Télécharger la présentation
La présentation est en train de télécharger. S'il vous plaît, attendez

1
Troubles de la sexualité masculine Quoi de neuf en 2014 ?
R.J. Opsomer, urologue Hubin, sexologue Centre de Pathologie Sexuelle Masculine (CPSM) Cliniques St Luc – 1200 Bruxelles
 Cliniques St Luc – 1200 Bruxelles.")
2
Plan de l’exposé Troubles de la sexualité masculine : une affaire de couple
Physiologie de la fonction sexuelle Anamnèse médicale et sexologique Cas clinique N°1 : Trouble érectile Questions et réponses Cas clinique N°2 : Trouble éjaculatoire

4
Anatomie du Pénis albuginée Corps caverneux Corps spongieux
Artère caverneuse albuginée Corps caverneux Corps spongieux

6
La Réponse Sexuelle chez l’homme
Période réfractaire

7
Physiologie I : la phase de Flaccidité
Veines ouvertes albuginée

8
Physiologie II : la phase d’Erection
Veines collabées albuginée

9
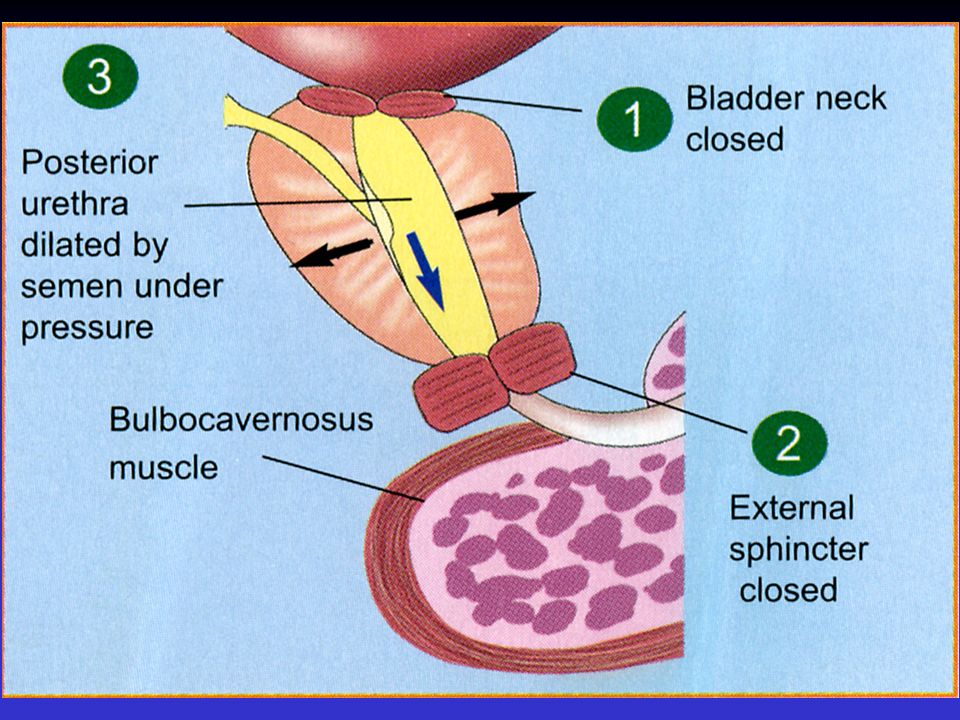
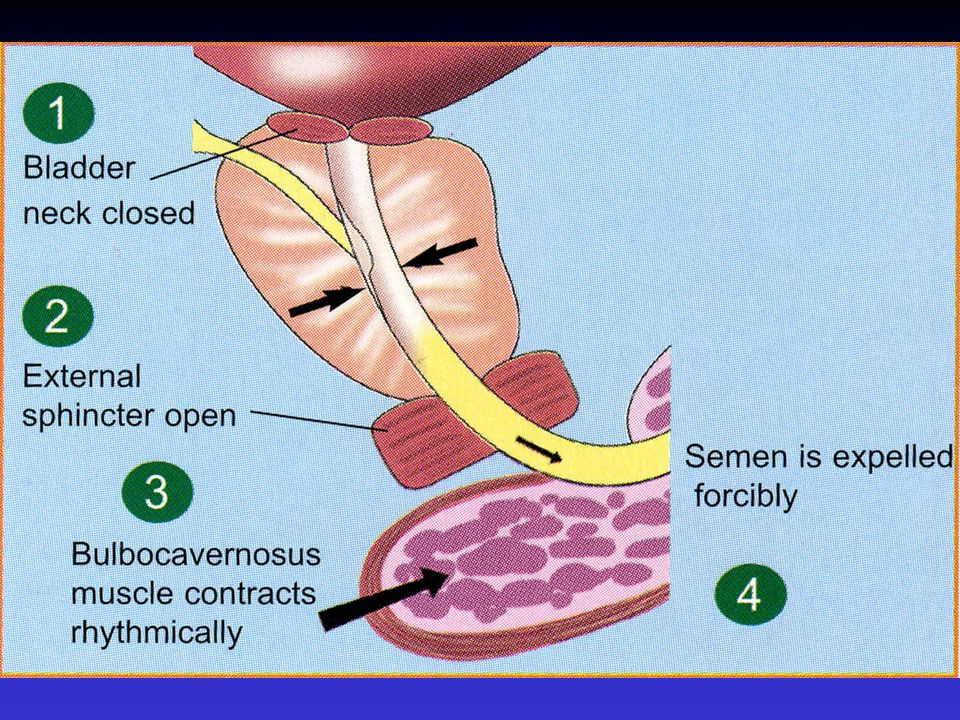
Le réflexe éjaculatoire :
Voies ascendantes Voies descendantes: - phase d’émission - phase d’éjection

13
Orgasme >< éjaculation
décharge centrale du « centre » orgasmique limbique après stimulation des récepteurs de l’urètre Ejaculation : décharge périphérique sous l’influence des centres médullaires et cérébraux après stimulation des récepteurs du gland

14
La Réponse sexuelle de la femme La Réponse sexuelle de l’homme

15
Evaluation d’un trouble d’érection : le rôle du médecin généraliste
Anamnèse et examen clinique Bilan de santé : biologie,.. 1er traitement (inhibiteurs de la PDE – 5) Si échec :avis de l’urologue : Bilan vasculaire : Doppler pulsé du pénis + IC PGE1 Bilan neurophysiologique : Arc Réflexe sacré Potentiels évoqués
 Si échec :avis de l’urologue : Bilan vasculaire : Doppler pulsé du pénis. + IC PGE1. Bilan neurophysiologique : Arc Réflexe sacré. Potentiels évoqués.")
16
La Consultation en sexologie
Anamnèse Examen clinique Biologie

17
Antécédents personnels
Antécédents chirurgicaux - urologiques : prostate, … - non-urologiques : carrefour aortique,…. - génito-sexuels Antécédents médicaux Facteurs de risques vasculaires ? Pathologies neuro ? Assuétudes ? Tabac, alcool…

18
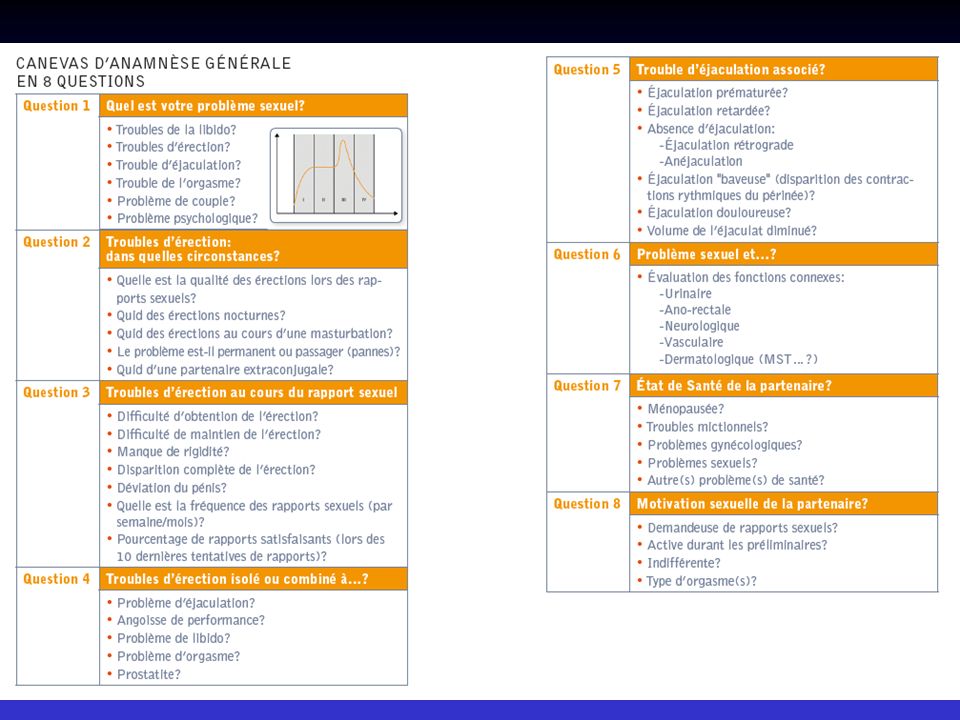
Quel est le problème sexologique ?
Trouble de libido? Trouble d’érection? Trouble d’éjaculation? Trouble de l’orgasme? Trouble combiné ?

19
Troubles d’érection: de quelle érection?
Érections lors des rapports sexuels Erections nocturnes Erections au cours d’une masturbation

20
Troubles d’érection Difficulté d’obtention de l’érection
Difficulté de maintien de l’érection Manque de rigidité Disparition complète de l’érection Au cours du rapport sexuel

21
Anamnèse Trouble d’érection isolé ? ou problème combiné ?
Problème d’éjaculation ? Angoisse de performance Problème de libido? Problème d’orgasme?

22
Troubles de l’éjaculation
Ejaculation retardée Absence d’éjaculation ( éjaculation rétrograde ) ( anéjaculation ) Éjaculation baveuse (disparition des contractions sphinctériennes) Ejaculation prématurée
 ( anéjaculation ) Éjaculation baveuse. (disparition des contractions sphinctériennes) Ejaculation prématurée.")
23
Anamnèse Trouble d’érection + éjaculation prématurée
Quid des aspects relationnels – psychologiques ?? Angoisse de performance ?

24
Problème sexologique et…
Évaluation des fonctions connexes: - urinaire - ano-rectale - neurologique - vasculaire

25
Etat de santé de la partenaire
Ménopausée ? Problèmes sexuels? - problème de libido ? - sécheresse vaginale ? - problème d’orgasme ?

26
Motivation de la partenaire
Demandeuse de rapports sexuels ? Active ? Indifférente ? Type d’orgasme ?

28
Le médecin généraliste et ses collègues
En sexologie, on pratique : la multidisciplinarité l’interdisciplinarité le multi-métiers

29
CPSM GYNÉCOLOGIE ANDROLOGIE UROLOGIE
Ménopause Infertilité masculine UROLOGIE Troubles d’érection et d’éjaculation CENTRE DE PATHOLOGIE SEXUELLE MASCULINE DERMATOLOGIE SEXOLOGIE MEDICALE CPSM PSYCHOPATHOLOGIE Dysfonction sexuelle et troubles psychiatriques ENDOCRINOLOGIE 29

30
Cas 1 : Trouble érectile Mr J.B. 62 ans Antécédents chirurgicaux
- appendicectomie (1970) - Prostatectomie radicale (2013) Antécédents médicaux : - Médications : - Motif de consultation : trouble érectile depuis la PRT Post-op : discrète incontinence urinaire (actuellement résolue) érections disparues
 - Prostatectomie radicale (2013) Antécédents médicaux : - Médications : - Motif de consultation : trouble érectile depuis la PRT. Post-op : discrète incontinence urinaire (actuellement résolue) érections disparues.")
31
Anamnèse sexologique En Pré-opératoire : En Post-opératoire :
- rapports sexuels satisfaisants - 2 rapports sexuels par semaine En Post-opératoire : Érections matinales disparues Tumescence pénienne lors des tentatives de rapports Anéjaculation (par la force des choses) Lubrification urétrale présente Orgasme émoussé Que faire ?
 Lubrification urétrale présente. Orgasme émoussé. Que faire")
32
Traitements Inhibiteurs de la PDE-5 : échec
Injections intracaverneuses de PGE 1 : efficaces Le patient pratique 1 injection par semaine Epouse : peu favorable (mais compréhensive) aux injections car il s’agit d’une sexualité programmée Avis de la sexologue
 aux injections car il s’agit d’une sexualité programmée. Avis de la sexologue.")
33
Adénomectomie prostatique versus Prostatectomie radicale

34
Adénomectomie prostatique chirurgie ouverte

35
Principe de l’adénomectomie prostatique

36
Adénomectomie vs Prostatectomie Radicale

37
Prostatectomie radicale

38
Evaluation d’un trouble d’érection : le rôle du médecin généraliste
Anamnèse et examen clinique Bilan de santé : biologie,.. 1er traitement (inhibiteurs de la PDE – 5) Si échec :avis de l’urologue : Bilan vasculaire : Doppler pulsé du pénis + IC PGE1 Bilan neurophysiologique : Arc Réflexe sacré Potentiels évoqués
 Si échec :avis de l’urologue : Bilan vasculaire : Doppler pulsé du pénis. + IC PGE1. Bilan neurophysiologique : Arc Réflexe sacré. Potentiels évoqués.")
39
Algorithme du traitement de la D.E.
I. Traitement oral : inhibiteurs de la PDE 5 - Sildénafil (Viagra) - Tadalafil (Cialis) - Vardénafil (Levitra) - Avanafil (Spedra) II. Injections intracaverneuses III. Pompe à vide Prothèses péniennes Si échec Si échec ou refus R.J.O- 2003
 - Tadalafil (Cialis) - Vardénafil (Levitra) - Avanafil (Spedra) II. Injections intracaverneuses. III. Pompe à vide. Prothèses péniennes. Si échec. Si échec ou. refus. R.J.O")
40
Un nouvel inhibiteur de la
phosphodiestérase de type 5 Avanafil - Spedra

41
SPEDRA tablets SPEDRA tablets are pale yellow and oval in appearance, and are debossed with “50”, “100” or “200” on one side. The tablets are provided in blisters in cartons of 4 or 12 tablets. Each tablet contains 50, 100 or 200 mg of avanafil References Avanafil Summary of Product Characteristics, 2013 Avanafil SmPC 2013

42
Commonly used oral PDE5 inhibitors: Timing of administration
Onset of action (minutes after dosing) Duration (hours) Sildenafil 60 minutes 4 Tadalafil 120 36 Vardenafil 60 Avanafil - SPEDRA Approximately 30 >6 hours References Avanafil Summary of Product Characteristics, 2013 Sildenafil Summary of Product Characteristics, June 2013 Vardenafil Summary of Product Characteristics, April 2013 Tadalafil Summary of Product Characteristics, April 2013 Kang SG, Kim JJ. Udenafil: efficacy and tolerability in the management of erectile dysfunction. Ther Adv Urol 2013;5:101-10 Spedra SmPC 2013; Sildenafil SmPC June 2013; Vardenafil SmPC April 2013; Tadalafil SmPC April 2013; Kang & Kim Ther Adv Urol 2013 FCT, film-coated tablet; ODT, orodispersible tablet; PDE, phosphodiesterase
 Duration (hours) Sildenafil. 60 minutes. 4. Tadalafil Vardenafil. 60. Avanafil - SPEDRA. Approximately 30. >6 hours. References. Avanafil Summary of Product Characteristics, Sildenafil Summary of Product Characteristics, June Vardenafil Summary of Product Characteristics, April Tadalafil Summary of Product Characteristics, April Kang SG, Kim JJ. Udenafil: efficacy and tolerability in the management of erectile dysfunction. Ther Adv Urol 2013;5: Spedra SmPC 2013; Sildenafil SmPC June 2013; Vardenafil SmPC April 2013; Tadalafil SmPC April 2013; Kang & Kim Ther Adv Urol FCT, film-coated tablet; ODT, orodispersible tablet; PDE, phosphodiesterase.")
43
Cas 2 : Ejaculation prématurée
Mr SF – 41 ans Antécédents chirurgicaux - fracture calcaneum dt - genou dt (ligaments) Antécédents médicaux - Asthme Médications Temesta Ventolin Sérétide
 Antécédents médicaux. - Asthme. Médications. Temesta. Ventolin. Sérétide.")
44
Histoire sexologique À 20 ans : déchirure du frein du gland lors du 1er rapport Marié durant 10 ans – 2 enfants - divorce mal vécu (épouse avait un partenaire extraconjugal) Pas de rapports sexuels durant 2 ans Nouvelle partenaire (43 ans) depuis 4 mois Ils se voient le WE uniquement : 1 à 2RS /WE Rapports sexuels : erection ok - mais éjaculation prématurée Stress – partenaire insatisfaite la partenaire lui a fait une réflexion blessante « ton pénis est trop petit » Spirale négative : espacement des rapports – aggravation de l’éjaculation prématurée Prescription : Dapoxétine (Priligy) Prise en charge sexologique indispensable (A Hubin)
 Pas de rapports sexuels durant 2 ans. Nouvelle partenaire (43 ans) depuis 4 mois. Ils se voient le WE uniquement : 1 à 2RS /WE. Rapports sexuels : erection ok - mais éjaculation prématurée. Stress – partenaire insatisfaite. la partenaire lui a fait une réflexion blessante « ton pénis est trop petit » Spirale négative : espacement des rapports – aggravation de l’éjaculation prématurée. Prescription : Dapoxétine (Priligy) Prise en charge sexologique indispensable (A Hubin)")
45
Dapoxetine in EAU Guidelines
Dapoxetine is the first and only drug approved for the on-demand treatment of premature ejaculation Dapoxetine has been approved (December 2008) for the on-demand treatment of PE in seven European countries (Sweden, Austria, Finland, Germany, Spain, Italy and Portugal). This is currently the first and only drug approved for such an indication. EAU. Guidelines on Male Sexual Dysfunction: Erectile dysfunction and premature ejaculation. (EAU 2012). 45
 for the on-demand treatment of PE in seven European countries (Sweden, Austria, Finland, Germany, Spain, Italy and Portugal). This is currently the first and only drug approved for such an indication. EAU. Guidelines on Male Sexual Dysfunction: Erectile dysfunction and premature ejaculation. (EAU 2012). 45.")
46
Dapoxetine site of action
Higher brain centres Data suggests that Dapoxetine site of action is at the brainstem level or above Data from Giuliano and Clement shows that the action of Dapoxetine in delaying ejaculation involves the lateral nucleus paragigantocellularis (nPGi) in the brainstem. The anatomical site of action of Dapoxetine has been investigated in animal models and shown to be located supraspinally, in the higher centres of the brain, and involving the lateral paragigantocellularis nucleus (nPGi). The role of the Pudendal nerve is to drive motor outputs to bulbospongiosus muscle, while the dorsal nerve of penis is mainly responsible of the afferent transmission of sensory inputs. In animal models electrical stimulation of the dorsal nerves of the penis has been shown to induce pudendal motoneuron reflex discharges (PMRDs), which can be measured at level of the motor branch of the pudendal nerve. Pudendal motorneuron reflex discharges (PMRDs) have beene measured following electrical stimulation of the dorsal nerves of the penis in rats following intrathecal administration of Dapoxetine. PMRDs were significantly delayed with Dapoxetine indicating a delay in the ejaculatory expulsion reflex. However, in rats with a lesion in the nPGi brain structure, the effects of Dapoxetine were abolished. afferent Dorsal nerve of penis efferent Pudendal nerve Motor supply to the bulbospongiosus muscle Clement et al. Eur Urol 2007;51(3): Giuliano & Clement. Eur Urol 2006;50(3): Giuliano. Trends Neurosci 2007;30(2):79-84. 46
 in the brainstem. The anatomical site of action of Dapoxetine has been investigated in animal models and shown to be located supraspinally, in the higher centres of the brain, and involving the lateral paragigantocellularis nucleus (nPGi). The role of the Pudendal nerve is to drive motor outputs to bulbospongiosus muscle, while the dorsal nerve of penis is mainly responsible of the afferent transmission of sensory inputs. In animal models electrical stimulation of the dorsal nerves of the penis has been shown to induce pudendal motoneuron reflex discharges (PMRDs), which can be measured at level of the motor branch of the pudendal nerve. Pudendal motorneuron reflex discharges (PMRDs) have beene measured following electrical stimulation of the dorsal nerves of the penis in rats following intrathecal administration of Dapoxetine. PMRDs were significantly delayed with Dapoxetine indicating a delay in the ejaculatory expulsion reflex. However, in rats with a lesion in the nPGi brain structure, the effects of Dapoxetine were abolished. afferent. Dorsal nerve of penis. efferent. Pudendal nerve. Motor supply to the bulbospongiosus muscle. Clement et al. Eur Urol 2007;51(3): Giuliano & Clement. Eur Urol 2006;50(3): Giuliano. Trends Neurosci 2007;30(2):")
47
Conclusions: Dapoxetine mode of action
Dapoxetine increases serotonin levels in the synaptic cleft by inhibiting re-uptake into the axonal terminal There is experimental support for the effect of acute/on demand Dapoxetine to delay ejaculation Site of action of Dapoxetine is supraspinal likely involving the nPGi, a key structure controlling ejaculation Dapoxetine undergoes rapid absorption and elimination, resulting in low drug accumulation The 30- and 60-mg doses of Dapoxetine demonstrate dose-proportional pharmacokinetics, which are unaffected by multiple dosing taken no more than once a day Peak concentrations reached within approx 1.3 hours Plasma concentrations at 24 hours <5% of peak The pharmacokinetic profile of Dapoxetine is unaffected by co-administration of PDE-5 inhibitors. Giuliano & Clement. Eur Urol 2006;50(3): Giuliano. Trends Neurosci 2007;30(2):79-84. 47
: Giuliano. Trends Neurosci 2007;30(2):")
48
Comment évaluer une éjaculation prématurée
Comment évaluer une éjaculation prématurée ? IELT Intravaginal Ejaculation Latency Time Délai entre la pénétration et l’éjaculation

49
Improvement in IELT after treatment with Dapoxetine
Study conducted in Asia and Australia * † Dapoxetine significantly increased IELT values. At 12 weeks, values were nearly 4-fold greater with Dapoxetine versus baseline. A marked increase in IELT values was noted with placebo, although increases with Dapoxetine were significantly greater. *P <0.001 vs. placebo; †week 12 or last observation carried forward. McMahon et al. J Sex Med 2010;7: 49

50
Improvement in perceived control over ejaculation after treatment with Dapoxetine
‘Over the past month was your control over ejaculation during sexual intercourse… very poor, poor, fair, good, very good?’ * † Dapoxetine significantly improved patients’ perception of control over ejaculation. When studied by category, Dapoxetine was associated with a large increase in the proportion of patients reporting “good” or “very good” control over ejaculation from baseline values (18.7%, 33.5% and 33.5% in the placebo, 30 mg and 60 mg Dapoxetine groups, respectively, at study endpoint). *P <0.001 vs. placebo; †Week 12 or last observation carried forward. McMahon et al. J Sex Med 2010;7: 50
. *P <0.001 vs. placebo; †Week 12 or last observation carried forward. McMahon et al. J Sex Med 2010;7:")
51
Dapoxetine: indication and use
Dapoxetine is indicated for the treatment of premature ejaculation (PE) in adult men aged 18 to 64 years. Dapoxetine should only be prescribed to patients who meet all the following criteria: An intravaginal ejaculatory latency time (IELT) of less than two minutes; and Persistent or recurrent ejaculation with minimal sexual stimulation before, on, or shortly after penetration and before the patient wishes; and Marked personal distress or interpersonal difficulty as a consequence of PE; and Poor control over ejaculation; and A history of premature ejaculation in the majority of intercourse attempts over the prior 6 months. Dapoxetine should be administered only as on-demand treatment before anticipated sexual activity. Dapoxetine should not be prescribed to delay ejaculation in men who have not been diagnosed with PE. A careful appraisal of individual benefit risk of Dapoxetine should be performed by the physician after the first four weeks of treatment (or at least after 6 doses of treatment) to determine whether continuing treatment with Dapoxetine is appropriate. Data regarding the efficacy and safety of Dapoxetine beyond 24 weeks are limited. The clinical need of continuing and the benefit risk balance of treatment with Dapoxetine should be re-evaluated at least every six months. PRILIGY®. SmPC.
 in adult men aged 18 to 64 years. Dapoxetine should only be prescribed to patients who meet all the following criteria: An intravaginal ejaculatory latency time (IELT) of less than two minutes; and. Persistent or recurrent ejaculation with minimal sexual stimulation before, on, or shortly after penetration and before the patient wishes; and. Marked personal distress or interpersonal difficulty as a consequence of PE; and. Poor control over ejaculation; and. A history of premature ejaculation in the majority of intercourse attempts over the prior 6 months. Dapoxetine should be administered only as on-demand treatment before anticipated sexual activity. Dapoxetine should not be prescribed to delay ejaculation in men who have not been diagnosed with PE. A careful appraisal of individual benefit risk of Dapoxetine should be performed by the physician after the first four weeks of treatment (or at least after 6 doses of treatment) to determine whether continuing treatment with Dapoxetine is appropriate. Data regarding the efficacy and safety of Dapoxetine beyond 24 weeks are limited. The clinical need of continuing and the benefit risk balance of treatment with Dapoxetine should be re-evaluated at least every six months. PRILIGY®. SmPC.")
52
Dapoxetine: occurrence of syncope
Orthostatic hypotension and syncope have been reported in clinical trials Frequency of syncope in clinical trials Placebo Dapoxetine 30 mg Dapoxetine 60 mg Syncope (%) 0.05 0.06 0.23 Percentages of patients reporting syncope during the treatment with Dapoxetine 30 mg or 60 mg on demand, or placebo. Results from an integrated analysis (n = 6,081) of the efficacy and the safety data from five randomized, double-blind, placebo-controlled, phase 3 studies, on men with PE. PRILIGY®. SmPC. McMahon et al. J Sex Med 2011;8:
 Percentages of patients reporting syncope during the treatment with Dapoxetine 30 mg or 60 mg on demand, or placebo. Results from an integrated analysis (n = 6,081) of the efficacy and the safety data from five randomized, double-blind, placebo-controlled, phase 3 studies, on men with PE. PRILIGY®. SmPC. McMahon et al. J Sex Med 2011;8:")
56
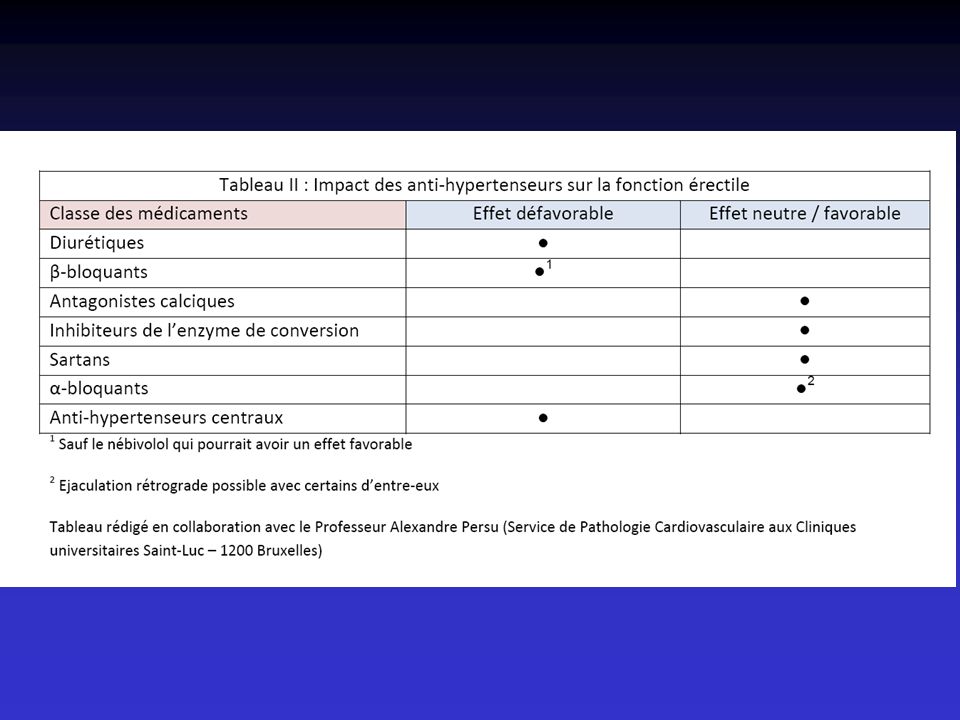
Dysfonction Endothéliale
Facteurs de Risque Maladies Cardiovasculaires Tabac TA Cholestérol Diabète Dysfonction Erectile Tabac TA Cholestérol Diabète Symptôme sentinelle ? D.E. Dysfonction Endothéliale Dénominateur Commun From Th Roumeguère – Hôpital Erasme - ULB H Solomon, J W Man, G Jackson. Heart. 2003

57
Physiopathologie de l’ éjaculation prématurée
La phase de plateau « raccourcie »

58
Traitement de l’éjaculation prématurée: les inhibiteurs de la re-captation de la sérotonine
Sertraline : Serlain Paroxétine : Aropax Fluoxétine : Prozac Clomipramine : Anafranil Dapoxétine : Priligy (30 ou 60 mg) avant le RS
 avant le RS.")
59
Et la partenaire… Témoin (indifférente ?) du trouble d’éjaculation ?
Victime ? Responsable ?

60
La partenaire est importante…
Dans l’anamnèse du trouble d’éjaculation Dans le bilan Dans le traitement… Notion de dynamique de couple

61
Les perturbations de l’éjaculation
Perturbations chronologiques - éjaculation prématurée - éjaculation retardée Perturbations balistiques - éjaculation rétrograde - anéjaculation

62
Etiologies de l’éjaculation rétrograde
Chirurgie de l’adénome bénin de la prostate Causes neurologiques : - diabète - trauma local Médicaments : alpha-bloquants

63
Etiologies de l’anéjaculation
Chirurgie radicale du cancer de : - prostate et vessie (anéjaculation par la force des choses) - digestive : rectum et colon gauche Chirurgie vasculaire Chirurgie rétropéritonéale Médicaments : agents sclérosants (phénol)
 - digestive : rectum et colon gauche. Chirurgie vasculaire. Chirurgie rétropéritonéale. Médicaments : agents sclérosants (phénol)")
64
Diagnostic différentiel : éjaculation rétrograde > anéjaculation
Anamnèse Examen microscopique des urines post-coïtales : spermatozoïdes (+) éjaculation rétrograde spermatozoïdes (-) anéjaculation
 éjaculation rétrograde. spermatozoïdes (-) anéjaculation.")
65
Orgasme sans éjaculation
Étiologie organique après chirurgie urologique pour cancer (prostate/ vessie) Etiologie psy inhibition centrale
 Etiologie psy. inhibition centrale.")
66
Ejaculation sans orgasme
Étiologie organique Traumatisme médullaire (blessés médullaires) Étiologie psy : stress
 Étiologie psy : stress.")
Présentations similaires