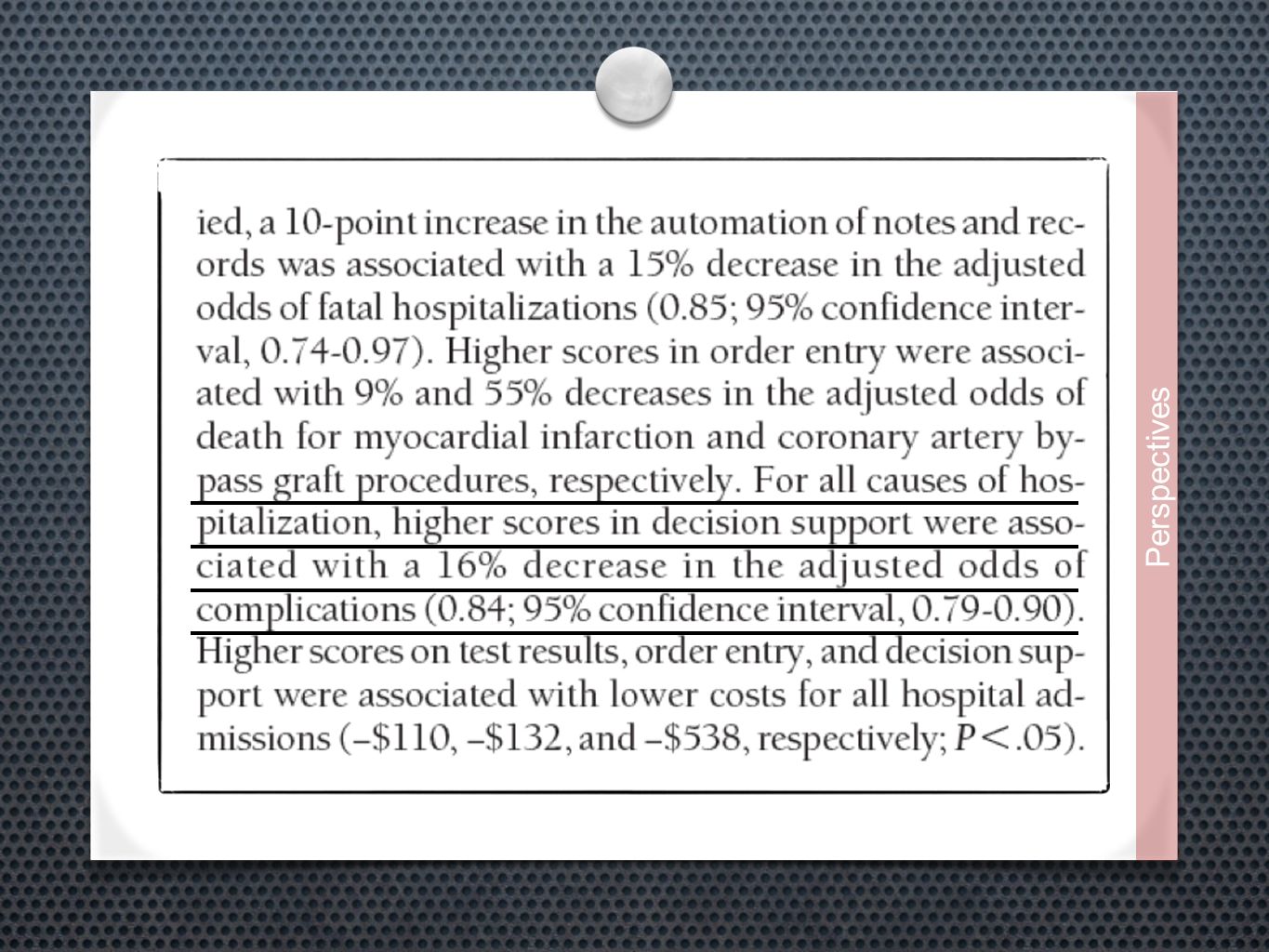
Evaluation Amarasingham R, Plantinga L, Diener-West M, Gaskin DJ, Rowe NR. Clinical Information Technologies and Inpatient Outcomes. A Multiple Hospital Study. Arch Intern Med 2009;169(2):108-114 Pédagogie
: Pédagogie.")
63
Perspectives

65
Lindenauer PK, Ling D, Pekow PS, Crawford A, Naglieri- Prescod D, Hoople N, Fitzgerald J, Benjamin EM. Physician characteristics, attitudes, and use of computerized order entry. J Hosp Med. 2006 Jul;1(4):221- 30. Physician characteristics, attitudes, and use of computerized order entry. Lindenauer PK, Ling D, Pekow PS, Crawford A, Naglieri- Prescod D, Hoople N, Fitzgerald J, Benjamin EM. Physician characteristics, attitudes, and use of computerized order entry. J Hosp Med. 2006 Jul;1(4):221- 30. Physician characteristics, attitudes, and use of computerized order entry. Perspectives
: Physician characteristics, attitudes, and use of computerized order entry. Lindenauer PK, Ling D, Pekow PS, Crawford A, Naglieri- Prescod D, Hoople N, Fitzgerald J, Benjamin EM. Physician characteristics, attitudes, and use of computerized order entry. J Hosp Med Jul;1(4): Physician characteristics, attitudes, and use of computerized order entry. Perspectives.")
66
van Wyk JT, van Wijk MA, Sturkenboom MC, et al. Electronic alerts versus on- demand decision support to improve dyslipidemia treatment: a cluster randomized controlled trial. Circulation 2008;117:371-8. 38 pratiques, 77 MG hollandais, 87 886 patients Perspectives

67
Shojania KG, Levinson W. Clinicians in quality improvement: a new career pathway in academic medicine. JAMA. 2009 Feb 18;301(7):766-8.Clinicians in quality improvement: a new career pathway in academic medicine. Shojania KG, Levinson W. Clinicians in quality improvement: a new career pathway in academic medicine. JAMA. 2009 Feb 18;301(7):766-8.Clinicians in quality improvement: a new career pathway in academic medicine. Perspectives
:766-8.Clinicians in quality improvement: a new career pathway in academic medicine. Shojania KG, Levinson W. Clinicians in quality improvement: a new career pathway in academic medicine. JAMA Feb 18;301(7):766-8.Clinicians in quality improvement: a new career pathway in academic medicine. Perspectives.")
68
Plan de la présentation 1. Problèmes et concepts 2. Professionnels et SI 3. Risk managers et SI 4. Dispositifs 5. Perspectives 6. Conclusion Source : http://www.efficience-ergonomie.com Conclusion

69
Evidence-based management is not widely used by health care managers for the following reasons: First, the business case for return on investment has not yet been reliably made. Second, widespread use would shift power away from senior toward junior managers. Third, hospital boards do not regularly review the quality of the managerial decision-making process. Richard dAquila, Daid Fine. The Practice of Evidence-Based Management. Health Administration Press, 2008 Conclusion

71
La qualité cest lévaluation de latteinte dobjectifs Dans le domaine de la qualité comme ailleurs, cest lanalyse des organisations qui prime Les technologies ne sont rien sans les usages Analyser la plus-value dune technologie cest dabord évaluer la performance dune organisation (risques) Les preuves existent : les comportements doivent évoluer et les décisions doivent être évaluées ; cest là que résident encore les difficultés Conclusion
 Les preuves existent : les comportements doivent évoluer et les décisions doivent être évaluées ; cest là que résident encore les difficultés Conclusion")
72
Qualité, Gestion des Risques et Systèmes d'Information Hospitaliers Conclusion

Présentations similaires





 in the Business.>")













