Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Cinétique de croissance des tumeurs
Une tumeur de 1cm de diamètre contient de 109~ 1010 cellules (30 temps de doublement) Peut être cliniquement silencieuse dans une masse tissulaire (masse abdominale ou thoracique) Les 10 temps de doublement suivants amènent la tumeur à une masse de 1kg (1012 cellules)
 Peut être cliniquement silencieuse dans une masse tissulaire (masse abdominale ou thoracique) Les 10 temps de doublement suivants amènent la tumeur à une masse de 1kg (1012 cellules)")
2
Cinétique de croissance tumorale:
une fois détectable la tumeur croit rapidement

3
Thérapeutique Les buts des traitements anticancéreux:
curatifs (adjuvant, néoadjuvant, métastatique) maintient de la qualité et de la durée de vie soulagement des symptômes (traitement palliatif) essais cliniques de nouveaux traitements A discuter avec le patient et sa famille
 maintient de la qualité et de la durée de vie. soulagement des symptômes (traitement palliatif) essais cliniques de nouveaux traitements. A discuter avec le patient et sa famille.")
4
Evaluation de la réponse thérapeutique individuelle 1
Evaluation de la réponse thérapeutique individuelle 1. Réponse complète (CR): disparition complète de toutes les manifestations tumorales 2. Réponse partielle (PR) . Diminution >50% de la taille tumorale sans progression d’autre localisation ni nouvelle tumeur 3. Maladie stable: pas d’augmentation de la masse tumorale ou diminution < 25% 4. Progression- Augmentation de la masse tumorale >25%, nouvelles lésions ou décès lié à la maladie
: disparition complète de toutes les manifestations tumorales 2. Réponse partielle (PR) . Diminution >50% de la taille tumorale sans progression d’autre localisation ni nouvelle tumeur 3. Maladie stable: pas d’augmentation de la masse tumorale ou diminution < 25% 4. Progression- Augmentation de la masse tumorale >25%, nouvelles lésions ou décès lié à la maladie.")
5
Efficacité globale du traitement dans des groupes de patients
• Durée de survie –semaines mois années • Taux de réponse (% de CR+PR) • Durée de réponse jusqu’à la progression • Toxicités- grading du NCI • Qualité de vie- requis par la FDA pour toutes les nouvelles molécules
 • Durée de réponse jusqu’à la progression • Toxicités- grading du NCI • Qualité de vie- requis par la FDA pour toutes les nouvelles molécules.")
6
Vinblastin-Vincristin Actinomycin D L-PAM AraC MOPP Bleomycin
1945 1950 1960 1970 1980 1990 2000 Nitrogen mustard Mercaptopurine Methotrexate Busulfan Cyclophosphamide Chlorambucil 5Fluoruracil Vinblastin-Vincristin Actinomycin D L-PAM AraC MOPP Bleomycin Doxorubicin DTIC-CCNU Cis Platin VP16 Mitoxantrone Taxol-Taxotere Oxaliplatine- G-CSF- Erythropoiétine Herceptin-Rituximab Glivec Gefitinib- crizotinib- Vemurafenib Premières rémissions complètes en hématologie Rechutes et résistance Associations médicamenteuses Multi- drug- resistance (MDR) Oncogenes- facteurs de croissance et récepteurs Anticorps monoclonaux P glycoprotéine et efflux des médicaments Antioncogènes Cycle cellulaire et signalisation Facteurs de croissance hématopoiétiques (HuR) Génétique des tumeurs familiales Ciblage thérapeutique
 Oncogenes- facteurs de croissance et récepteurs. Anticorps monoclonaux. P glycoprotéine et efflux des médicaments. Antioncogènes. Cycle cellulaire et signalisation. Facteurs de croissance hématopoiétiques (HuR) Génétique des tumeurs familiales. Ciblage thérapeutique.")
7
Complexité du ciblage thérapeutique des cancers
D’après Hanahan and Weinberg – Cell 2000 Invasion tissulaire et métastase Potentiel réplicatif illimité Angiogenèse active Insensibilité aux régulateurs négatifs Autosuffisance des signaux de croissance Résistance à l’apoptose

8
LOG kill hypothesis The example shows the effects of tumor burden, scheduling, initiation/duration of treatment on patient survival. The tumor burden in an untreated patient would progress along the path described by the RED LINE – The tumor is detected (using conventional techniques) when the tumor burden reaches 109 cells The patient is symptomatic at cells Dies at 1012 cells. DARK BLUE LINE: Infrequent scheduling of treatment courses with low (1 log kill) dosing and a late start prolongs survival but does not cure the patient (i.e., kill rate < growth rate) LIGHT BLUE LINE: More intensive and frequent treatment, with adequate (2 log kill) dosing and an earlier start is successful (i.e., kill rate > growth rate) GREEN LINE: Early surgical removal of the primary tumour decreases the tumour burden. Chemotherapy will remove persistant secondary tumours, and the total duration of therapy does not have to be as long as when chemotherapy alone is used.
 when the tumor burden reaches 109 cells. The patient is symptomatic at cells. Dies at 1012 cells. DARK BLUE LINE: Infrequent scheduling of treatment courses with low (1 log kill) dosing and a late start prolongs survival but does not cure the patient (i.e., kill rate < growth rate) LIGHT BLUE LINE: More intensive and frequent treatment, with adequate (2 log kill) dosing and an earlier start is successful (i.e., kill rate > growth rate) GREEN LINE: Early surgical removal of the primary tumour decreases the tumour burden. Chemotherapy will remove persistant secondary tumours, and the total duration of therapy does not have to be as long as when chemotherapy alone is used.")
9
Dommages cellulaires provoqués par la chimithérapie cytotoxique
1- blocage de la synthèse des précurseurs de l’ADN 2- Interaction directe avec l’ADN 3- Inhibition de la synthèse de l’ADN 4- Interférence avec la transcription 5- Inhibition de la synthèse des protéines 6- L’effet global est la mort cellulaire par apopotose ou nécrose

10
Spécificités des traitements anticancéreux
Les cytotoxiques ne distinguent pas les cellules cancéreuses des cellules normales Les cellules cancéreuses sont plus fréquemment impliquées dans la multiplication cellulaire et sont plus sensibles aux effets toxiques des cytotoxiques La moelle osseuse, l’épithélium digestif et les follicules pileux sont les plus sensibles aux effets toxiques

11
Resistance to Cytotoxic Drugs
Increased expression of MDR-1 gene for a cell surface P-glycoprotein MDR-1 gene is involved with drug efflux Drugs that reverse MDR : verapamil, quinidine, cyclosporine MDR increases resistance to natural drug products including the anthracyclines, vinca alkaloids, and epipodophyllotoxins

12
Modes of Resistance to Anticancer Drugs
Mechanism Drugs or Drug Groups Change in sensitivity (or ↑ level) or ↓ binding affinity of target enzymes or receptors Etoposide, methotrexate, vinca alkaloids, estrogen & androgen receptors Decreased drug accumulation via ↑ expression of glycoprotein transporters, or ↓ permeability Methotrexate, alkylating agents, dactinomycin Formation of drug-inactivating enzymes Purine & pyrimidine antimetabolites Production of reactive chemicals that “trap” the anticancer drug Alkylators, bleomycin, cisplatin. doxorubicin Increased nucleic acid repair mechanisms Alkylating agents, cisplatin Reduced activation of pro-drugs
 or ↓ binding affinity of target enzymes or receptors. Etoposide, methotrexate, vinca alkaloids, estrogen & androgen receptors. Decreased drug accumulation via ↑ expression of glycoprotein transporters, or ↓ permeability. Methotrexate, alkylating agents, dactinomycin. Formation of drug-inactivating enzymes. Purine & pyrimidine antimetabolites. Production of reactive chemicals that trap the anticancer drug. Alkylators, bleomycin, cisplatin. doxorubicin. Increased nucleic acid repair mechanisms. Alkylating agents, cisplatin. Reduced activation of pro-drugs.")
13
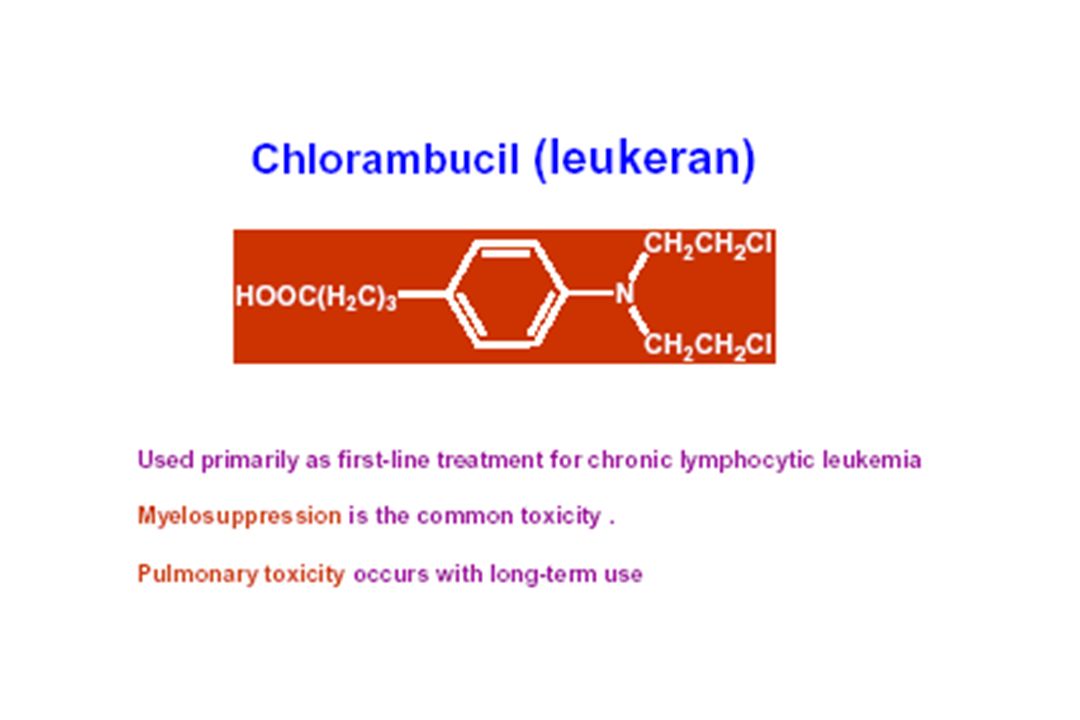
Les agents alkylants Sont responsables de la production d’ions très réactifs chargés positivement Ces ions forment des liaisons covalentes avec des régions electrophiles sur des molécules biologiques (Nucléotides, protéines AA) La liaison de ces alkylants fonctionnels au DNA est la cause de la mort (mutagenese, apoptose)
 La liaison de ces alkylants fonctionnels au DNA est la cause de la mort (mutagenese, apoptose)")
14
Alkylating agents Cyclophosphamide Cisplatin Procarbazine Busulfan
Mechlorethamine

15
Utilisation clinique Non-Hodgkin’s lymphoma Breast Ca Ovarian Ca
Neuroblastoma

16
Toxicités associées aux alkylants
Nausées vomissements Myélosuppression Alopécie Stérilité infertilité Second cancer Cystite hémorragique Neurotox Nephrotox Déficit immunitaire SIADH

17
Cyclophosphamide is a prodrug that must be oxidized by P450 enzymes in the liver to become pharmacologically active. Hydroxylation converts cyclophosphamide to 4-hydroxycyclophosphamide; this active metabolite can be further oxidized to the inactive metabolite 4-ketocyclophosphamide, or undergo ring cleavage to the active metabolite aldophosphamide. Aldophosphamide can be oxidized by aldehyde oxidase to the inactive metabolite carboxyphosphamide or be converted to the highly toxic metabolites acrolein and phosphoramide mustard. Accumulation of acrolein in the bladder can cause hemorrhagic cystitis; this adverse effect of cyclophosphamide can be ameliorated by coadministration of mesna, a sulfhydryl compound that inactivates the acrolein (not shown).
..")
18
ADR Acrolein is the metabolite
Responsible for causing hemorrhagic cystitis Suprapubic pain Hematuria Cyctoscopic findings ***This is prevented/treated by MESNA (mercaptoethanesulfonate) Rarely cyclophosphamide can cause SIADH and pulmonary toxicity
 Rarely cyclophosphamide can cause SIADH and pulmonary toxicity.")
25
Procarbazine MOA: forms hydrogen peroxide, which generates free radicals that cause DNA damage Important component of regimens especially for Hodgkin’s lymphoma ADR ***Disulfiram like reactions

26
Autres alkylants: les dérivés du Platine
Le Cis Platine

27
Cisplatin Platinum analog Same MOA as cyclophosphamide
**Used in testicular carcinoma Also used for Ca of bladder, lung and ovary Carboplatin is new drug with better safety profile ADR Nephrotoxicity (prevented by Amifostine***) ***Ototoxicity (acoustic nerve damage) Peripheral neuritis Severe nausea and vomiting
 ***Ototoxicity (acoustic nerve damage) Peripheral neuritis. Severe nausea and vomiting.")
28
Strategies pour améliorer les thérapeutiques
C CISPLATINE CARBOPLATINE Oxalato 1,2-trans-L-diaminocyclohexane platinium (OXALIPLATINE) l N H N H 3 O N H 2 O O 3 P t P t P t C l N H 3 O N H O 3 N H O 2 O Cibles et toxicité- mécanismes d’action- différents
 l. N. H. N. H. 3. O. N. H. 2. O. O. 3. P. t. P. t. P. t. C. l. N. H. 3. O. N. H. O. 3. N. H. O. 2. O. Cibles et toxicité- mécanismes d’action- différents.")
30
Anticancer Antibiotics
Anthracyclines: Doxorubicin (Adriamycin) Daunorubicin Bleomysin Dactinomycin Mitomycin
 Daunorubicin. Bleomysin. Dactinomycin. Mitomycin.")
31
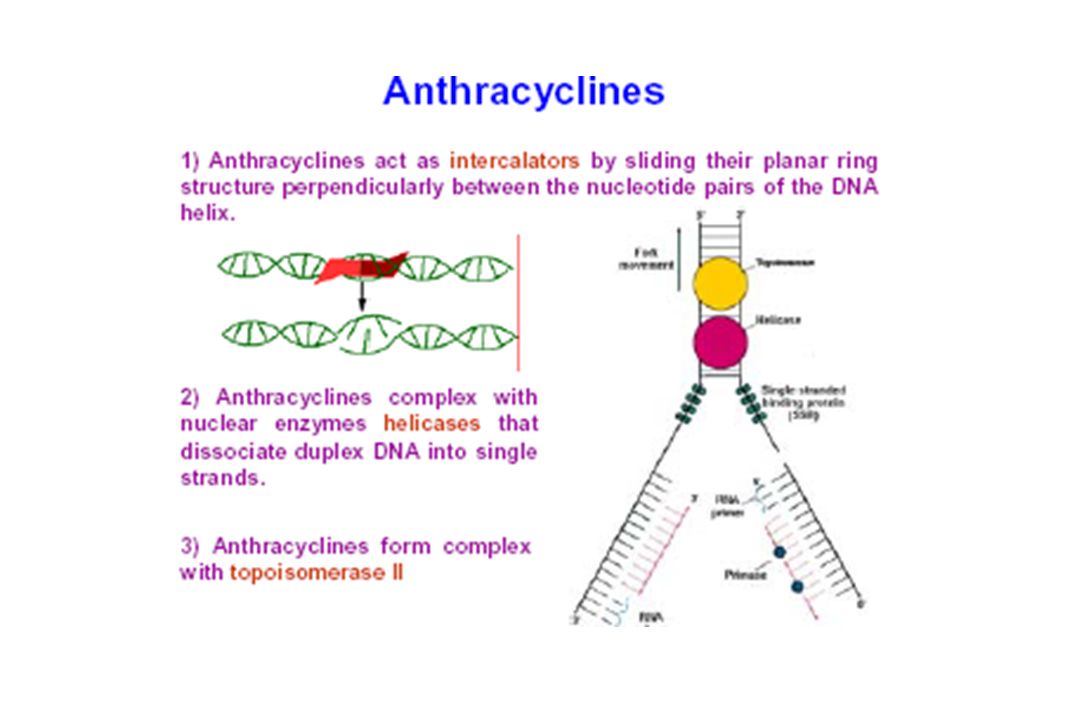
Doxorubicin & Daunorubicin
These drugs intercalate between base pairs, inhibit topoisomerase II and also generate free radicals They block RNA and DNA synthesis and cause strand scission *These are CCNS drugs Used as a component in ABVD regimen in Hodgkin’s lymphoma ABVD regimen • Adriamycin (generic name Doxorubicin) • Bleomycin (common brand name: blenoxane) • Vinblastine (common brand names: velban, velsar, velbe) • Dacarbazine (common brand name: DTIC, DTIC-Dome)
 • Bleomycin (common brand name: blenoxane) • Vinblastine (common brand names: velban, velsar, velbe) • Dacarbazine (common brand name: DTIC, DTIC-Dome)")
32
ADR Cardiac toxicity (due to generation of free radicals)
Acute form: arrthythmias, ECG changes, pericarditis, myocarditis Chronic form: ***Dilated cardiomyopathy, heart failure ****Rx with dexrazoxane This is an inhibitor of iron mediated free radical generation Bone marrow depression, Total alopecia Radiation recall reaction

33
Toxicités les plus communes avec les antibiotiques anticancéreux
Myélosuppression Mucite Nausées vomissements Alopécie Causticité Toxicités plus spécifiques Pulmonaires Cutanées Rappel de radiation Fièvre Toxicité cardiaque

38
Les antimétabolites sont des analogues structuraux de substances biologiquement impliquées dans la fonction cellulaire Ils vont interférer avec la synthèse des acides nucléiques en s’incorporant frauduleusement ou En inhibant de manière spécifique des enzymes critiques de la synthèse des acides nucléiques Ils sont cycle spécifique – Phase S

39
Fludarabine Phosphate
Legend Drug Class Sub-class Prototype Drug Trimetrexate Pemetrexed Cytarabine Gemcitabine Capecitabine Thioguanine Fludarabine Phosphate Cladribine 39

40
Antimetabolits: sites of drug action

41
Methotrexate

42
Methotrexate (MTX) MTX is a folic acid analog that binds with high affinity to the active catalytic site of dihydrofolate reductase (DHFR) Thus it interferes with the synthesis of tetrahydrofolate (THF) THF serves as the key one-carbon carrier for enzymatic processes involved in de novo synthesis of thymidylate, purine nucleotides, and the amino acids serine and methionine. Inhibition of these various metabolic processes thereby interferes with the formation of DNA, RNA, and key cellular proteins. Intracellular formation of polyglutamate metabolites is critically important for the therapeutic action of MTX. MTX polyglutamates are selectively retained within cancer cells, and they display increased inhibitory effects on enzymes involved in de novo purine nucleotide and thymidylate biosynthesis, making them important determinants of MTX's cytotoxic action.
 THF serves as the key one-carbon carrier for enzymatic processes involved in de novo synthesis of thymidylate, purine nucleotides, and the amino acids serine and methionine. Inhibition of these various metabolic processes thereby interferes with the formation of DNA, RNA, and key cellular proteins. Intracellular formation of polyglutamate metabolites is critically important for the therapeutic action of MTX. MTX polyglutamates are selectively retained within cancer cells, and they display increased inhibitory effects on enzymes involved in de novo purine nucleotide and thymidylate biosynthesis, making them important determinants of MTX s cytotoxic action.")
43
Mechanism of Resistance
1. Decreased drug transport 2. Altered DHFR 3. Decreased polyglutamate formation 4. Increased levels of DHFR

44
Contd.. Most commonly used anticancer drug.
Cell cycle specific (CCS) drug and acts during S phase of the cell cycle. Antineoplastic, immunosuppressant and antiinflammatory Used in RA, psoriasis Well absorbed orally; can also be given IM, IV or intrathecally**. It is bound to plasma proteins, does not cross the BBB and most of the drug is excreted unchanged in urine. It is a weak acid and so is excreted better at high urine pH. Appropriate hydration and alkalinizing the urine is important to prevent renal tox with MTX
 drug and acts during S phase of the cell cycle. Antineoplastic, immunosuppressant and antiinflammatory. Used in RA, psoriasis. Well absorbed orally; can also be given IM, IV or intrathecally**. It is bound to plasma proteins, does not cross the BBB and most of the drug is excreted unchanged in urine. It is a weak acid and so is excreted better at high urine pH. Appropriate hydration and alkalinizing the urine is important to prevent renal tox with MTX.")
45
ADR Bone marrow suppression (BMS) Mucositis Folic acid deficiency
The toxic effects of MTX on normal cells is reduced by administering folinic acid (leucovorin) This is called leucovorin rescue **** Higher the dose of MTX more the leucovorin you give**
 This is called leucovorin rescue **** Higher the dose of MTX more the leucovorin you give**")
46
Leucovorin Rescue Mechanism of action of methotrexate and the effect of administration of leucovorin. FH2 = dihydrofolate FH4 = tetrahydrofolate dTMP = deoxythymidine monophosphate dUMP = deoxyuridine mono phosphate.

47
6-Mercaptopurine (6-MP) & Thioguanine
Both 6-MP and Thioguanine are activated by HGPRT to toxic nucleotides that inhibit several enzymes involved in purine metabolism ***Resistance is due to cancer cells having d activity of HGPRT Cancer cells also es alkaline phosphatase that inactivate toxic nucleotides

48
6-MP & Allopurinol 6-MP is metabolized in the liver by xanthine oxidase and the inactive metabolites are excreted in the urine ***Allopurinol is used frequently to treat/prevent hyperuricemia caused by many anticancer drugs. If Allopurinol is used with 6-MP then the dose of 6-MP is reduced by more than 75% Why??

49
Cytarabine (Ara-C) Cytarabine arabinoside is a pyrimidine antimetabolite The drug is activated by kinases to AraCTP This acts as an inhibitor of DNA polymerase ***of all antimetabolites, this is the most specific for S phase of tumor cell cycle It is an important component in acute lukemia regimens ADR: at high doses cause neurotoxicity (cerebellar dysfunction and peripheral neuritis) Hand-foot syndrome***
 Hand-foot syndrome***")
50
5-FU Mechanism of the cytotoxic action of 5-FU
5-FU is converted to 5-FdUMP, which competes with deoxyuridine monophosphate (dUMP) for the enzyme thymidylate synthetase. 5-FU = 5-fluorouracil 5-FUR = 5-fluorouridine 5-FUMP = 5-fluorouridine monophosphate 5-FUDP = 5-fluorouridine diphosphate 5-FUTP = 5-fluorouridine triphosphate dUMP = deoxyuridine monophosphate dTMP = deoxythymidine monophosphate 5-FdUMP = 5-fluorodeoxyuridine monophosphate.
 for the enzyme thymidylate synthetase. 5-FU = 5-fluorouracil. 5-FUR = 5-fluorouridine. 5-FUMP = 5-fluorouridine monophosphate. 5-FUDP = 5-fluorouridine diphosphate. 5-FUTP = 5-fluorouridine triphosphate. dUMP = deoxyuridine monophosphate. dTMP = deoxythymidine monophosphate. 5-FdUMP = 5-fluorodeoxyuridine monophosphate.")
51
Contd.. 5-FU causes, “thymidineless death” of cells
Resistance is due to d activation of 5-FU and d thymidylate synthase activity Uses and ADR Metastatic carcinomas of the breast and the GI tract, hepatoma Carcinomas of the ovary, cervix, urinary bladder, prostate, pancreas, and oropharyngeal areas Combined with levamisole for Rx of colon cancer ADR: nausea, mucositis, diarrhea, ***hand and foot syndrome, Alopecia, hyperpigmentation, neurologic deficits, bone marrow depression Hand-foot syndrome is a side effect of some chemotherapy drugs that results when a small amount of drug leaks out of the blood vessels, damaging tissues. This tends to happen in the hands and the feet because of the increased friction and heat that your extremities are exposed to through daily activities. Symptoms can be prevented by avoiding friction and heat. Treatment consists of reducing or stopping treatment with the drug that caused the syndrome. You may be able to prevent symptoms by avoiding friction or heat. Symptoms of hand-foot syndrome include: Tingling or burning Redness Flaking Swelling Small blisters Small sores on the palms of the hands or soles of the feet

52
Stratégies pour améliorer les thérapeutiques
N F O C 1 U 2 5 _ E n i l u r a c e A B - ( 4 ) ' D R 3 d T h P s M CAPECITABINE Stratégies pour améliorer les thérapeutiques Nombreux médicaments adaptés à la forme orale: Taxanes, Vinorelbine, Inhibiteurs de TOPO-1…
 D. R. 3. d. T. h. P. s. M. CAPECITABINE Stratégies pour améliorer les thérapeutiques. Nombreux médicaments adaptés à la forme orale: Taxanes, Vinorelbine, Inhibiteurs de TOPO-1…")
55
Teniposide Docetaxel Vinblastine Vincristine Vinorelbine Irinotecan
All derived from plant extracts 55

57
Vinka alkaloids (Vinblastine, vincristine)
These drugs block the formation of mitotic spindle by preventing the assembly of tubulin dimers into microtubules ***They act primarily on the M phase of cancer cell cycle Resistance is due to d efflux of drugs from tumor cells

58
VinCristine (oncovan)
VinBlastine VinCristine (oncovan) Uses ; (ABVD) Hodgkin’s disease Lymphomas Carcinoma Breast Testicular tumors Toxicity: Bone marrow suppression, anorexia, nausea, vomiting & Diarrhea, Alopecia Uses: (MOPP) Childhood leukemias Childhood tumors-Wilm’s tumor, Neuroblastoma, Hodgkin’s disease Peripheral neuritis with Paresthesia, Muscle weakness ***Vincristine has marrow sparing effect ABVD regimen: • Adriamycin (generic name Doxorubicin) • Bleomycin (common brand name: blenoxane) • Vinblastine (common brand names: velban, velsar, velbe) • Dacarbazine (common brand name: DTIC, DTIC-Dome) MOPP regimen • Mustargen (generic name mechlorethamine, MSD, mustine or nitrogen mustard) • Vincristine (also called Oncovin or VCR) • Procarbazine (also called Matulane or possibly Natulan) • Prednisone (sometimes called Deltasone or Orasone)
 Uses ; (ABVD) Hodgkin’s disease Lymphomas. Carcinoma Breast. Testicular tumors. Toxicity: Bone marrow. suppression, anorexia, nausea, vomiting & Diarrhea, Alopecia. Uses: (MOPP) Childhood leukemias. Childhood tumors-Wilm’s tumor, Neuroblastoma, Hodgkin’s disease. Peripheral neuritis with. Paresthesia, Muscle weakness. ***Vincristine has marrow sparing effect. ABVD regimen: • Adriamycin (generic name Doxorubicin) • Bleomycin (common brand name: blenoxane) • Vinblastine (common brand names: velban, velsar, velbe) • Dacarbazine (common brand name: DTIC, DTIC-Dome) MOPP regimen. • Mustargen (generic name mechlorethamine, MSD, mustine or nitrogen mustard) • Vincristine (also called Oncovin or VCR) • Procarbazine (also called Matulane or possibly Natulan) • Prednisone (sometimes called Deltasone or Orasone)")
59
Etoposide & Teniposide
Acts by inhibiting topoisomerase II These drugs are most active in late S and early G2 phase Used in combination Tx of small cell carcinoma of lung, prostrate and testicular carcinomas Other topoisomerase inhibitors: Topotecan, Irinotecan Both act by inhibiting topoisomerase-I

60
Topoisomerase inhibitors

62
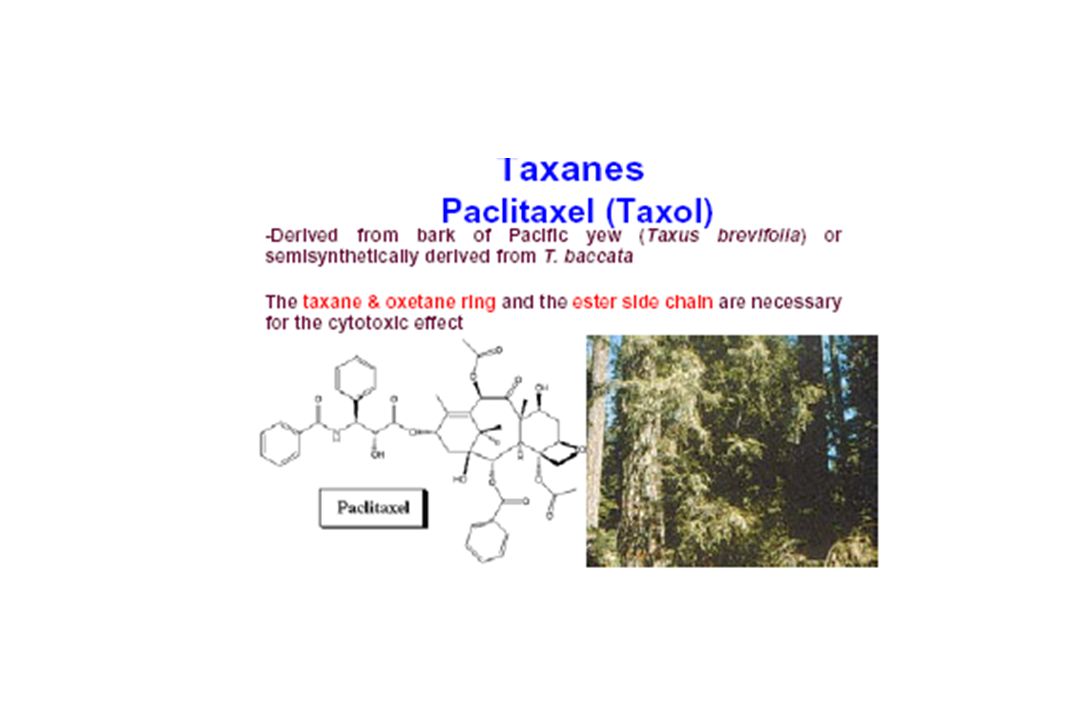
Paclitaxel & Docetaxel
These drugs act by interfering with mitotic spindle They prevent micotubule disassembly into tubulin monomers Taxanes animation ADR Neutropenia Peripheral neuropathy

63
Etoposide (VP16 et teniposide VM26

67
General problems with anticancer drugs
Most of them are antiproliferative, i.e. they damage DNA and so initiate apoptosis. They also affect rapidly dividing normal cells. This leads to toxicity which are usually severe. To greater or lesser extent the following toxicities are exhibits by all anticancer drugs.

68
ADR of Antineoplastic Drugs in Humans

69
Distinctive Toxicities of Some Anticancer Drugs
Toxicity Drug(s) Renal Cisplatin,* methotrexate Hepatic 6-MP, busulfan, cyclophosphamide Pulmonary Bleomycin,* busulfan, procarbazine Cardiac Doxorubicin, daunorubicin Neurologic Vincristine,* cisplatin, paclitaxel Immunosuppressive Cyclophosphamide, cytarabine, dactinomycin, methotrexate Other Cyclophosphamide (hemorrhagic cystitis); procarbazine (leukemia); asparaginase* (pancreatitis) *Less Bone marrow suppression – “marrow sparing”
 Renal. Cisplatin,* methotrexate. Hepatic. 6-MP, busulfan, cyclophosphamide. Pulmonary. Bleomycin,* busulfan, procarbazine. Cardiac. Doxorubicin, daunorubicin. Neurologic. Vincristine,* cisplatin, paclitaxel. Immunosuppressive. Cyclophosphamide, cytarabine, dactinomycin, methotrexate. Other. Cyclophosphamide (hemorrhagic cystitis); procarbazine (leukemia); asparaginase* (pancreatitis) *Less Bone marrow suppression – marrow sparing")
70
Chemotherapeutic agents are much more toxic to tissues that have a high growth fraction than to tissues that have a low growth fraction. Proliferating cells are especially sensitive to chemotherapy because cytotoxic drugs usually act by disrupting DNA synthesis or mitosis, cellular activities that only proliferating cells carry out. Unfortunately, toxicity to the anticancer agents is to any rapidly dividing cells. (e.g. bone marrow, hair follicles, sperm forming cells).
.")
71
Prevention or Management of Drug Induced toxicities
The toxicities of some anticancer drugs can be well anticipated and hence be prevented by giving proper medications E.g. mesna is given to prevent hemorrhagic cystitis by cyclophosphamide Dexrazoxane, is used to reduce the risk of anthracycline-induced cardiomyopathy

72
Hormonal agents Glucocorticoids Sex hormone antagonists GnRH analogs
Aromatase inhibitors

73
Glucocorticoids (Prednisone)
Because of their marked lympholytic action, they are used in acute leukemias and lymphomas. Have anti-inflammatory effect Increase appetite Produce euphoria (feeling of well being) Increase body weight Suppress hypersensitivity reaction due to certain anticancer drugs Control hypercalcemia Control bleeding Have non-specific antipyretic effect Increase the antiemetic effect of ondansetron/granisetron/ metoclopramide
 Increase body weight. Suppress hypersensitivity reaction due to certain anticancer drugs. Control hypercalcemia. Control bleeding. Have non-specific antipyretic effect. Increase the antiemetic effect of ondansetron/granisetron/ metoclopramide.")
74
Sex hormone antagonists

75
Tamoxifen It is a SERM Blocks the binding of estrogen to receptors of estrogen sensitive cancer cells in bresat tissue It is used in receptor positive breast carcinoma Also useful in progestin resistant endometrial carcinoma ADR: Hot flushes, vaginal bleeding and venous thrombosis Other drugs Flutamide: androgen receptor antagonist used in prostatic carconima ADR for flutamide includes: gynecomastia, hot flushes

76
MOA of drugs

77
GnRH analogs Leuprolide, gosarelin and naferelin
Effective in management of Prostatic carcinomas When given in constant doses they inhibit release of pituitary LH and FSH These drugs suppress gonadal function due to down regulation and desensitization of Gn-RH receptors ADR Leuprolide may cause gynecomastia, hematuria, impotence and testicular atrophy Gonadotropin-releasing hormone is normally secreted by the hypothalamus and stimulates the anterior pituitary to secrete the gonadotropic hormones, luteinizing hormone (LH; the primary stimulus for the secretion of testosterone by the testes), and follicle-stimulating hormone (FSH; which stimulates the secretion of estrogen). The synthetic nonapeptides, leuprolide [loo-PROE-lide] and goserelin [GOE-se-rel-in], are analogs of GnRH. As GnRH agonists, they occupy the GnRH receptor in the pituitary, which leads to its desensitization and, consequently, inhibition of release of FSH and LH. Thus, both androgen and estrogen syntheses are reduced. Response to leuprolide in prostatic cancer is equivalent to that of orchiectomy (surgical removal of one or both testes), with regression of tumor and relief of bone pain.
, and follicle-stimulating hormone (FSH; which stimulates the secretion of estrogen). The synthetic nonapeptides, leuprolide [loo-PROE-lide] and goserelin [GOE-se-rel-in], are analogs of GnRH. As GnRH agonists, they occupy the GnRH receptor in the pituitary, which leads to its desensitization and, consequently, inhibition of release of FSH and LH. Thus, both androgen and estrogen syntheses are reduced. Response to leuprolide in prostatic cancer is equivalent to that of orchiectomy (surgical removal of one or both testes), with regression of tumor and relief of bone pain.")
78
Aromatase inhibitors The aromatase reaction is responsible for the extra-adrenal synthesis of estrogen from androstenedione This takes place in liver, fat, muscle, skin, and breast tissue, including breast malignancies. Peripheral aromatization is an important source of estrogen in postmenopausal women. Aromatase inhibitors decrease the production of estrogen in these women.

79
Contd..

80
Contd.. Anastrozole and Letrozole
These drugs inhibit the aromatase enzyme ****Used in Tx of postmenopausal women with metastatic breast ca (1st line drug) ADR includes: bone pain and peripheral edema
 ADR includes: bone pain and peripheral edema.")
Présentations similaires





















.>")




>")



